CD Markers
CD61

Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: CD61
CD61
Author: Pamela Wirth, Ph.D.
Board of reviewers: Frido Bruehl, M.D.
Editorial Board Member: Christian M. Schürch, M.D., Ph.D.
Last author update: 27 February 2024
Last staff update: 27 February 2024
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: CD61
Table of Contents
Definition / general | Essential features | Terminology | Pathophysiology | Diagrams / tables | Clinical features | Interpretation | Uses by pathologists | Prognostic factors | Microscopic (histologic) description | Microscopic (histologic) images | Positive staining - normal | Positive staining - disease | Negative staining | Molecular / cytogenetics description | Sample pathology report | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Wirth P. CD61. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/cdmarkerscd61.html. Accessed March 30th, 2025.
Definition / general
- Membrane glycoprotein that associates with CD41 to form a heterodimeric complex (CD61 / CD41); dominant integrin on platelets that is essential for normal platelet function (J Hematol Oncol 2019;12:26)
- CD61 binds to several matrix proteins, including fibrinogen, which is important to blood clotting (Alberts: Molecular Biology of the Cell, 4th Edition, 2002)
Essential features
- CD61, also known as GP3A and β3 integrin, is an adhesion receptor on the membrane of cells with a megakaryocytic lineage (Histol Histopathol 2002;17:347, F1000Res 2016;5:F1000)
- CD61 forms heterodimer with CD41 known as glycoprotein IIb - IIIa complex
- CD61 is encoded by ITGB3 gene
- Dominant integrin on platelets and is highly expressed
- Important mediator of platelet aggregation
- Activated glycoprotein IIb - IIIa complex binds fibrinogen or von Willebrand factor to bridge platelets together
- CD61 is encoded by ITGB3 gene
- CD61 can promote invasion and migration in tumors (Am J Transl Res 2019;11:7195)
Terminology
- β3 integrin (ITGB3)
- Integrin subunit beta 3
- GP3A
Pathophysiology
- Platelet aggregation is mediated by binding of fibrinogen to sites on the glycoprotein IIb - IIIa receptor complex (Biochem J 1995;309:613)
- Hereditary defect of glycoprotein IIb - IIIa receptor complex causes Glanzmann thrombasthenia, an autosomal recessive bleeding disorder (Transfus Med Rev 2016;30:92)
- TGFβ is the main upstream factor of integrins and when elevated, leads to increased levels of mesenchymal-like cancer cells (Am J Transl Res 2019;11:7195)
Diagrams / tables
Images hosted on other servers:

Superfamily of integrins
Clinical features
- Expressed on macrophages, endothelial cells, fibroblasts, megakaryocytes, osteoclasts, mast cells and platelets
- Present in normal tissue and tumors (Histol Histopathol 2002;17:347)
Interpretation
- Membrane, intracellular
- Cytoplasmic expression in megakaryocytes and platelets
Uses by pathologists
- Identify platelets, megakaryocytes and platelet thrombi
- Count platelets in thrombocytopenic patients (Br J Haematol 2001;112:584)
Prognostic factors
- CD61 upregulation is related to poor survival on non-small cell lung cancer, breast cancer, cervical cancers, pancreatic ductal adenocarcinomas, T cell acute lymphoblastic leukemia and gliomas (Transl Lung Cancer Res 2019;8:323, Am J Transl Res 2019;11:7195, Commun Biol 2021;4:490)
Microscopic (histologic) description
- CD61 is expressed on platelets, megakaryocytes, monocytes, macrophages and endothelial cells (Barclay: The Leucocyte Antigen Factsbook, 2nd Edition, 1997)
- CD41 interacts with CD61 to form the glycoprotein IIb - IIIa receptor complex
- Expressed on platelets and megakaryocytes
- CD41 interacts with CD51 to form the vitronectin receptor
- Expressed on endothelial cells, monocytes, platelets and osteoclasts
- CD41 interacts with CD61 to form the glycoprotein IIb - IIIa receptor complex
Microscopic (histologic) images
Contributed by Pamela Wirth, Ph.D. (sources: University of Toronto and Human Protein Atlas)
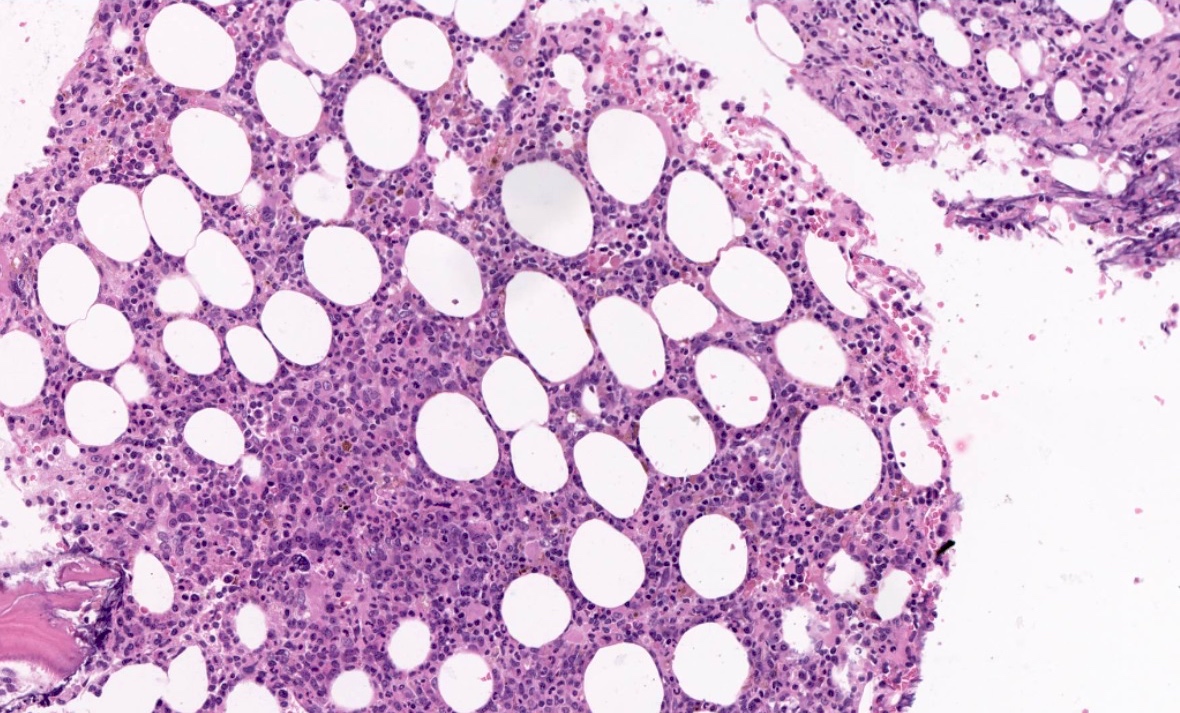
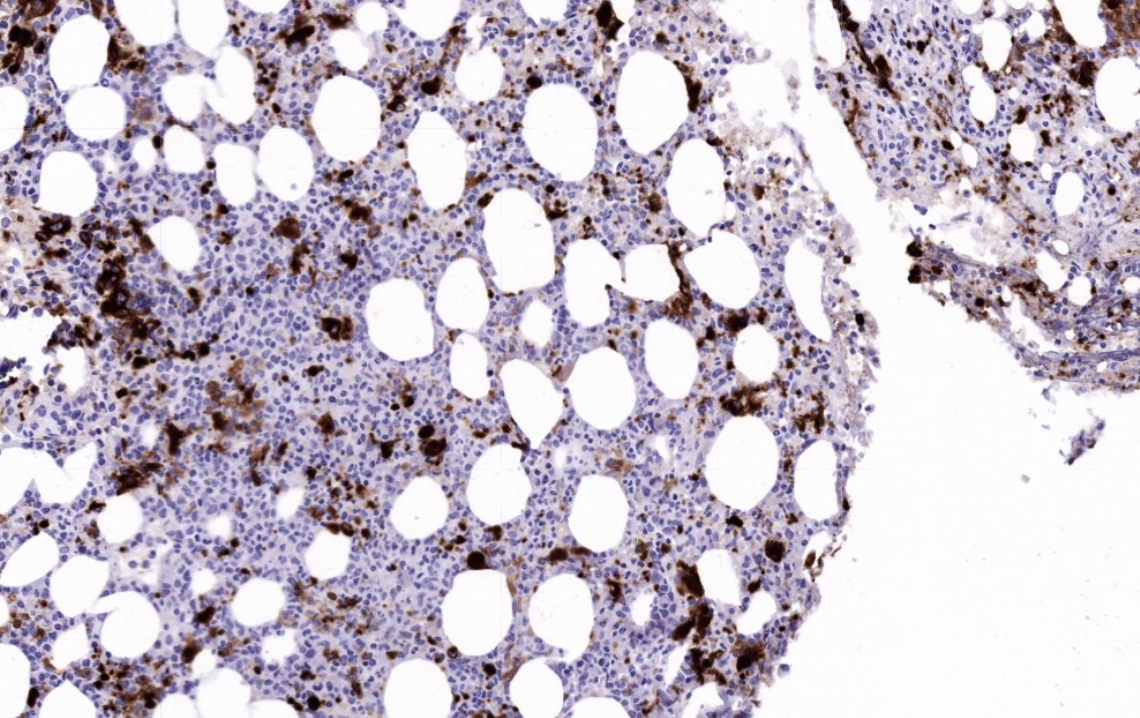
Bone marrow biopsy
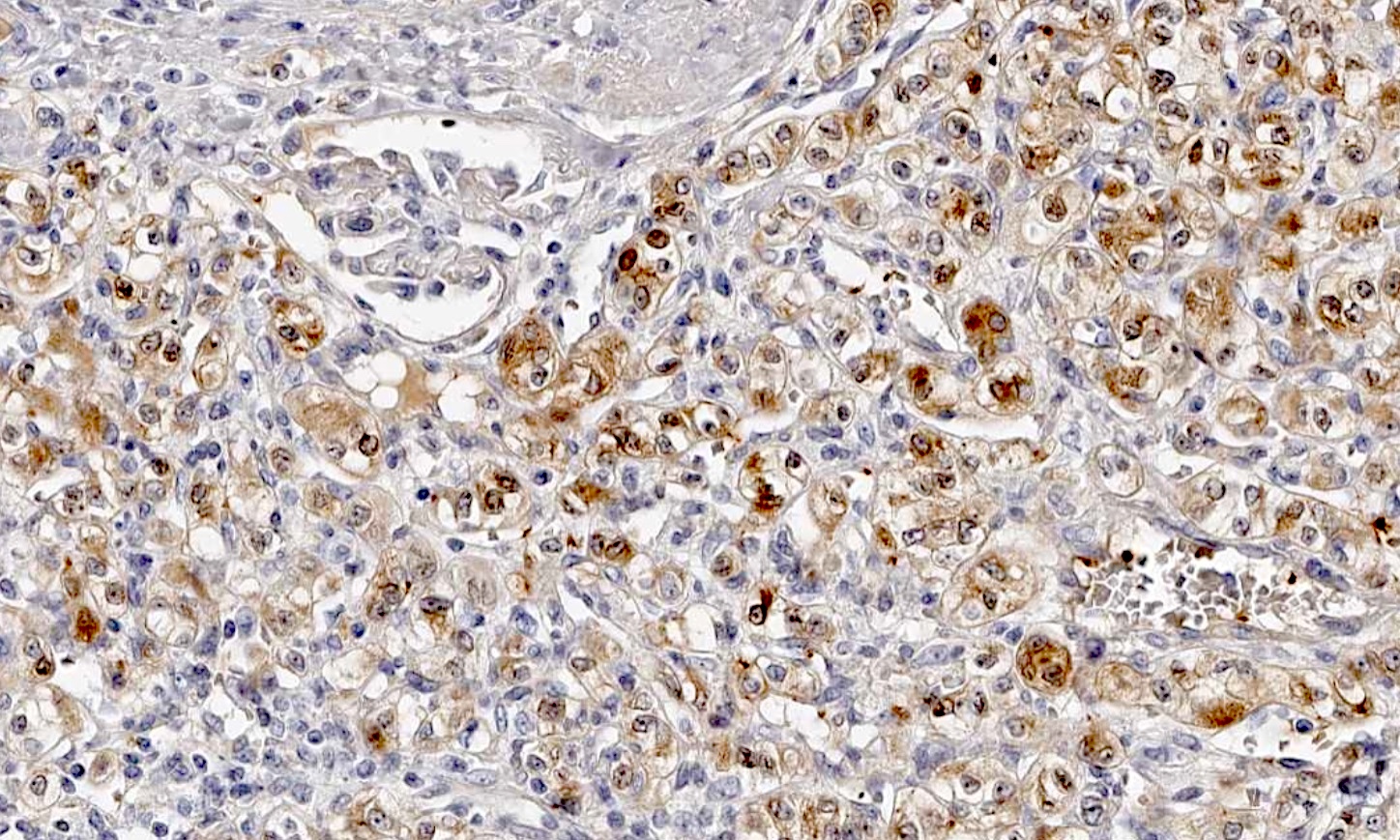
Liver
cholangiocarcinoma
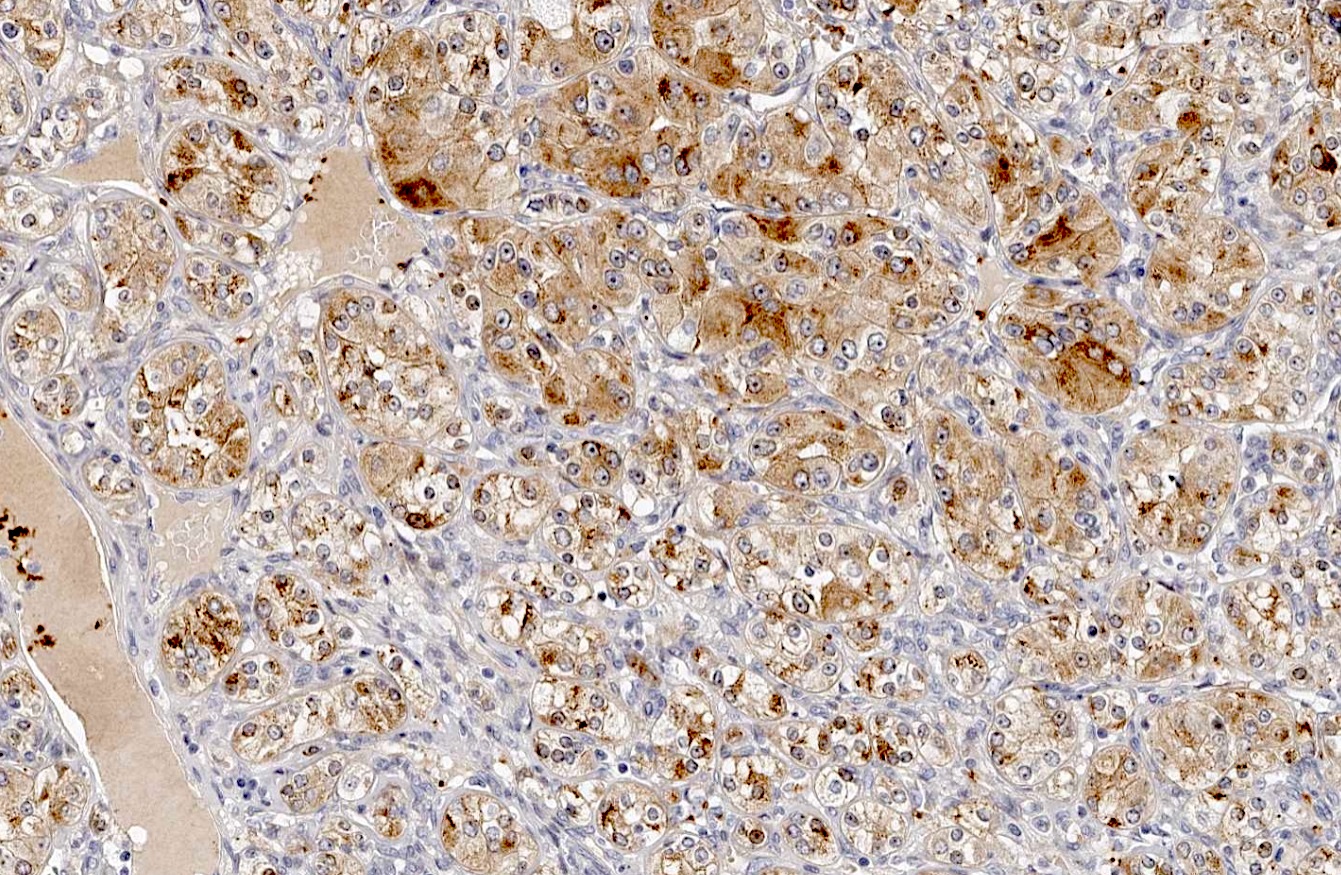
Kidney adenocarcinoma
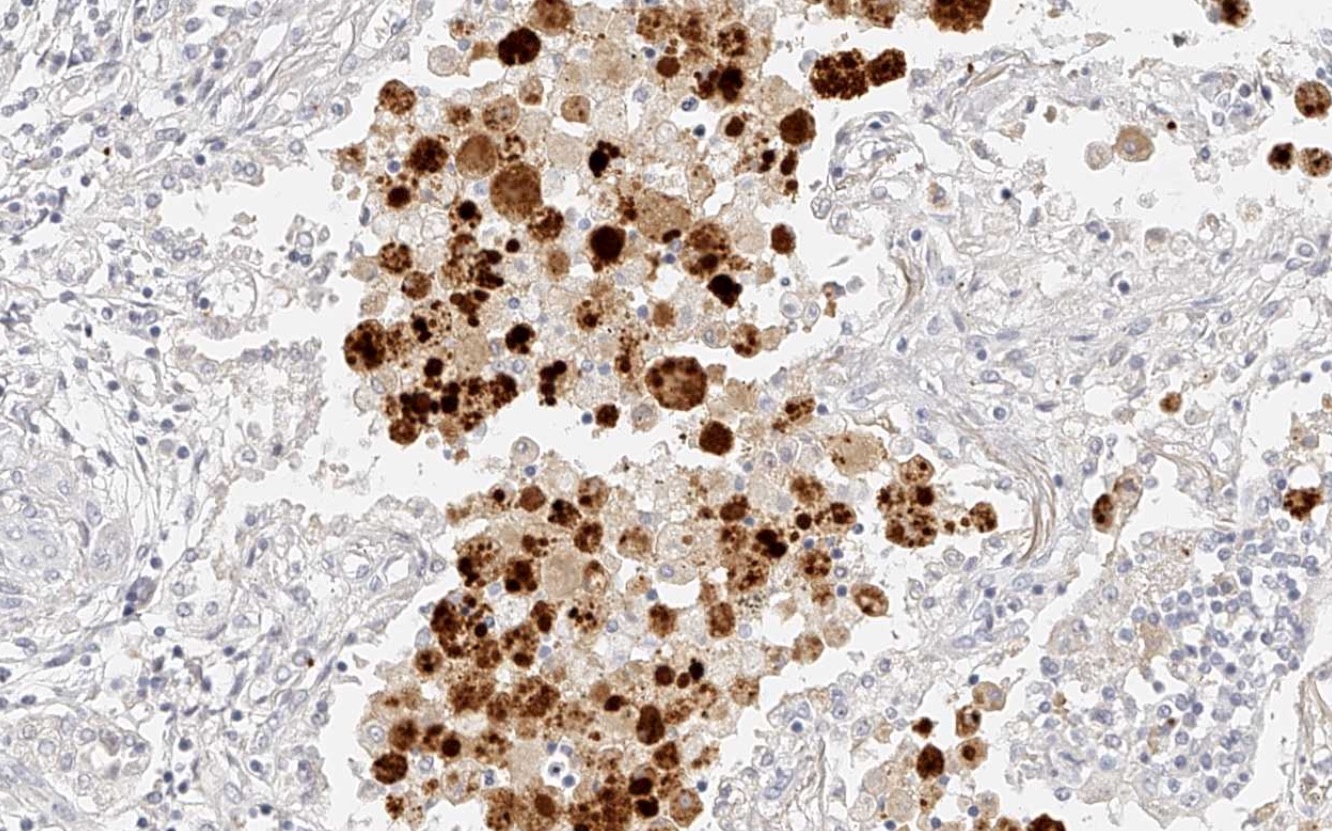
Lung squamous cell carcinoma
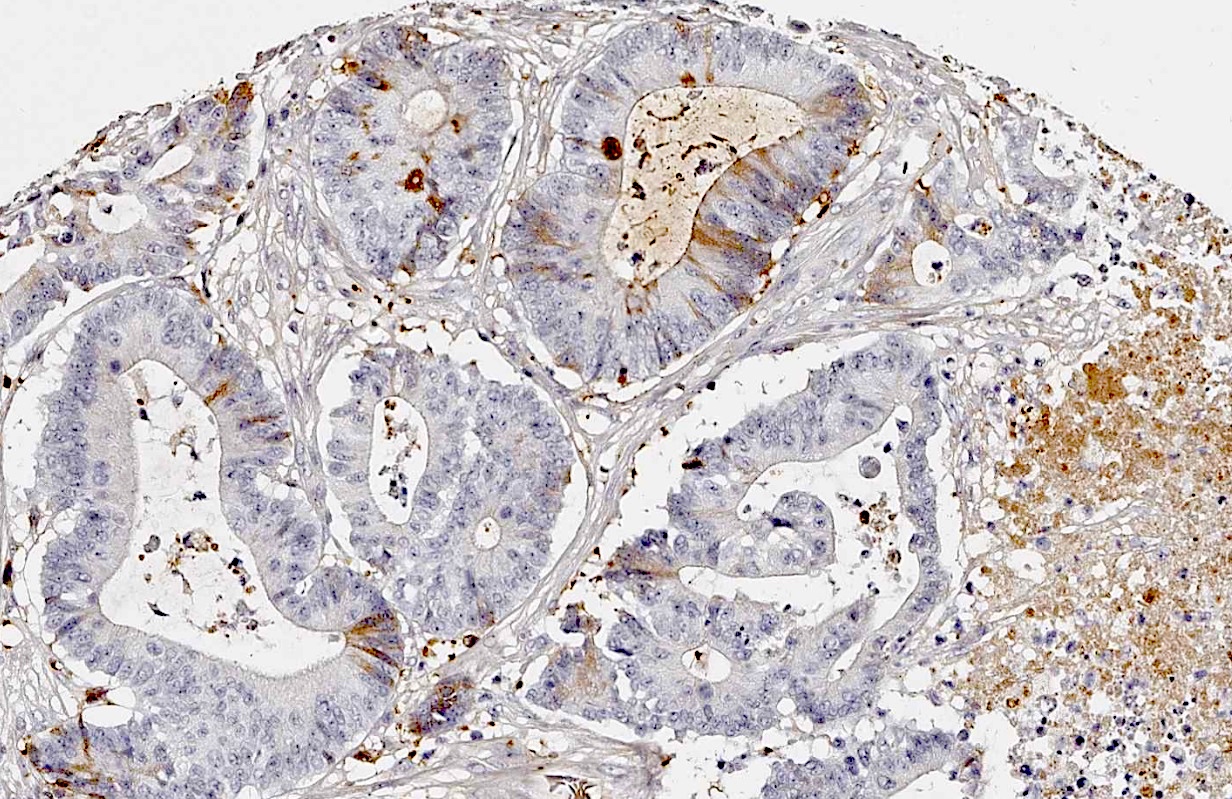
Colon carcinoma
Positive staining - normal
- Cytoplasmic staining of normal and abnormal megakaryocytes, platelets, occasional endothelial cells, some myeloid precursor cells
Positive staining - disease
- Useful in identifying micromegakaryocytes, abnormal megakaryocytes and megakaryoblasts in cases of acute megakaryoblastic leukemia, myeloproliferative disorders and myelodysplastic syndromes (Am J Clin Pathol 2018;150:461, Virchows Arch B Cell Pathol Incl Mol Pathol 1992;62:275)
- CD61 may assist in marking tumor associated thrombi in follicular thyroid carcinoma in order to distinguish true vascular invasion from mimics (Head Neck Pathol 2020;14:399)
- Identification of microthrombi in renal biopsies from patients with lupus nephritis and those receiving calcineurin inhibitor therapy (Head Neck Pathol 2020;14:399)
Negative staining
- Acute myeloid leukemia without maturation (AML M0 - M6) (Arch Pathol Lab Med 2011;135:44)
Molecular / cytogenetics description
- Glanzmann thrombasthenia is caused by a defect in the platelet integrin receptor essential to platelet aggregation and hemostasis
- Mutations involve missense, nonsense, frameshift or point mutations in ITGA2B or ITGB3 genes located on chromosome 17q21 (Orphanet J Rare Dis 2006;1:10)
Sample pathology report
- Bone marrow aspirate:
- Acute leukemia of ambiguous lineage, NOS (see comment)
- Comment: A 68 year old man presented with suspected leukemia. Bone marrow aspiration revealed 85% blasts with positive expression for CD34, CD7, TdT, CD33, CD117 and CD61, while being negative for MPO, CD19, CD22, CD79a and CD3.
Board review style question #1
An infant is evaluated for bleeding of the gums and ongoing nose bleeds. A complete blood count comes back with normal platelet count but prolonged bleeding time. Evaluation by flow cytometry and IHC indicates markedly decreased CD41 and CD61. Genetic sequencing indicated mutated ITGA2B. What is the most likely diagnosis?
- Factor V Leiden
- Glanzmann thrombasthenia
- Hemophilia B (characterized by deficiency in factor VIII or IX, caused by X linked recessive trait)
- Von Willebrand disease
Board review style answer #1
B. Glanzmann thrombasthenia. Significantly decreased levels of CD41 and CD61 is diagnostic for Glanzmann thrombasthenia. Answer A is incorrect because factor V Leiden involves a mutated F5 gene resulting in thrombophilia. Answer C is incorrect because hemophilia B is caused by an X linked recessive trait, not a mutated ITGA or ITGB gene. Answer D is incorrect because von Willebrand disease is caused by variants in the VWF gene.
Comment Here
Reference: CD61
Comment Here
Reference: CD61
Board review style question #2
CD61 assists in the identification of which cell type?
- Granulocytes
- Megakaryocytes
- Plasma cells
- T cells
Board review style answer #2
B. Megakaryocytes. CD61 is a glycoprotein found on megakaryocytes, platelets and their precursors. Answer A is incorrect because granulocytes are identified by CD66b. Answer C is incorrect because plasma cells are distinguished by their expression of CD38 and CD138. Answer D is incorrect because other CD markers such as CD3, CD4 and CD8 are used to identify this cell type.
Comment Here
Reference: CD61
Comment Here
Reference: CD61
