
Chemistry, toxicology & urinalysis
General chemistry
Metabolism
Parathyroid hormone
Author: Patricia Tsang, M.D., M.B.A.
Editorial Board Member: Andrey Bychkov, M.D., Ph.D.
Last author update: 23 July 2020
Last staff update: 5 May 2021
Copyright: 2020-2025, PathologyOutlines.com, Inc.
PubMed Search: Parathyroid hormone pathology[title]

Table of Contents
Definition / general | Essential features | Pathophysiology | Diagrams / tables | Clinical features | Laboratory | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Tsang P. Parathyroid hormone. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/chemistryPTH.html. Accessed April 2nd, 2025.
Definition / general
- Hormone secreted by parathyroid glands for maintaining blood calcium homeostasis
- Has reciprocal effect on phosphate metabolism
- Its release controlled by ionized calcium level with negative feedback system
- 84 amino acids derived from cleavage of prepro parathyroid hormone (PTH); biologic activity due to 34 amino acids at amino terminus; other portions are inert but may give false positives in detection systems
- Binding of PTH to its receptor stimulates cAMP and phosphatidylinositol diphosphate
- Note: PTH related protein is rarely produced by benign lesions (Am J Clin Pathol 1996;105:487)
Essential features
- Maintains serum calcium within a tight range of around 9 - 10 mg/dL
- Mobilizes calcium from bone, increases calcium reabsorption from the kidney and stimulates calcium absorption from the gut (Compr Physiol 2016;6:561)
- Primary hyperparathyroidism leads to elevated PTH, elevated blood calcium and reduced blood phosphate; managed most commonly by parathyroidectomy
- Intraoperative rapid PTH assays are useful as an indicator for successful surgical removal of the PTH hypersecreting parathyroid tissue
- Both second and third generation PTH assays measure 1-84 full length intact PTH protein
- Third generation assays are more specific and do not target truncated protein fragments
- While second and third generation assays tend to correlate well (correlation coefficient close to 1.0), third generation assays may generate significantly lower absolute PTH values (Metabolism 2013;62:1416)
Pathophysiology
- PTH maintains serum calcium homeostasis by exerting the following biological effects:
- Activates and increases the number of osteoclasts, mobilizing calcium from bone
- Increases renal tubular reabsorption of calcium
- Activates 1-alpha-hydroxylase, which increases conversion of inactive vitamin D to the active dihydroxy form in kidneys
- Active form of vitamin D promotes GI calcium absorption
- Increases urinary phosphate excretion, which reduces calcium loss
- Reference: Front Horm Res 2018;50:1
Diagrams / tables
Images hosted on other servers:
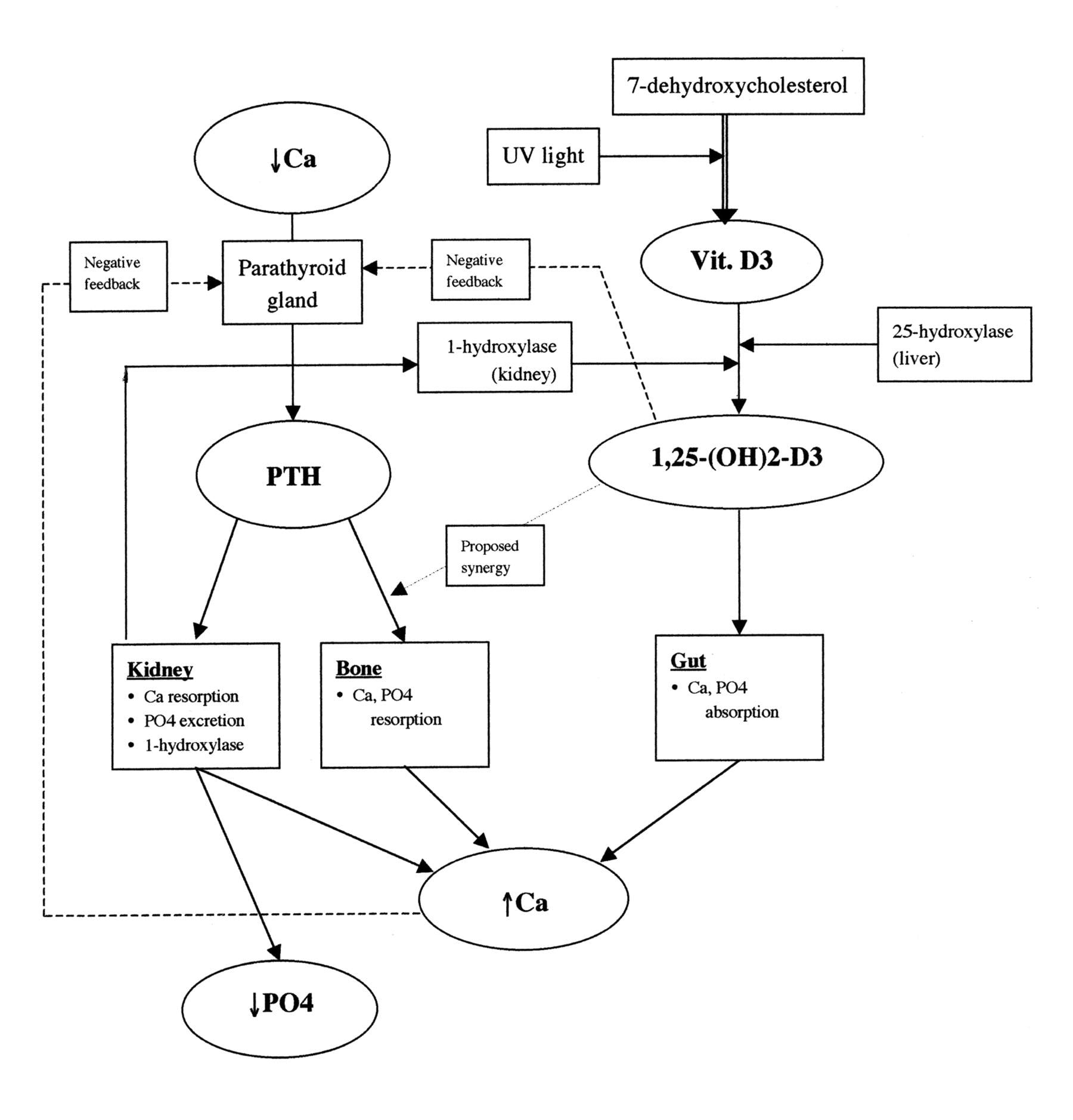
Biologic effects of PTH and
vitamin D on calcium and
phosphate metabolism
Clinical features
- Primary hyperparathyroidism
- Relatively common endocrine disorder (up to 80 per 100,000) caused by overactive parathyroid glands
- 80% single adenoma, 10 - 15% hyperplasia, 5% multiple adenomas (Nat Rev Endocrinol 2018;14:115)
- Presents with elevated circulating PTH, hypercalcemia and hypophosphatemia
- Can lead to osteoporosis, bone fractures, hypercalciuria and nephrolithiasis (Best Pract Res Clin Rheumatol 2020;101514)
- Managed with parathyroidectomy that leads to rapid decline in PTH level
- Intraoperative rapid PTH assay: certain assays enable results in less than 20 minutes (Endocr Pract 2011;17:2)
- Short half life of PTH (2 - 5 minutes) provides sensitive indication of successful removal of hypersecreting parathyroid gland(s)
- Serial intraoperative PTH levels for trending are a common practice
- Secondary hyperparathyroidism
- Common complication of chronic renal disease that can lead to reduced vitamin D production
- Low serum calcium or elevated phosphate leads to parathyroid hyperplasia and elevated circulating PTH (Ther Apher Dial 2019;23:309)
- Elevated PTH can result in abnormal bone turnover (renal osteodystrophy)
- Tertiary hyperparathyroidism
- Most common in patients with chronic secondary hyperparathyroidism who have been on dialysis for years
- Observed in 1 - 3% of patients with renal failure (Am J Otolaryngol 2017;38:630)
- Hypertrophied parathyroid glands oversecrete PTH in an autonomic fashion despite resolution of the underlying condition (e.g. renal transplant)
- Resulting hypercalcemia and hyperphosphatemia can lead to diffuse calcinosis
- Hypoparathyroidism
- Relatively rare heterogeneous condition characterized by insufficient circulating PTH (Expert Opin Drug Saf 2017;16:617)
- Leads to hypocalcemia and hyperphosphatemia
- Treated by vitamin D (inactive and active) and oral calcium tablets
- Hypercalcemia of malignancy (breast, lung, kidney, myeloma) due to:
- Release of PTH related protein, usually in advanced disease (squamous cell carcinoma, lung cancer, hepatoma) or
- Osteolytic metastases with local release of cytokines (IL1, TNF alpha) (multiple myeloma, breast cancer, renal cell carcinoma)
Laboratory
- Second generation (intact PTH) assays widely used today
- However, the intact assay also detects N truncated fragments (e.g. 7-84 PTH) that may exert effects opposite to those of full length 1-84 PTH
- Different assays measure varying types and amounts of these circulating fragments, which can lead to inconsistent results among platforms (National Kidney Foundation: Parathyroid Hormone and Secondary Hyperparathyroidism in Chronic Kidney Disease [Accessed 15 July 2020])
- Third generation PTH assay specifically targets 1-84 PTH without detecting 7-84 PTH and other fragments (Clin Chem Lab Med 2018;56:1476)
- May potentially enable better standardization of PTH values across platforms than second generation assays
- Values tends to be numerically lower than those from second generation assays
- Close communication with clinicians warranted when changing assays between generations
- Primary hyperparathyroidism
- Type of PTH assay used will not affect diagnosis or management because the precise concentration of PTH is less relevant (Endocr Rev 2019;40:1468)
- Secondary hyperparathyroidism due to chronic kidney disease
- Clinical guideline recommends maintaining PTH level at twofold to ninefold above the upper limit of normal, corresponding to about 130 - 600 pg/mL (depending on assay platform used) (National Kidney Foundation: Parathyroid Hormone and Secondary Hyperparathyroidism in Chronic Kidney Disease [Accessed 15 July 2020])
- Intraoperative rapid PTH assay
- Third generation assays can provide a faster indication of treatment success than second generation assays (Surgery 2020 [Epub ahead of print])
Board review style question #1
Which of the following sets of laboratory values is characteristic of primary hyperparathyroidism?
- Elevated blood PTH, elevated calcium, elevated phosphate
- Elevated blood PTH, reduced calcium, elevated phosphate
- Elevated blood PTH, elevated calcium, reduced phosphate
- Elevated blood PTH, reduced calcium, reduced phosphate
Board review style answer #1
C. In primary hyperparathyroidism, the elevated blood PTH physiologically increases serum calcium and reciprocally reduces serum phosphate.
Comment Here
Reference: Parathyroid hormone
Comment Here
Reference: Parathyroid hormone
Board review style question #2
Which of the following describes the difference between second generation and third generation PTH assays?
- Second generation PTH assays detect the 1-84 intact PTH protein in addition to the N truncated 7-84 fragment, while the third generation assays detect only the 1-84 intact PTH
- PTH values are numerically interchangeable between second generation and third generation assays
- Second generation PTH assays provide faster results as compared to third generation assays for intraoperative PTH evaluation
- Third generation PTH assays are more comprehensive than second generation assays by detecting more circulating PTH fragments
Board review style answer #2
A. Third generation PTH assays do not detect 7-84 PTH and other fragments, which second generation assays typically do.
Comment Here
Reference: Parathyroid hormone
Comment Here
Reference: Parathyroid hormone
