

Cervix
Other epithelial tumors
Adenoid cystic carcinoma
Author: Carlos Parra-Herran, M.D.

Last author update: 1 April 2017
Last staff update: 17 May 2021
Copyright: 2007-2024, PathologyOutlines.com, Inc.
PubMed Search: Adenoid cystic carcinoma cervix


Table of Contents
Definition / general | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Cytology images | Positive stains | Negative stains | Electron microscopy description | Molecular / cytogenetics description | Differential diagnosis | Additional referencesCite this page: Parra-Herran C. Adenoid cystic carcinoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/cervixadenoidcystic.html. Accessed December 26th, 2024.
Definition / general
- Uncommon (less than 1% of primary cervical adenocarcinomas), occurs in elderly, black women with multiple pregnancies
- Recently characterized by Xing et al, who divide adenoid cystic carcinomas of the lower female genital tract (cervix and vulva) in two distinct groups (Am J Surg Pathol 2016;40:529):
| Pure adenoid cystic carcinoma | Mixed carcinoma with adenoid cystic differentiation | |
|---|---|---|
| Patient age | Median 48 years, range 27 - 74 | Median 76 years, range 50 - 86 |
| Adenoid cystic component | 100% | Usually < 25% |
| High risk HPV | Not detected | Detected (usually HPV16) |
| p16 immunohistochemistry | Nondiffuse | Diffuse and strong |
| Perineural invasion | ~50% | Absent |
- Poor prognosis due to frequent local recurrences and distant metastases in approximately 50% of cases (Am J Surg Pathol 1988;12:134)
- Adenoid cystic carcinoma may be a component of a mixed malignant lesion; commonly admixed with squamous cell carcinoma, adenoid basal carcinoma and even carcinosarcoma (Am J Surg Pathol 2001;25:338)
Case reports
- 83 year old white woman with cervical mass (Arch Pathol Lab Med 2004;128:817)
Treatment
- Surgery is the primary form of treatment, if early stage
- Complete excision is required to exclude the possibility of a second component (squamous cell or adenoid basal carcinomas)
- Radiotherapy and chemotherapy in elderly or advanced stage
Gross description
- Irregular, polypoid, friable cervical mass
Gross images
Contributed by Ihab Hosny, M.D.


Various images
Microscopic (histologic) description
- Adenoid cystic carcinoma of the uterine cervix displays the same morphologic features of its counterparts in the salivary gland, larynx / trachea / lung, breast and vulva
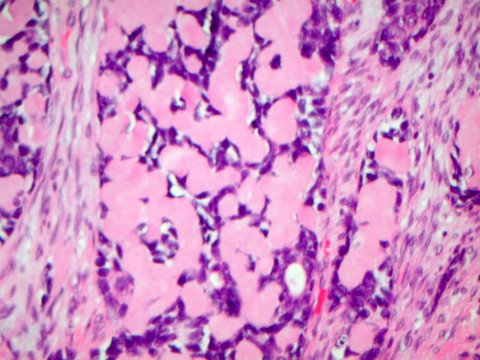
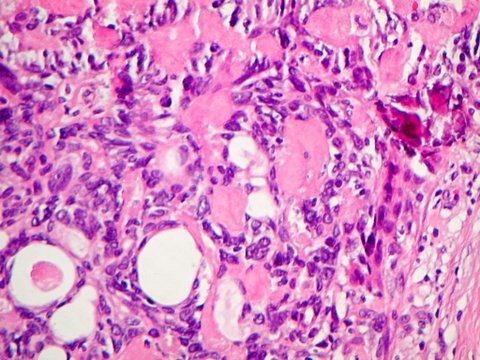
- The tumor is composed of basaloid cells arranged in cribriform, tubular and solid growth patterns
- Tumors with cribriform architecture have cystic areas containing mucinous or eosinophilic secretions, alternating with pseudocystic areas containing basement membrane-like material [positive for collage type IV and periodic acid-Schiff (PAS) stain] (Am J Surg Pathol 1999;23:448)
- Tumors with solid growth also have basement membrane-like material around tumor nests and cords (IInt J Gynecol Pathol 1992;11:2)
Microscopic (histologic) images
AFIP images
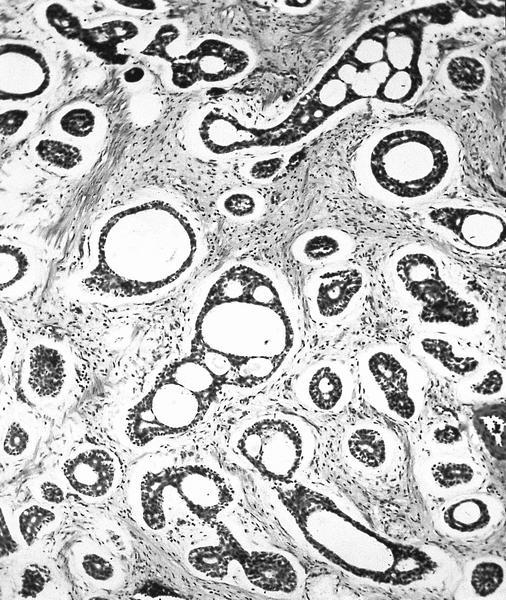
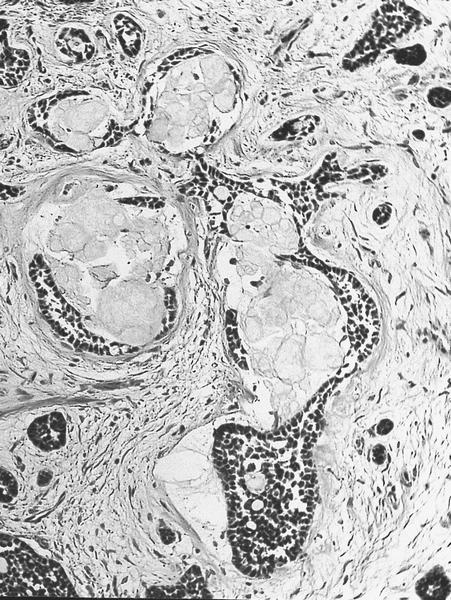
Cribriform architecture and basement membrane material
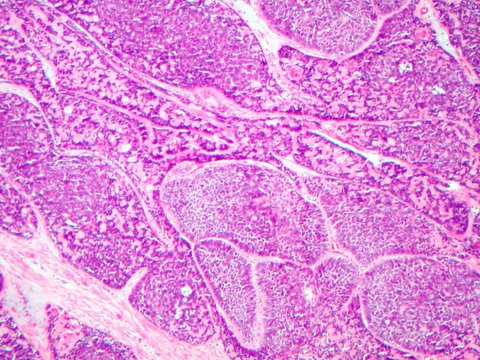
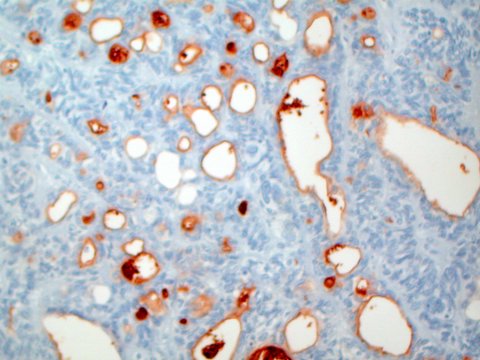
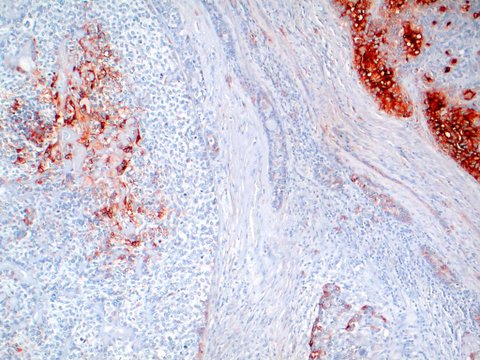
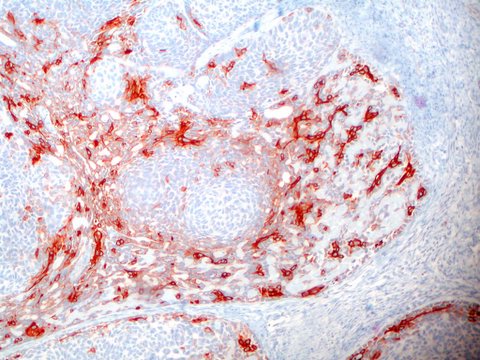
Contributed by Carlos Parra-Herran, M.D.

Contributed by Ihab Hosny, M.D.

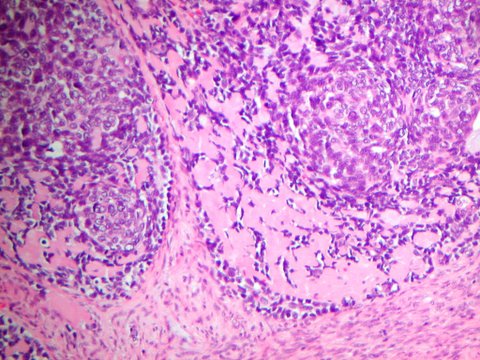

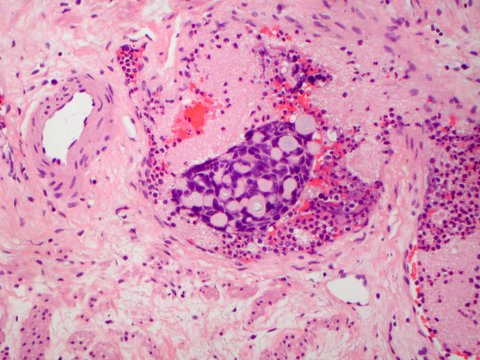
Vascular invasion

Actin
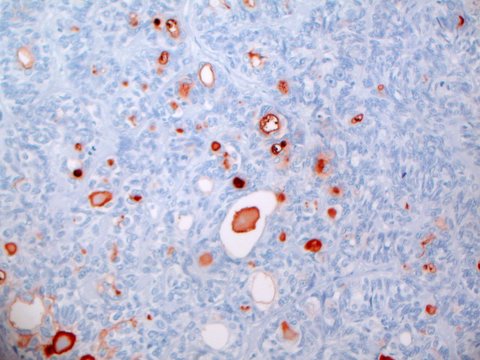
CEA
EMA
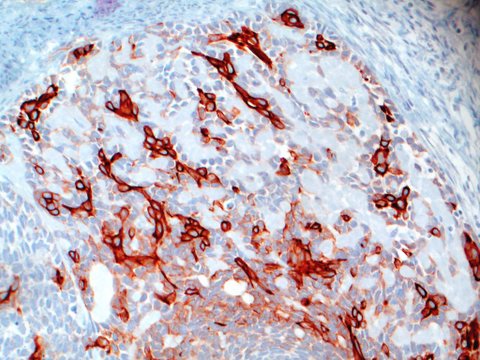
High molecular weight keratin
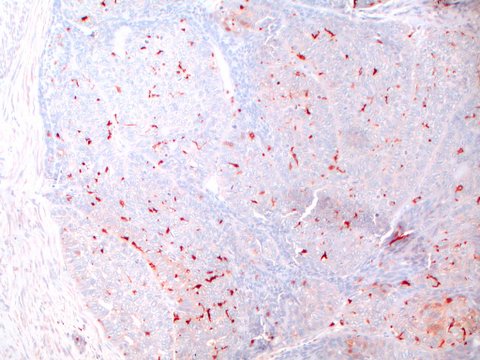
S100
Cytology description
- Three dimensional clusters of tumor cells forming small acini or glandular patterns in a necrotic background (J Pathol Transl Med 2015;49:396)
- Nuclei have variable size, are hyperchromatic with irregular and angulated membranes and coarse chromatin, which may surround opaque orangeophilic contents (Acta Cytol 2010;54:1039, Coll Antropol 2010;34:233)
- Dysplastic or malignant squamous cells may be present (Acta Cytol 1996;40:1304)
Cytology images
Images hosted on other servers:

Three dimensional structures
Positive stains
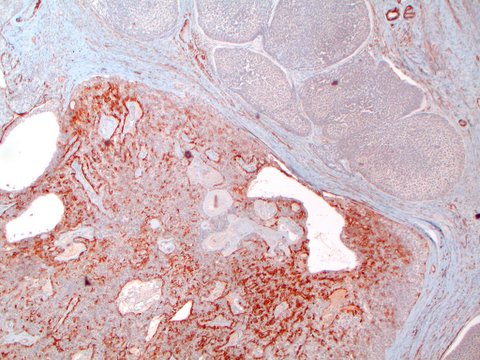
- Keratin, type IV collagen, laminin (extracellular basement membrane), HHF35, focal CEA and EMA
- CD117 (c-kit): can be focal (Int J Gynecol Pathol 2012;31:25)
- Myoepithelial markers (S100, p63)
- MYB expression has been recently reported (Diagn Pathol 2015;10:145)
Negative stains
Electron microscopy description
- Redundant basal lamina forming pseudocysts, intercellular spaces and occasional true lumens with microvilli (Am J Clin Pathol 1982;77:494)
Molecular / cytogenetics description
- A subset of cases is positive for high risk HPV, particularly HPV16+ (J Clin Pathol 1996;49:805)
- NFIB gene rearrangements, described in adenoid cystic carcinomas in salivary glands, breast and vulva, have not been documented in the cervix yet (Int J Gynecol Pathol 2017;36:289)
Differential diagnosis
- Adenoid basal carcinoma: no intraluminal hyaline material, smaller and less pleomorphic nuclei, usually no type IV collagen or laminin (Am J Surg Pathol 1999;23:448)
- Both lesions can coexist
- Adenoid cystic carcinoma has more nuclear atypia, expansile growth pattern, distinct stromal reaction and necrosis; mitotic figures, angiolymphatic invasion and hyalinized stroma are common
Additional references

