

Cervix
Other epithelial tumors
Small cell neuroendocrine carcinoma
Last author update: 1 May 2007
Last staff update: 11 September 2023
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: Small cell carcinoma [title] cervix




Table of Contents
Definition / general | Terminology | Epidemiology | Pathophysiology | Clinical features | Prognostic factors | Case reports | Treatment | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Cytology images | Positive stains | Negative stains | Electron microscopy description | Molecular / cytogenetics description | Differential diagnosis | Additional referencesCite this page: Perunovic B, Sunassee A. Small cell neuroendocrine carcinoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/cervixsmallcell.html. Accessed December 24th, 2024.
Definition / general
- Rare (1 - 5% of invasive cervical carcinomas)
- Clinically aggressive with rapid metastases and poor prognosis
Terminology
- Amphicrine carcinoma: small cell carcinoma combined with squamous cell carcinoma or adenocarcinoma
Epidemiology
- Women ages 25 to 87 years (median ~42 years)
- Associated with HPV 18 (Am J Surg Pathol 1991;15:28)
Pathophysiology
- Coexisting SIL is rare; endocrine cell hyperplasia may be a precursor lesion
- HPV 18 > HPV 16
Clinical features
- Vaginal bleeding, post-coital spotting, lower abdominal pain (J Clin Diagn Res 2014;8:147)
- Cervical mass / bulkiness
- Frequently presents with parametrial invasion and pelvic lymph node metastases
- Paraneoplastic syndromes include Cushing syndrome, carcinoid syndrome, SIADH, hypoglycemia (Cytojournal 2013;10:17)
- Mostly pure form, but may coexist with cervical squamous cell carcinoma or adenocarcinoma (Cytojournal 2013;10:17)
- May develop after a negative Pap test to an advanced stage between screenings (Case Rep Pathol 2014;2014:971464)
- 5 year survival is 30 - 40%; relapse in 2/3 at median 8 months (Gynecol Oncol 2004;93:27), poor prognostic factors are smoking and high stage (Cancer 2003;97:568), focal glandular differentiation does not affect prognosis
Prognostic factors
- FIGO stage at presentation, age at diagnosis, deep stromal invasion, clinical stage (nodal and hematogenous metastasis), baseline state of health (Case Rep Pathol 2014;2014:971464, Gynecol Oncol 2014;134:410, Int J Gynecol Cancer 2014;24:272, Eur J Gynaecol Oncol 2012;33:68)
Case reports
- 27 year old woman with amphicrine carcinoma (Am J Clin Pathol 1992;97:516)
- 27 year old woman with 6 cm cervical mass (Case of the Week #327)
- 27 year old woman with rapidly growing cervical polyp during pregnancy (Gynecol Oncol 2001;81:117)
- 59 year old woman with syndrome of inappropriate antidiuretic syndrome (Mod Pathol 1996;9:397)
- 70 year old woman with G - CSF producing tumor (Diagn Cytopathol 2000;23:269)
Treatment
- Radical hysterectomy with bilateral lymphadenectomy, radiation therapy and chemotherapy
Gross description
- Erythematous cervix, often barrel shaped, with small exophytic mass
- May be ulcerative and infiltrative
Microscopic (histologic) description
- Loose aggregates of uniform small cells with indistinct cell borders, scant cytoplasm, hyperchromatic nuclei with fine granular chromatin, nuclear molding, indistinct nucleoli, extensive mitotic activity, single cell necrosis
- May form sheets with small acini resembling rosettes
- Necrosis common
- Vascular invasion in 9%
- Resembles counterpart in lung
- Patterns include insular (solid nests / islands of cells with peripheral palisading and retraction of stroma), perivascular and thick trabeculae with serpiginous (wavy) growth
- Variable amyloid deposition
- May have minor (< 10%) component of glandular or squamous differentiation
- Often no associated inflammation
Microscopic (histologic) images
AFIP and Case #327
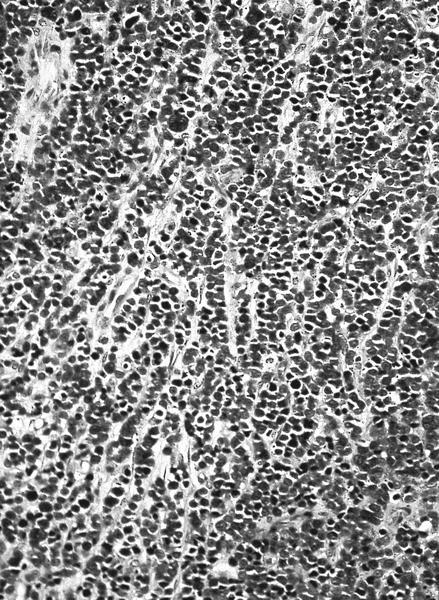
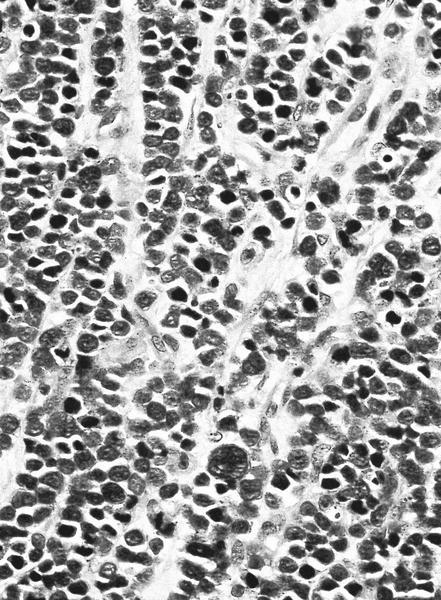
Sheets of small cells with scant cytoplasm and hyperchromatic nuclei
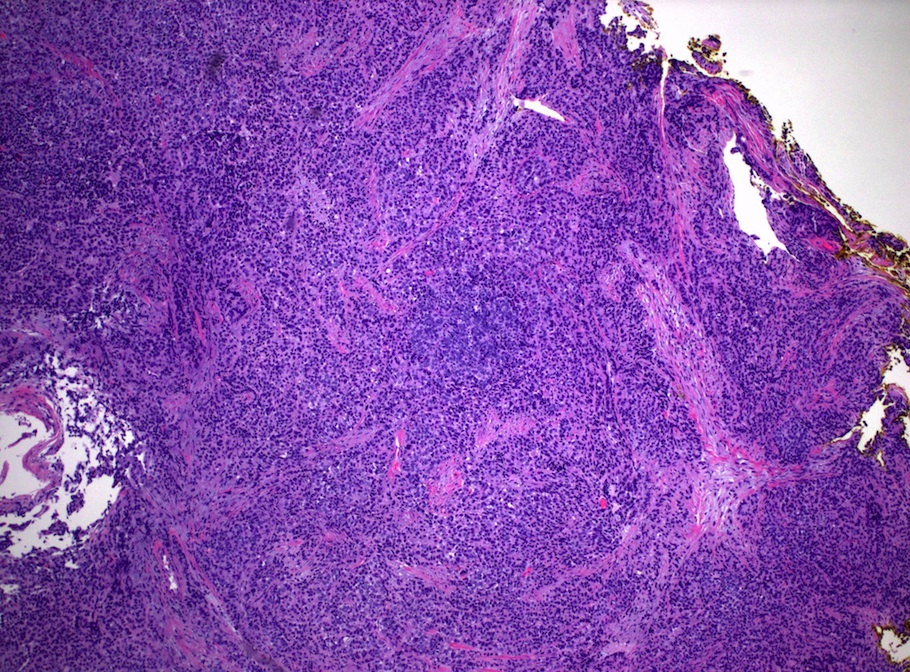
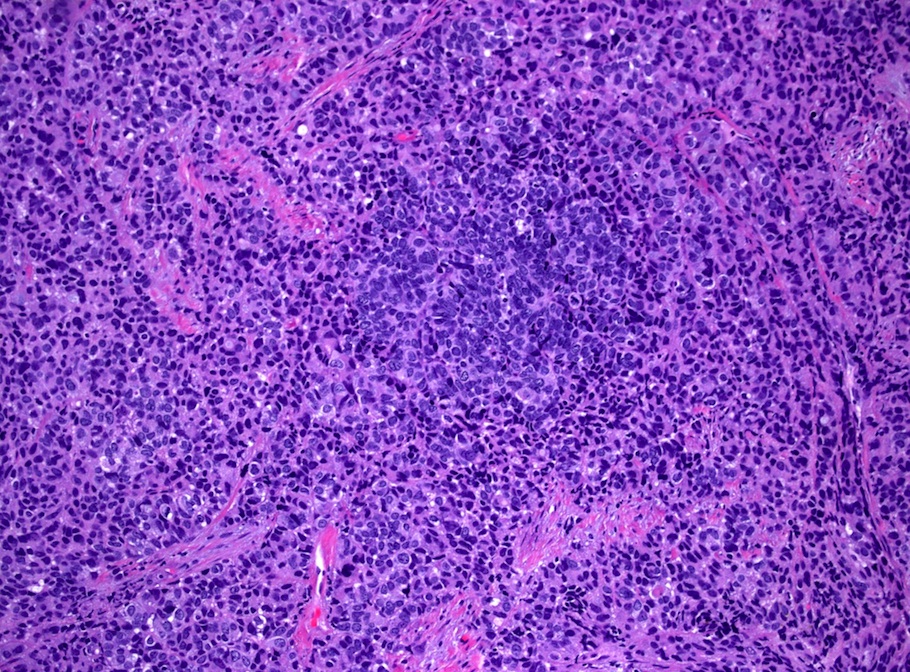
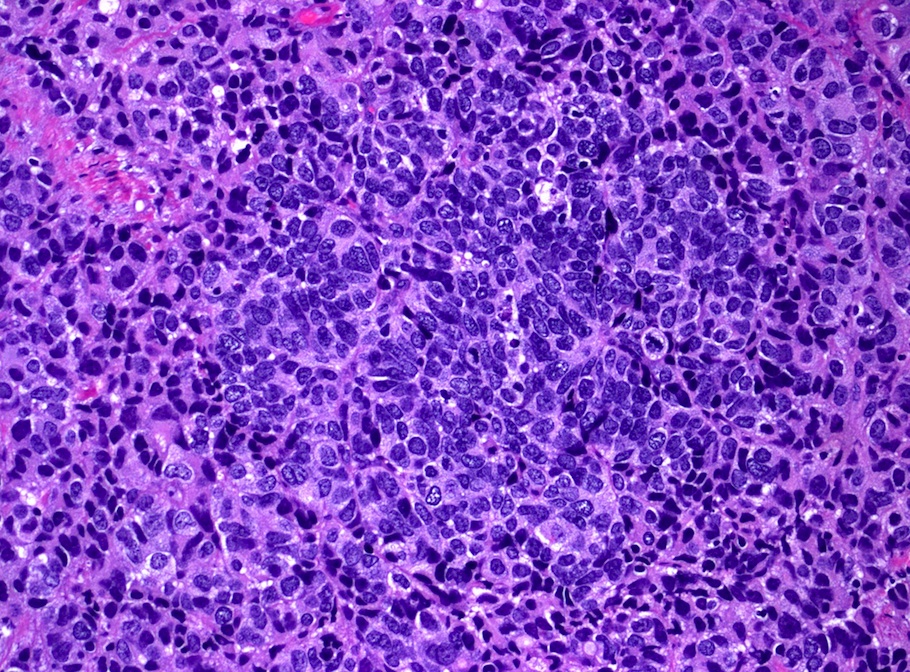
H&E
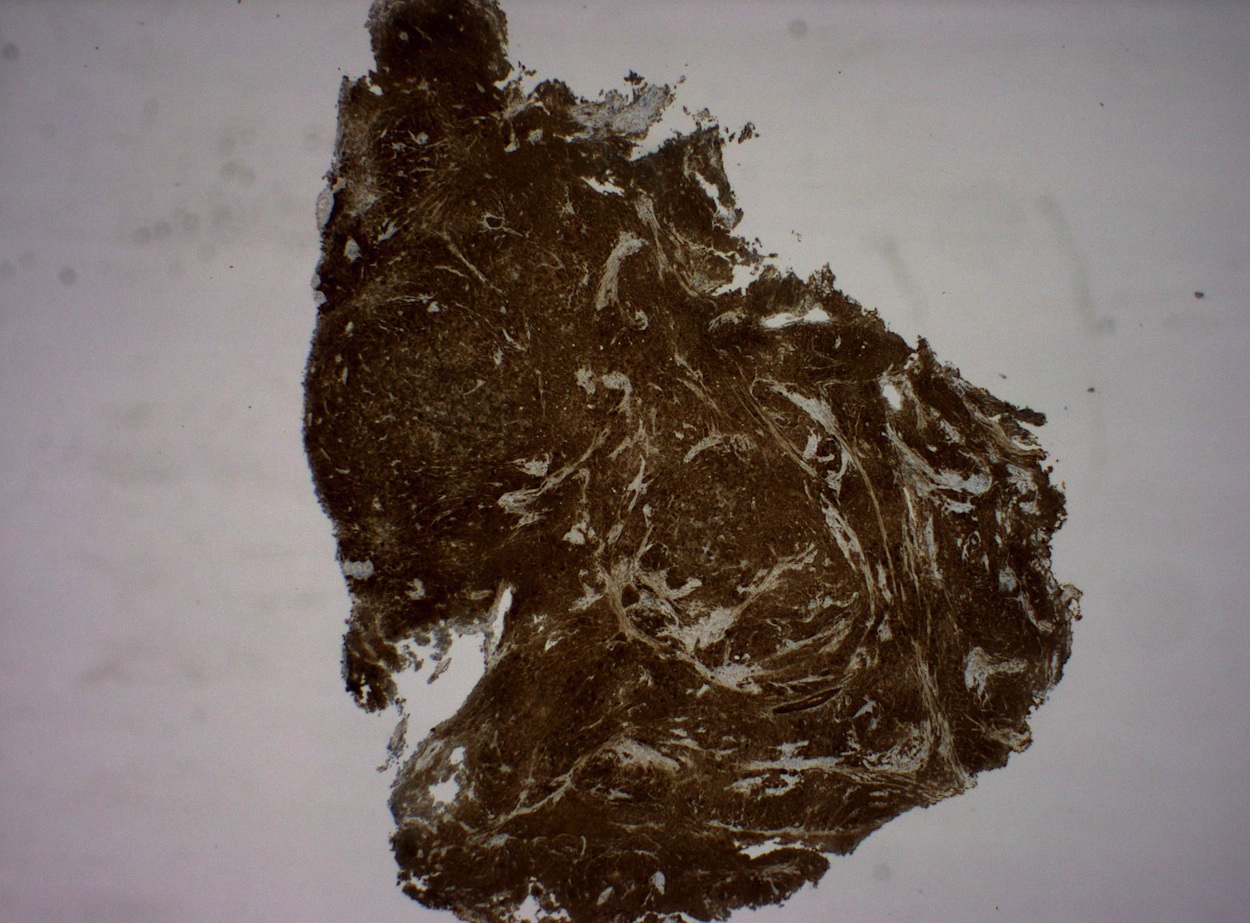
CK7
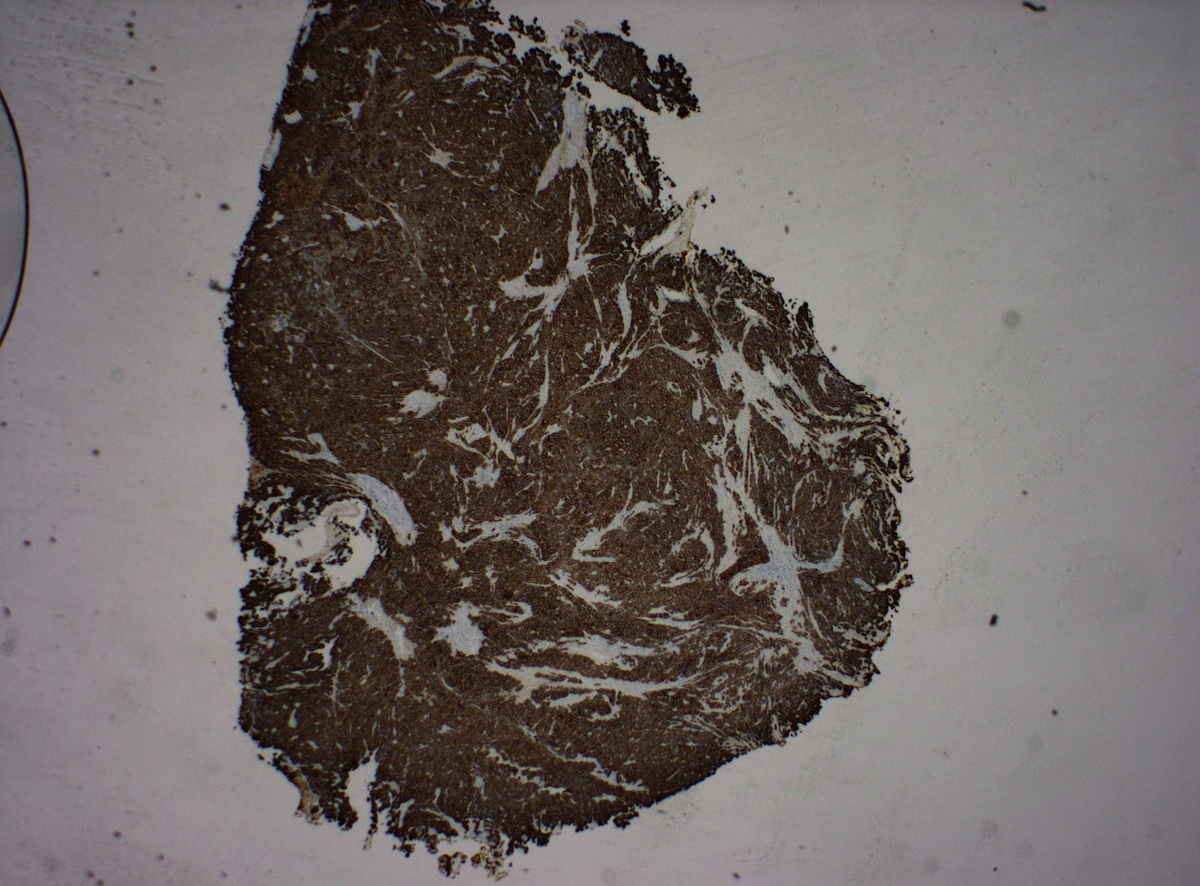
p16
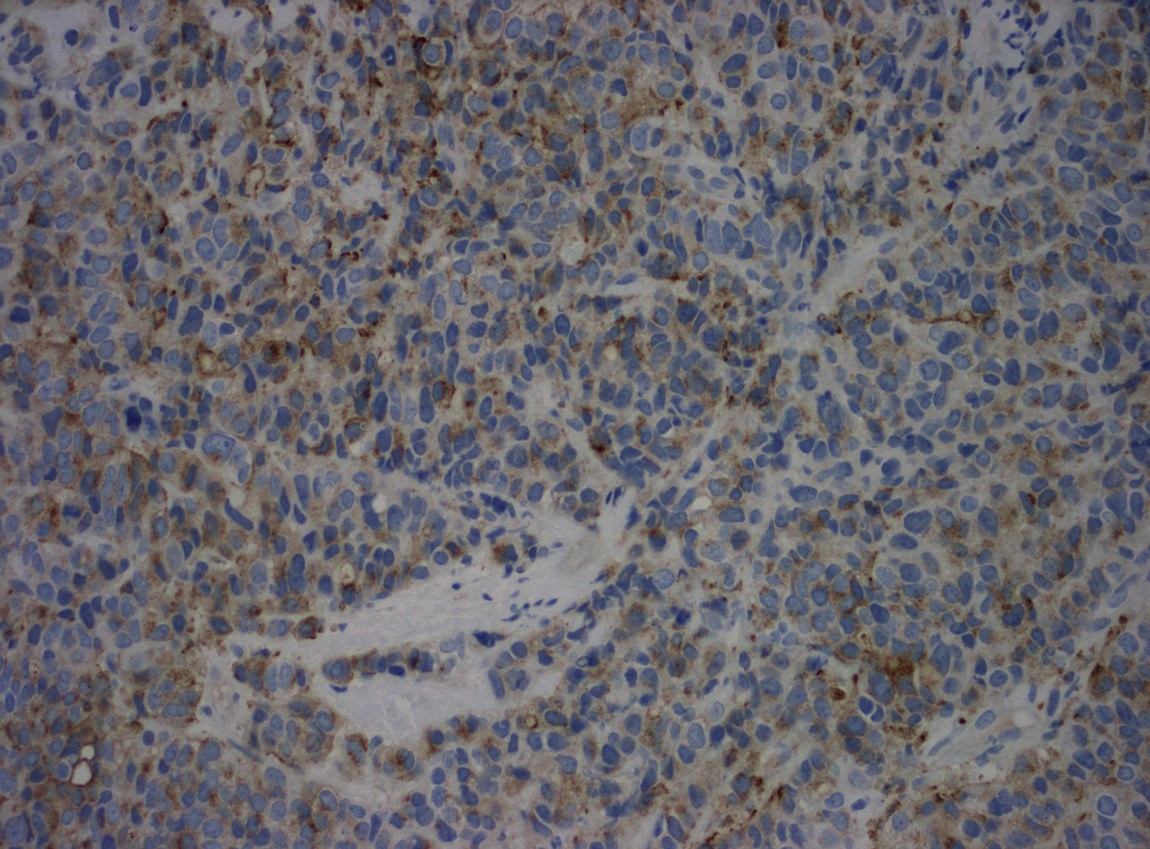
Chromogranin
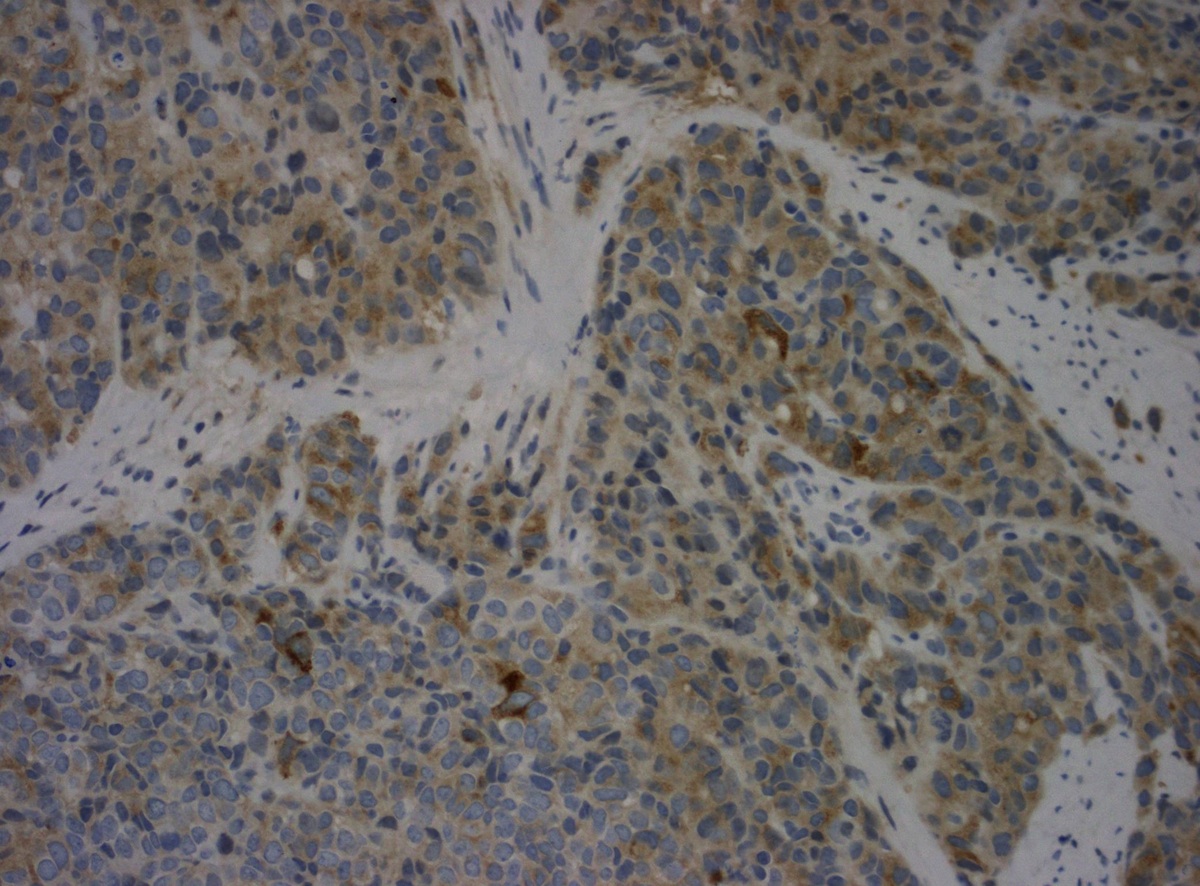
Synaptophysin
Cytology description
- Pap slides are usually moderately to highly cellular
- Cells appear in loosely cohesive multidimensional aggregates and sheets as well as single and dispersed
- Cells are monotonous in size (approximately 2x intermediate squamous cell nuclei) (Case Rep Pathol 2014;2014:971464)
- Very high nuclear/cytoplasmic ratios with delicate rims of amphophilic cytoplasm
- Nuclei have finely granular/stippled chromatin, with nuclear molding and smear artifact
- Mitotic figures common
- Background is mostly clear but may have granular proteinaceous diathesis material (clinging diathesis) and apoptotic degenerated single tumor cells (Case Rep Pathol 2014;2014:971464, Acta Cytol 1998;42:978, Acta Cytol 2003;47:56, Diagn Cytopathol 2001;24:46)
Cytology images
Images hosted on other servers:

Lesional cells, Pap

Single necrotic cells, Pap

Amphophilic cytoplasm

Large aggregates of malignant cells

Malignant cells loosely cohesive

Scant cytoplasm

PanCK

Synaptophysin

p16
Positive stains
- Note: small cell carcinoma is a morphologic diagnosis regardless of stain results
- CD56 is sensitive but not specific (Int J Gynecol Pathol 2005;24:113)
- Variable TTF1
Negative stains
Electron microscopy description
- Cells are tightly packed with close apposition of cell membranes
- Dense core secretory granules
Molecular / cytogenetics description
- Frequent loss of heterozygosity at 3p and 11p
Differential diagnosis
- Three specific cytomorphological criteria are the most reliable features for separating small cell from non-small cell carcinoma:
- Nuclear molding
- Finely granular "salt and pepper" chromatin
- Scant delicate cytoplasm
- Follicular cervicitis: reactive polymorphous population including lymphocytes in every stage of maturation as well as germinal center macrophages containing phagocytosed cellular debris
- Lymphoma: cells individually scattered and loosely arranged in a dirty background with inflammatory cells; nuclear molding infrequent but high grade lymphoma may have pseudomolding which resembles real molding
- Rhabdomyosarcoma or other small blue cell sarcomas
- Squamous cell carcinoma: tumor cells arranged singly or in syncytial aggregates with smooth cell borders, high N/C ratio, more cytoplasm than small cell carcinoma, coarsely granular hyperchromatic nuclei with irregularly distributed chromatin, nuclear molding not seen
- Small cell squamous cell carcinoma: well defined nests similar to large cell nonkeratinizing squamous cell carcinoma
- Carcinoid tumor
- Metastatic carcinoma: lung or other sites
Additional references

