
Cervix
Premalignant / preinvasive lesions - cytology
Atypical glandular cells (cytology)
Authors: Joseph Reznicek, M.D., Bonnie Choy, M.D.
Editorial Board Member: Ricardo R. Lastra, M.D.

Last author update: 26 September 2023
Last staff update: 17 September 2024
Copyright: 2006-2025, PathologyOutlines.com, Inc.
PubMed Search: Atypical glandular cells cervix cytology


Table of Contents
Definition / general | Essential features | CPT coding | Sites | Diagrams / tables | Clinical features | Laboratory | Management | Case reports | Cytology description | Cytology images | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Reznicek J, Choy B. Atypical glandular cells (cytology). PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/cervixcytologyagc.html. Accessed April 1st, 2025.
Definition / general
- Atypical glandular cells encompass a broad and challenging differential diagnosis and include entities such as atypical endocervical cells and atypical endometrial cells
Essential features
- Criteria based on the 2014 Bethesda System for Reporting Cervical Cytology (Nayar: The Bethesda System for Reporting Cervical Cytology, 3rd Edition, 2015)
- Atypical glandular cells fall under the Bethesda system general diagnostic heading of epithelial abnormalities, glandular
- Atypical glandular cells encompass both endocervical cell and endometrial cell abnormalities
- Atypical endocervical cells may be further classified as follows: atypical endocervical cells, NOS or atypical endocervical cells, favor neoplastic
- Atypical endocervical cells, favor neoplastic should be rendered when cell morphology is slightly insufficient for an interpretation of endocervical adenocarcinoma in situ or invasive adenocarcinoma
- Atypical endometrial cells are generally not further classified as favor neoplastic because this distinction has been shown to be poorly reproducible
CPT coding
- For screening Pap tests (routine and high risk): smear
- For screening Pap tests (routine and high risk): liquid based
- Manual screening only
- ThinPrep Imager assisted screening
- FocalPoint (instrument only)
- FocalPoint (with manual screening)
- For diagnostic Pap tests: smear
- For diagnostic Pap tests: liquid based
- Manual screening only
- ThinPrep Imager assisted screening
- FocalPoint (instrument only)
- FocalPoint (with manual screening)
Sites
- Cervix
Diagrams / tables
Images hosted on other servers:

Algorithm for initial workup of AGC

Algorithm for management after diagnostic examination
Clinical features
- Atypical glandular cell (AGC) reporting rates are published by the College of American Pathologists (CAP) for benchmarking purposes
- High grade lesions are identified in 10 - 40% of AGC cytology cases on follow up (Nayar: The Bethesda System for Reporting Cervical Cytology, 3rd Edition, 2015)
- Squamous lesions (high grade squamous intraepithelial lesion [HSIL] / cervical intraepithelial neoplasia [CIN] grade 2 - 3) occur more often than glandular lesions
- HSIL and adenocarcinoma in situ (AIS) frequently coexist
Laboratory
- HPV testing may be used as part of screening, triage and surveillance (J Am Soc Cytopathol 2020;9:291)
- Initially endorsed as triage test for atypical squamous cells of undetermined significance (ASCUS) cytologic result in 2001
- Approved for
- Cotesting in 2003
- Postcolposcopic / posttreatment follow up and risk stratification using partial genotype (HPV 16 / 18) in 2006
- Primary screening option in 2014
- 5 FDA approved HPV testing platforms
- Qiagen Hybrid Capture
- Hologic Cervista
- Hologic Aptima
- Roche Cobas: FDA approved for primary screening
- Becton Dickinson Onclarity: FDA approved for primary screening
- Note: HPV result plays no role in the cytologic examination or grading of SIL
Management
- Management guidelines are per the 2019 ASCCP Risk Based Management Consensus Guidelines for Abnormal Cervical Cancer Screening Tests and Cancer Precursors (J Low Genit Tract Dis 2020;24:102)
- Atypical glandular cells
- All subcategories (except atypical endometrial cells; see below) regardless of HPV result are recommended to proceed to colposcopy (with endocervical sampling if not pregnant) and endometrial sampling (if at least 35 years of age or < age 35 and at risk for endometrial neoplasia)
- Atypical glandular cells, NOS or atypical endocervical cells, NOS
- No CIN2+, AIS or cancer detected
- Cotest at 1 and 2 years
- Any abnormality → colposcopy
- Both tests negative → cotest 3 years later
- CIN2+ detected but no glandular neoplasia
- Manage per 2019 ASCCP guidelines
- Cotest at 1 and 2 years
- No CIN2+, AIS or cancer detected
- Atypical glandular cells, favor neoplastic
- If no adenocarcinoma in situ (AIS) or invasive carcinoma are detected by colposcopy / biopsy, then proceed to diagnostic excisional procedure
- Atypical endometrial cells
- Endometrial and endocervical sampling is recommended
- If no endometrial pathology, perform colposcopy
Case reports
- 29 year old woman with high grade squamous intraepithelial lesion and adenocarcinoma in situ of cervix, initially presented as atypical endocervical cells, favor neoplastic, on cervical cytology (Diagn Cytopathol 2008;36:823)
- 41 year old woman with endometriosis mimicking atypical glandular cells on cervical cytology (J Cytol 2017;34:61)
- 48 year old woman with high grade serous ovarian carcinoma with serous tubal intraepithelial carcinoma, initially presented as atypical glandular cells, favor neoplastic, on cervical cytology (Taiwan J Obstet Gynecol 2015;54:183)
Cytology description
- Diagnostic criteria (Nayar: The Bethesda System for Reporting Cervical Cytology, 3rd Edition, 2015)
- Atypical endocervical cells, NOS
- Cells occur in sheets and strips with some cell crowding, nuclear overlap or pseudostratification
- Nuclear enlargement and increased N:C ratio
- Anisonucleosis
- Mild nuclear hyperchromasia and chromatin irregularities
- Occasional nucleoli
- Rare mitotic figures
- Distinct cell borders
- Atypical endocervical cells, favor neoplastic
- Abnormal cells occur in sheets and strips with nuclear crowding, overlap or pseudostratification
- Rare cell groups with rosettes (gland formations) or feathering
- Nuclei are enlarged and often elongated with some hyperchromasia and coarse chromatin with heterogeneity
- Occasional mitoses or apoptotic debris
- Cell borders may be ill defined
- Atypical endometrial cells
- Atypical endometrial cells are generally not further classified as favor neoplastic because this distinction has been shown to be poorly reproducible
- Cells occur in small groups, usually 5 - 10 cells per group
- Nuclei are slightly enlarged compared with normal endometrial cells
- Mild hyperchromasia and chromatin heterogeneity
- Atypical endocervical cells, NOS
Cytology images
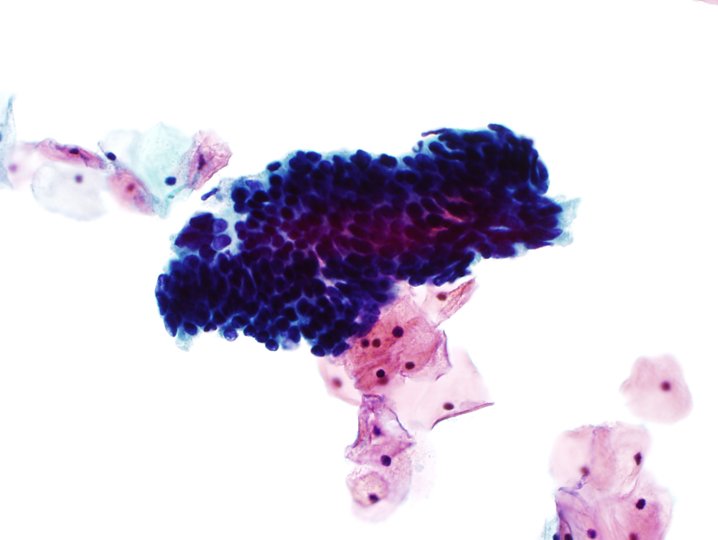
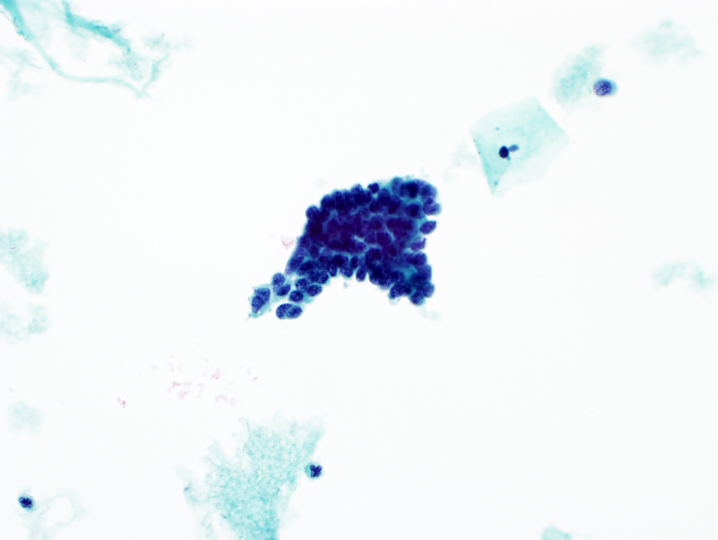
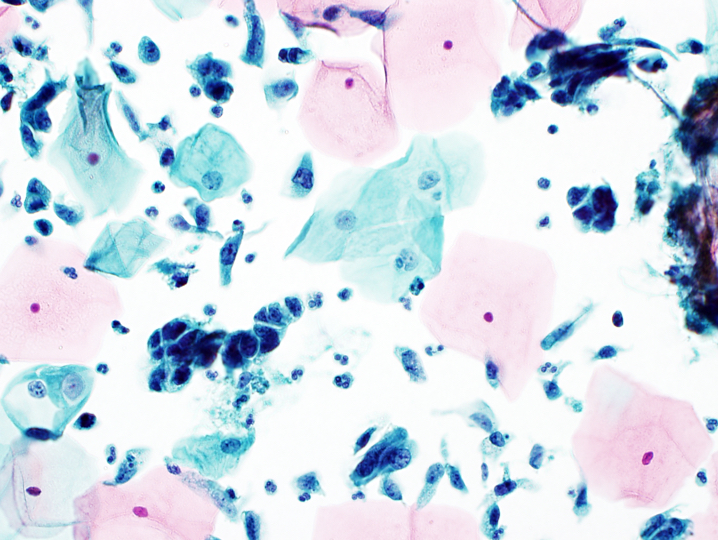
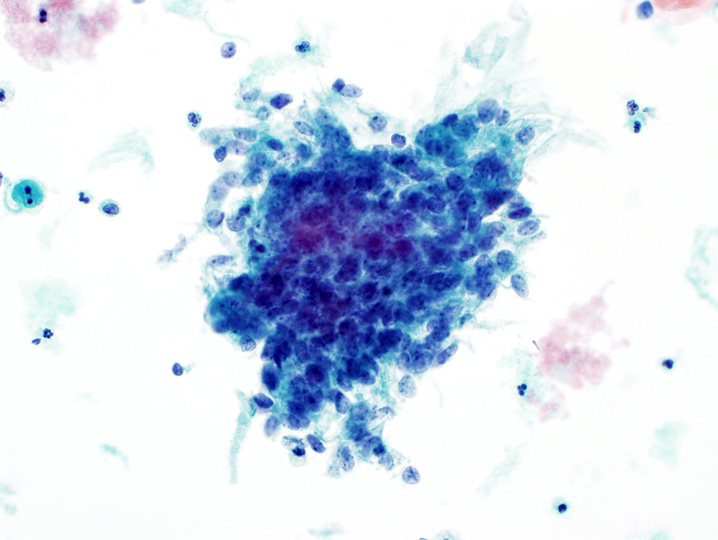
Contributed by Joseph Reznicek, M.D.
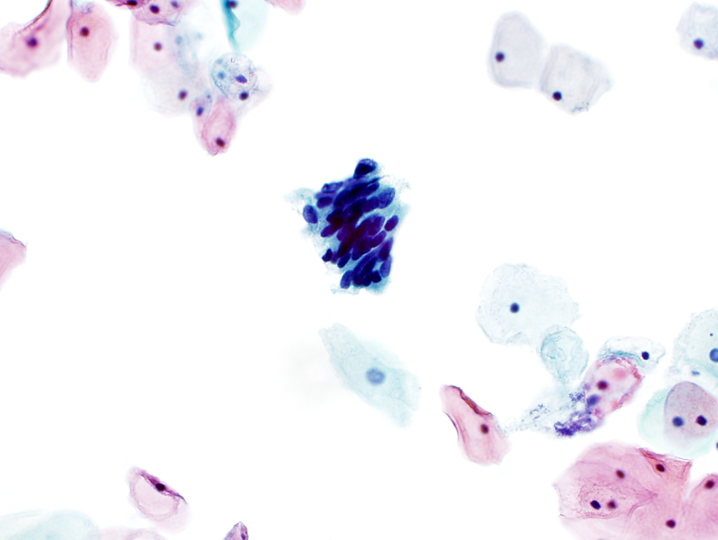

Atypical endocervical cells, favor neoplastic
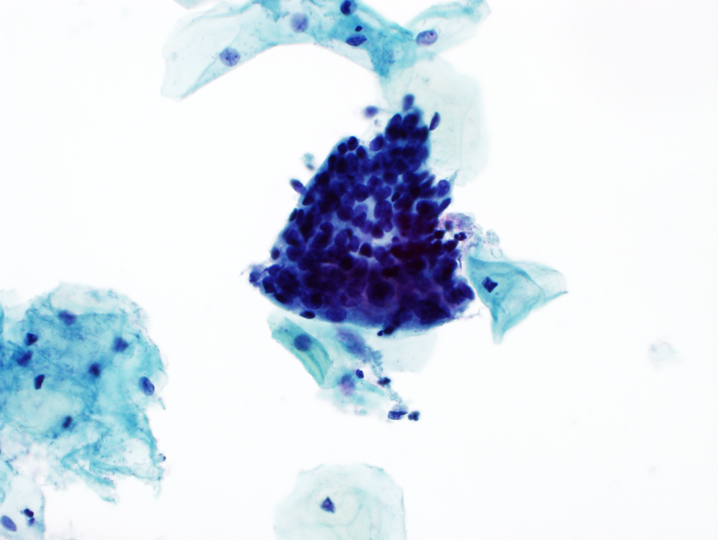
Atypical glandular cells, NOS

Atypical glandular cells, NOS
Endocervical adenocarcinoma
Endometrial adenocarcinoma
Images hosted on other servers:

WHO digital atlas
Sample pathology report
- Gynecologic pap:
- Statement of adequacy:
- Satisfactory for evaluation
- Transformation zone component present
- Final interpretation:
- Epithelial cell abnormality, glandular cell
- Atypical glandular cells, favor neoplastic (see comment)
- Comment: Suggest colposcopy (with endocervical sampling) and endometrial sampling as clinically indicated.
- Statement of adequacy:
Differential diagnosis
- Isolated endocervical cells:
- Presence of small nucleoli
- Finely granular and evenly distributed chromatin
- Smooth nuclear contours
- Granular or finely vacuolated cytoplasm, occasionally with some elongation
- Exfoliated cells may have rounded up appearance and high N:C ratio
- Retain columnar cytoplasmic configuration with eccentrically placed nuclei
- Endocervical adenocarcinoma in situ (AIS):
- Hyperchromatic nuclei with fine to coarse chromatin
- Nuclear membrane irregularities and notching
- High N:C ratio
- Feathering or rosette formation
- Directly sampled endometrium:
- Nuclei slightly larger than those of intermediate squamous cells
- Lower N:C ratio
- Smooth nuclear membranes
- Maintain nuclear polarity when seen in clusters with associated endometrial stromal cells
- Endocervical adenocarcinoma:
- Abundant abnormal columnar shaped cells
- Enlarged nuclei with irregular chromatin distribution and nuclear membrane irregularities
- Finely vacuolated cytoplasm
- Macronucleoli
- Endometrial adenocarcinoma:
- Small, tight clusters or single round cells
- Enlarged, hyperchromatic nuclei with small to prominent nucleoli
- Scant, often vacuolated cytoplasm
- Mitotic figures and apoptotic bodies present
- Intracytoplasmic neutrophils within single cells or small groups
- In liquid based preparations, 3 dimensional groups and clusters or papillary configuration are common
- Watery or finely granular tumor diathesis is variably present; in liquid based preparations, it is often less prominent and identified as finely granular debris clinging to the periphery of clusters of cells
- HSIL:
- Nuclear atypia, including nuclear enlargement, irregular nuclear contours with frequent prominent indentations / grooves, generally hyperchromatic, lack of nucleoli
- High N:C ratio
- Lacks specific architectural features of AIS such as feathering, rosettes and pseudostratified strips of columnar cells
- Tubal metaplasia:
- Apical terminal bar and cilia
- Same sized nuclei as squamous metaplastic nuclei
- Basally placed nucleus with smooth nuclear contours
- May have higher N:C ratio than normal endocervical cells
Board review style question #1
Board review style answer #1
A. Atypical glandular cells, favor neoplastic. The image shows endocervical cells with crowding, nuclear overlap, hyperchromasia and focal feathering. Answers B, C and D are incorrect because cytologic features of endometrial adenocarcinoma, HSIL and tubal metaplasia are not seen.
Comment Here
Reference: Atypical glandular cells (cytology)
Comment Here
Reference: Atypical glandular cells (cytology)
Board review style question #2
A cervical cytology specimen from a 36 year old woman is signed out as atypical glandular cells, favor neoplastic. According to the 2019 ASCCP guidelines, which of the following is the next most appropriate step in management?
- Colposcopy with biopsy
- Endometrial sampling only
- HPV testing
- Return to care in 6 months
Board review style answer #2
A. Colposcopy with biopsy. Colposcopy with biopsy is the single best answer choice in this scenario per the 2019 ASCCP guidelines. All atypical glandular cell subcategories regardless of HPV result are recommended to proceed to colposcopy. HPV testing alone, endometrial sampling alone and return to care in 6 months are not appropriate.
Comment Here
Reference: Atypical glandular cells (cytology)
Comment Here
Reference: Atypical glandular cells (cytology)
