
Cervix
Premalignant / preinvasive lesions - cytology
LSIL (cytology)
Authors: Lucy Jager, M.D., Bonnie Choy, M.D.
Editorial Board Member: Marc Pusztaszeri, M.D.
Deputy Editor-in-Chief: Jennifer A. Bennett, M.D.

Last author update: 31 January 2022
Last staff update: 8 December 2023
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed search: LSIL[TI] cervix cytology


Table of Contents
Definition / general | Essential features | CPT coding | Sites | Etiology | Clinical features | Laboratory | Management | Cytology description | Cytology images | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Jager L, Choy B. LSIL (cytology). PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/cervixcytologyLSIL.html. Accessed March 30th, 2025.
Definition / general
- Changes in squamous cells associated with human papillomavirus (HPV) infection, encompassing mild dysplasia and cervical intraepithelial neoplasia (CIN) 1
Essential features
- Lesion of intermediate or superficial cells caused by low risk and high risk HPV
- Most are transient infections with little risk for oncogenesis
- Criteria based on the 2014 Bethesda System for Reporting Cervical Cytology (see Bethesda system):
- Nuclear atypia, including nuclear enlargement (> 3x the area of normal intermediate nuclei), hyperchromasia, anisonucleosis, coarsely granular / smudgy / densely opaque chromatin, variable nuclear membranes, binucleation / multinucleation
- Koilocytosis or dense orangeophilia must be accompanied by nuclear abnormalities
CPT coding
- For screening Pap tests (routine and high risk): smear
- For screening Pap tests (routine and high risk): liquid based
- Manual screening only
- ThinPrep Imager assisted screening
- FocalPoint (instrument only)
- FocalPoint (with manual screening)
- For diagnostic Pap tests: smear
- For diagnostic Pap tests: liquid based
- Manual screening only
- ThinPrep Imager assisted screening
- FocalPoint (instrument only)
- FocalPoint (with manual screening)
Sites
- Cervix, vagina, anus
Etiology
- Caused by a number of low risk and high risk HPVs (J Clin Pathol 2002;55:244, N Engl J Med 2003;348:518)
- Low risk HPV: 6, 11, 42, 43, 44, 53, 54, 57, 66
- High risk HPV: 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 68
Clinical features
- Accounts for ~2.5% of all Pap test results (Arch Pathol Lab Med 2010;134:331)
- Most are transient infections with little risk for oncogenesis
- ~60% regress spontaneously (Int J Gynecol Pathol 1993;12:186)
- 30% persist
- 10% progress to high grade squamous intraepithelial lesion (HSIL)
- 18% of women with an low grade squamous intraepithelial lesion (LSIL) Pap result prove to have HSIL on biopsy (Am J Obstet Gynecol 2003;188:1406)
- < 1% of untreated progress to invasive cancer (Obstet Gynecol 1998;92:727)
Laboratory
- HPV testing may be used as part of screening, triage and surveillance (J Am Soc Cytopathol 2020;9:291)
- Initially endorsed as triage test for atypical squamous cells of undetermined significance (ASCUS) cytologic result in 2001
- Approved for:
- Cotesting in 2003
- Postcolposcopic / posttreatment follow up and risk stratification using partial genotype (HPV 16 / 18) in 2006
- Primary screening option in 2014
- 5 U.S. Food and Drug Administration (FDA) approved HPV testing platforms
- QIAGEN Hybrid Capture
- Hologic Cervista
- Hologic Aptima
- Roche Cobas: FDA approved for primary screening
- Becton Dickinson Onclarity: FDA approved for primary screening
- Note: HPV result plays no role in the cytologic examination or grading of SIL
Management
- 2019 American Society of Colposcopy and Cervical Pathology (ASCCP) risk based management consensus guidelines for abnormal cervical cancer screening tests and cancer precursors (J Low Genit Tract Dis 2020;24:102)
- Personalized risk based recommendations based on a patient's risk of CIN 3+, as determined by a combination of current results and past history (including unknown history)
Cytology description
- Diagnostic criteria (Nayar: The Bethesda System for Reporting Cervical Cytology, 3rd Edition, 2015)
- Large, mature cells (equal in size to a normal superficial or intermediate squamous cell) with abundant cytoplasm
- Cells seen singly, in clusters, as well as in sheets
- Nuclear atypia
- Nuclear enlargement > 3x the area of normal intermediate nuclei
- Low but slightly increased N/C ratio
- Generally hyperchromatic but may be normochromatic
- Anisonucleosis
- Coarsely granular, smudgy or densely opaque chromatin
- Variable nuclear contours ranging from smooth to very irregular with notches
- Binucleation and multinucleation common
- Absent or inconspicuous nucleoli
- Cytoplasmic cavities (koilocytes): characteristic viral cytopathic feature
- Broad, sharply delineated clear perinuclear zone and a peripheral rim of densely stained cytoplasm
- Dense, eosinophilic cytoplasm of increased keratinization with little or no evidence of koilocytosis
- Koilocytosis or dense orangeophilia must be accompanied by nuclear abnormalities
- Large, mature cells (equal in size to a normal superficial or intermediate squamous cell) with abundant cytoplasm
Cytology images
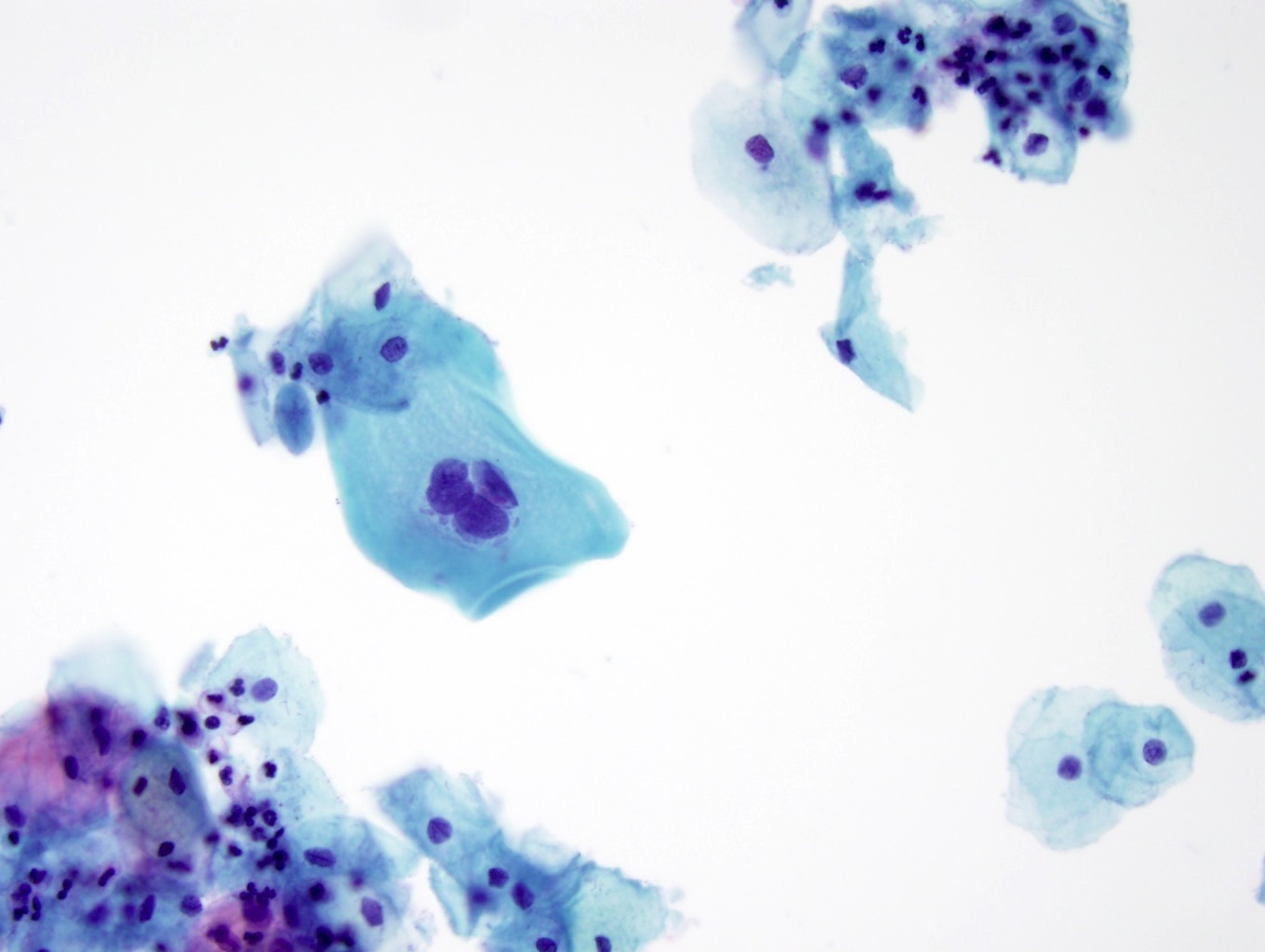
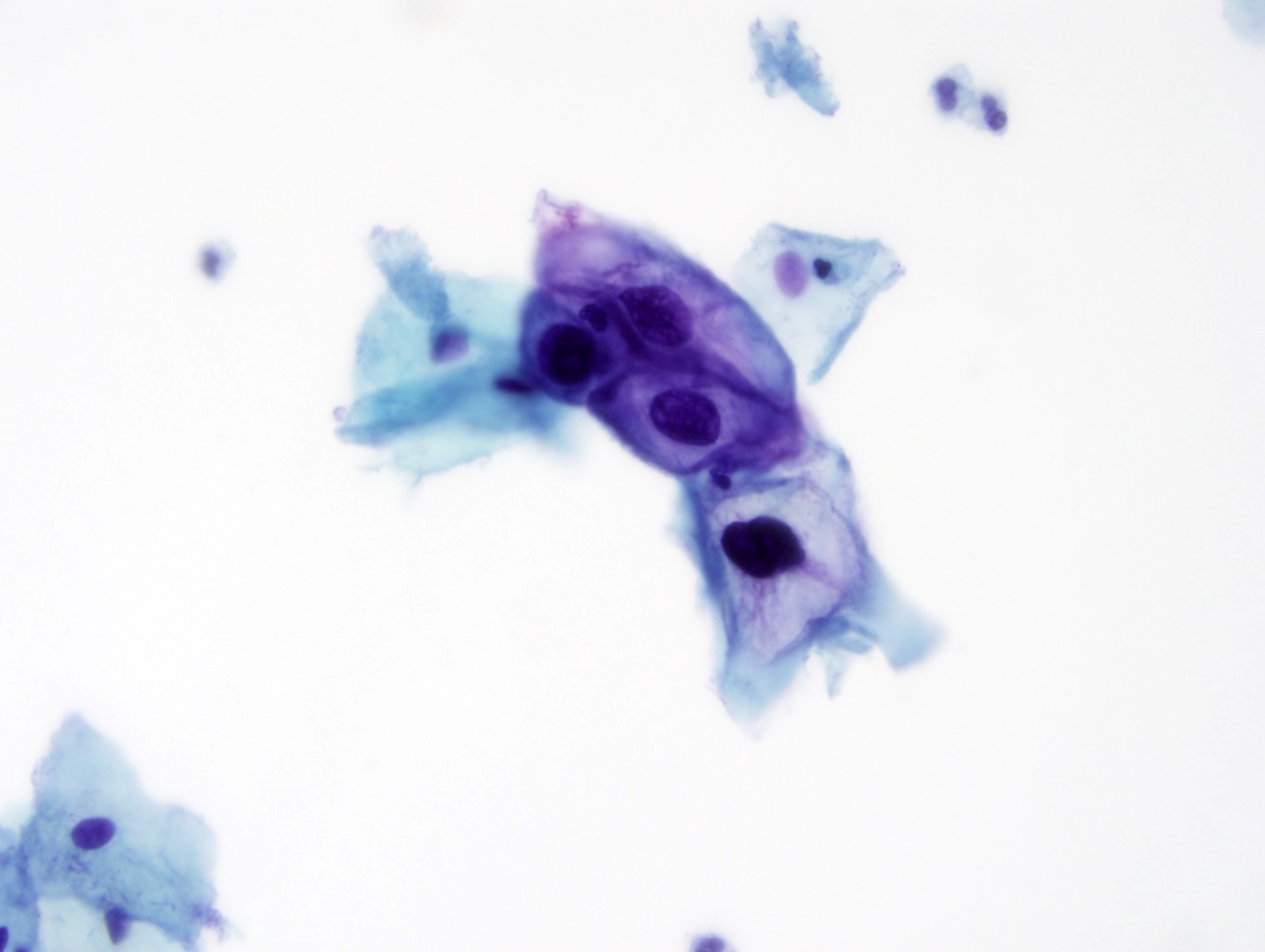
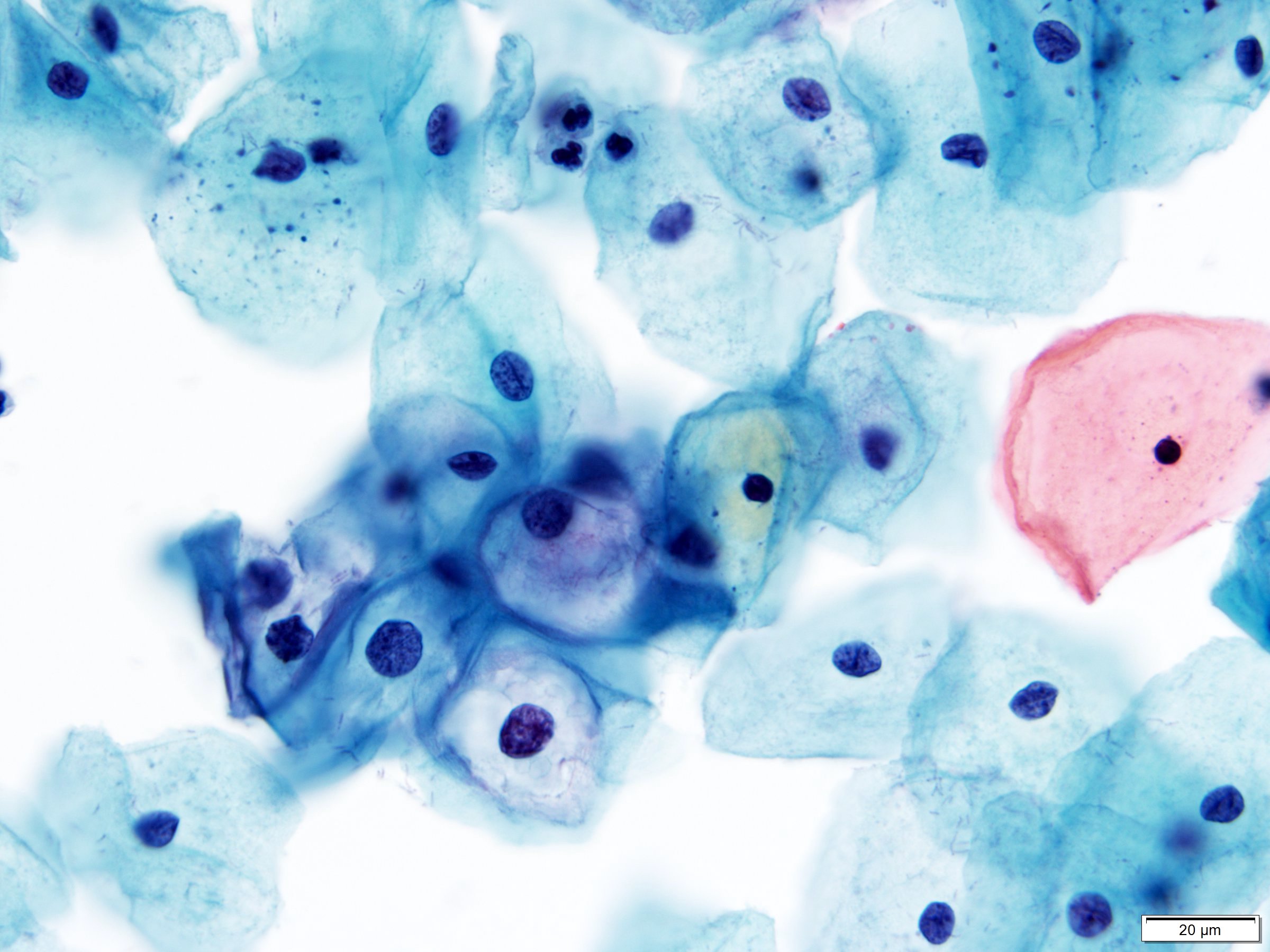
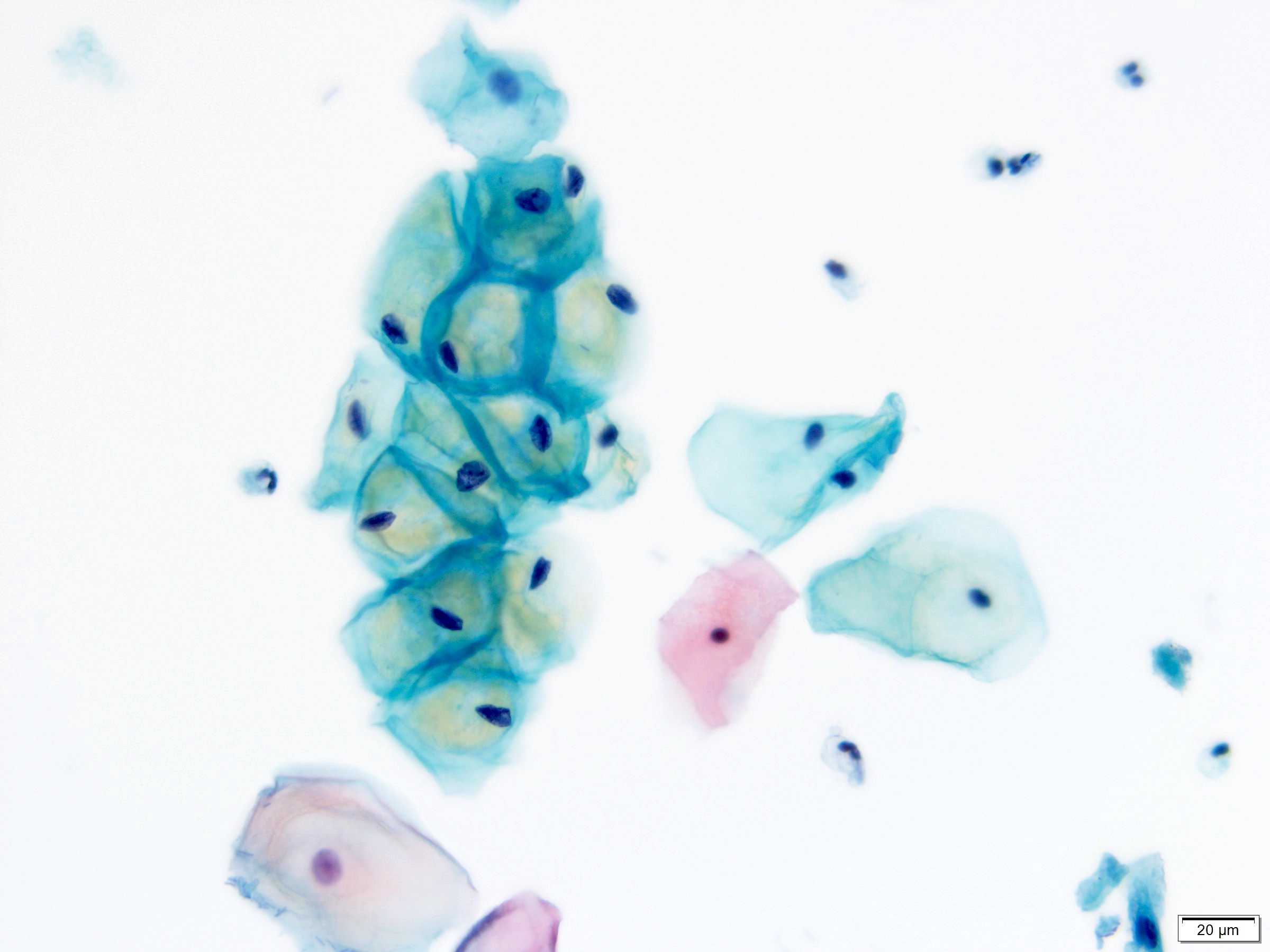
Contributed by Lucy Jager, M.D. and Bonnie Choy, M.D.
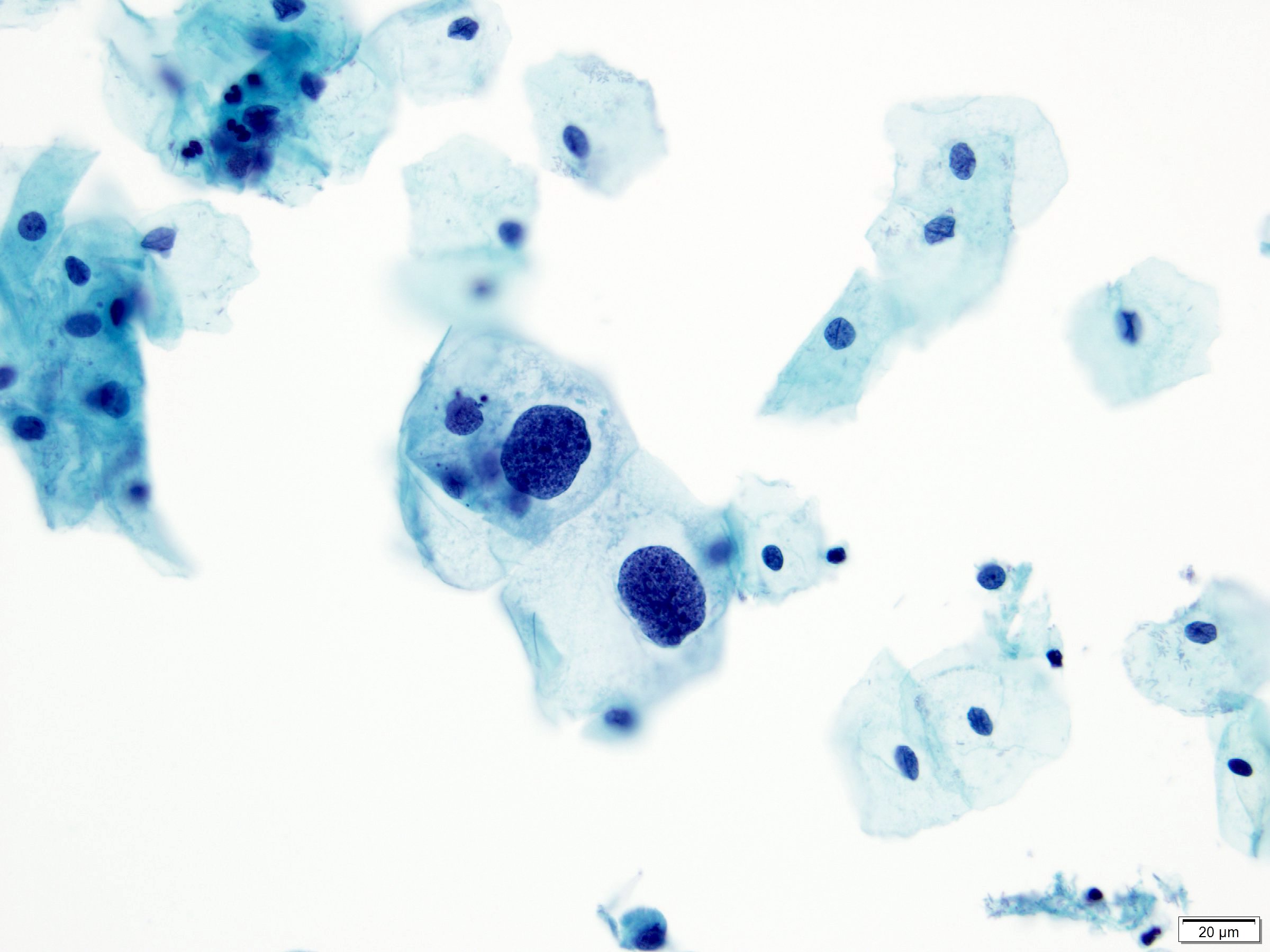
Nuclear enlargement and hyperchromasia
Multinucleation

Binucleation and perinuclear cavitation
Koilocytosis with nuclear abnormalities
Koilocytosis with nuclear abnormalities
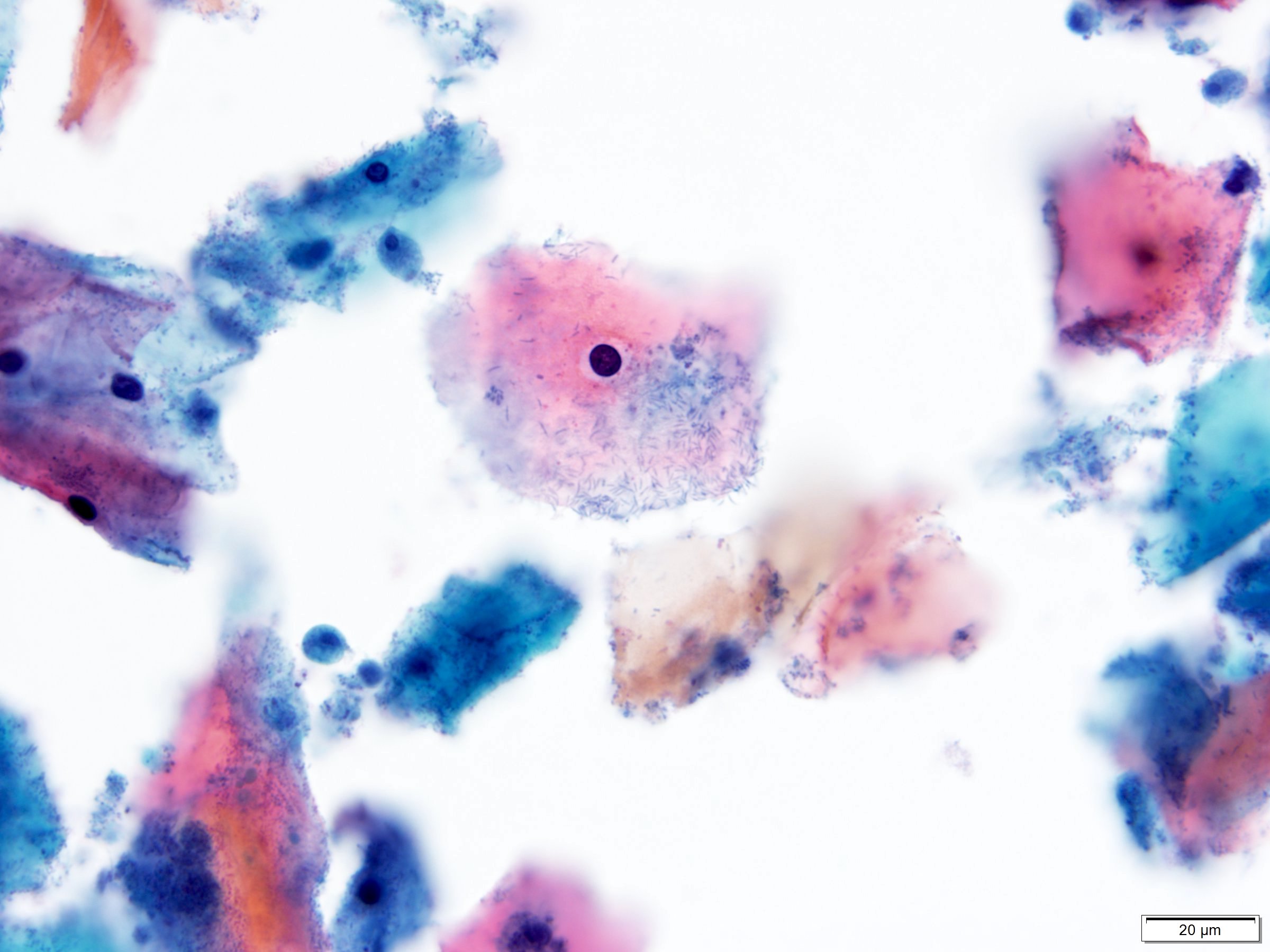
Pseudokoilocytes
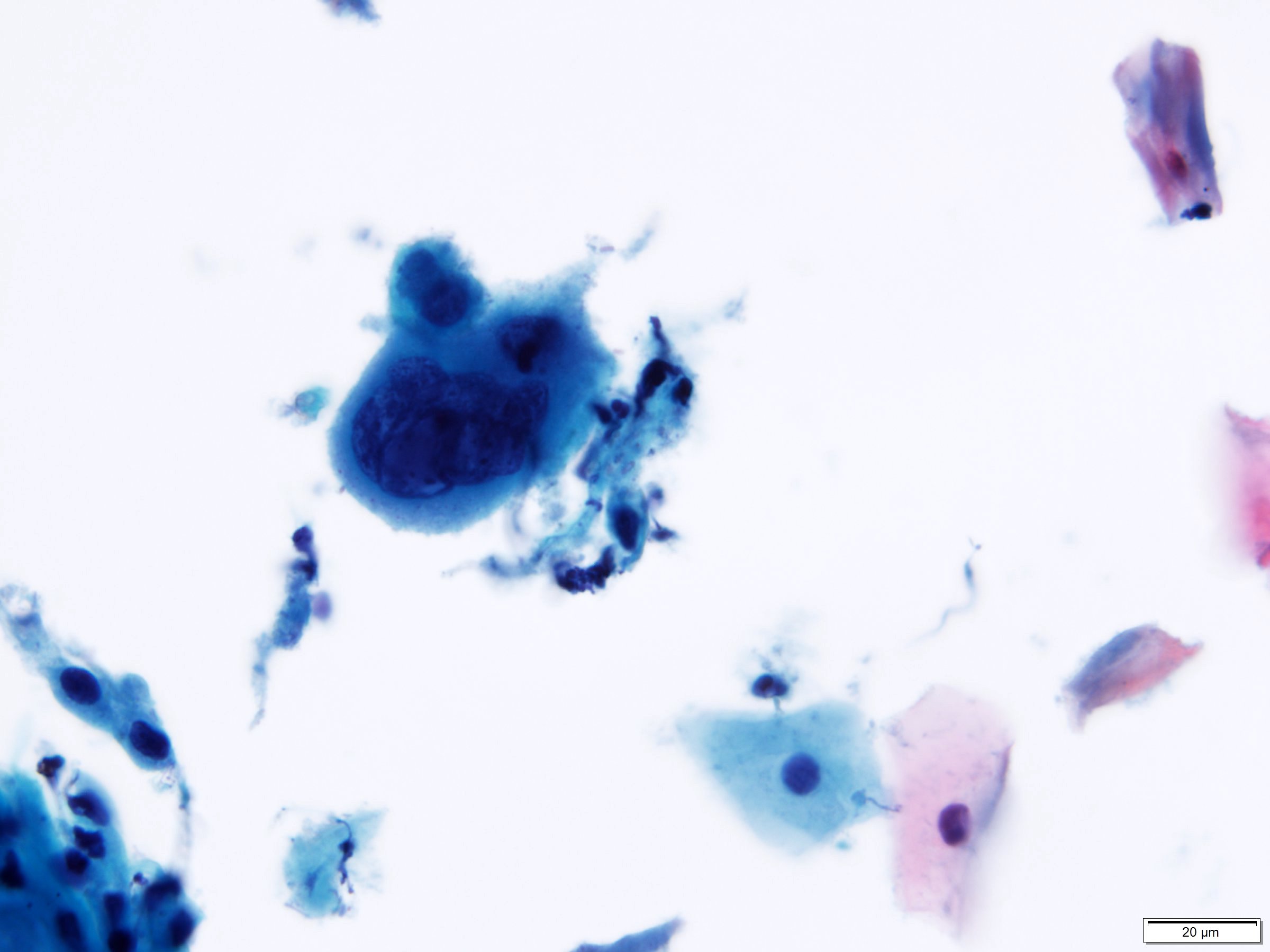
Herpes cytopathic effect
Images hosted on other servers:

WHO digital atlas
Sample pathology report
- Statement of adequacy:
- Satisfactory for evaluation
- Transformation zone component present
- Final interpretation:
- Epithelial cell abnormality, squamous cell
- Low grade squamous intraepithelial lesion (LSIL)
Differential diagnosis
- Pseudokoilocytosis:
- Small perinuclear halo without any significant nuclear abnormality
- Seen in association with reactive / inflammatory conditions like Trichomonas infection
- Glycogen cytoplasmic vacuolization appears yellow, refractile and cracked
- Small perinuclear halo without any significant nuclear abnormality
- Herpes cytopathic effect:
- Early herpes cytopathic effect shows nuclear enlargement and degenerative chromatin but lack other changes of HPV cytopathic effect (koilocytosis)
- Cells with classic features of herpes (multinucleation, nuclear molding, margination of chromatin and clear, ground glass nuclei) will also be present
- Radiation changes:
- Large, bizarre cells with normal N/C ratio
- Binucleation and multinucleation common
- Cytoplasmic vacuolization and polychromasia (2 toned) without perinuclear clearing and peripheral condensation
- Atypical squamous cells of undetermined clinical significance (ASCUS):
- Nuclei approximately 2.5 - 3x the area of the nucleus of a normal intermediate squamous cell or 2x the size of a squamous metaplastic cell nucleus
- Slightly increased N/C ratio
- Minimal nuclear hyperchromasia and irregular chromatin distribution or nuclear shape
- Nuclear abnormalities associated with dense orangeophilic cytoplasm (atypical parakeratosis)
- Cytoplasmic changes suggestive of HPV cytopathic effect (incomplete koilocytosis)
- Reactive endocervical cells:
- Enlarged, polygonal shaped cell with prominent nucleolus and granular cytoplasm
Board review style question #1
Which of the following is the correct interpretation of the cervical cytology shown above from a 32 year old woman?
- Atypical glandular cells, NOS
- Atypical squamous cells of undetermined significance (ASCUS)
- Benign reactive squamous cells
- High grade squamous intraepithelial lesion (HSIL)
- Low grade squamous intraepithelial lesion (LSIL)
Board review style answer #1
Board review style question #2
This routine cervical cytology specimen was obtained from a 33 year old woman. What is the correct interpretation?
- Atypical squamous cells cannot exclude HSIL (ASCH)
- Atypical squamous cells of undetermined significance (ASCUS)
- High grade squamous intraepithelial lesion (HSIL)
- Low grade squamous intraepithelial lesion (LSIL)
- Negative for intraepithelial lesion or malignancy (NILM)
Board review style answer #2
