

Cervix
Benign / nonneoplastic epithelial lesions
Arias Stella reaction
Author: Leonel Maldonado, M.D.

Last author update: 6 March 2006
Last staff update: 5 May 2021
Copyright: 2006-2024, PathologyOutlines.com, Inc.
PubMed search: Arias Stella cervix


Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Case reports | Treatment | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Positive stains | Negative stains | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1Cite this page: Maldonado L. Arias Stella reaction. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/cervixariasstella.html. Accessed November 27th, 2024.
Definition / general
- First described in 1954 by Dr. Javier Arias-Stella (AMA Arch Pathol 1954;58:112)
- Refers to nuclear changes in endocervical glands similar to those in endometrium commonly seen during pregnancy (10%) or postpartum
Essential features
- The main characteristic is cellular enlargement, mainly of the nucleus, to double or many times the normal size; without this feature, the phenomenon cannot be diagnosed
- The cells have abundant clear or oxyphilic cytoplasm and large atypical, hyperchromatic and irregular nuclei with variable chromatin distribution
- Associated with pregnancy (intrauterine or ectopic), oral contraceptive use or trophoblastic disease
Terminology
- Also known as Arias-Stella phenomenon, effect or change
ICD coding
- N88.8: other specified noninflammatory disorders of cervix uteri
- N88.9: noninflammatory disorder of cervix uteri, unspecified
Epidemiology
- The Arias-Stella reaction occurs in the endocervix of pregnant women at a frequency that ranges between 9% and 37.5% (Adv Anat Pathol 2002;9:12)
- The Arias-Stella reaction is seen in women between 19 and 44 years of age
Sites
- Affects glandular cells of the endometrium, but also of the endocervix and fallopian tube
- Can also be seen in other areas or lesions, including endometriosis, endocervical polyps, vaginal adenosis, germinal inclusion cysts of the ovary, paraovarian and paratubal cysts and mucinous cystadenoma (Adv Anat Pathol 2002;9:12, Int J Gynecol Pathol 1982;1:145)
Pathophysiology
- In response to high levels of human chorionic gonadotropin and exposure to estrogens and progesterone stimulation, proliferative (estrogens) and secretory (progesterone) activity occur together, resulting in large, pleomorphic cells with large, hyperchromatic nuclei and prominent nucleoli (Adv Anat Pathol 2002;9:12)
Etiology
- Pregnancy and oral contraceptive use
Clinical features
- Almost always associated with pregnancy (either intrauterine or ectopic) or with trophoblastic disease; it rarely occurs secondary to hormone therapy, especially progestins
- Arias-Stella reaction in the cervix can present as involvement of an endocervical polyp or as an incidental finding in cervical tissue obtained for other reasons
Case reports
- 25 year old pregnant woman with Arias-Stella reaction in bladder endometriosis (Pathol Res Pract 2009;205:653)
- 33 year old woman with Arias-Stella reaction in pap smear due to uterine adenomyomatomatous polyp (Acta Obstet Gynecol Scand 2007;86:106)
- 35 year old woman with Arias-Stella reaction due to cervical pregnancy (Acta Cytol 1994;38:218)
- Cervicovaginal smear of nonpregnant woman undergoing infertility treatment with clomiphene and beta-hCG (Diagn Cytopathol 2005;32:94)
Treatment
- Arias-Stella changes disappear after pregnancy
Gross description
- A significant number of cases present with a polyp (Am J Surg Pathol 2004;28:608)
Microscopic (histologic) description
- Main characteristic is cellular enlargement, mainly of the nucleus, to double or many times the normal size; without this feature, the phenomenon cannot be diagnosed (Am J Surg Pathol 2004;28:608)
- The glandular cells are large with abundant clear or oxyphilic cytoplasm and large atypical, hyperchromatic nuclei demonstrating irregularity of the nuclear contour and variability of the chromatin distribution, ranging from even to dense
- Nuclei typically protrude into the gland lumen, giving the cell a hobnail appearance
- Intraglandular proliferation can be striking, producing a papillary or cribriform pattern
- Rare mitotic figures can be seen
- Tissue specimens will often show other features associated with gestation, such as decidual change
- It is most commonly seen in the upper endocervical canal but can involve glands anywhere in the endocervix
- Affects superficial or deep glands; tends to be focal, but may be extensive, producing a confluent appearance
- Five histologic variants reported (Adv Anat Pathol 2002;9:12):
- Minimal atypia: nuclear enlargement is minimal and occurs in limited foci; usually at the beginning of gestation
- Early secretory pattern: resembles normal early secretory endometrium with subnuclear or subnuclear / supranuclear vacuoles
- Secretory or hypersecretory pattern: the classically recognized pattern; glandular cells with intense and diffuse cytoplasmic vacuolization; enlarged and hyperchromatic nuclei are usually pyknotic
- Regenerative, proliferative or nonsecretory pattern: no or minimal evidence of secretory activity; enlarged nuclei show a vesicular configuration or a granular chromatin with a well delineated nuclear membrane
- Monstrous cell pattern: usually focal, with giant and bizarre nuclei, which involve all the cells in the glands
Microscopic (histologic) images
Contributed by Leonel Maldonado, M.D.
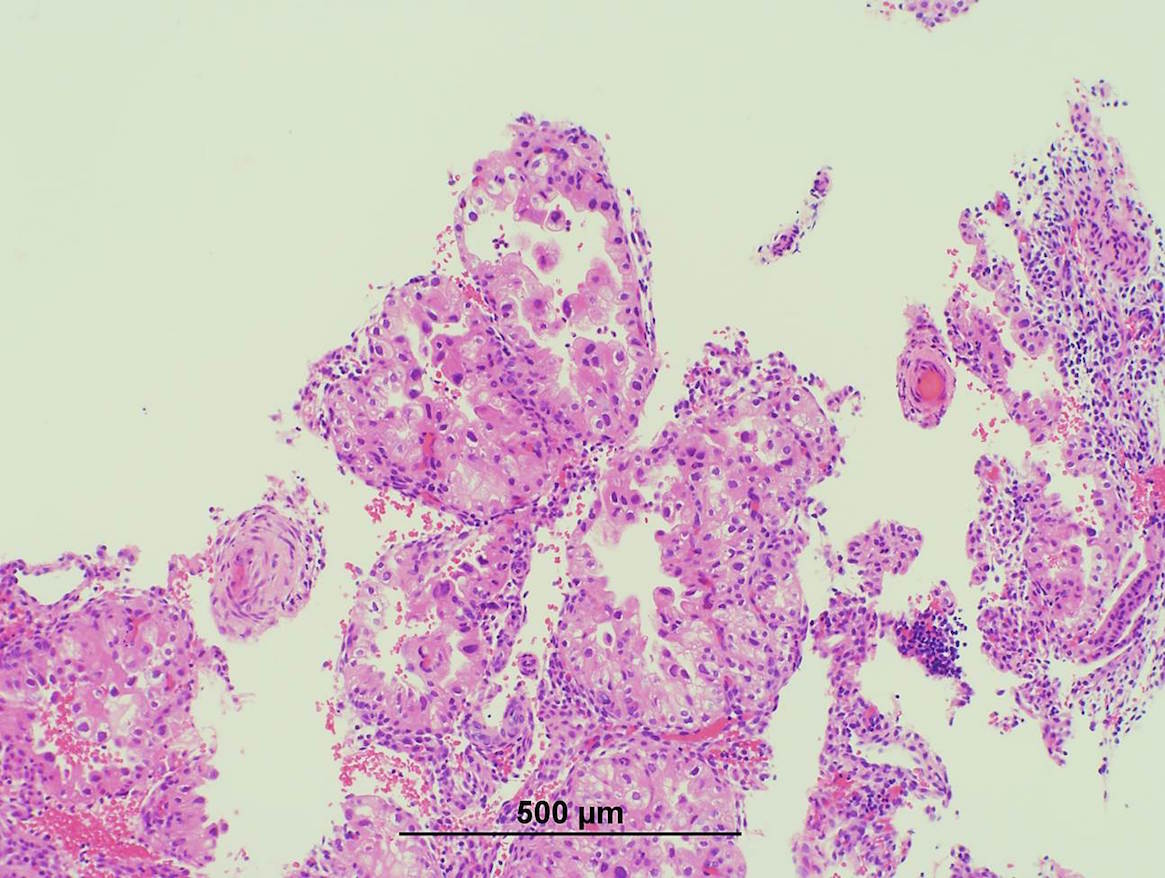
Arias-Stella reaction, 10×
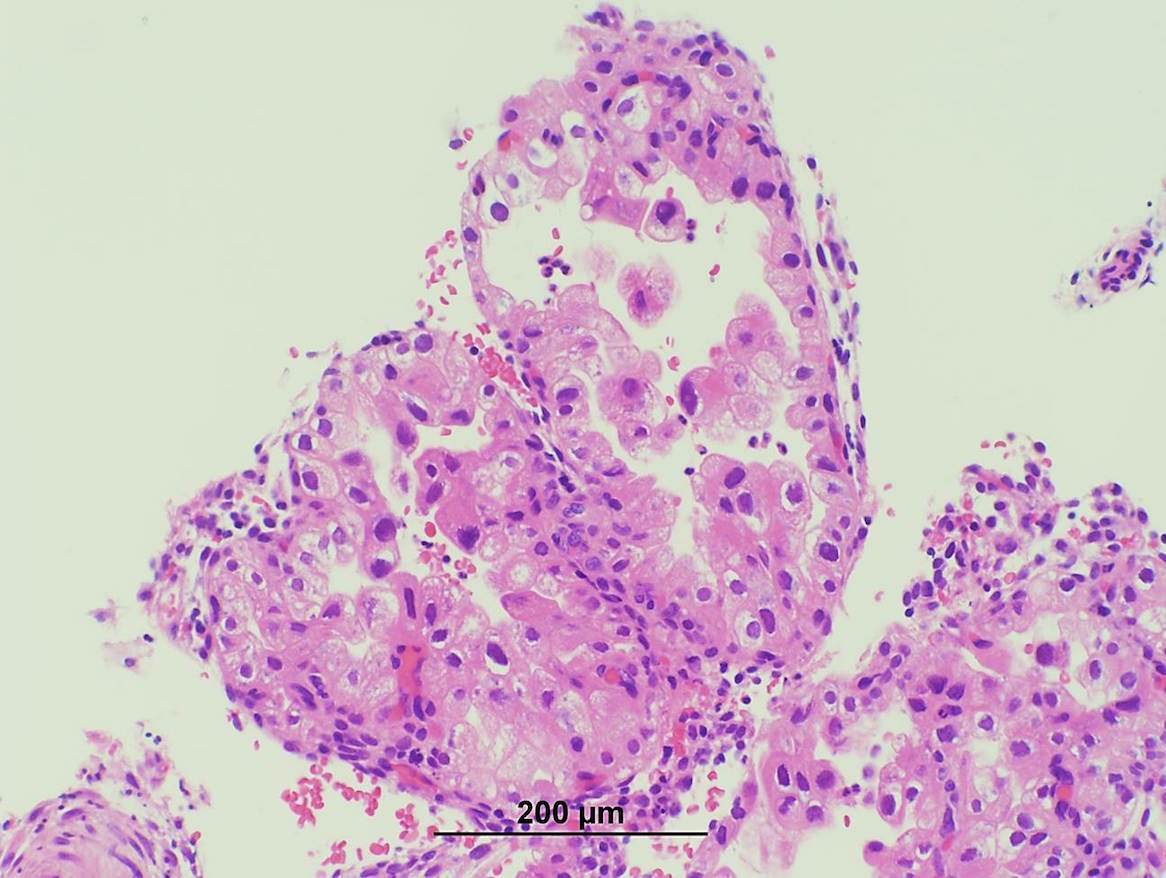
Arias-Stella reaction, 20×
Cytology description
- Arias-Stella reaction is uncommonly seen in Pap smears
- Often overdiagnosed as SIL, but pregnant women with atypical glandular lesions (AGUS) may have SIL on subsequent biopsy (Acta Cytol 2001;45:294)
- Characterized by large, pleomorphic cells with large, hyperchromatic, eccentrically located nuclei with fine to granular chromatin and prominent nucleoli (can be multiple)
- The cytoplasm is abundant and pale, fine to coarsely vacuolated and PAS positive
- No stratification or crowding occurs
- Arias-Stella cells are polyploid (but not aneuploid)
- Mitotic figures and intranuclear cytoplasmic invaginations may be seen
Negative stains
- Wild type p53
Differential diagnosis
- Clear cell carcinoma: forms a mass, has desmoplasia, is infiltrative with irregular glandular distribution, uniformly marked cytologic atypia, high N / C ratio, mitotic activity (Am J Surg Pathol 2004;28:608)
- In contrast to clear cell carcinoma, Arias-Stella reaction shows low rates of Ki67 nuclear reactivity and do not overexpress p53 (i.e. they have wild type p53 expression)
- Radiation or chemotherapy induced changes
- Serous papillary carcinoma
- HPV related / endocervical adenocarcinoma
Additional references
Board review style question #1
The colposcopic examination of a 32 year old female with heavy menstrual bleeding showed an abnormal transformation zone. A cervical biopsy was performed and the histologic findings are shown below:
-
The main histologic characteristic needed for the diagnosis of this condition is
- Abundant clear cytoplasm
- Cellular enlargement, mainly of the nucleus, many times the normal size
- Hyperchromatic, irregular nuclei with variable chromatin distribution
- Its involvement of the glands in the endocervical canal
- Its papillary architecture
Board review style answer #1
B. Cellular enlargement, mainly of the nucleus, many times the normal size
Comment Here
Reference: Arias Stella reaction
Comment Here
Reference: Arias Stella reaction

