
CNS nontumor
Toxic and metabolic disorders
Radiation injury
Authors: Palgun Nisarga, M.D., Kymberly A. Gyure, M.D.
Editorial Board Member: Meaghan Morris, M.D., Ph.D.
Deputy Editor-in-Chief: Chunyu Cai, M.D., Ph.D.


Last author update: 24 July 2023
Last staff update: 24 July 2023
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Radiation injury

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Diagrams / tables | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Frozen section description | Frozen section images | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Cytology images | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Nisarga P, Gyure KA. Radiation injury. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/cnsradiationinjury.html. Accessed March 30th, 2025.
Definition / general
- Radiation therapy is commonly used as adjuvant therapy for primary and secondary malignant CNS neoplasms
- Includes autonomic, cognitive and functional deficits
- Spectrum of toxic CNS effects is classified based on time of appearance of symptoms
- Histological features range from no obvious lesions to overt brain necrosis
Essential features
- Radiation injury mainly affects white matter
- Typically classified based on time of appearance of symptoms
- Late focal radiation injury: differential diagnosis includes recurrent / residual tumor
- Acute, early delayed and late (diffuse) radiation injury: clinical and radiological diagnosis
Terminology
- Radiation induced brain injury
- CNS lesions secondary to radiation injury are typically classified based on time of appearance of symptoms (see Diagrams / tables) (Radiat Res 2000;153:357)
- Acute radiation induced brain injury: days to weeks
- Early delayed radiation induced brain injury: weeks to 3 - 6 months
- Late radiation induced brain injury (focal and diffuse): > 3 - 6 months
- CNS lesions secondary to radiation injury are typically classified based on time of appearance of symptoms (see Diagrams / tables) (Radiat Res 2000;153:357)
- Treatment induced necrosis of brain (in neurooncology setting): also known as late radiation induced brain injury, focal type; includes chemoradiation or only radiation effects
- Necrotizing leukoencephalopathy: diffuse white matter injury following chemotherapy with or without radiation (AJNR Am J Neuroradiol 1991;12:45)
- Radiation induced brain cavernomas (Acta Biomed 2019;90:77)
- Radiation induced brain aneurysms (World Neurosurg 2020;135:339)
- Additional terminologies
- Pseudoprogression - transient, weeks to < 6 months
- Progressive disease - recurrent / residual disease status post therapy
- Pseudoresponse - frequently observed in high grade glioma patients treated with angiogenesis inhibitors (e.g.. bevacizumab) (Semin Neurol 2017;37:589)
ICD coding
- ICD-10: G93.89 - other specified disorders of brain
- Not well characterized
- Applicable to postradiation encephalopathy
Epidemiology
- Radiation therapy (adjuvant) for primary and secondary malignant CNS neoplasms
- Prevalence of late radiation induced brain injury
- Based on clinical and imaging features: 37 - 58% among survivors, with an overall prevalence of 14% (AJNR Am J Neuroradiol 1991;12:45)
- Based on histologic features: 4 - 5% (Int J Radiat Oncol Biol Phys 1981;7:243, Cancer 1975;36:1681)
Sites
- White matter in field of (or adjacent to) previous radiation therapy in primary and metastatic CNS neoplasms
- White matter of inferior temporal lobe and lower part of brain stem in nasopharyngeal carcinomas
- Based on site, radiation induced brain injuries are classified as (IntechOpen: Radiation Induced Brain Injury After Radiotherapy for Brain Tumor [Accessed 7 April 2023])
- Cerebral type
- Brain stem type
- Cerebellar type
- Mixed type
- Based on site, radiation induced brain injuries are classified as (IntechOpen: Radiation Induced Brain Injury After Radiotherapy for Brain Tumor [Accessed 7 April 2023])
Pathophysiology
- Acute radiation induced brain injury: disruption of blood brain barrier, edema and increased intracranial pressure (focal)
- Early delayed radiation induced brain injury: transient demyelination
- Late radiation induced brain injury (focal and diffuse): microvascular injury resulting in tissue hypoxia, demyelination and gliosis, white matter necrosis
- Experimental hypothesis
- Vascular hypothesis (late radiation injury)
- Radiation induced vascular changes: vessel wall thickening, vessel dilation and endothelial cell nuclear enlargement (dose dependent); capillary rarefaction
- Parenchymal / glial hypothesis
- Dynamic interaction between the 2 hypotheses
- Vascular hypothesis (late radiation injury)
- Pseudoprogression
- Not well understood (Neuro Oncol 2019;21:1118)
- Transient interruption of myelin synthesis secondary to radiation injury to oligodendrocytes could be a possible mechanism (Int J Mol Sci 2014;15:11832)
- Higher incidence in treated MGMT methylated glioblastoma (2 times) compared to the unmethylated tumors (J Clin Oncol 2008;26:2192)
- Reference: Front Oncol 2012;2:73
Etiology
- Unknown predisposing intrinsic factors (brain location treated, age, clinical status, tumor diagnosis and genetic susceptibility) (Neurooncol Adv 2020;2:vdaa057, Neuro Oncol 2019;21:1118)
- Partly identified extrinsic factors (dose / technique of the therapy) (Neurooncol Adv 2020;2:vdaa057, Neuro Oncol 2019;21:1118)
- Acute CNS syndrome is seen with > 30 Gy; white matter necrosis is seen with > 60 Gy
- Uncommon with modern radiation techniques (Front Oncol 2012;2:73)
- Late radiation injury (both focal and diffuse) is seen with the modern radiation techniques (Front Oncol 2012;2:73)

Clinical features
- Latency: 0 - 32 years (mean: 6 years)
- Clinical features are heterogeneous and difficult to predict
- Acute radiation induced brain injury: headache, fatigue and drowsiness
- Transient worsening of symptoms
- Early delayed radiation induced brain injury: generalized weakness, somnolence, attention deficits and short term memory loss
- Usually transient
- Late radiation induced brain injury: reflects damage to both hippocampal and nonhippocampal dependent domains (irreversible / progressive / fatal)
- Focal radiation injury: focal neurologic deficits and focal increase in intracranial pressure
- Indistinguishable from symptoms due to a mass of any kind
- Principal clinical differential diagnosis is recurrent / residual tumor (progressive disease)
- Diffuse radiation injury (cognitive impairment): decreased verbal memory, spatial memory, attention, problem solving ability and executional functions
- Can also have depression, anxiety and somatization
- Focal radiation injury: focal neurologic deficits and focal increase in intracranial pressure
- Advanced stages: dementia, stupor state, hallucinations and delusion
- Pseudoprogression
- Occurs in ~21 - 31% of malignant gliomas treated with radiation and chemotherapy
- Significant mass effect and clinical neurologic deficits (Semin Neurol 2017;37:589)
- Suggest a transient course with spontaneous recovery (Int J Mol Sci 2014;15:11832)
- References: IntechOpen: Radiation Induced Brain Injury After Radiotherapy for Brain Tumor [Accessed 7 April 2023], Front Oncol 2012;2:73, Neuro Oncol 2019;21:1118
Diagnosis
- Acute, early delayed and late (diffuse) radiation injury: clinical and radiological diagnosis
- Late (focal) radiation injury (diagnostic ambiguity)
- Clinically and radiographically overlap with recurrent / residual disease
- Histopathologic diagnosis depends on pathologist's experience and subjective impression
- Radiation necrosis versus recurrent / residual tumor
- Requires multidisciplinary approach (neuropathologist, neuroradiologist, radiation oncologist, neurosurgeon and neurooncologist) (J Neurooncol 2013;113:485)
- Reference: Neuro Oncol 2019;21:1118
Radiology description
- Late (focal) radiation injury
- CT: focal hypodensity, contrast enhancement, mass effect
- MRI: focal decreased signal on T1WI; focal hyperintensity on T2WI, contrast enhancement, mass effect
- Late (diffuse) radiation injury
- CT: diffuse white matter hypodensity, contrast enhancement, mass effect
- MRI: diffuse decreased white matter signal on T1WI; diffuse white matter hyperintensity on T2WI
- Pseudoprogression
- Represents a unique, transient, predominantly radiographic phenomenon encountered in patients with high grade glioma status post chemoradiation
- MRI - increase in abnormal nodular enhancement on T1 post contrast; increase in T2/FLAIR signal hyperintensities (suggestive of cerebral edema) (Semin Neurol 2017;37:589)
- Reference: AJNR Am J Neuroradiol 1991;12:45
Radiology images
Images hosted on other servers:

Focal radiation necrosis

Differential diagnoses

Hemorrhagic radiation injury

Diffuse white matter injury

Diffuse white matter change (severe)

Concurrent focal and diffuse white matter injury

Diffuse necrotizing leukoencephalopathy


Radiation necrosis of pons

Abnormal enhancement in left occipital lobe

Irregular enhancement around surgical cavity

Pseudoprogression
Prognostic factors
- Radiation necrosis and pseudoprogression without active tumor is associated with better prognosis (J Neurooncol 2013;113:485)
- Active malignant tumor portends poor prognosis (percentage treatment response has limited prognostic value) (J Neurooncol 2019;141:421)
- Increased Ki67 proliferation index is associated with worse prognosis
- See Etiology
Case reports
- 23 year old woman with remote history of low grade brainstem glioma, with delayed radiation induced stroke (Pediatr Neurol 2019;98:87)
- 37 year old man with radiation retinopathy after external beam irradiation for nasopharyngeal carcinoma (Pract Radiat Oncol 2018;8:366)
- 52 year old man with cystic radiation encephalopathy after radiotherapy treatment for nasopharyngeal carcinoma (BMC Neurol 2021;21:59)
- 59 year old man's autopsy revealing late delayed radiation injury following radiotherapy treatment at age 14 (Neuropathology 2019;39:106)
Treatment
- Symptomatic treatment
- Oral corticosteroids for symptomatic cases
- Resection with frozen section diagnosis
- No known medical therapy for cognitive impairment (Front Oncol 2012;2:73)
- Hippocampal avoidance strategies
- Stereotactic conformal radiotherapy
- Intensity modulated radiotherapy
- Proton beam therapy
- Potential therapies under investigation (IntechOpen: Radiation Induced Brain Injury After Radiotherapy for Brain Tumor [Accessed 7 April 2023], Neurooncol Adv 2020;2:vdaa057)
- Antiplatelet and anticoagulation
- Reactive oxygen species (ROS) scavengers
- Improving microcirculation: butylphthalide
- Neurogenesis: neural stem cell therapy
- Renin angiotensin system inhibitors
- Anti-VEGF antibody
- Hyperbaric oxygen treatment
- Exercise
- Small molecule compounds targeting p53 isoform Δ133p53α
- Peroxisomal proliferator activated receptor agonists
- Memantine
- Lithium
Gross description
Frozen section description
- Gross: see Gross description
- Squash / smears: see Cytology description
- Microscopy
- Challenging to differentiate between postradiation effects (radiation induced atypia) and brain tumor (residual / recurrent)
- Experience improves accuracy
- Seek second opinion when unsure
- See Microscopic (histologic) description - focal late radiation injury; and see Differential diagnosis - focal late radiation induced brain injury (treatment induced necrosis) versus recurrent / residual tumor
Frozen section images
Contributed by Palgun Nisarga, M.D.
Negative for tumor
Recurrent / residual tumor
Microscopic (histologic) description
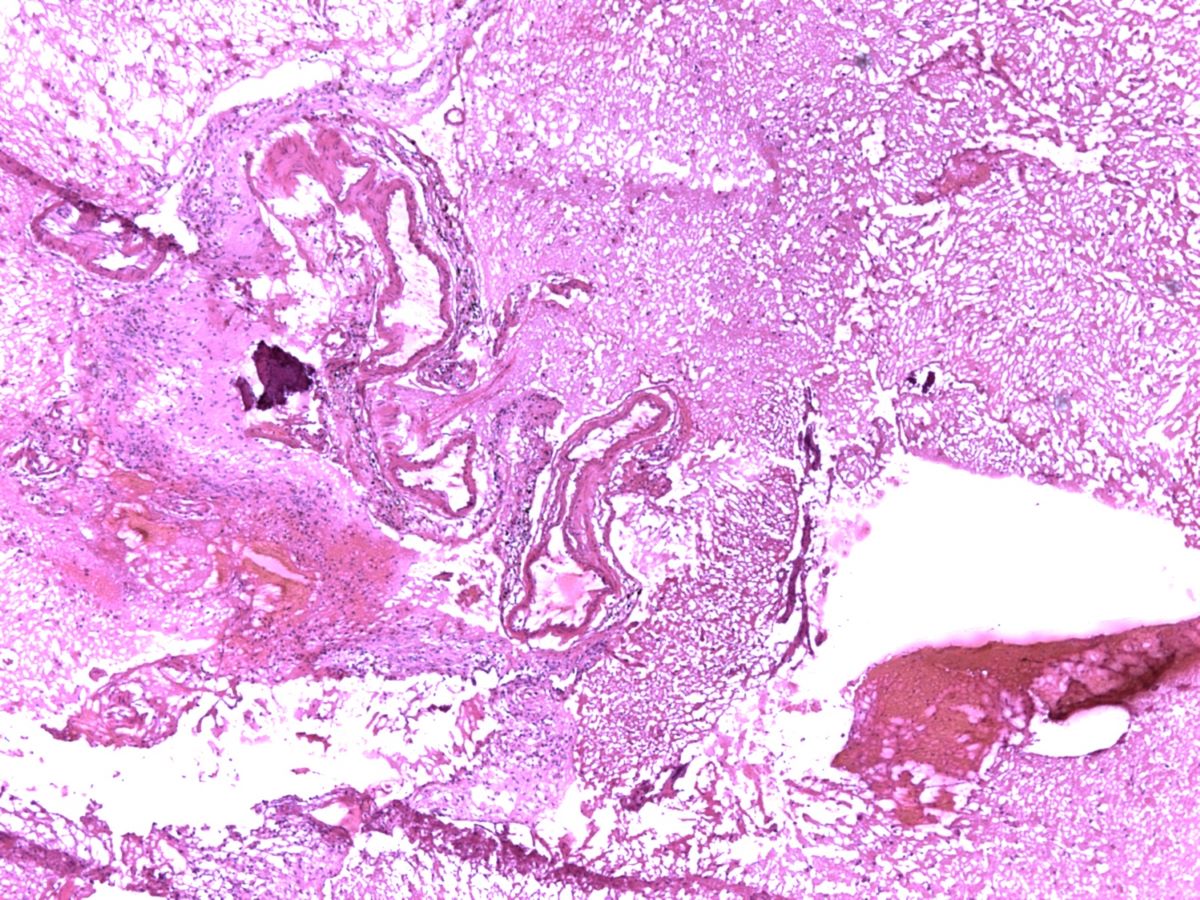
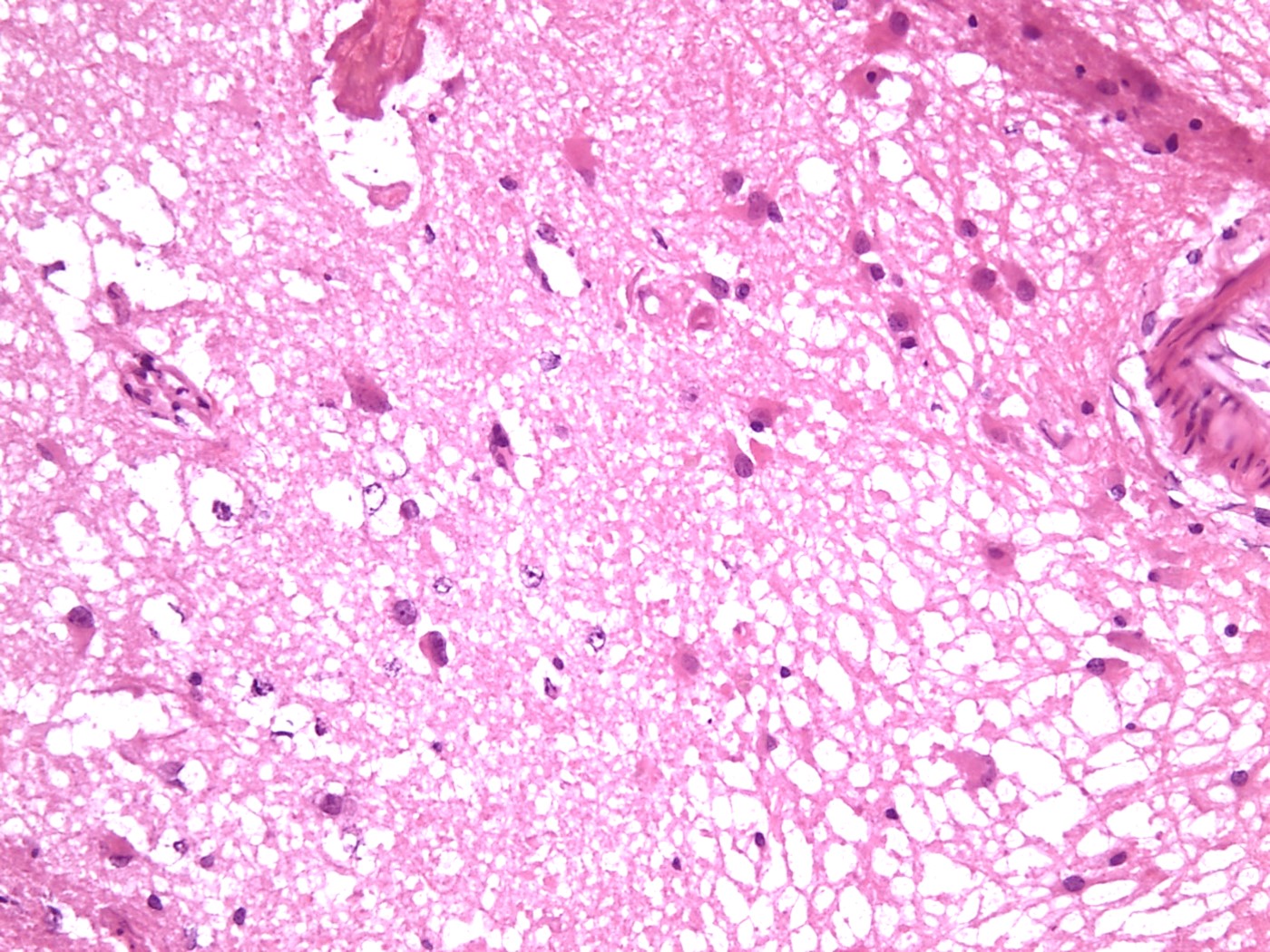
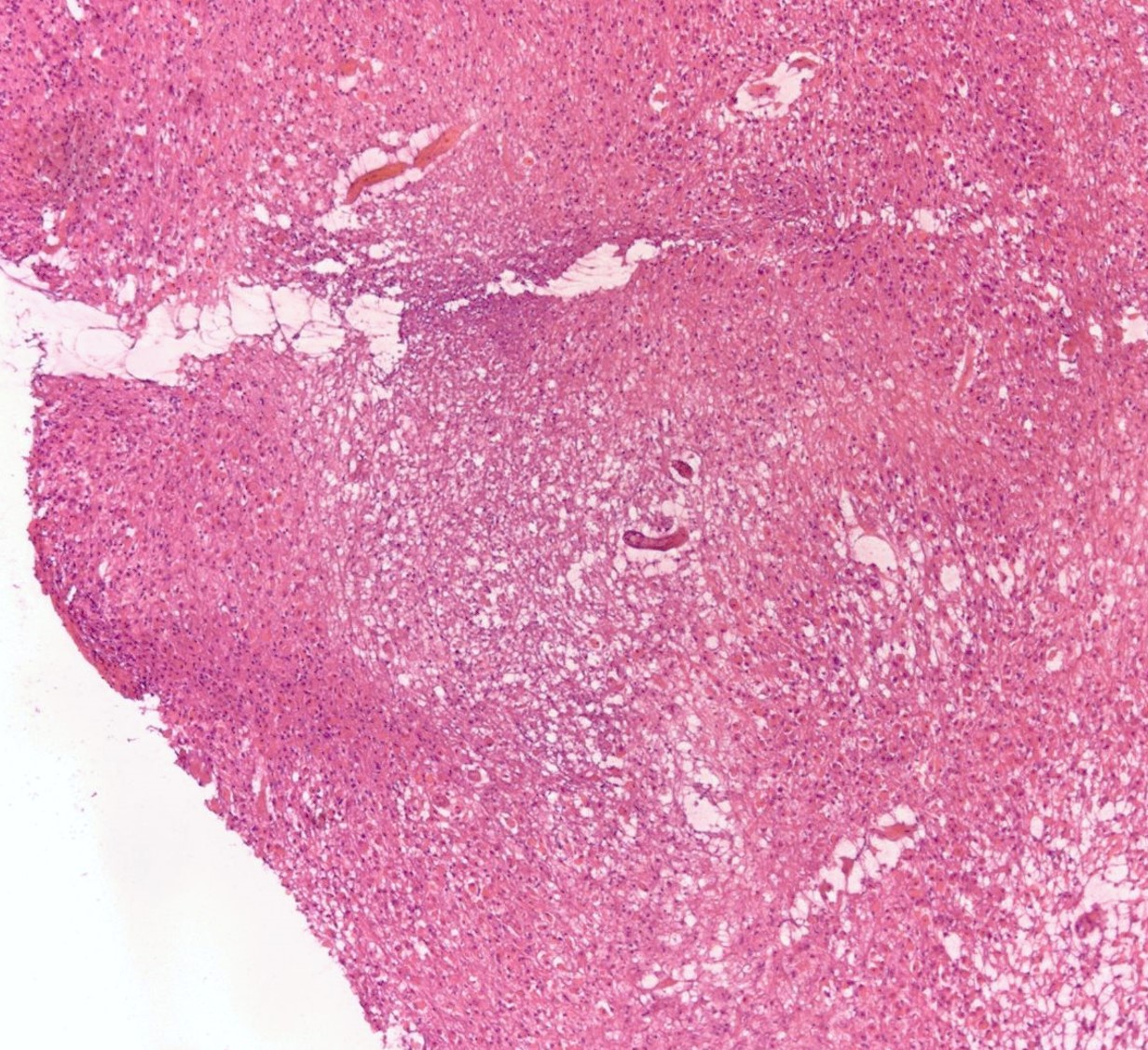
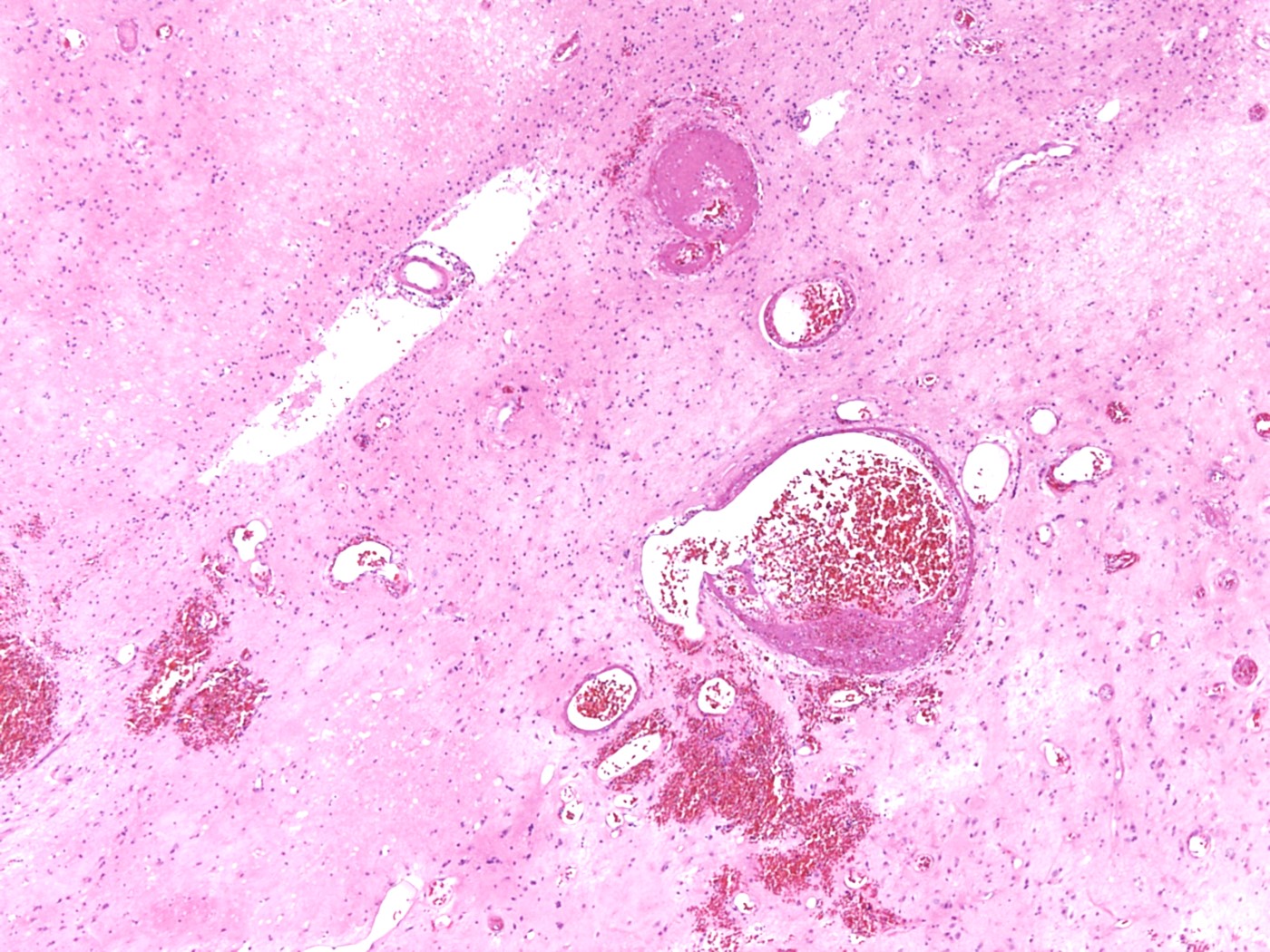
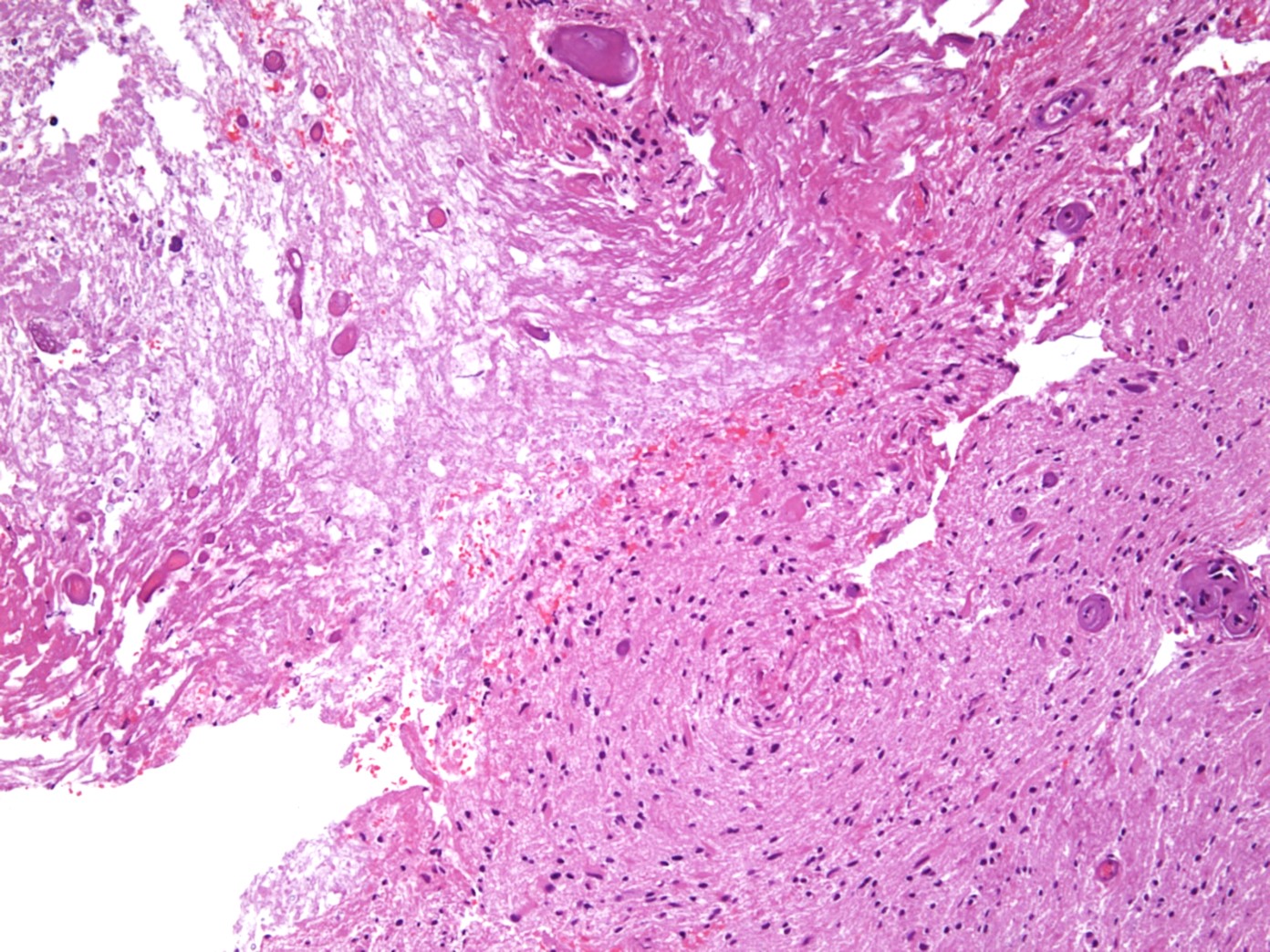
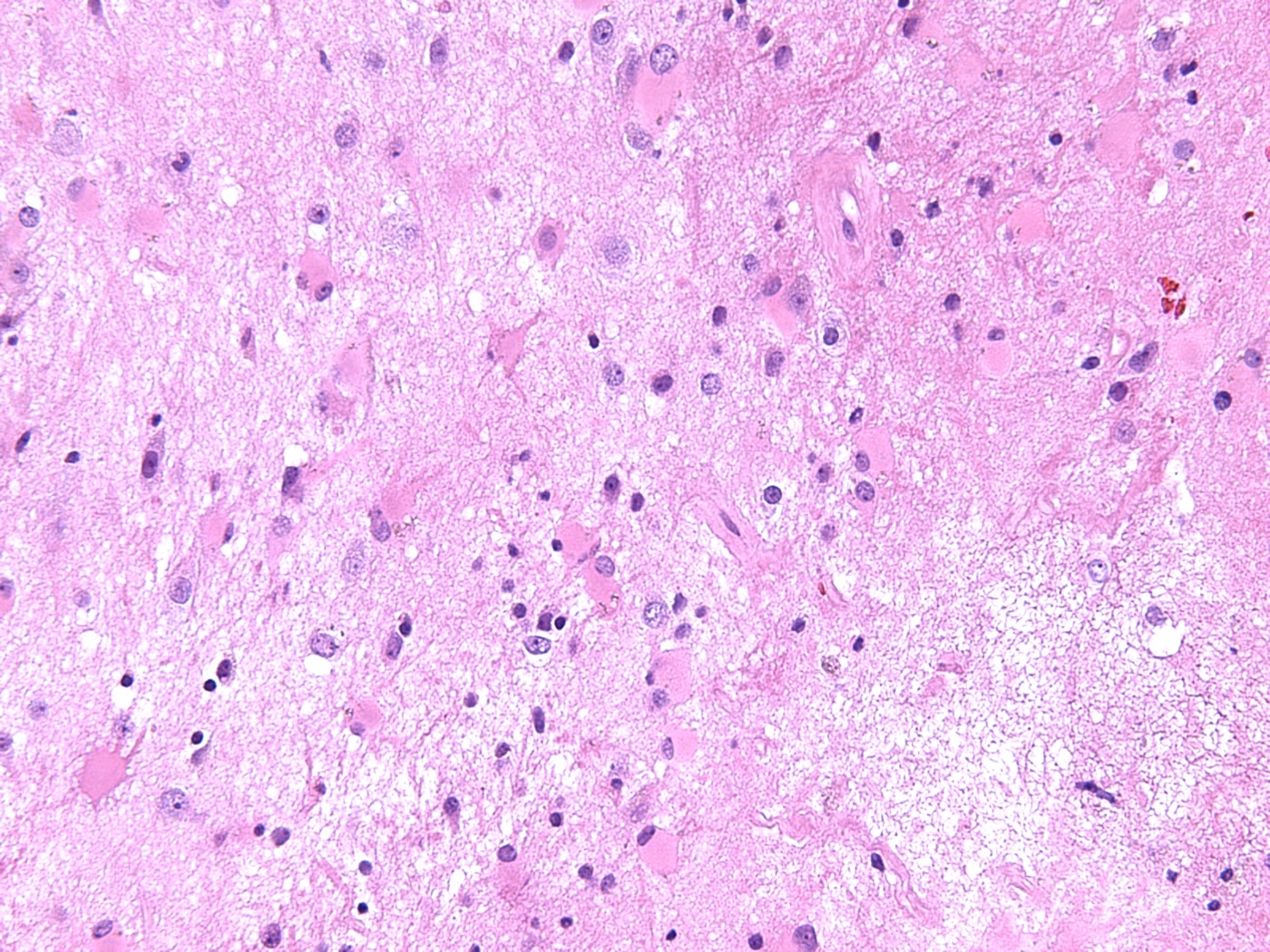
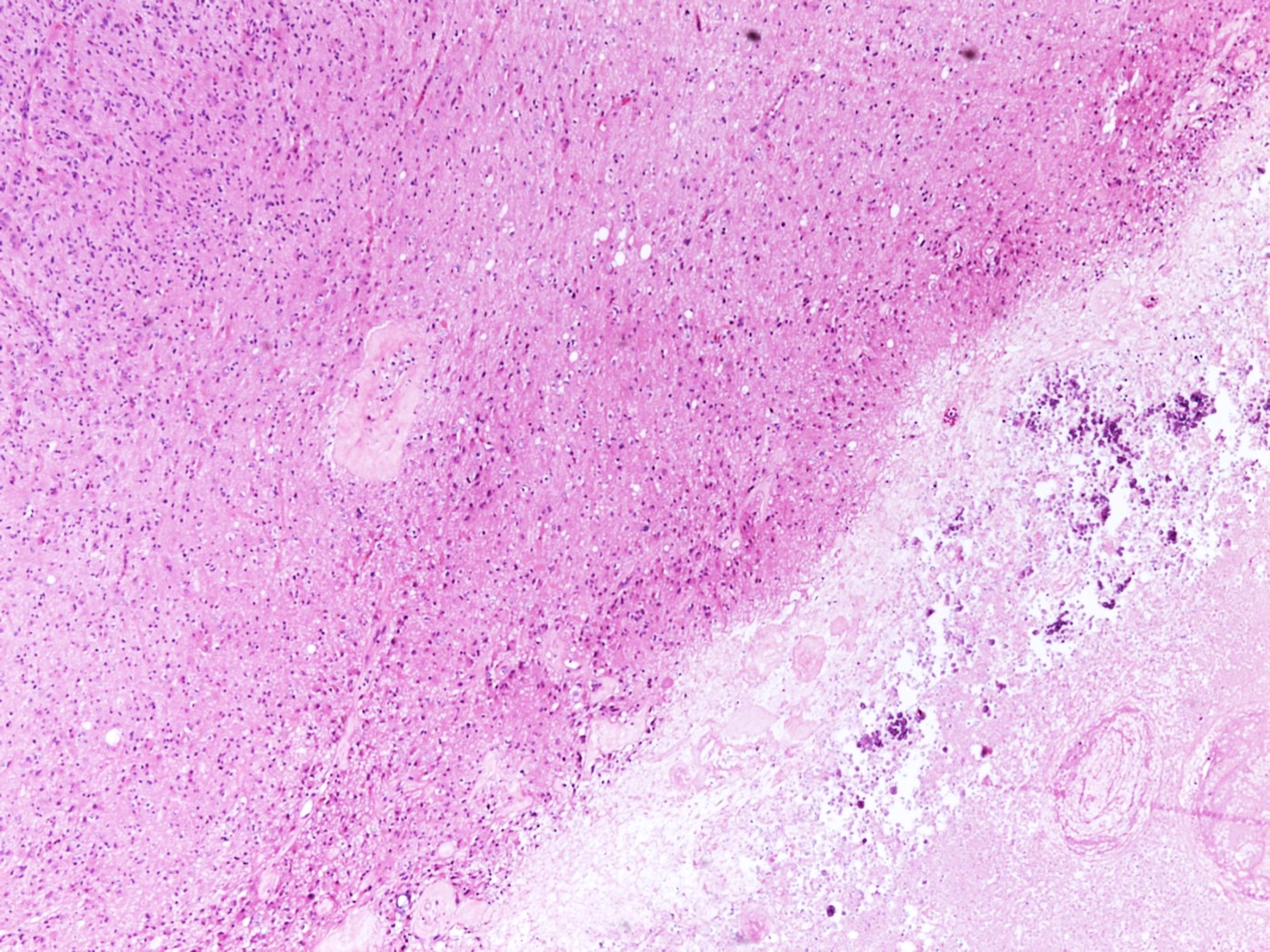
- Focal late radiation injury
- Hyalinization and fibrinoid necrosis of small arteries and arterioles (characteristic finding) and narrow lumens with endothelial proliferation
- White matter changes range from minimal changes to rarefaction of myelin and reactive gliosis to coagulative necrosis
- With or without perivascular mononuclear infiltrate
- Radiation induced cytologic atypia
- Diffuse late radiation injury
- Histopathologic diagnosis not indicated
- White matter changes similar to focal late radiation injury
- Pseudoprogression
- No established histopathological classification criteria for treatment necrosis or pseudoprogression (Neuro Oncol 2019;21:1118)
- Progressive disease
- Tumor cellularity depends on the treatment (radiation) response
- In practice, the most common histologic finding is radiation necrosis with active tumor (J Neurooncol 2019;141:347)
- References: AJNR Am J Neuroradiol 1991;12:45, IntechOpen: Radiation Induced Brain Injury After Radiotherapy for Brain Tumor [Accessed 7 April 2023]
Microscopic (histologic) images
Contributed by Palgun Nisarga, M.D.
Negative for tumor
Negative for tumor
Recurrent / residual tumor
Cytology description
Cytology images
Contributed by Palgun Nisarga, M.D.
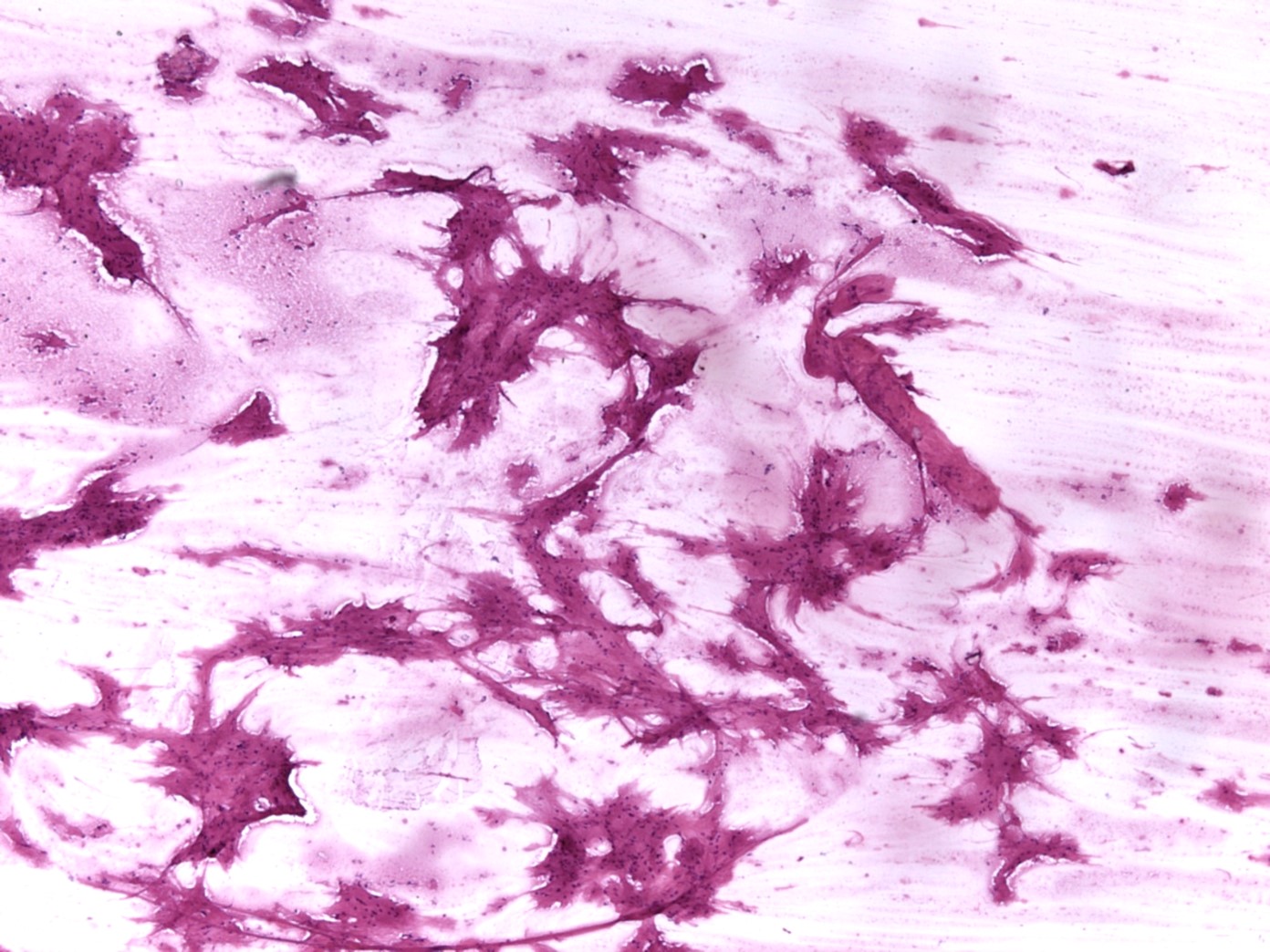
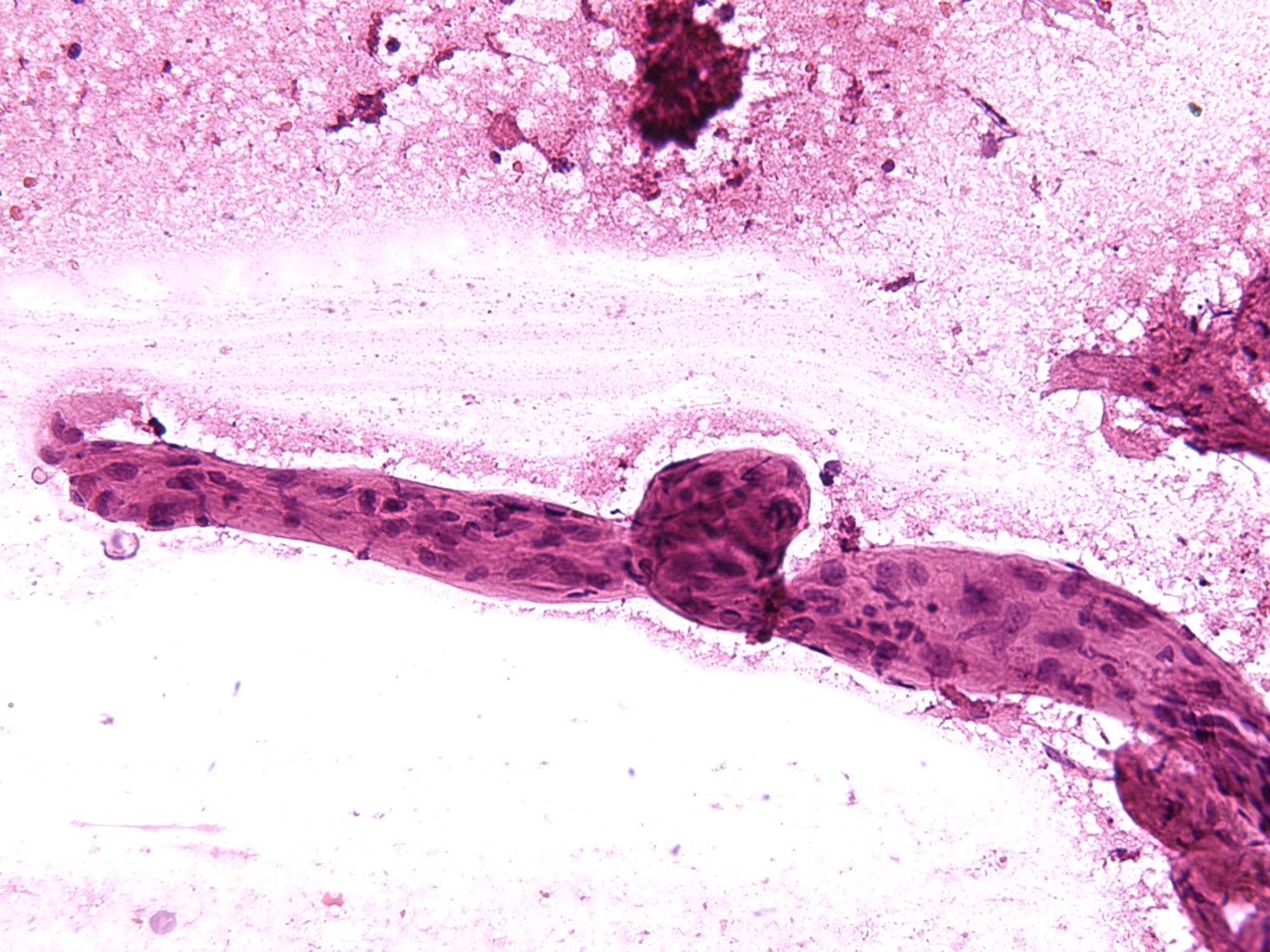
Squash preparation (frozen)
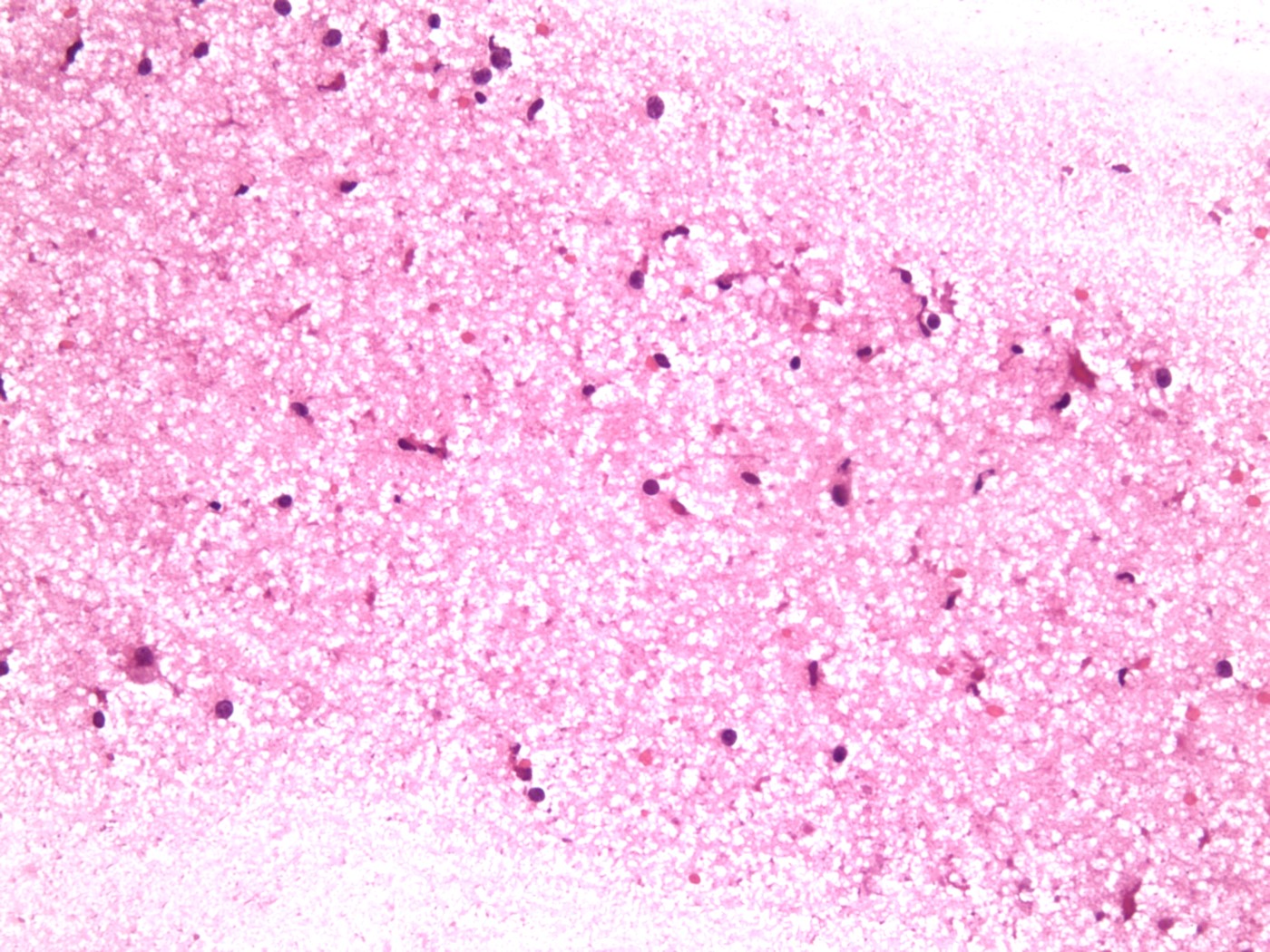
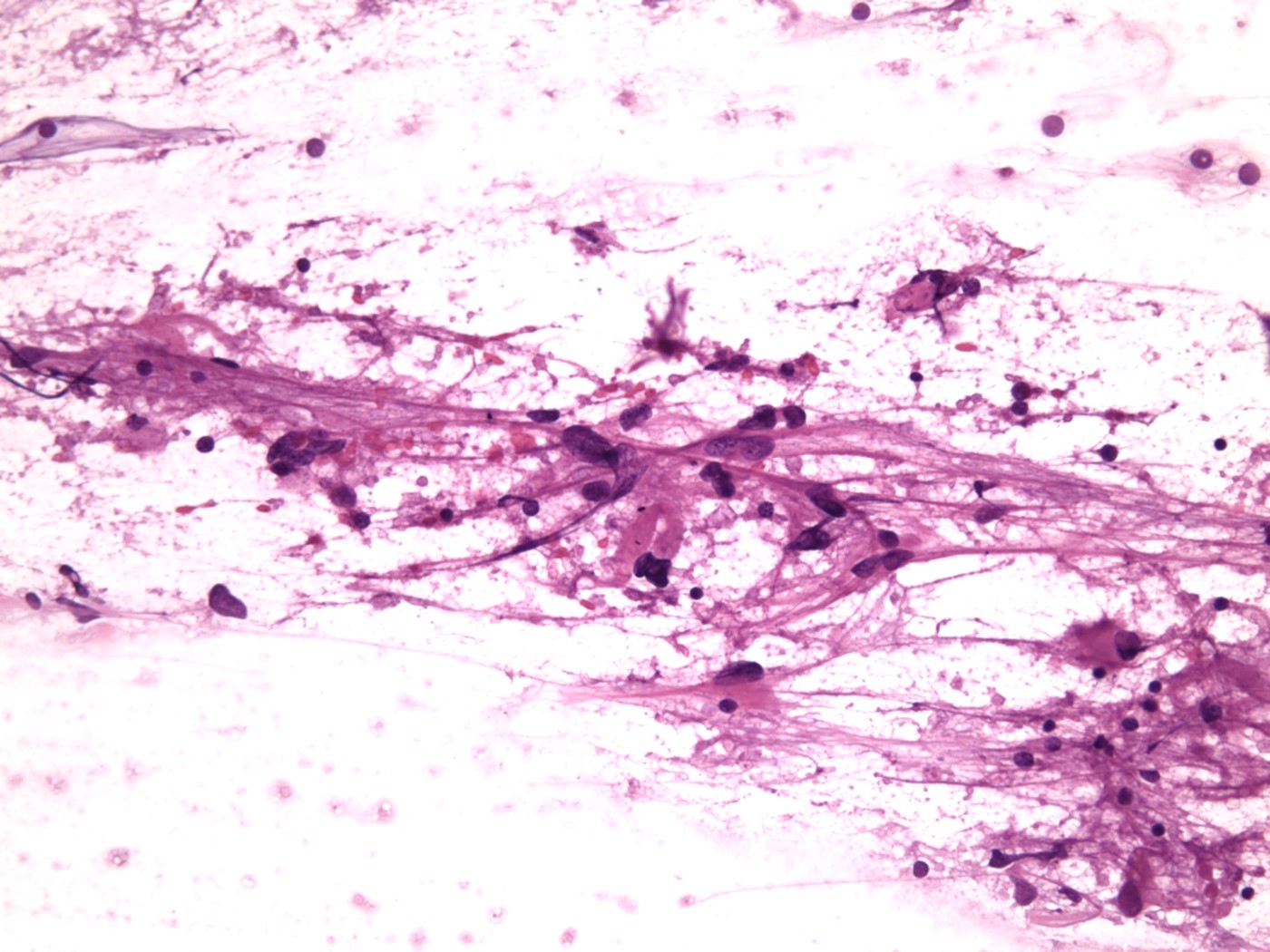
Squash preparation (frozen)
Sample pathology report
- Brain, right temporal, resection:
- Changes consistent with radiation / chemotherapy effect
- No evidence of tumor
- Brain, left frontal, resection:
- Recurrent / residual glioblastoma with changes consistent with radiation / chemotherapy effect
Differential diagnosis
- Focal late radiation induced brain injury (treatment induced necrosis) versus recurrent / residual tumor:
- Clinical and radiological features similar
- Radiation necrosis
- Hyalinization and fibrinoid necrosis of small arteries and arterioles (characteristic finding) and endothelial proliferation
- Reactive gliosis to coagulative necrosis
- Perivascular mononuclear infiltrate may be present
- Recurrent / residual tumor
- Tumor cells should be differentiated from radiation induced atypia
- IDH1 (R132H) is useful in astrocytomas to differentiate from reactive astrocytes
- Ki67 could be helpful; no established cutoff value
- Molecular studies may be helpful (Strahlenther Onkol 2022;198:873, J Neurooncol 2013;113:485)
- Diffuse late radiation induced brain injury versus Alzheimer disease and dementia spectrum disorders:
- Clinically and radiologically different diseases
- Histopathologic diagnosis not required
- References: IntechOpen: Radiation Induced Brain Injury After Radiotherapy for Brain Tumor [Accessed 7 April 2023], Neurooncol Adv 2020;2:vdaa057, AJNR Am J Neuroradiol 1991;12:45
Board review style question #1
Intraoperative histopathologic evaluation is recommended in which of the following types of brain radiation injury?
- Acute radiation induced brain injury
- Early delayed radiation induced brain injury
- Early delayed and late focal radiation induced brain injury
- Late diffuse radiation induced brain injury
- Late focal radiation induced brain injury
Board review style answer #1
E. Late focal radiation induced brain injury. Late focal radiation injury can be confused with residual / recurrent tumor based on the imaging findings. Answers A - D are incorrect because they have imaging findings different from that of a tumor.
Comment Here
Reference: Radiation injury
Comment Here
Reference: Radiation injury
Board review style question #2
What is the characteristic histopathologic finding in focal (late) radiation induced brain injury?
- Coagulative necrosis with reactive gliosis
- Hyalinization and fibrinoid necrosis of small sized arteries
- Narrow vascular lumen with endothelial proliferation
- Perivascular mononuclear infiltrate
- Rarefaction of myelin
Board review style answer #2
B. Hyalinization and fibrinoid necrosis of small sized arteries. Answers A, C, D and E are incorrect because these findings are nonspecific for radiation injury and can be seen in other conditions.
Comment Here
Reference: Radiation injury
Comment Here
Reference: Radiation injury
