
Chemistry, toxicology & urinalysis
Organ specific
Thyroid
Thyroid function panel
Author: Panudda Srichomkwun, M.D., M.Sc.
Editorial Board Members: Andrey Bychkov, M.D., Ph.D., Patricia Tsang, M.D., M.B.A.

Last author update: 25 June 2020
Last staff update: 18 May 2021
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Thyroid function panel [title]

Table of Contents
Thyroid function test interpretation | Thyroid stimulating hormone (TSH) | Thyroid hormone (T4, T3 and rT3) | Total thyroid hormone measurement | Free thyroid hormone measurement | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Srichomkwun P. Thyroid function panel. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/chemistrythyroidfunction.html. Accessed April 2nd, 2025.
Thyroid function test interpretation
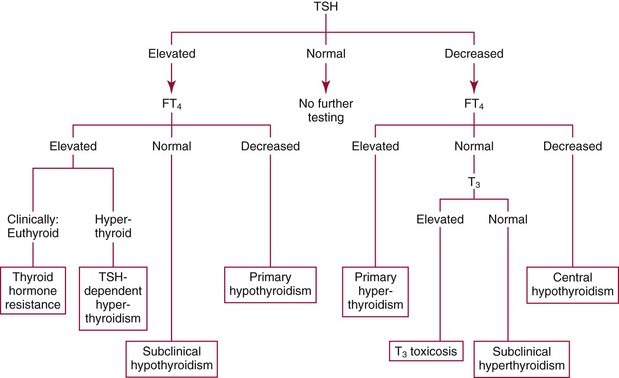
- Thyroid function test (TFT) algorithm (Best Pract Res Clin Endocrinol Metab 2013;27:745)

- Initial screening with serum thyroid stimulating hormone (TSH) level is the most common approach
- If TSH level is abnormal, free thyroxine (T4) should be evaluated
- A commonly used screening panel is TSH with reflex to free T4
- Free triiodothyronine (T3) can be added for the evaluation of hyperthyroidism when free T4 is not elevated
- Potential confounding factors for TFT interpretation
- Age: age specific reference ranges are important in newborn and elderly
- Pregnancy
- Low TSH (first trimester; secondary to increased human chorionic gonadotropin [hCG])
- High total T4 and T3 (from first trimester; secondary to increased thyroxine binding globulin [TBG])
- Changes in free T4 and T3
- Trimester specific reference ranges should be used wherever possible
- Levothyroxine (LT4) therapy: mildly elevated free T4 (but normal free T3), intermittent hormone ingestion may result in normal or elevated free T4 but fails to normalize TSH
- Confounding medications / supplements: alter thyroid physiology (e.g. amiodarone) or cause artifactual laboratory results (e.g. heparin or biotin) (N Engl J Med 2019;381:749)
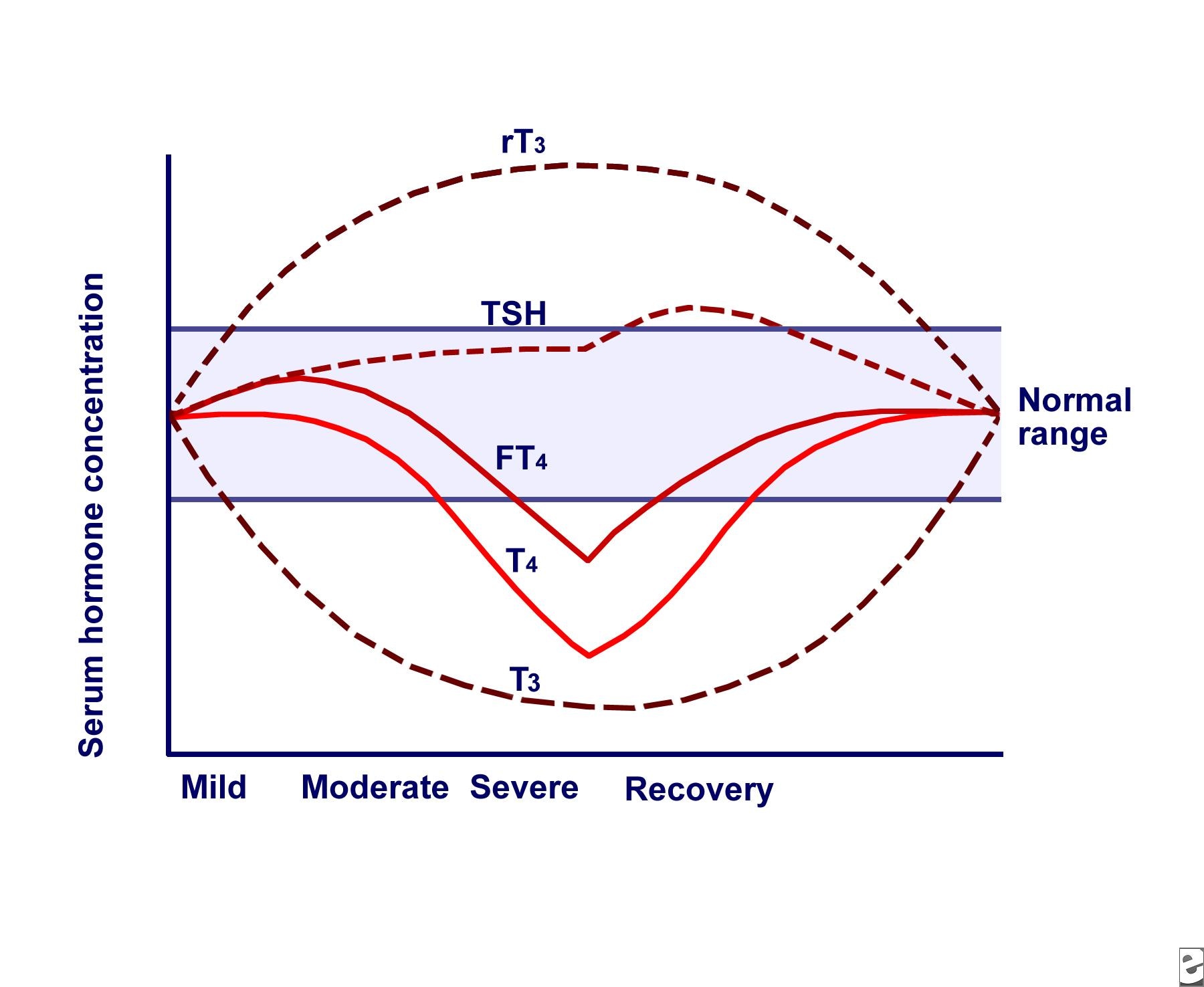
- Nonthyroidal illness (NTI): different TFT results depend on severity of illness (eMedicine: Euthyroid Sick Syndrome [Accessed 25 June 2020])

- Mild illness: low free T3, normal free T4, normal or low TSH (also known as low T3 syndrome)
- Severe illness: very low free T3, low free T4, normal or low TSH
- Recovery phase: low free T3, low free T4, high TSH (usually < 20 μU/mL)
- TFT patterns and associated clinical conditions (Best Pract Res Clin Endocrinol Metab 2013;27:745)

- Low free T3/T4 and high TSH: primary hypothyroidism
- Normal free T3, low free T4 and high TSH: early primary hypothyroidism
- High free T3/T4 and low TSH: primary hyperthyroidism (toxic adenoma, multinodular goiter or Graves disease)
- Normal free T3, high free T4 and low TSH (T4 toxicosis): iodine induced hyperthyroidism, primary hyperthyroidism with NTI
- High free T3, normal free T4 and low TSH (T3 toxicosis): primary hyperthyroidism in iodine deficiency area, earliest stages of primary hyperthyroidism
- Low free T3/T4 and normal or low TSH: central hypothyroidism, NTI
- High free T3/T4 and normal or high TSH: interference, familial dysalbuminemic hyperthyroxinemia (FDH), TSH secreting pituitary adenoma, resistance to thyroid hormone, acute psychiatric disorder, drug (amiodarone, heparin)
- Normal free T3/T4 and high TSH: subclinical hypothyroid, poor compliance of LT4, NTI recovery phase, TSH resistance, assay interference (heterophile antibodies, macroTSH)
- Normal free T3/T4 and low TSH: subclinical hyperthyroidism, recent treatment of thyrotoxicosis, assay interference, drug (steroid, dopamine)

Thyroid stimulating hormone (TSH)
-
General
- Also called thyrotropin
- Hypothalamic-pituitary-thyroid (HPT) axis regulates TSH release
- Hypothalamus secretes the thyroid releasing hormone (TRH), which stimulates thyrotrophs in the anterior pituitary to secrete TSH which consists of alpha subunit (same sequence as luteinizing hormone, follicle stimulating hormone, human chorionic gonadotropin [hCG]) and beta unit (differs from other hormones)
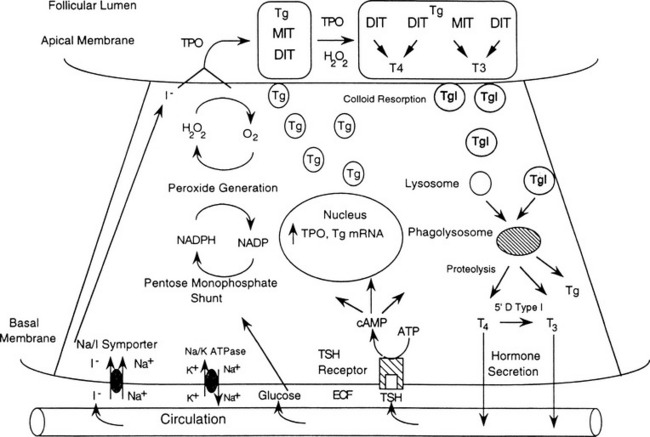
- Binding TSH to TSH receptor on thyroid follicular cell promotes increased uptake of iodide into thyroid follicular cells by active transport via sodium iodide symporter, synthesis of thyroglobulin, formation of T3 and T4, release of T3 and T4 into circulation (Ento Key: Thyroid Physiology and Thyroid Function Testing [Accessed 25 June 2020])

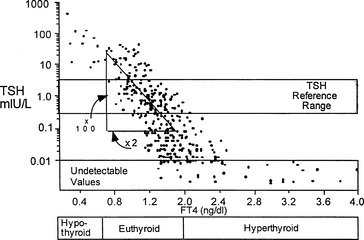
- T4 and T3 can exert negative feedback on TSH levels, with high levels of T3/T4 decreasing TSH (negative feedback) and low levels of T3/T4 increasing TSH levels from the anterior pituitary (positive feedback)

- There is a log linear relationship between T3/T4 and TSH with minor changes in TH resulting in major changes in TSH (Ento Key: Thyroid Physiology and Thyroid Function Testing [Accessed 25 June 2020])

- Most TSH assays use a "sandwich" format with 2 antibodies - capture and labeled detection - directed against different epitopes on TSH

- Presence of human anti-animal antibodies in a patient's serum can interfere with TSH measurement if directed against the same species as the assay antibodies, leading to falsely high TSH (Endocr Rev 2018;39:830)
- Depends on different platforms and methods: average 0.4 - 4 μU/mL
- Initial screening test for thyroid dysfunction unless the conditions below are suspected; in such cases, add free T4 and possibly also free T3 (PLoS One 2018;13:e0196631, Best Pract Res Clin Endocrinol Metab 2013;27:745):
- Confounding intercurrent illness or medication use
- Recent treatment for hyper or hypothyroidism
- Erratic or poor adherence to levothyroxine therapy
- Genetic or acquired disorders of the HPT axis
- Interference in thyroid function panel
- Annual screening for patients receiving thyroid hormone replacement therapy (target is 1 - 4 μU/mL) (wait 6 weeks to retest due to altered dose)
- Monitor target of thyroid hormone suppressive therapy after thyroidectomy in patients with differentiated thyroid carcinoma (target is 0.5 - 2.0 μU/mL if low risk, 0.1 - 0.5 μU/mL if moderate risk and < 0.1 μU/mL if high risk) (Thyroid 2016;26:1)
TSH measurement

TSH reference value
Indications for TSH testing
Thyroid hormone (T4, T3 and rT3)
General
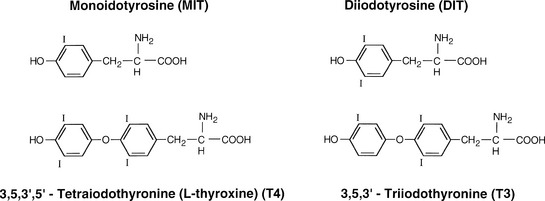
- The 2 principal thyroid hormones are thyroxine (also known as T4 or L-3,5,3',5'-tetraiodothyronine) and triiodothyronine (T3 or L-3,5,3'-triiodothyronine) (Ento Key: Thyroid Physiology and Thyroid Function Testing [Accessed 25 June 2020])

- Thyroxine (T4)
- Usual daily production is 110 nmol/day; half life is 5 - 7 days
- 100% produced in thyroid
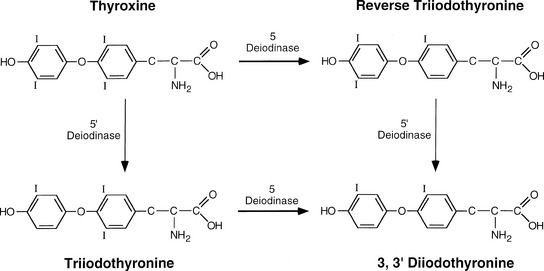
- 50% of T4 is 5' deiodinated to form T3, 40% is 5 deiodinated to form reverse T3 via 5-deiodinase (Ento Key: Thyroid Physiology and Thyroid Function Testing [Accessed 25 June 2020])

- Triiodothyronine (T3)
- Usual daily production is 50 nmol/day; half life is 1 day
- 80% from deiodination of T4 in nonthyroid tissue, 20% arises in thyroid gland
- Most of the TH circulating in the blood is bound to TH binding proteins: thyroxine binding globulin (TBG), transthyretin (TTR) and albumin
- Only a very small fraction of unbound TH (0.03% of T4 and 0.3% of T3) is biologically active and signal all tissues by binding TH nuclear receptor (THR)
- TH is metabolized by deiodination, conjugation with glucuronide and sulfate, ether link cleavage and side chain modification (oxidative deamination and decarboxylation) (Endotext: Metabolism of Thyroid Hormone [Accessed 25 June 2020])

- Reverse T3 (rT3)
- Also known as 3,3',5'-triiodothyronine
- Biologically inactive metabolite of T4 formed by selective deiodination
- Not routinely measured
- Serum rT3 levels are increased in systemic nonthyroidal illnesses except chronic renal failure and in patients taking drugs such as amiodarone, propylthiouracil, dexamethasone, propranolol and ipodate
Total thyroid hormone measurement
- Easier to measure than free TH
- Many inherited, acquired conditions and drugs can alter TBG level
- Pregnancy, contraceptive pills, estrogen receptor modulators, 5-fluorouracil, liver diseases, methadone, heroin, acute intermittent porphyria, hypothyroidism and inherited TBG excess (TBG-E) increase serum TBG resulting in high total TH but normal free TH
- Androgens, corticosteroids, hyperthyroidism, terminal illnesses and inherited TBG deficiency (TBG-D) decrease serum TBG resulting in low total TH but normal free TH
- Serum total TH is usually measured by immunoassay (automated competitive binding chemiluminescent assays)
- Serum total TH is also measured by liquid chromatography tandem mass spectrometry (LC-MS/MS) which results in more specific and accurate TH value than immunoassay but this technique needs expensive equipment and clinical expertise (Anal Bioanal Chem 2010;397:1831)
Free thyroid hormone measurement
- Free T4 measurement is preferred to total T4 whereas total T3 is preferred to free T3 (Best Pract Res Clin Endocrinol Metab 2013;27:689)
- Presence of factors in serum that affect free TH measurement include:
- Interferences (T4/T3 antibodies, human anti-animal antibodies) (Endocr Rev 2018;39:830)
- Variant thyroid hormone binding proteins: dominantly inherited genetic variants of albumin (familial dysalbuminemic hyperthyroxinemia [FDH] or transthyretin [transthyretin associated hyperthyroxinemia (TTR-AH)])
- Drugs (e.g. heparin and aspirin) (N Engl J Med 2019;381:749)
Methods of free TH measurement
- Free T4 index
- Free T4 index is calculated by dividing the total T4 by the T3 uptake ratio (percentage)
- T3 uptake test is performed by incubating the patient's serum with radiolabeled T3 tracer and subsequently adding resin that traps the remaining unbound radiolabeled T3; the value reported is the percent of tracer bound to the resin, which varies inversely with the number of available free binding sites for T3
- T3 uptake was designed to distinguish TBG excess and deficiency from hyperthyroidism and hypothyroidism:
- Hyperthyroidism: high serum total T4, high T3 uptake, high free T4 index
- TBG excess: high serum total T4, low T3 uptake, normal free T4 index
- Hypothyroidism: low serum total T4, low T3 uptake, low free T4 index
- TBG deficiency: low serum total T4, high T3 uptake, normal free T4 index
- Free TH ligand assays (indirect method) (Biochemia Medica 2016;26:436)
- Competition immunoassay is used
- Serum TH compete with labeled TH analog for a fixed number of TH antibody binding sites
- Serum TH compete with an immobilized TH analog for a labeled TH antibody
- Free hormone concentration is inversely proportional to the signal generated with fluorescence or chemiluminescence
- Different immunoassay platforms are available

- 1 step labeled T4 analog (Immulite, Siemens)
- 1 step analog 2 step incubation (Cobas, Roche Diagnostics)
- 2 step labeled T4 analog method (DXi, Beckman Coulter, Architect, Abbott)
- 1 step labeled antibody method (Vitros, Ortho Clinical Diagnostics)
- 2 step method was less susceptible to T4/3 autoantibodies than the 1 step method
- Competition immunoassay is used
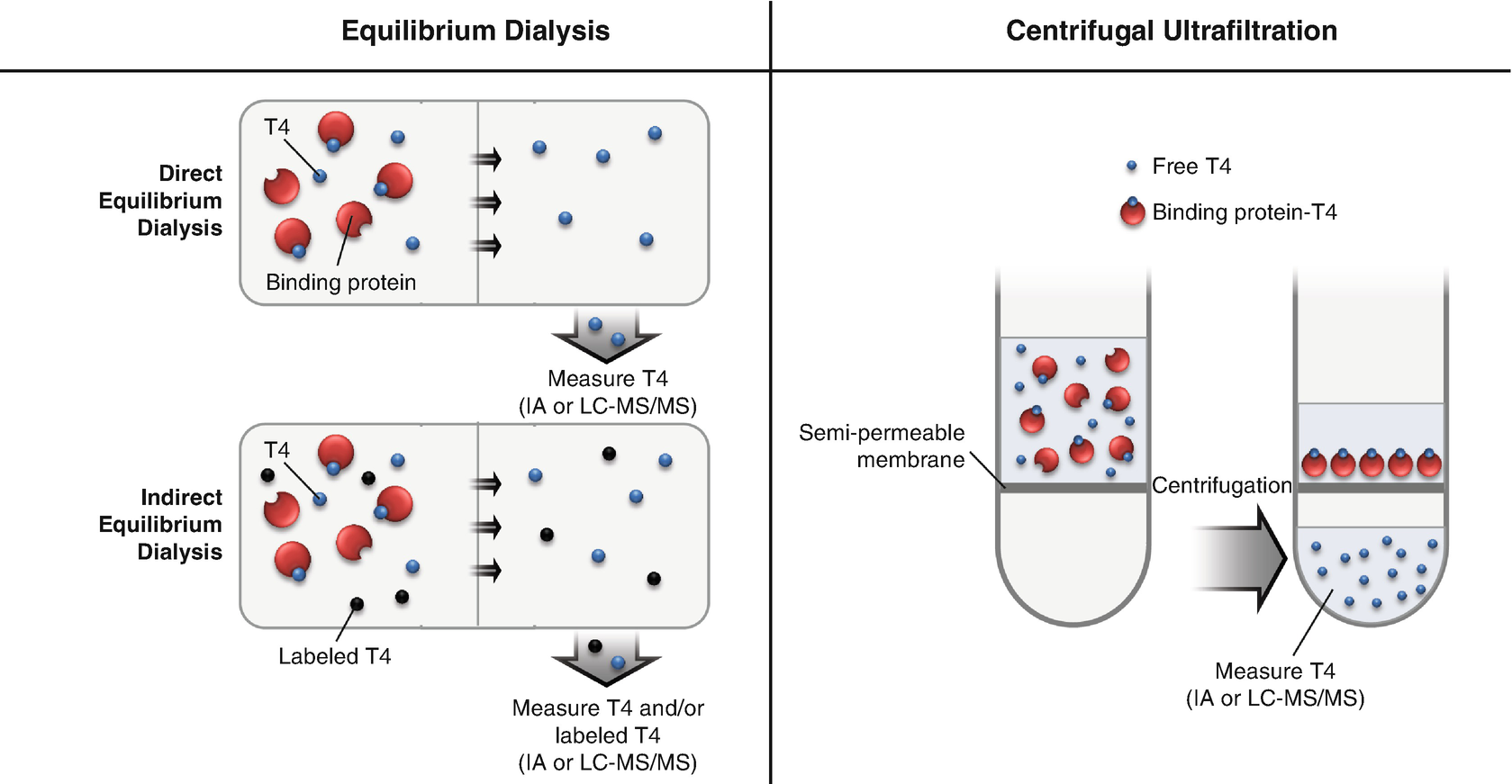
- Ultrafiltration (UF) and equilibrium dialysis (ED) (direct method) (Best Pract Res Clin Endocrinol Metab 2013;27:689)
- Methods with physical separation against ultrafiltrate / dialysate membrane and direct measurement of free T4 in protein depleted serum by immunoassay or LC-MS/MS

- Not affected by changes in binding protein concentration, T4/T3 autoantibodies or nonthyroidal illness
- Free thyroid hormone concentrations measured by LC-MS/MS correlate to a greater degree with log TSH values compared to concentrations measured by immunoassay (Clin Chem 2009;55:1380)
- Time consuming, expensive and requires rigorous control of the pH, temperature, membrane type / cutoff, minimum dilution and dialysis buffer
- Methods with physical separation against ultrafiltrate / dialysate membrane and direct measurement of free T4 in protein depleted serum by immunoassay or LC-MS/MS

Reference value
- Depends on different platforms and methods
- Cobas, Roche Diagnostics
- FT4 12 - 22 pmol/L (0.93 - 1.7 ng/dL)
- FT3 3.1 - 6.8 pmol/L (2 - 4.4 pg/mL)
Conversion factor
- FT4: multiply by 12.87 to convert from ng/dL to pmol/L
- FT3: multiply by 1.54 to convert from pg/dL to pmol/L
Board review style question #1
A 65 year old man with no history of thyroid disease is admitted to the medical intensive care unit for septic shock. Thyroid function test is performed due to hyponatremia: TSH 5 μU/mL (0.3 - 4.1), free T4 0.9 ng/dL (0.8 - 1.8), free T3 1.2 pg/mL (1.6 - 4).
What is the most likely cause of abnormal thyroid function test in this patient?
What is the most likely cause of abnormal thyroid function test in this patient?
- Heterophile antibodies
- Nonthyroidal illness
- Primary hypothyroidism
- Subclinical hypothyroidism
- TSH producing pituitary adenoma
Board review style answer #1
B. Nonthyroidal illness. TFT showed normal free T4, low T3 and slightly elevated TSH. Nonthyroidal illness is the likely background condition. In the early course of illness, free T3 will firstly decrease due to decrease of peripheral conversion while free T4 is still maintained; TSH level is variable (0.1 - 20 μU/mL). Heterophile antibodies is incorrect because normally heterophile antibodies will interfere with TSH measurement, causing falsely high TSH but normal free T4 and T3 level. Primary hypothyroidism is incorrect because free T4 level is normal and TSH level is too low for primary hypothyroidism. Subclinical hypothyroidism is incorrect because free T3 level is low. TSH producing pituitary adenoma is incorrect because free T3 and T4 level is not high. TFT pattern in TSH producing pituitary adenoma is high free T3/T4 and normal or high TSH.
Comment Here
Reference: Thyroid function panel
Comment Here
Reference: Thyroid function panel
Board review style question #2
A 55 year old woman with weight gain and fatigue was found to have an elevated serum TSH and was started on levothyroxine (LT4). She was referred for assistance in managing thyroid replacement therapy. Physical examination showed a pulse rate of 80 beats per minute, no goiter or thyroidectomy scar and normal deep tendon reflexes.
Which of the following is the most likely explanation for these findings?
| Date | TSH (0.3 - 4.1 μU/mL) | FT4 (0.8 - 1.8 ng/dL) | Levothyroxine dose (mg/day) |
| June 2019 | 12 | 1.3 | None |
| September 2019 | 11 | 1.7 | 0.075 |
| December 2019 | 10.5 | 2.1 | 0.100 |
Which of the following is the most likely explanation for these findings?
- Free T4 autoantibodies
- Heterophile antibodies
- Poor absorption of levothyroxine
- Resistance to thyroid hormone
- TSH producing pituitary adenoma
Board review style answer #2
B. Heterophile antibodies. Normal free T4 and high TSH on 06/2019 were compatible with subclinical hypothyroidism. Differential diagnosis is NTI recovery phase, TSH resistance, assay interference (heterophile antibodies, macroTSH), poor absorption of levothyroxine. After trial of LT4 replacement TFT, there were high free T4 and high TSH (similar level as the initial TSH) levels. The most likely explanation is that the patient had heterophile antibodies that caused falsely elevated TSH. When the patients takes LT4, free T4 level is elevated but TSH still high at the same level because of heterophile antibodies.
Free T4 autoantibodies is incorrect since free T4 level was normal at initial evaluation. Poor absorption of levothyroxine is incorrect since free T4 level increased after LT4 treatment. Resistance to thyroid hormone is incorrect since free T4 level was normal at presentation. TSH producing pituitary adenoma is incorrect since the patient did not have clinical thyrotoxicosis and free T4 level was normal at initial evaluation.
Comment Here
Reference: Thyroid function panel
Comment Here
Reference: Thyroid function panel
