

Uterus
Smooth muscle tumors
Leiomyosarcoma
Editorial Board Member: Stephanie L. Skala, M.D.
Deputy Editor-in-Chief: Jennifer A. Bennett, M.D.


Last author update: 13 December 2022
Last staff update: 23 May 2023
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed search: Leiomyosarcoma


Table of Contents
Definition / general | Essential features | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Frozen section description | Microscopic (histologic) description | Microscopic (histologic) images | Virtual slides | Positive stains | Negative stains | Molecular / cytogenetics description | Molecular / cytogenetics images | Videos | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Monsrud A, Turashvili G. Leiomyosarcoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/uteruslms.html. Accessed December 24th, 2024.
Definition / general
- Rare, malignant mesenchymal tumor derived from myometrial smooth muscle
- Most common sarcoma of the gynecologic tract
Essential features
- Rare tumor, mostly found in uterine corpus
- 3 subtypes: spindled / conventional (most common), myxoid, epithelioid
- Diagnostic triad: marked cytologic atypia, tumor cell necrosis and increased mitoses (mitotic count depends on subtype)
- Poor prognosis even at low stage (Histopathology 2009;54:355, Curr Probl Cancer 2019;43:283, Asia Pac J Clin Oncol 2020;16:e63)
ICD coding
Epidemiology
- Rare, 3 - 9% of all uterine cancers
- ~70% of uterine sarcomas (Frumovitz: Diagnosis and Treatment of Rare Gynecologic Cancers, 1st Edition, 2022, Lancet Oncol 2009;10:1188)
- Peak incidence is > 50 years old; range of 30 - 70 years (Medicine (Baltimore) 2020;99:e21766)
Sites
- Uterus corpus
- Cervix, rare
Pathophysiology
- Derived from smooth muscle
- Vast array of associated cytogenetic abnormalities but none are consistent or diagnostic
- Most frequently mutated genes: TP53 (~30%), ATRX (~25%) and MED12 (~20%) (Proc Natl Acad Sci U S A 2021;118:e2025182118)
Etiology
- Most patients do not have predisposing risk factors
- Rare associations include:
- Prior pelvic radiation (Arch Gynecol Obstet 2019;300:389, Cancer 1986;58:2003)
- Tamoxifen use for > 5 years (Int J Gynecol Cancer 2008;18:352)
- Very rare cases may arise from a pre-existing leiomyoma (J Minim Invasive Gynecol 2020;27:926, Mod Pathol 2009;22:1303, Int J Gynecol Pathol 2022;41:552)
- Black women have a 2 fold higher risk compared with white women (Br J Cancer 2013;108:727)
- Hereditary retinoblastoma and Li-Fraumeni syndrome are characterized by increased incidence of leiomyosarcoma (Curr Probl Cancer 2019;43:283)
- In one series, increased predisposition reported in Finnish hereditary leiomyomatosis / renal cell carcinoma syndrome kindreds (J Med Genet 2006;43:523)
Clinical features
- Nonspecific symptoms:
- Abnormal uterine bleeding, pelvic or abdominal pain
- Rapidly growing uterine mass in a postmenopausal woman
- Usually an incidental finding, identified in 0.13% of hysterectomies for benign indication and 0.39% of hysterectomies for uterine leiomyomas (Am J Obstet Gynecol 2019;220:179.e1)
Diagnosis
- Myomectomy, hysterectomy
Laboratory
- No laboratory values are diagnostic:
- Some studies suggest leiomyosarcomas have higher levels of lactate dehydrogenase (LDH) versus uterine leiomyoma (BMC Cancer 2020;20:514)
- Variable success as a predictive marker
Radiology description
- No pathognomonic findings
- Difficult to distinguish from benign smooth muscle tumors (Curr Opin Oncol 2021;33:464)
- TVUS:
- Most common initial imaging modality
- Successfully detects uterine leiomyomas
- Does not differentiate between leiomyomas and leiomyosarcomas
- Most common initial imaging modality
- CT: not indicated for assessing uterine masses
- May show irregular central zones of low attenuation, suggesting necrosis and hemorrhage
- MRI, conventional techniques:
- Ill defined borders
- Central nonenhancement
- T1 weighted images with hyperintensity associated with tumoral hemorrhage or necrosis
- T2 weighted images show heterogeneous intermediate to high signal intensities
- Advanced imaging modalities show potential diagnostic improvement:
- Machine learning
- Radiomics
- Texture analysis (Jpn J Radiol 2022;40:385)
Radiology images
Images hosted on other servers:

Large intrauterine mass

Heterogeneous mass with irregular borders
Prognostic factors
- Most important prognostic factor is stage
- Additional prognostic measures include age, tumor size, mitotic rate and lymphovascular invasion
- High recurrence rate (50 - 70%) regardless of stage at initial diagnosis
- Poor prognosis even if the tumor is confined to the uterus
- More favorable prognosis if tumor is < 5 cm and confined to the uterus
- 5 year overall survival (OS) rate for all stages is poor, ranging from 15 to 25%
- OS rates are more favorable at low stages (1 - 2), ranging from 40 to 70%
- Morcellation is associated with significantly increased risk of recurrence (Gynecol Oncol 2021;160:99)
- Risk stratification model, including mitoses > 25 per 2.4 mm2 (10 high power fields), atypical mitoses, coagulative necrosis, lymphovascular invasion and serosal abutment, is significantly associated with disease free and disease specific survival in stage I tumors (Mod Pathol 2022;35:794):
- 3 risk groups include low risk (0- 2 points), intermediate risk (3 - 5 points) and high risk (6 - 13 points)
- Serosal abutment and lymphovascular invasion can be omitted for myomectomy or morcellated specimens
Case reports
- 46 year old hemodynamically unstable woman with fever (Cureus 2020;12:e11586)
- 51 year old woman with metastatic leiomyosarcoma to the breast (Case Rep Pathol 2020;2020:8037646)
- 53 year old woman with diffuse abdominal pain and abnormal vaginal bleeding (Clin Pathol 2022;15:2632010X221105224)
- 59 year old woman with microsatellite instability high uterine leiomyosarcoma (Gynecol Oncol Rep 2021;35:100701)
- 68 year old woman with uterine myxoid leiomyosarcoma (Rom J Morphol Embryol 2021;62:883)
Treatment
- Surgical resection (hysterectomy) is standard treatment for patients with localized leiomyosarcoma:
- Adjuvant chemotherapy for early stage disease is controversial
- Bilateral salpingo-oophorectomy is reasonable in peri and postmenopausal patients
- Lymphadenectomy is only indicated if there is evidence of concerning lymph nodes (J Adv Pract Oncol 2022;13:70, StatPearls: Leiomyosarcoma [Accessed 26 October 2022])
- Radiotherapy is indicated for palliative care purposes in advanced or metastatic disease (Cancer Med 2022;11:2906):
- No evidence for increased overall survival
- Adjuvant chemotherapy is indicated for metastatic / recurrent tumors
- Immunotherapy is a potential option for MSI high uterine leiomyosarcoma (Gynecol Oncol Rep 2021;35:100701)
- Hormonal therapy may be an option in hormone receptor positive tumors
Clinical images
Images hosted on other servers:

Uterus with dilated cervix

Large exophytic intrauterine mass

Large mass
Gross description
- Often a solitary, bulky, fleshy mass within the myometrium - intramural (majority), submucosal, subserosal or pedunculated:
- Hemorrhagic, necrotic and cystic areas upon sectioning
- Grossly invasive / infiltrative
- Rarely may arise in the cervix (5%)
- Average diameter is 10 cm:
- ~25% are < 5 cm
- Myxoid leiomyosarcoma:
- Gelatinous cut surface
- Friable
- References: Oncol Res Treat 2018;41:680, Arch Pathol Lab Med 2008;132:595
Gross images
Contributed by Ashley Monsrud, M.D.
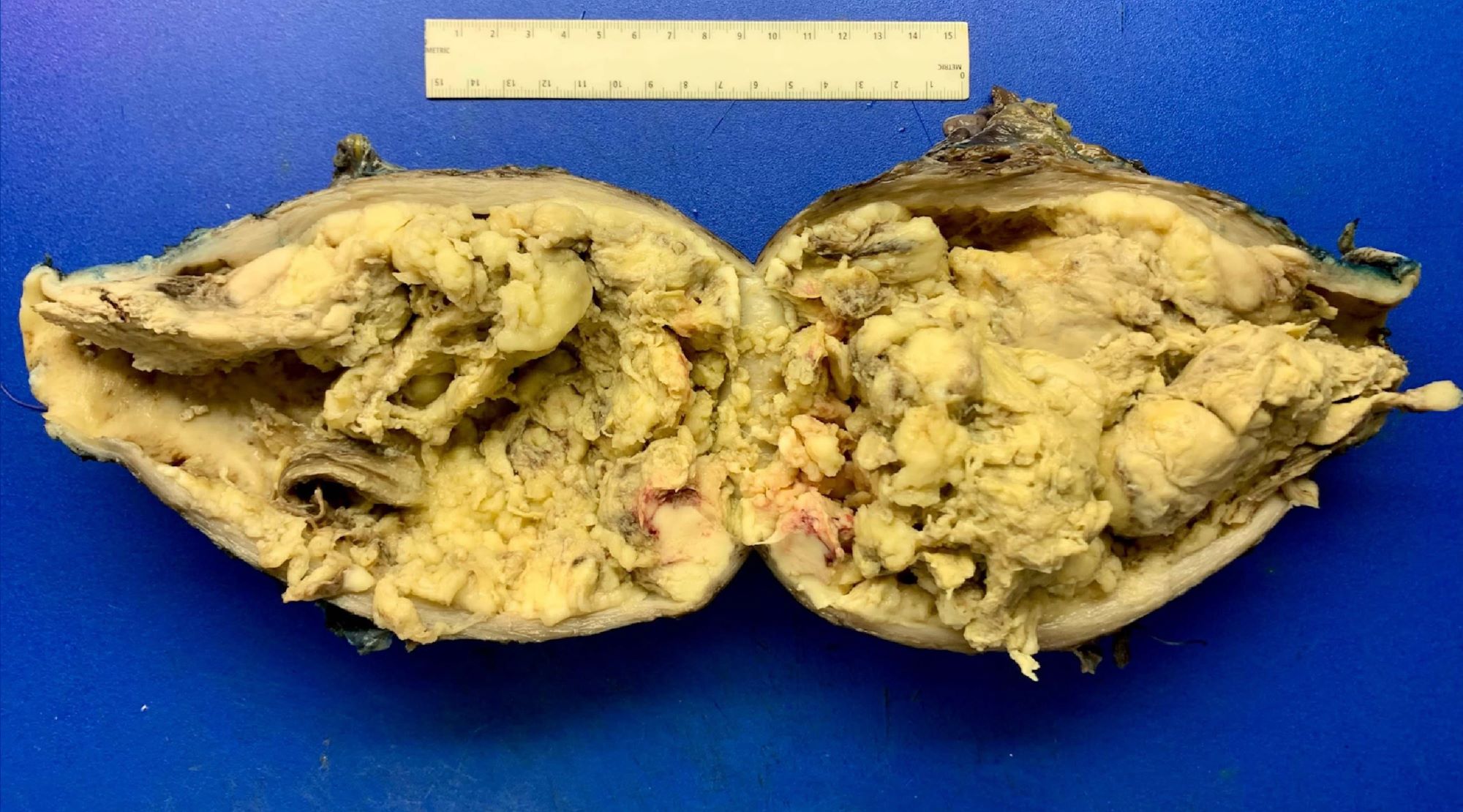
Formalin fixed, intracavitary leiomyosarcoma
Images hosted on other servers:

Large mass
Frozen section description
- Not usually performed
- If done, assess:
- Cellularity
- Significant cytologic atypia
- Number of unequivocal mitotic figures
- Tumor cell necrosis:
- Karyorrhexis, perivascular cuffs of viable tumor cells in a background of necrosis and ghost cells are diagnostic clues for tumor cell necrosis (Am J Surg Pathol 2021;45:1179)
- If malignant criteria are met:
- Best practice is to call "malignant mesenchymal tumor”
Microscopic (histologic) description
- Conventional / spindle cell type:
- Essential diagnostic criteria:
- Requires 2 of 3 histologic features:
- Marked cytologic atypia
- ≥ 10 mitoses / 10 high power fields
- Tumor cell necrosis
- Identified by abrupt transition from viable tumor cells to necrotic cells (ghost cells, apoptotic bodies may be seen)
- Granulation tissue surrounding necrosis is absent
- Requires 2 of 3 histologic features:
- Growth pattern:
- Cellular tumor comprised of long intersecting or haphazard fascicles
- Infiltrative border (common)
- Rarely, may arise from background leiomyoma
- Cytologic features:
- Spindle / elongated cells
- Eosinophilic cytoplasm
- Hyperchromatic nuclei often with moderate to severe nuclear pleomorphism (can be deceptively bland and uniform)
- Atypical mitoses are frequently identified
- Multinucleated and osteoclast-like giant cells may be seen
- Essential diagnostic criteria:
- Myxoid leiomyosarcoma:
- Diagnosis based on ≥ 1 of the following:
- Moderate to severe cytologic atypia
- Coagulative tumor cell necrosis
- ≥ 2 mitosis / 10 high power fields
- Infiltrative borders / irregular margins
- Growth pattern:
- Hypocellular tumor with abundant myxoid stroma
- Fascicular or nodular patterns are uncommon
- Myxoid stroma may be difficult to differentiate from hydropic change in small / limited samples
- Extensive sampling is generally required for diagnosis
- Diagnosis based on ≥ 1 of the following:
- Epithelioid leiomyosarcoma:
- Diagnosis based on ≥ 1 of the following:
- Moderate to severe cytologic atypia
- Tumor cell necrosis
- ≥ 4 mitoses / 10 high power fields
- Growth pattern:
- Arranged in nests, cords or sheets
- May show pseudoglandular spaces
- Cytologic features:
- > 50% of round or polygonal cells with eosinophilic or clear cytoplasm
- Rarely, extensive hyalinization
- Alternative criteria include ≥ 2 of the following features: moderate or severe atypia, ≥ 4 mitoses / 2.4 mm2 and tumor cell necrosis (Am J Surg Pathol 2022;46:464)
- Diagnosis based on ≥ 1 of the following:
- Classification systems used:
- FIGO
- TNM
- References: Arch Pathol Lab Med 2008;132:595, StatPearls: Leiomyosarcoma [Accessed 26 October 2022]
Microscopic (histologic) images
Contributed by Ashley Monsrud, M.D. and Paulette Mhawech-Fauceglia, M.D.
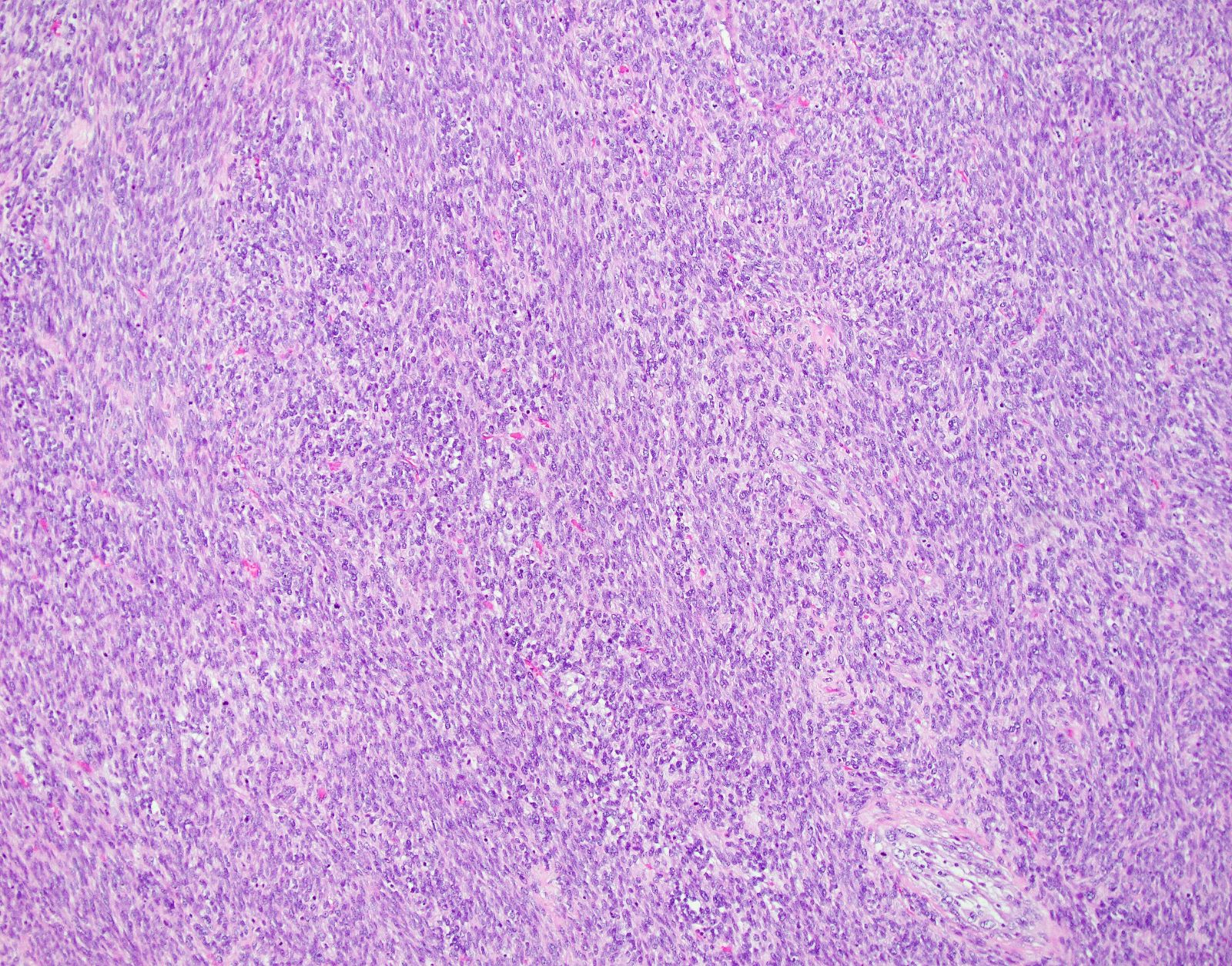

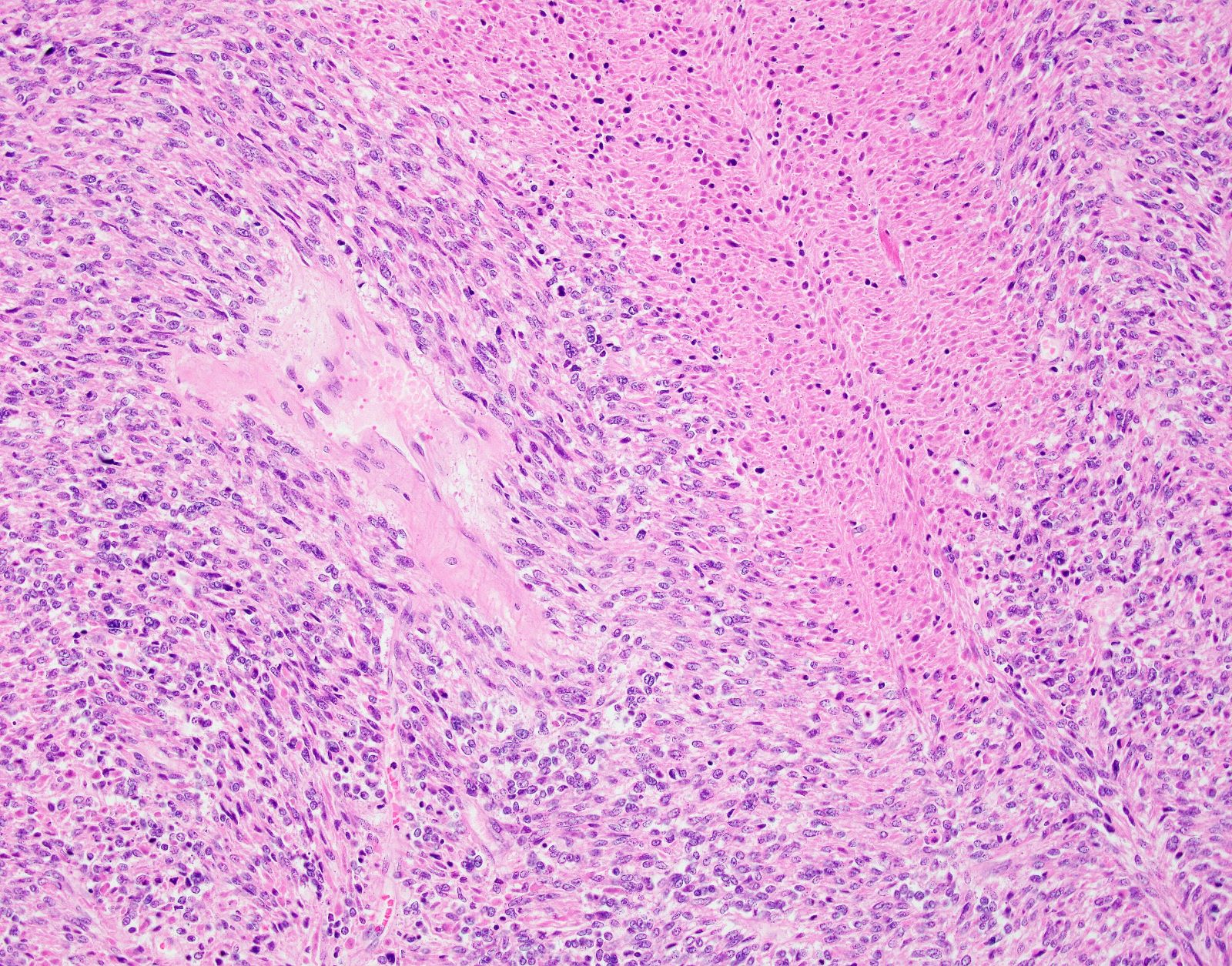
Spindle cell leiomyosarcoma
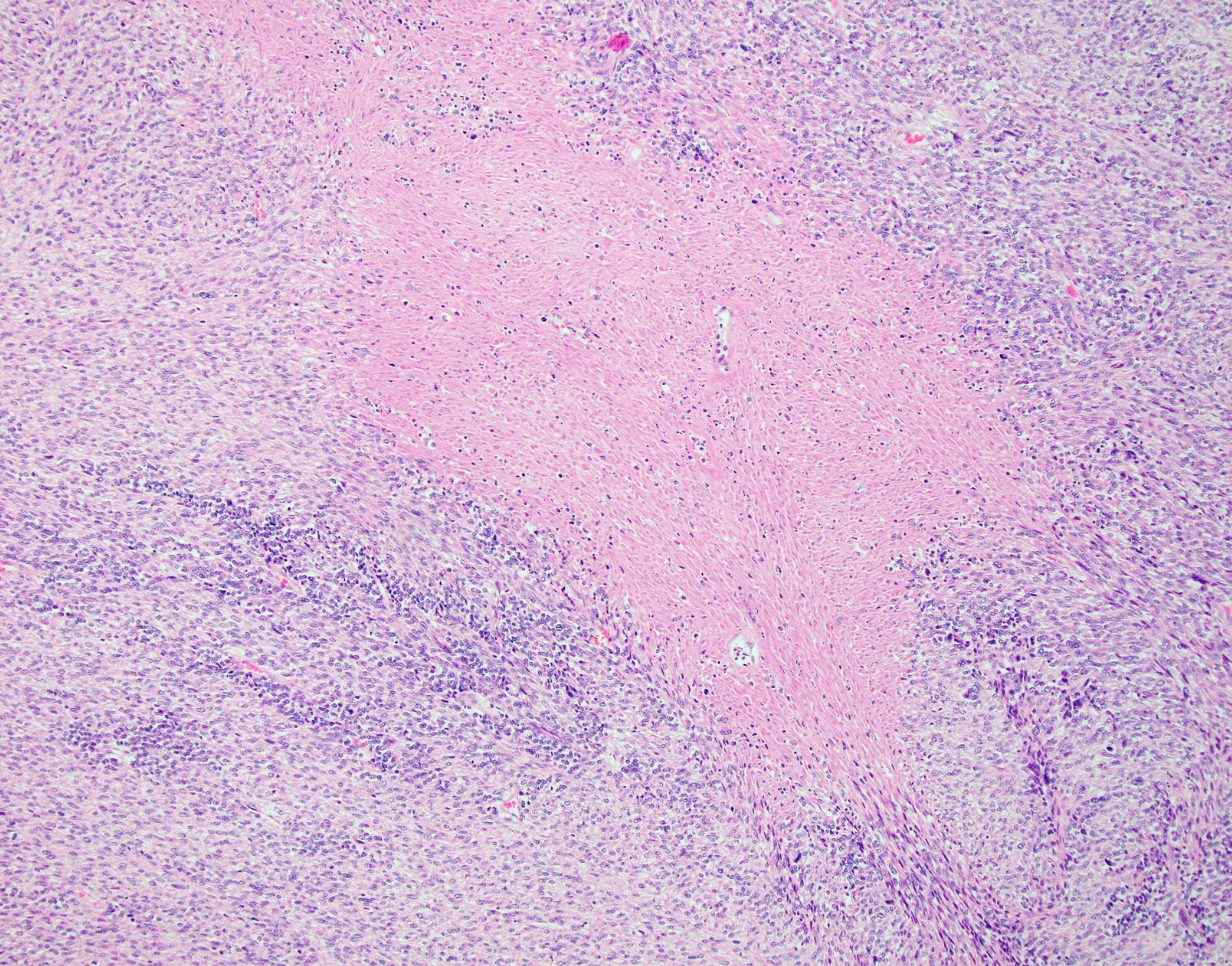
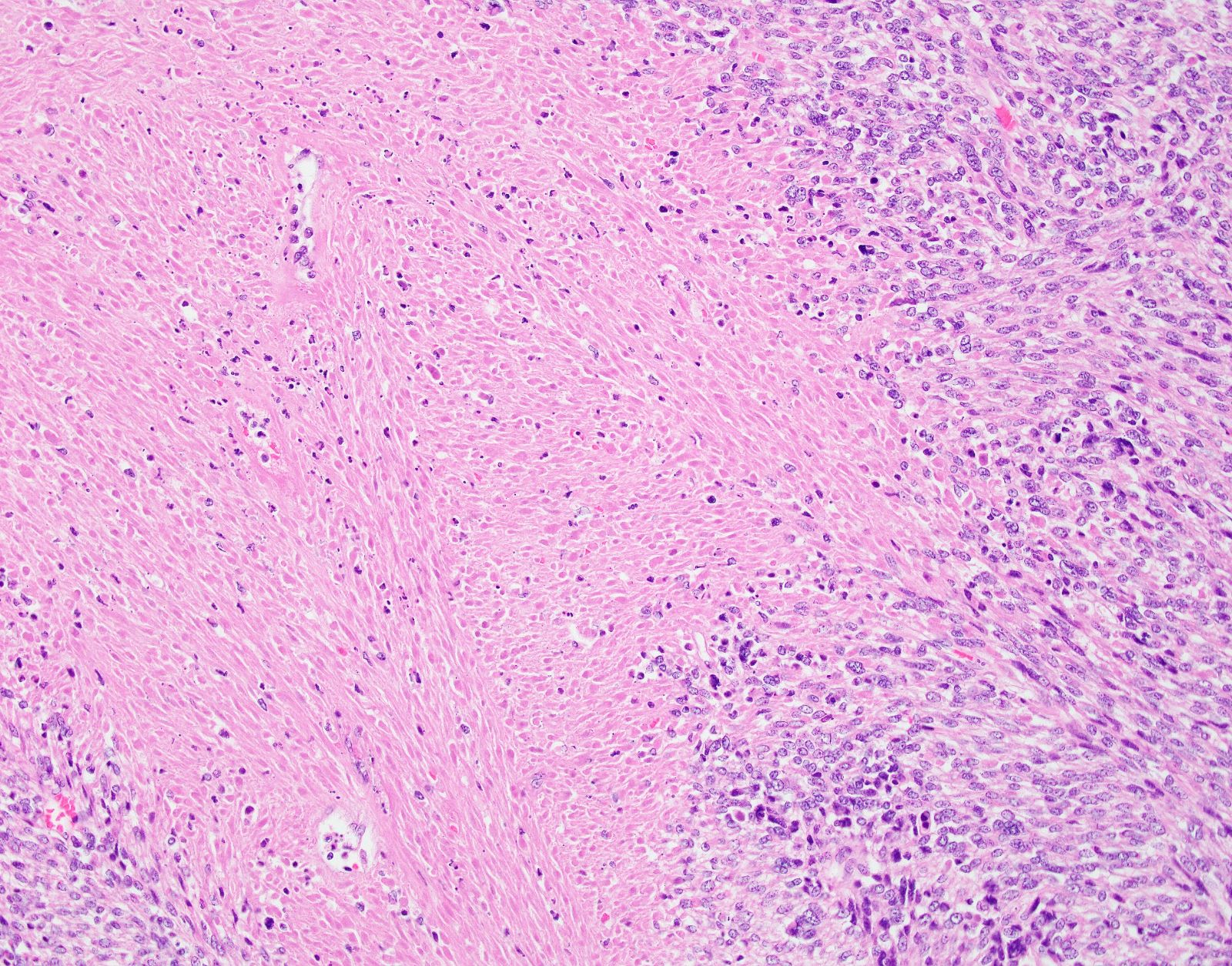
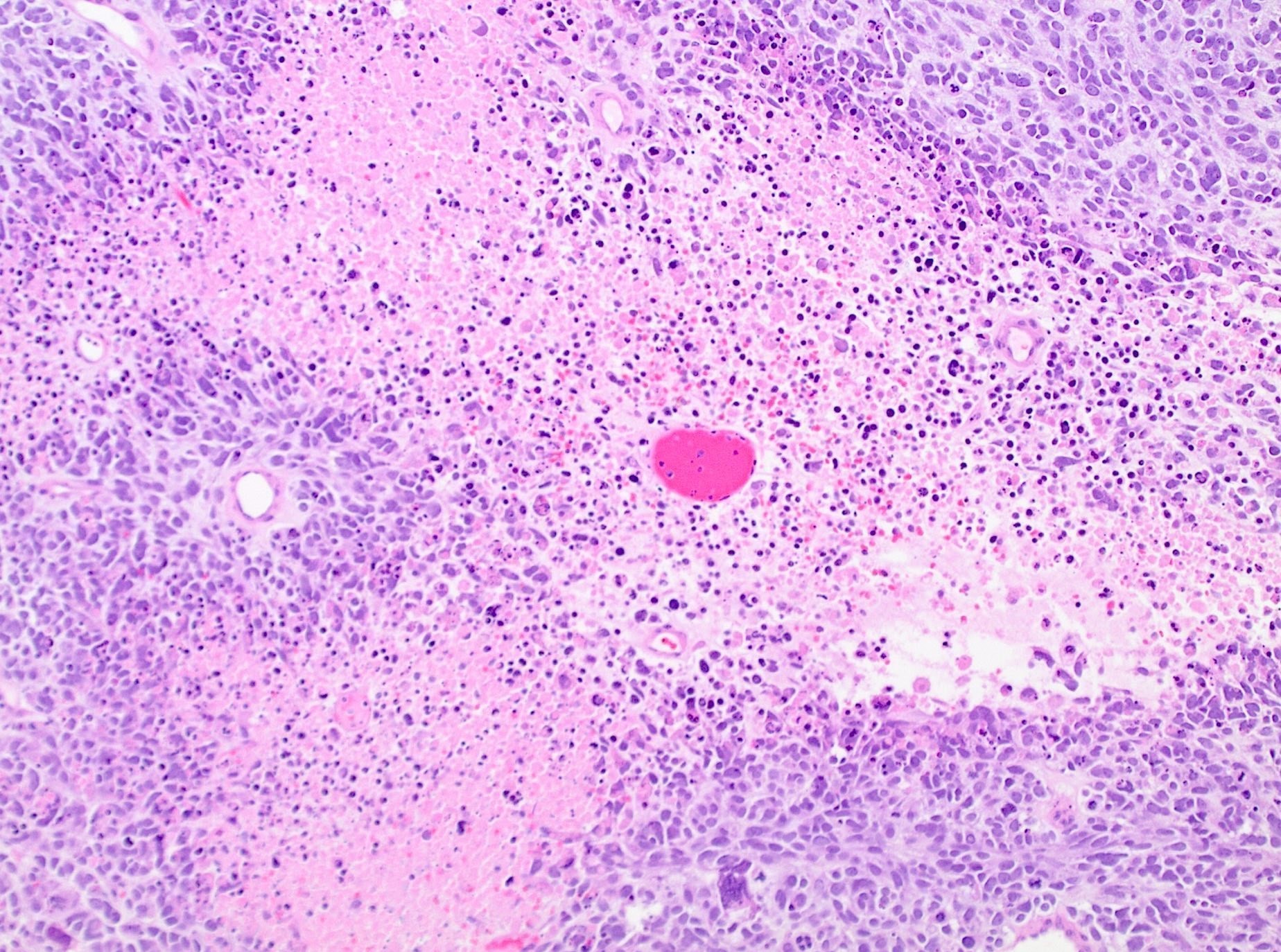
Tumor cell necrosis
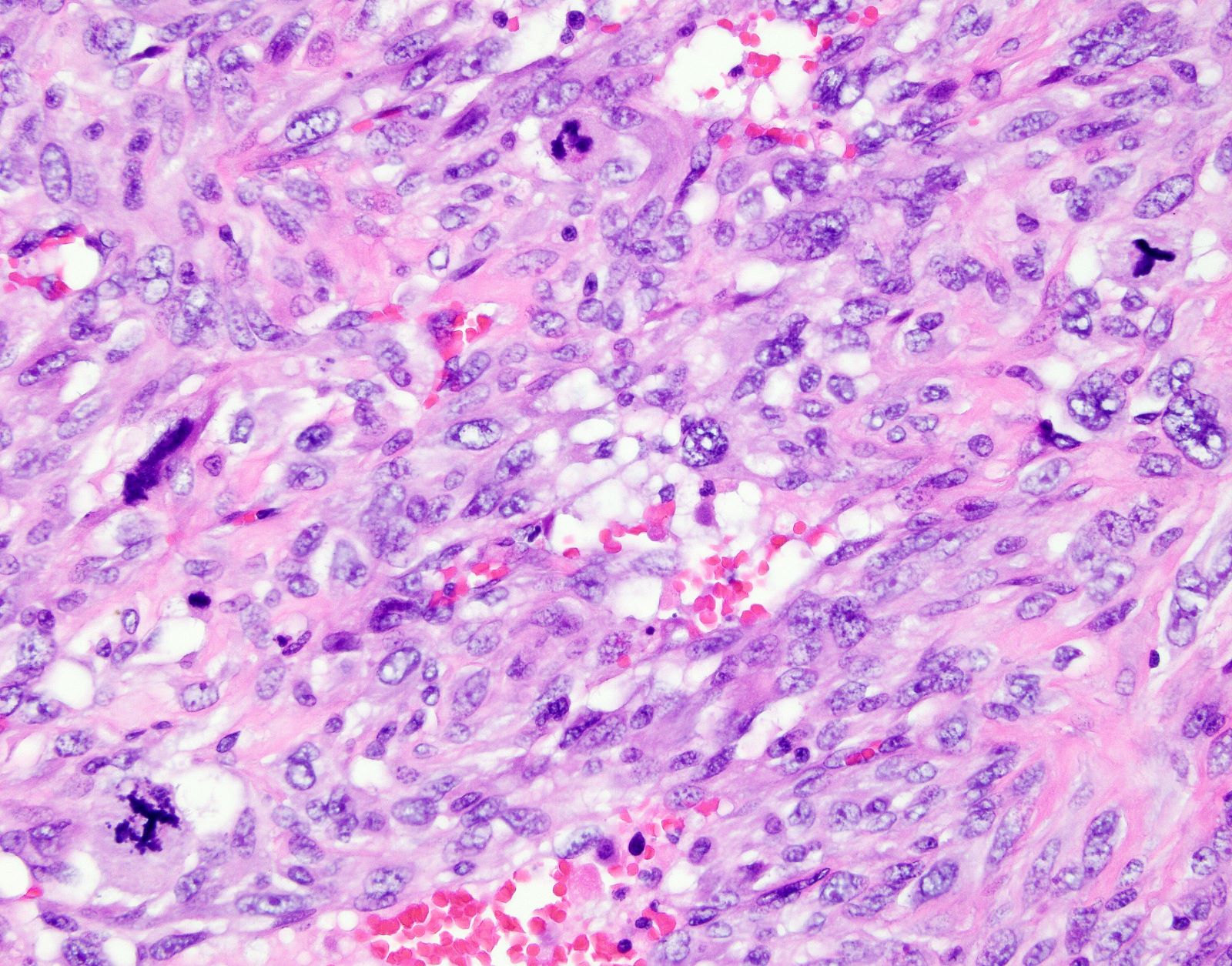
Atypical mitotic figures
Hypercellular tumor
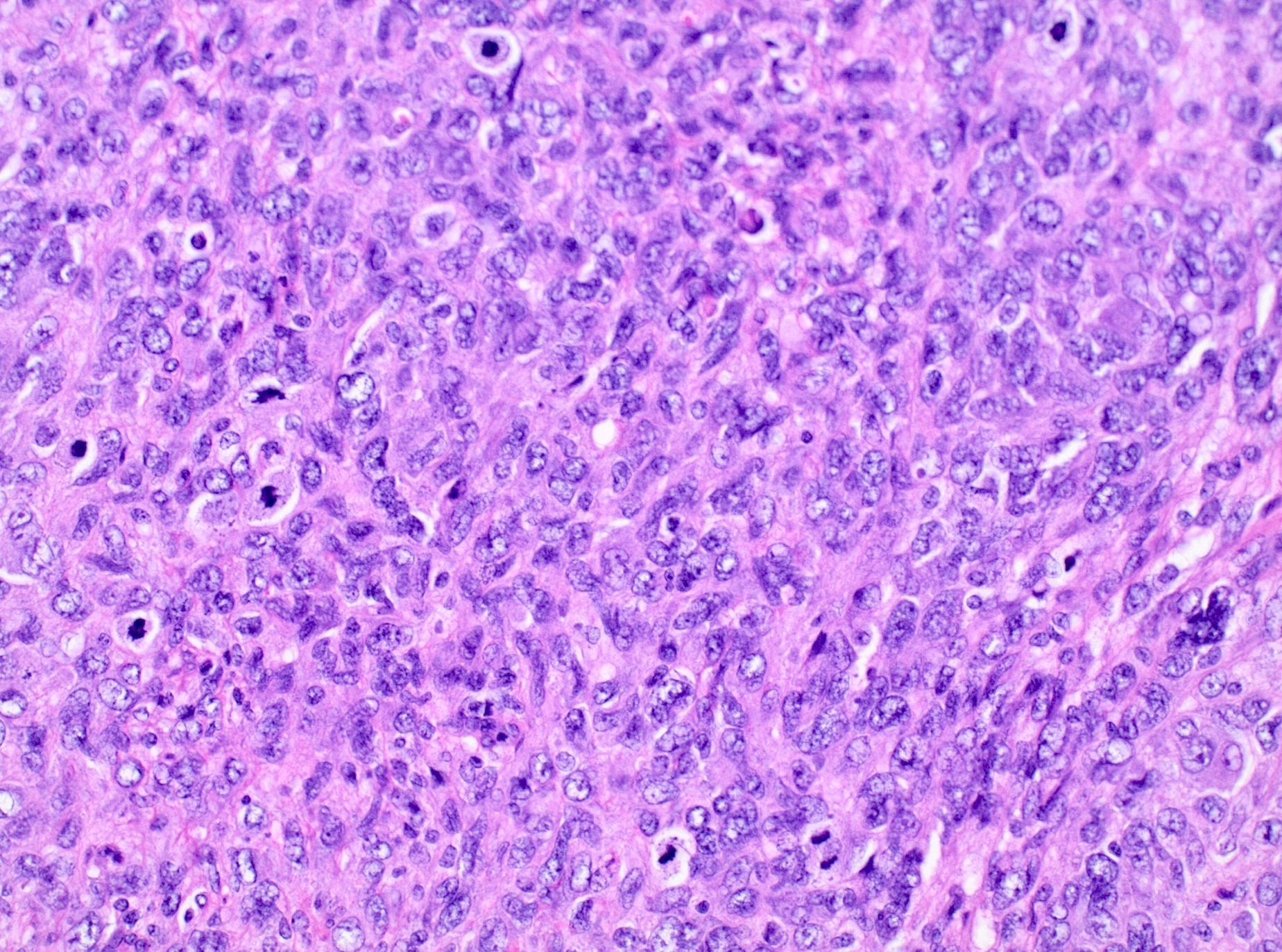
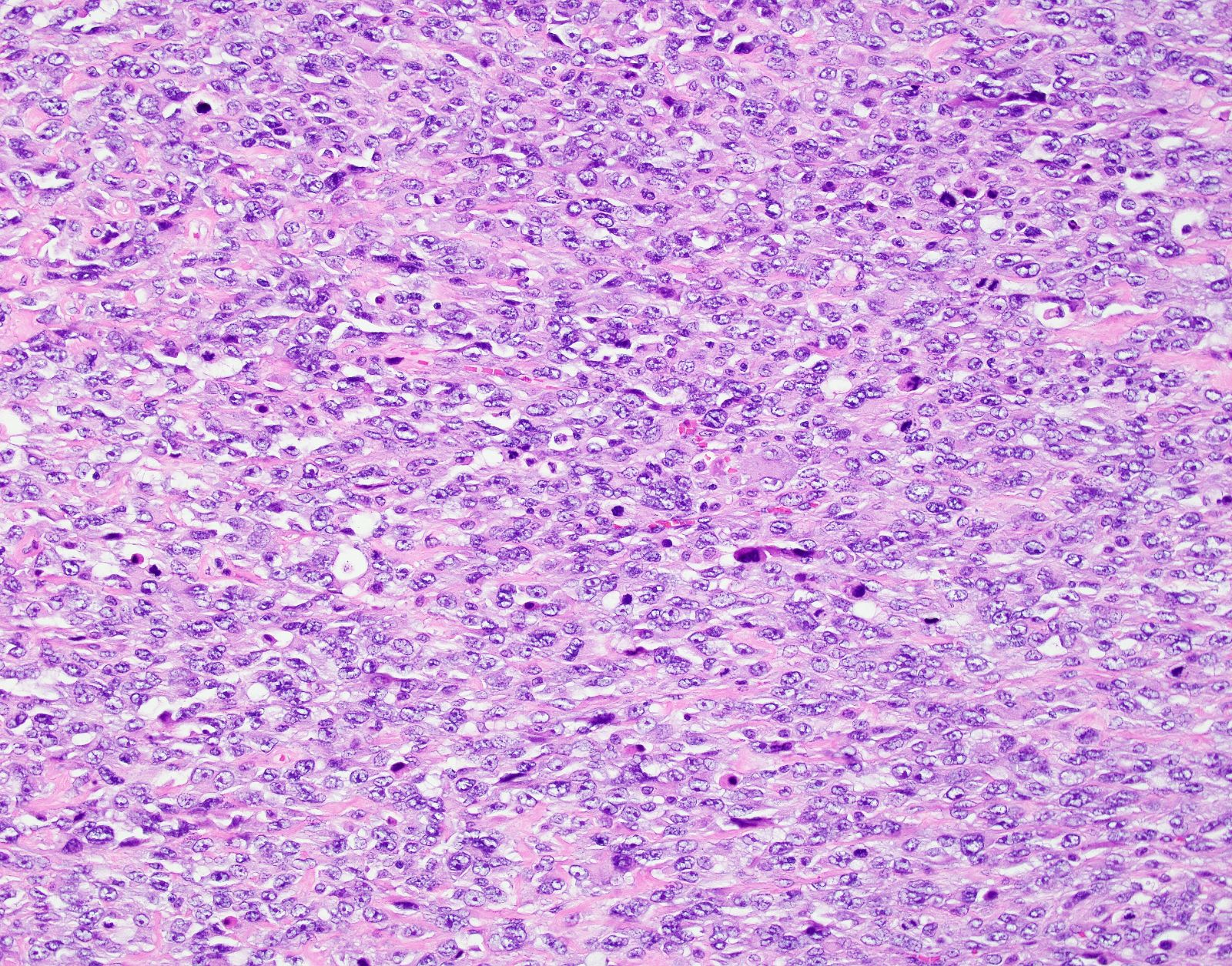
Nuclear atypia

Numerous mitoses
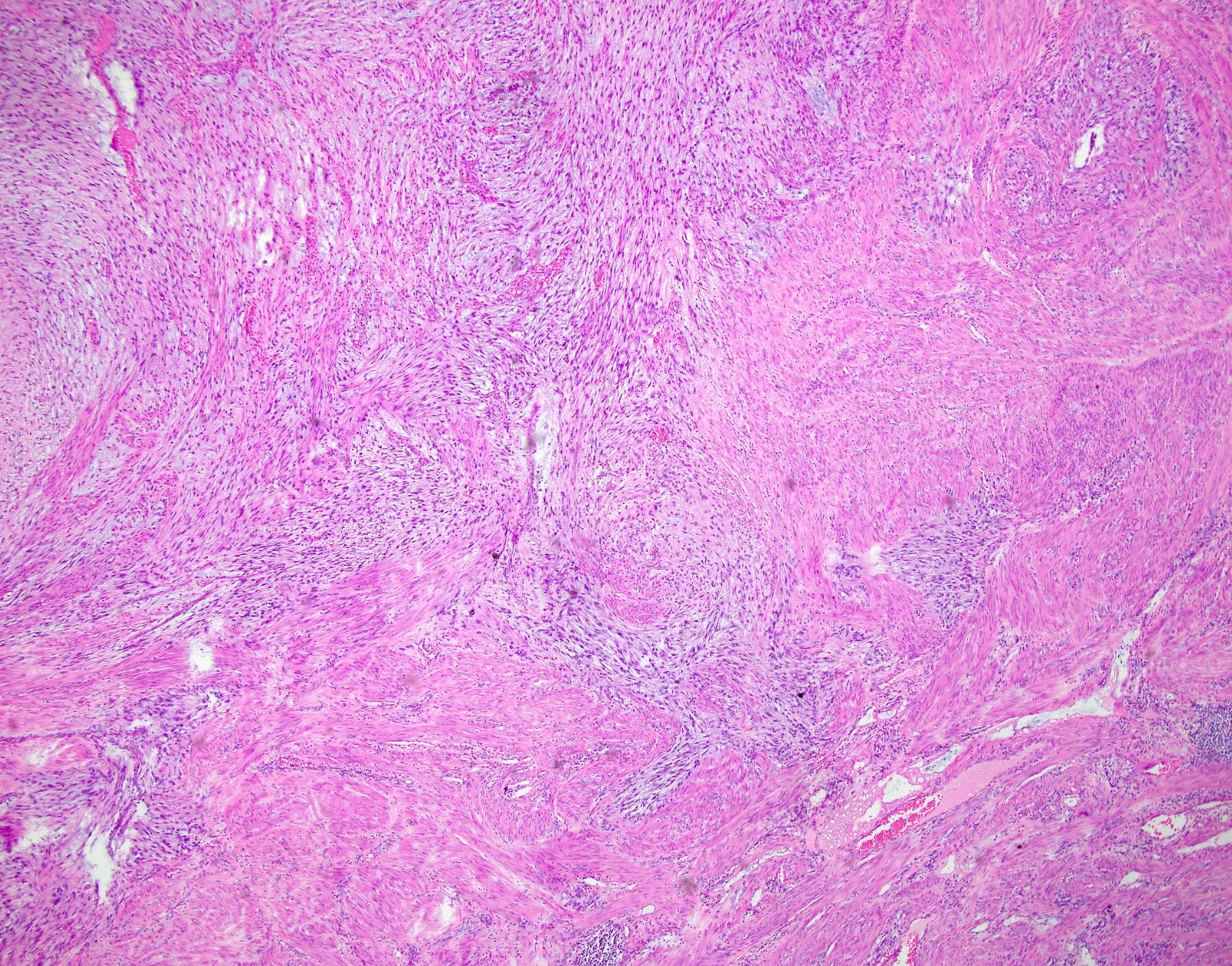
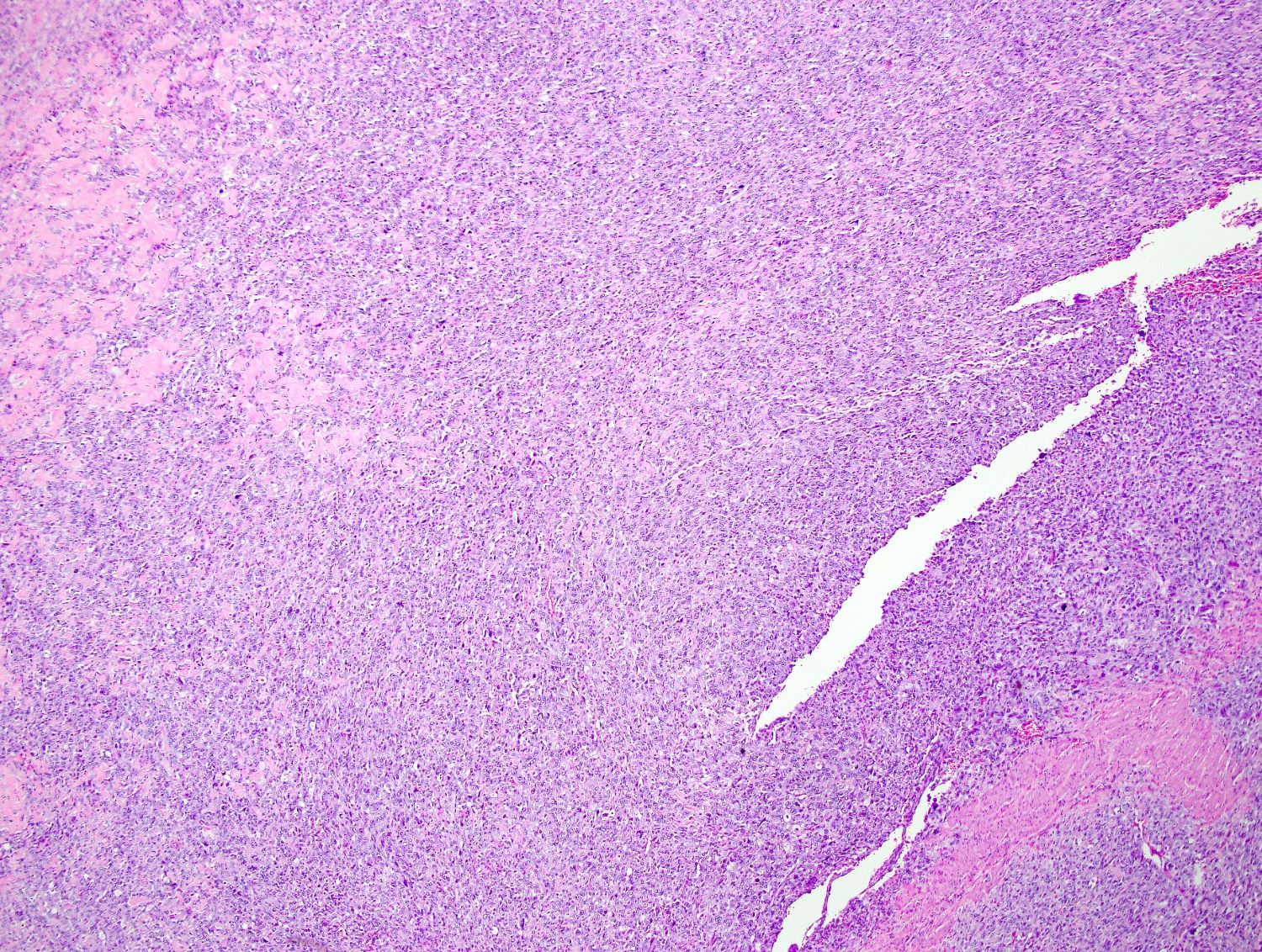
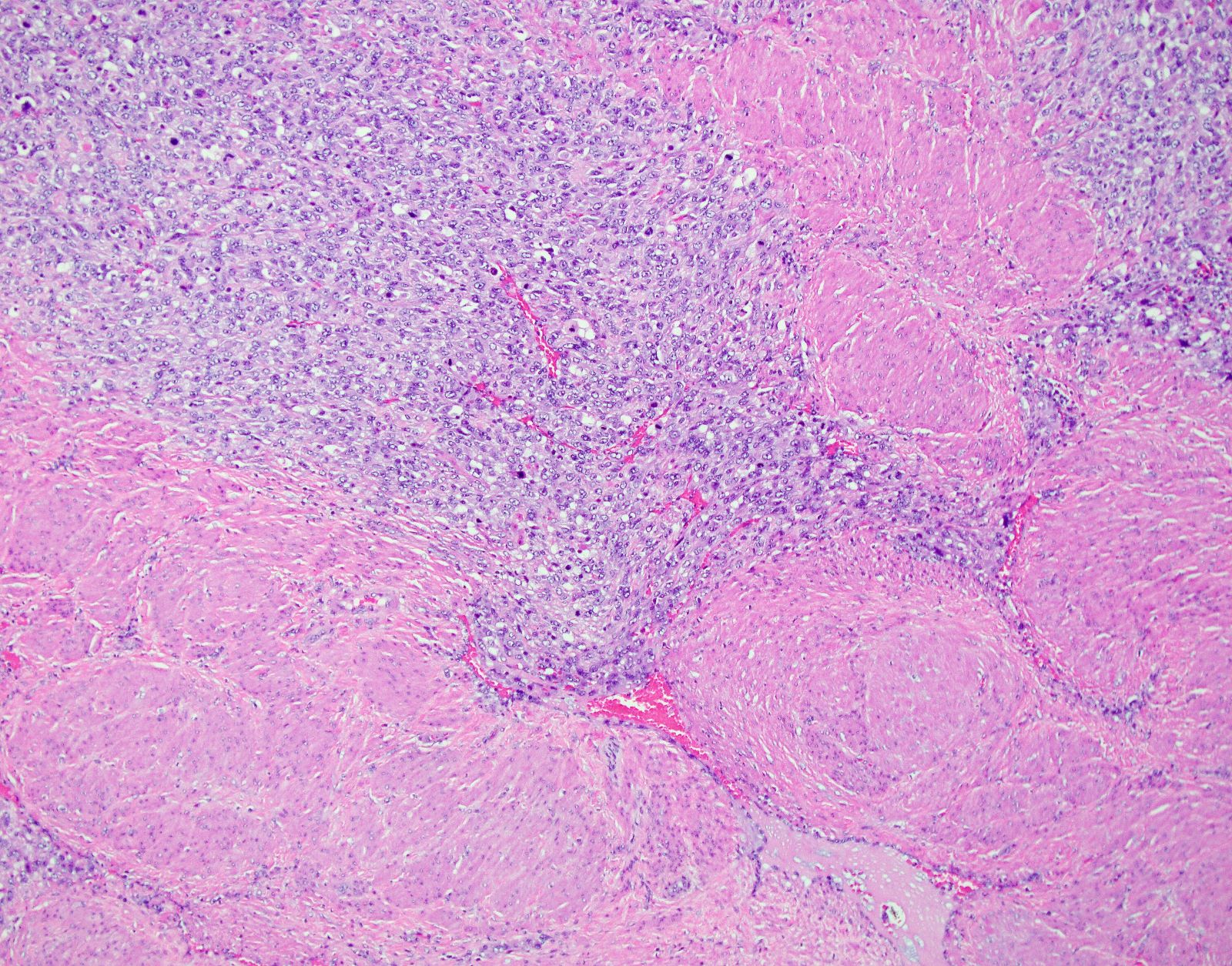
Myxoid leiomyosarcoma, infiltrating border

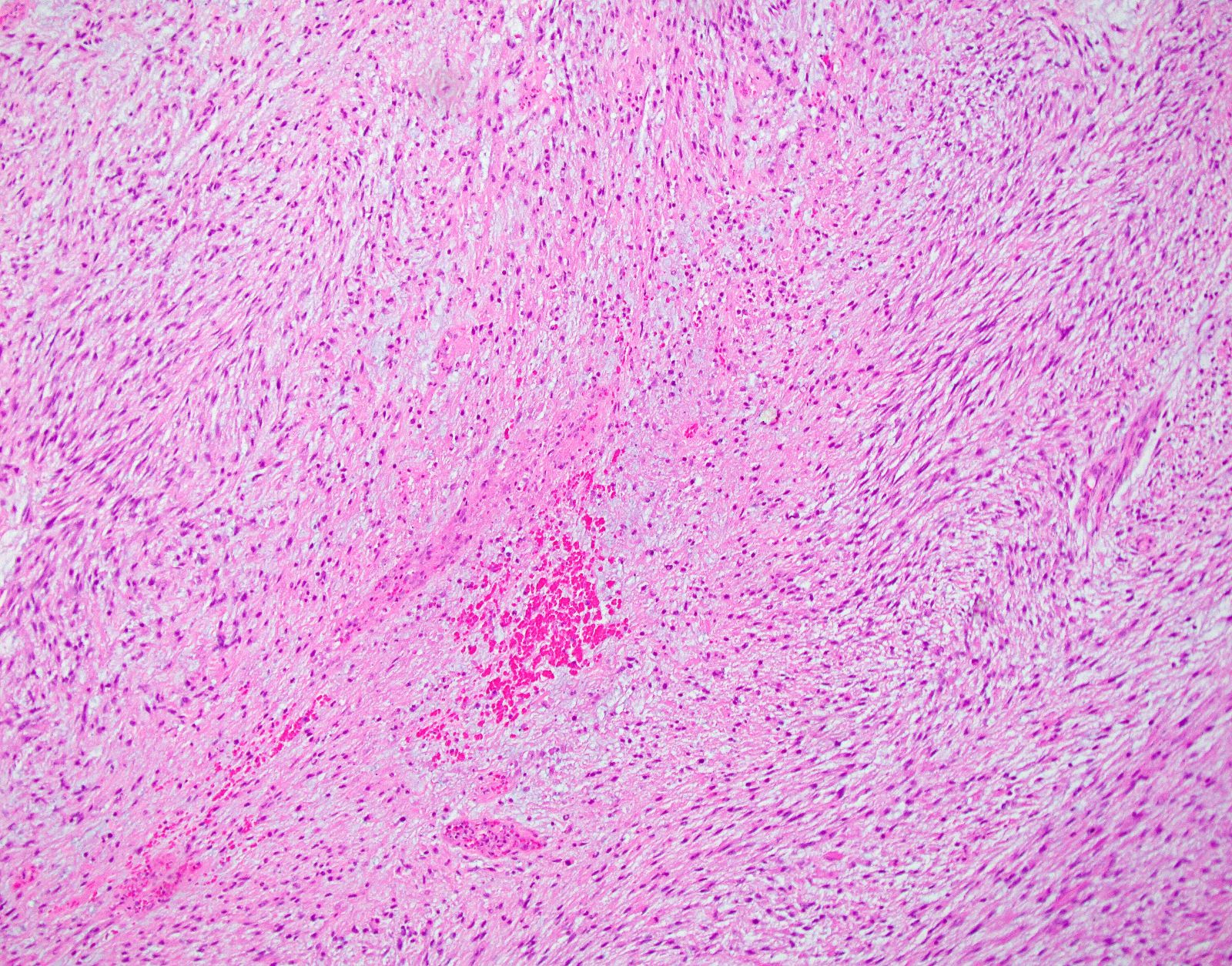
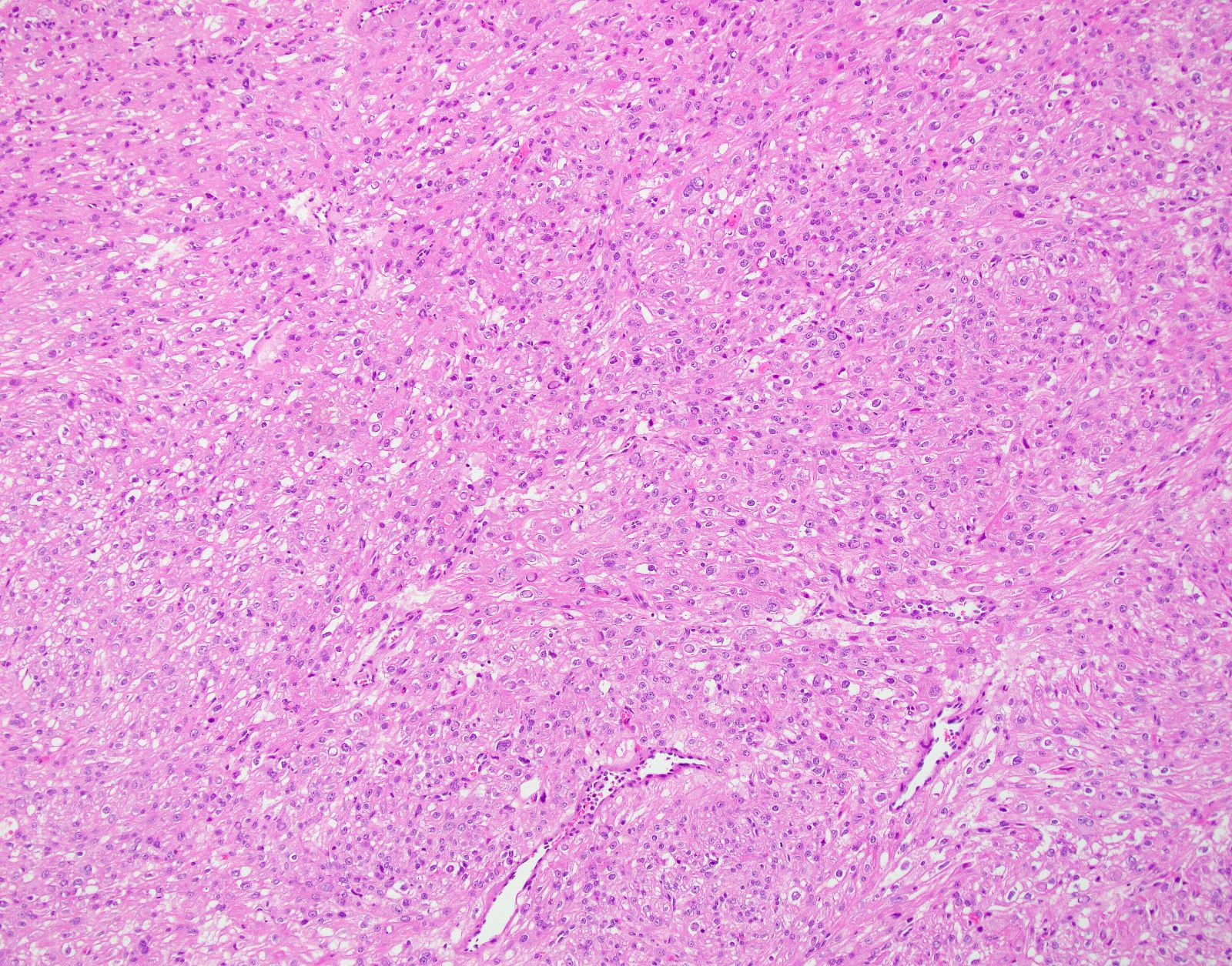
Myxoid leiomyosarcoma
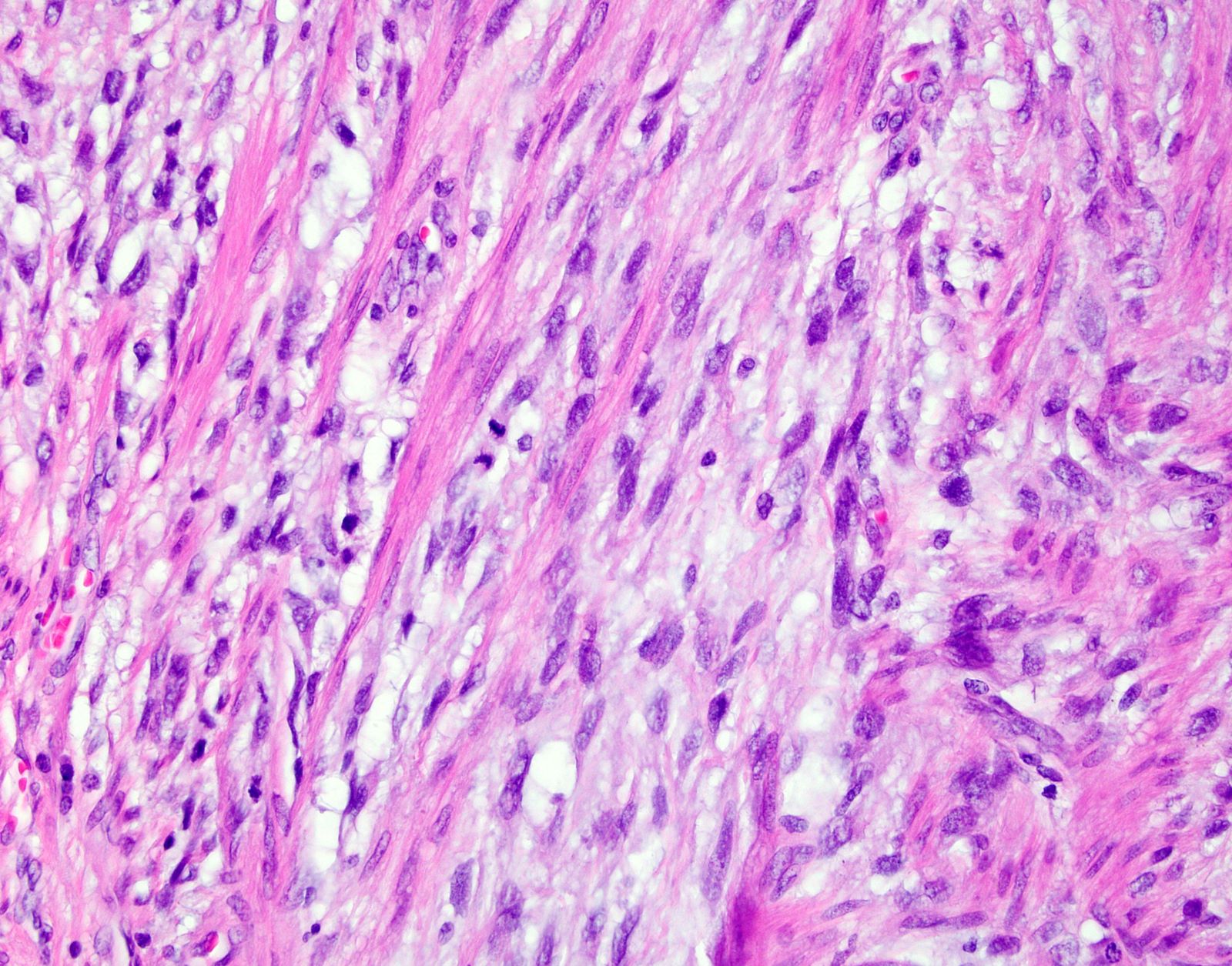
Mitotic figures in myxoid leiomyosarcoma
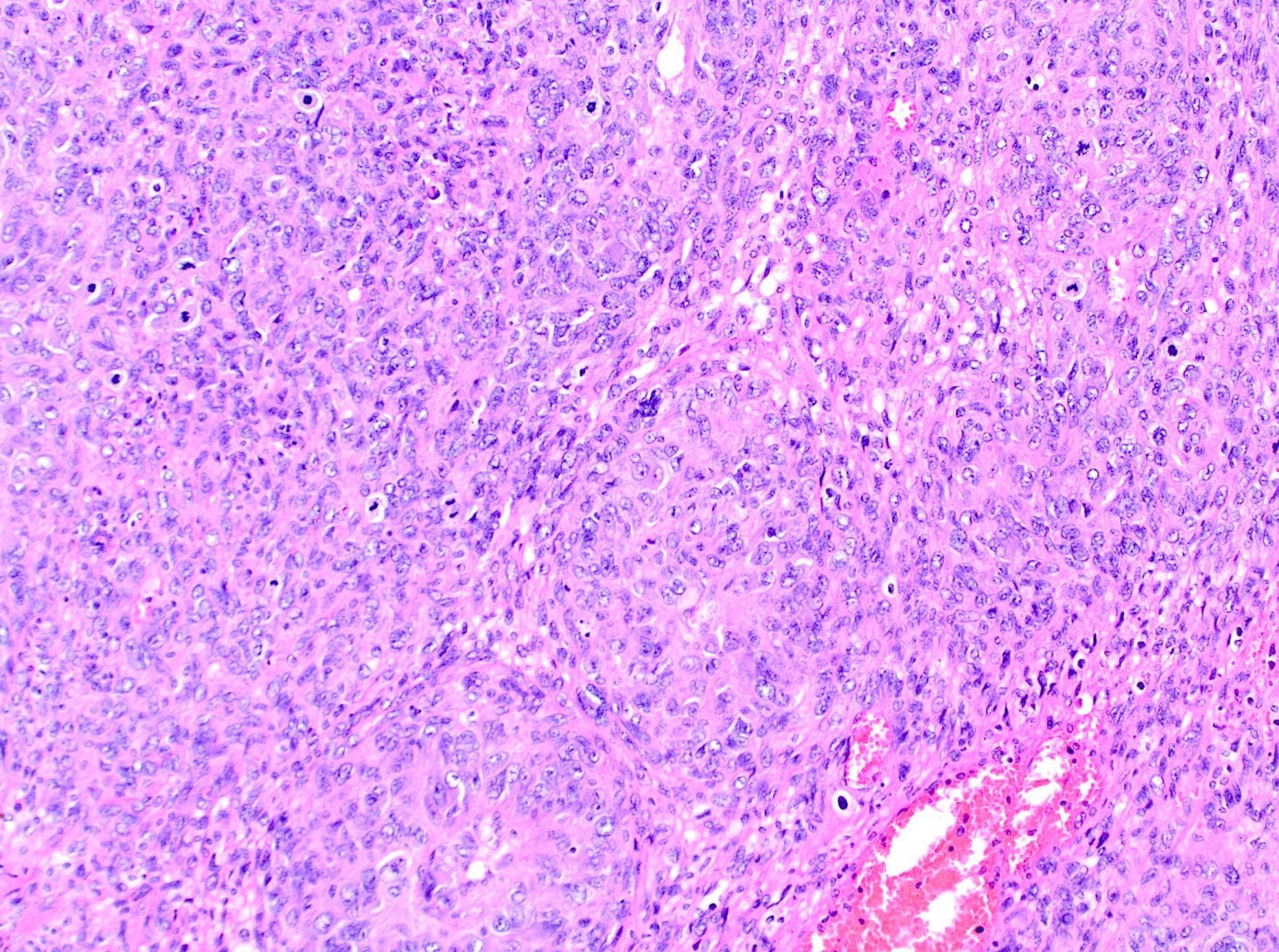
Epithelioid leiomyosarcoma
Epithelioid leiomyosarcoma
Infiltration of adjacent myometrium
Solid growth pattern

Nuclear atypia
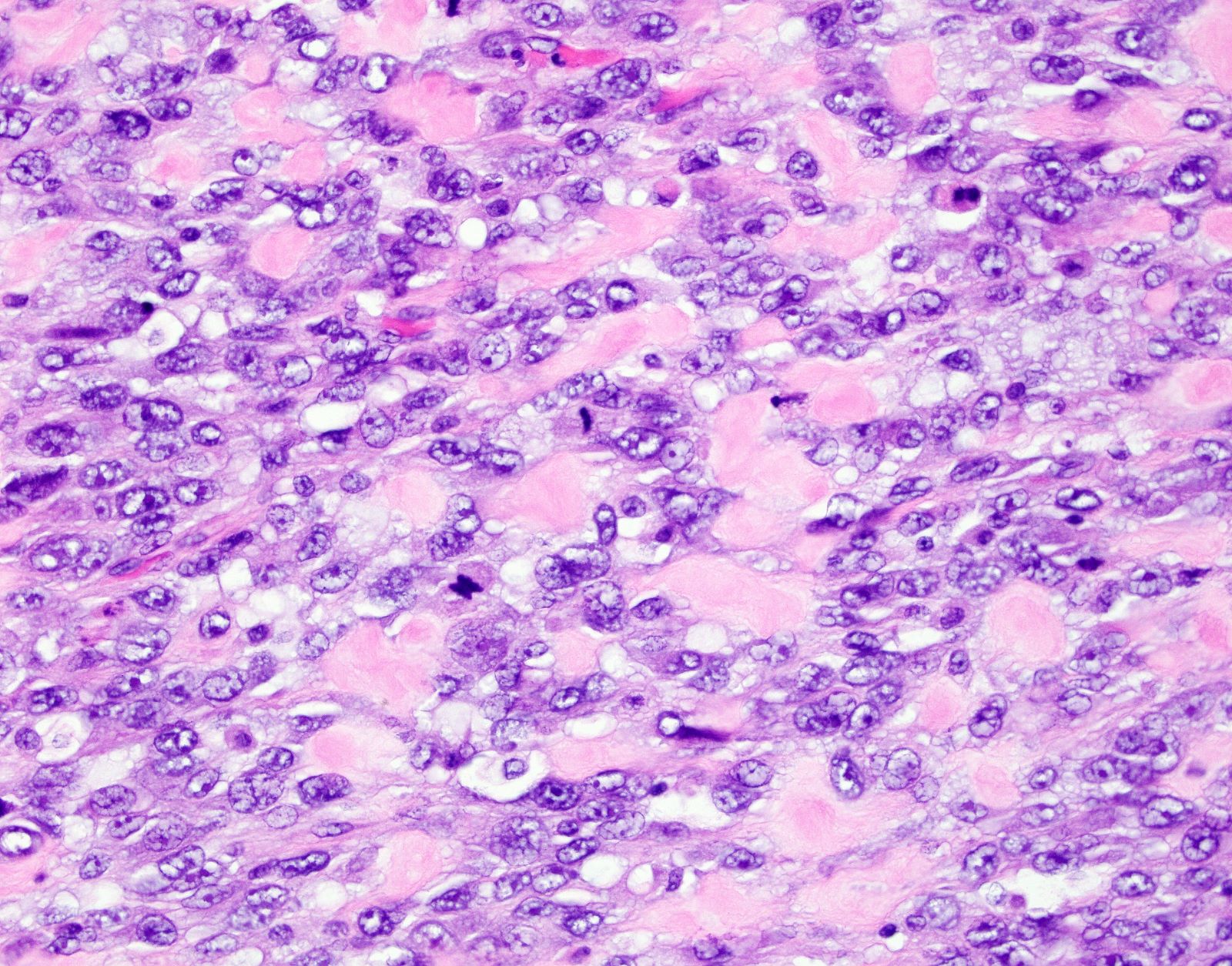
Epithelioid subtype
Virtual slides
Images hosted on other servers:

Leiomyosarcoma with extensive lymphovascular invasion

Expanding pelvic mass in 60 year old woman
Positive stains
- Smooth muscle markers including h-caldesmon (more specific), desmin and SMA:
- May be weak or patchy, especially in myxoid leiomyosarcoma (Adv Anat Pathol 2017;24:354)
- p53 may show aberrant expression (Histopathology 2017;70:1138)
- p16 often shows diffuse expression (Histopathology 2017;70:1138)
- ER / PR
- WT1, keratins, EMA and CD10 are often positive (Am J Surg Pathol 2002;26:403)
- Myxoid subtypes: Alcian blue, colloidal iron and PLAG1 (~50%) (Am J Surg Pathol 2019;43:382, Mod Pathol 2019;32:1688)
- High Ki67 proliferation index (> 10% nuclear staining) can be helpful unless if differentiating from a leiomyoma with bizarre nuclei (Int J Gynecol Pathol 2020;39:354, Int J Gynecol Pathol 2021;40:257)
Negative stains
- HMB45, MelanA, TFE3, MITF and cathepsin K (usually negative or focally and weakly positive) (Int J Gynecol Pathol 2020;39:529, Am J Surg Pathol 2021;45:77, Am J Surg Pathol 2022;46:464)
- ALK
- Androgen receptor (AR) (may be positive)
- Cyclin D1 (rare exceptions)
- S100
Molecular / cytogenetics description
- No specific diagnostic / pathognomonic molecular alterations
- Substantial mutational heterogeneity, widespread DNA copy number alterations including chromothripsis and frequent whole genome duplication (Nat Commun 2018;9:144)
- Hallmarks of "BRCAness", including alterations in homologous recombination DNA repair genes, multiple structural rearrangements and enrichment of specific mutational signatures (Proc Natl Acad Sci U S A 2021;118:e2025182118, Nat Commun 2018;9:144)
- Alternative telomere lengthening (78%) (Nat Commun 2018;9:144)
- Somatic mutations (BMC Cancer 2017;17:639, Proc Natl Acad Sci U S A 2021;118:e2025182118, Nat Commun 2018;9:144)
- TP53 (30 - 60%)
- ATRX (24 - 30%)
- RB1 (27 - 61%)
- MED12 (~20%)
- PTEN (~31 - 57%)
- C-MYC (18%) and TERT (26%) amplifications (Proc Natl Acad Sci U S A 2021;118:e2025182118)
- NR4A3::PGR fusion or PGR rearrangements in 35% of epithelioid leiomyosarcomas (Am J Surg Pathol 2019;43:810)
- PLAG1 rearrangements in ~25% of myxoid leiomyosarcomas (Am J Surg Pathol 2019;43:382)
Molecular / cytogenetics images
Images hosted on other servers:

Somatic mutational landscape
Videos
Review of uterine leiomyosarcoma
Sample pathology report
- Uterus and cervix, total hysterectomy:
- Myometrium:
- Leiomyosarcoma
- Tumor size: 15 cm
- Cytologic atypia: diffuse, marked
- Coagulative tumor cell necrosis: present
- Mitotic count: 25 per 10 high power fields
- Lymphovascular invasion: negative
- Margin status: negative
- Other findings: leiomyomata
- See synoptic report
- Endometrium: inactive
- Uterine serosa: benign
- Cervix: benign
- Myometrium:
Differential diagnosis
- Endometrial stromal sarcoma:
- Low grade endometrial stromal sarcoma:
- Tumor cells resemble proliferative type endometrial stroma
- Minimal cytologic atypia and low mitotic index
- Diffusely positive for CD10 and ER / PR but h-caldesmon typically negative or weak expression
- Cyclin D1 (focal)
- ~66% harbor gene fusions:
- JAZF1::SUZ12 (most common), followed by JAZF1::PHF1, EPC1::PHF1 and MEAF6::PHF1
- High grade endometrial stromal sarcoma:
- Round or spindle high grade cells with brisk mitoses and necrosis
- Infiltrative growth pattern
- Molecular alterations are: YWHAE::NUTM2A / YWHAE::NUTM2B fusion, ZC3H7B::BCOR and BCOR internal tandem duplication (ITD)
- Low grade endometrial stromal sarcoma:
- Leiomyoma variants:
- Mitotically active leiomyoma:
- No cytologic atypia or coagulative tumor cell necrosis
- 6 - 14 mitoses / 10 HPF
- Leiomyoma with apoplectic changes:
- Zonation phenomena (benign smooth muscle away from necrotic areas)
- Cellular leiomyoma:
- Increased cellularity but no cytologic atypia or tumor necrosis
- Leiomyoma with bizarre nuclei:
- Scattered or diffuse bizarre nuclei with adjacent areas of classic leiomyoma
- Myxoid leiomyoma:
- Usually focal myxoid change within a conventional leiomyoma, no coagulative tumor cell necrosis, cytologic atypia or mitotic activity
- Epithelioid leiomyoma:
-
No coagulative tumor cell necrosis, cytologic atypia or mitotic activity
- Mitotically active leiomyoma:
- Smooth muscle tumors of uncertain malignant potential (STUMP):
- Some but not all criteria are met for uterine leiomyosarcoma:
- Spindled smooth muscle tumors: focal / multifocal or diffuse cytologic atypia and 2 - 4 mitoses / mm2 (6 - 9 mitoses / 10 high power fields, 0.55 mm field of diameter, 0.24 mm2 in area) but lacking coagulative necrosis; unequivocal coagulative necrosis but lacking cytologic atypia or elevated mitoses; elevated mitoses at > 6 mitoses / mm2 or > 15 mitoses / 10 high power fields (FD = 0.55, 0.24 mm2 in area) but lacking coagulative necrosis or cytologic atypia; diffuse cytologic atypia and uncertain mitotic count, often due to prominent karyorrhexis but lacking coagulative necrosis
- Epithelioid smooth muscle tumors: epithelioid morphology with 2 - 3 mitoses / 10 high power fields (FD = 0.55, 0.24 mm2 in area) but lacking moderate to severe cytologic atypia and coagulative necrosis
- Myxoid smooth muscle tumors: myxoid morphology but lacking mitotic activity, moderate to severe cytologic atypia, coagulative necrosis and infiltrative / irregular borders
- Some but not all criteria are met for uterine leiomyosarcoma:
- Inflammatory myofibroblastic tumor:
- Spindle cell neoplasm with myxoid stroma and associated lymphoplasmacytic inflammatory cells
- Atypia can range from mild to severe
- ALK staining is seen in most tumors and ALK rearrangement is seen in 80% of cases (Mod Pathol 2017;30:1489)
- Perivascular epithelioid cell tumor:
- Composed of epithelioid or spindled cells with eosinophilic to clear cytoplasm with variable cytologic atypia and mitoses
- Cells may be organized in a perivascular fashion, short fascicles, sheets or nests
- Melanin rarely present
- Typically strongly HMB45 positive and often MelanA or MITF positive
- Cathepsin K staining
- A subset harbor TSC1 and TSC2 alterations or TFE3 fusion (Mod Pathol 2022;35:515)
Additional references
Board review style question #1
What mitotic count per 10 high power fields is used to aid in diagnosing spindle cell leiomyosarcoma of the uterus?
- > 1 mitosis per 10 high power fields
- ≥ 5 mitoses per 10 high power fields
- ≥ 10 mitoses per 10 high power fields
- Not a diagnostic criterion
Board review style answer #1
C. ≥ 10 mitoses per 10 high power fields. Uterine spindle cell leiomyosarcomas are diagnosed based on the presence of 2 of 3 morphologic features: a mitotic count of ≥ 10 mitoses per 10 high power fields, moderate to marked cytologic atypia and coagulative tumor cell necrosis.
Comment Here
Reference: Leiomyosarcoma
Comment Here
Reference: Leiomyosarcoma
Board review style question #2
A 62 year old woman underwent a hysterectomy for a uterine mass. Immunohistochemical stains show that the tumor is positive for h-caldesmon and desmin and negative for CD10 and ALK. What is the most likely diagnosis?
- Endometrial stromal sarcoma
- High grade endometrial adenocarcinoma
- Inflammatory myofibroblastic tumor
- Leiomyosarcoma, myxoid subtype
Board review style answer #2
D. Leiomyosarcoma, myxoid subtype. The image shows a myxoid mesenchymal tumor with infiltrative borders. The morphologic findings combined with the immunophenotype is consistent with leiomyosarcoma, myxoid subtype.
Comment Here
Reference: Leiomyosarcoma
Comment Here
Reference: Leiomyosarcoma

