
Breast
Inflammatory / infectious
Silicone leak / lymphadenopathy
Authors: Maria A. Arafah, M.D., Afaf M. Alsharhan, M.D.
Editorial Board Members: Gary Tozbikian, M.D., Julie M. Jorns, M.D.


Last author update: 18 May 2021
Last staff update: 25 April 2023
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Silicone breast implants


Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Virtual slides | Cytology description | Positive stains | Negative stains | Electron microscopy description | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Arafah MA, Alsharhan AM. Silicone leak / lymphadenopathy. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/breastsiliconebreastimplants.html. Accessed April 1st, 2025.
Definition / general
- Foreign body inflammatory reaction induced by silicone
- Diffuse in the breast → silicone mastitis
- Nodular in the breast → silicone granulomas
- Leakage to regional lymph nodes → silicone lymphadenitis
Essential features
- Complication of leakage or rupture of silicone containing breast prosthesis or as a reaction to silicone injection
- Foreign body inflammatory reaction induced by silicone
- Most common sites: breast, regional lymph nodes
Terminology
- Silicone granuloma
- Silicone mastitis
- Silicone lymphadenopathy
ICD coding
Epidemiology
- Incidence rates vary between manufactures and radiological detection methods (Gland Surg 2017;6:163):
- 10 year incidence for Allergan round: 9.3% (primary augmentation) and 35.4% (primary / revision reconstruction) (Plast Reconstr Surg 2014;133:1354)
- 10 year incidence for Allergan shaped: 17.7% (primary augmentation) and 12.4% (primary reconstruction) (Aesthet Surg J 2015;35:145)
- 6 year incidence for Mentor round: 1.1% (primary augmentation) and 3.8% (primary reconstruction) (Aesthetic Plast Surg 2009;33:440)
- 6 year incidence for Mentor shaped: 2.1% (primary augmentation) and 1.5% (primary reconstruction) (Plast Reconstr Surg 2012;129:1381)
- 8 year incidence for Sientra: 6.4% (primary augmentation) and 2.8% (primary reconstruction) (Aesthet Surg J 2016;36:404)
Sites
- Breast and regional lymph nodes
Pathophysiology
- See etiology
Clinical features
- In breast:
- Breast implant rupture is often clinically silent (Ann Plast Surg 2005;54:583)
- Palpable masses
- Change in breast size, shape or firmness
- Breast pain
- Induration of skin, draining sinuses, deformity
- In lymph nodes:
- Incidental finding
- Painful or enlarged lymph nodes:
- Axillary (Breast J 2020;26:1821)
- Internal mammary (J Med Imaging Radiat Oncol 2021;65:216)
- Cervical (Ann R Coll Surg Engl 2016;98:e118)
Diagnosis
- Can be suspected clinically and radiologically
- Histopathology is the gold standard for a definitive diagnosis
Radiology description
- Mammography: radiopaque silicone outside the implant shell in the breast or lymph nodes with or without irregular and coarse calcifications
- Ultrasound: extracapsular silicone in the breast or lymph nodes (snowstorm sign) (Indian J Radiol Imaging 2016;26:216)
- Magnetic resonance imaging: high signal intensity deposits in the breast or lymph nodes
Radiology images
Images hosted on other servers:

Rupture of silicone implant (mammography)

Snowstorm sign (ultrasound)

Extracapsular free silicone conglomerates (MRI)
Case reports
- 34 year old woman with silicone breast implant associated fibromatosis (J Surg Case Rep 2018;2018:rjy249)
- 35 year old woman with extensive silicone lymphadenopathy mimicking lymphoma (Ann Surg Treat Res 2017;93:331)
- 39 year old woman with pericarditis after breast implant rupture (Cardiol Res 2018;9:381)
- 45 year old woman with silicone nipple discharge (Int J Surg Case Rep 2020;74:73)
- 57 year old woman with silicone implant incompatibility syndrome (BMJ Case Rep 2017;2017:bcr2016218709)
- 58 year old woman with breast implant associated anaplastic large cell lymphoma (Case Rep Hematol 2018;2018:2414278)
- 72 year old woman with silicone granuloma associated with pectoral muscle involvement (Eur J Breast Health 2018;14:54)
Treatment
- Replacement of the prosthesis with removal of the surrounding contracture (Clin Plast Surg 2021;48:1)
- Excision of enlarged masses or lymph nodes caused by migration of silicone (Am J Med 2018;131:1383)
- Total mastectomy to control significant inflammatory or cosmetic complications (Indian J Plast Surg 2015;48:317)
Gross description
- Firm to hard nodular surface, gritty if there is calcification (Insights Imaging 2018;9:59)
- Cystic spaces containing thick pale yellow or white material
Gross images
Contributed by Debra L. Zynger, M.D.

Breast mass
Images hosted on other servers:

Fibrous capsule

Silicone lymphadenopathy
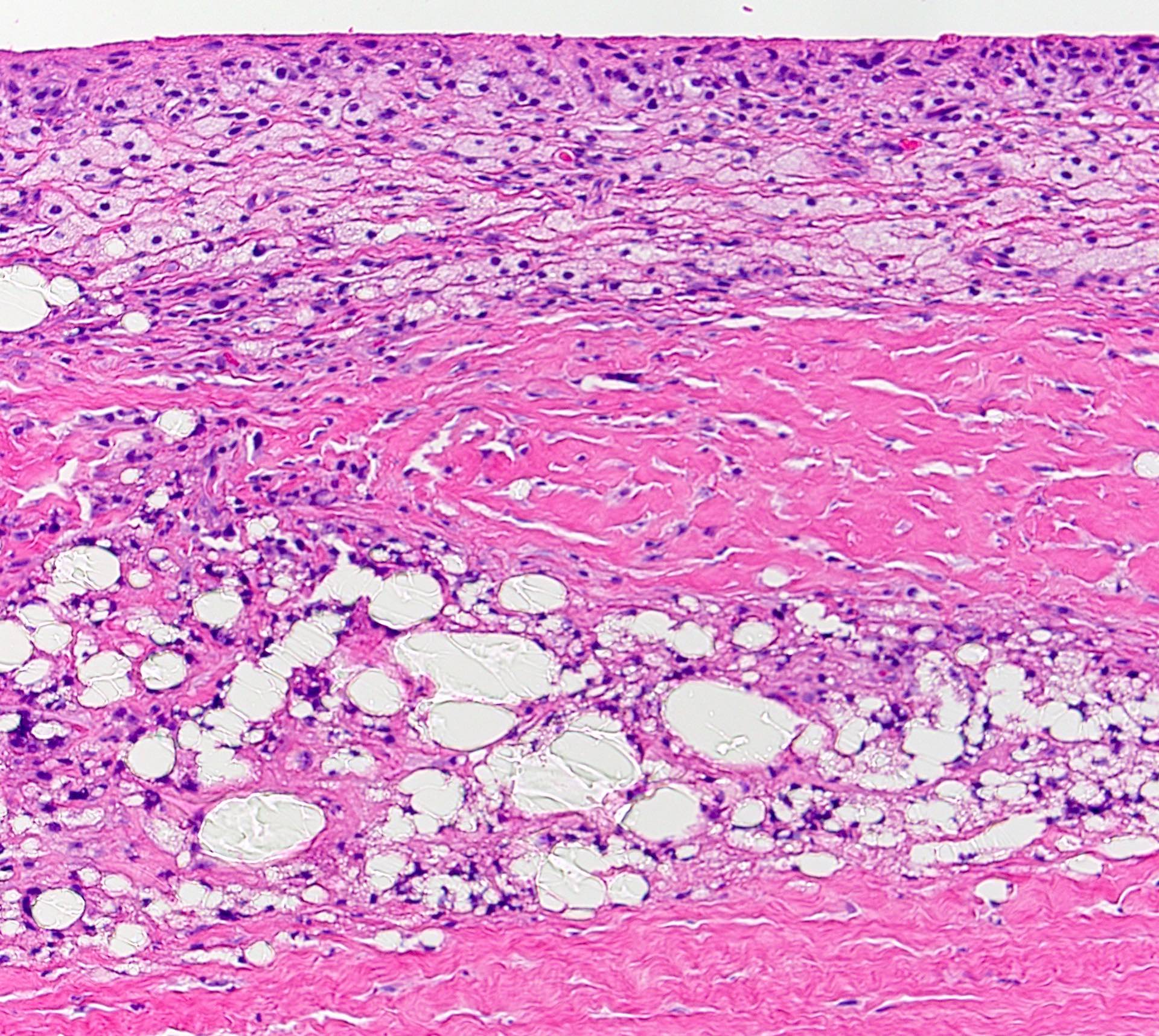
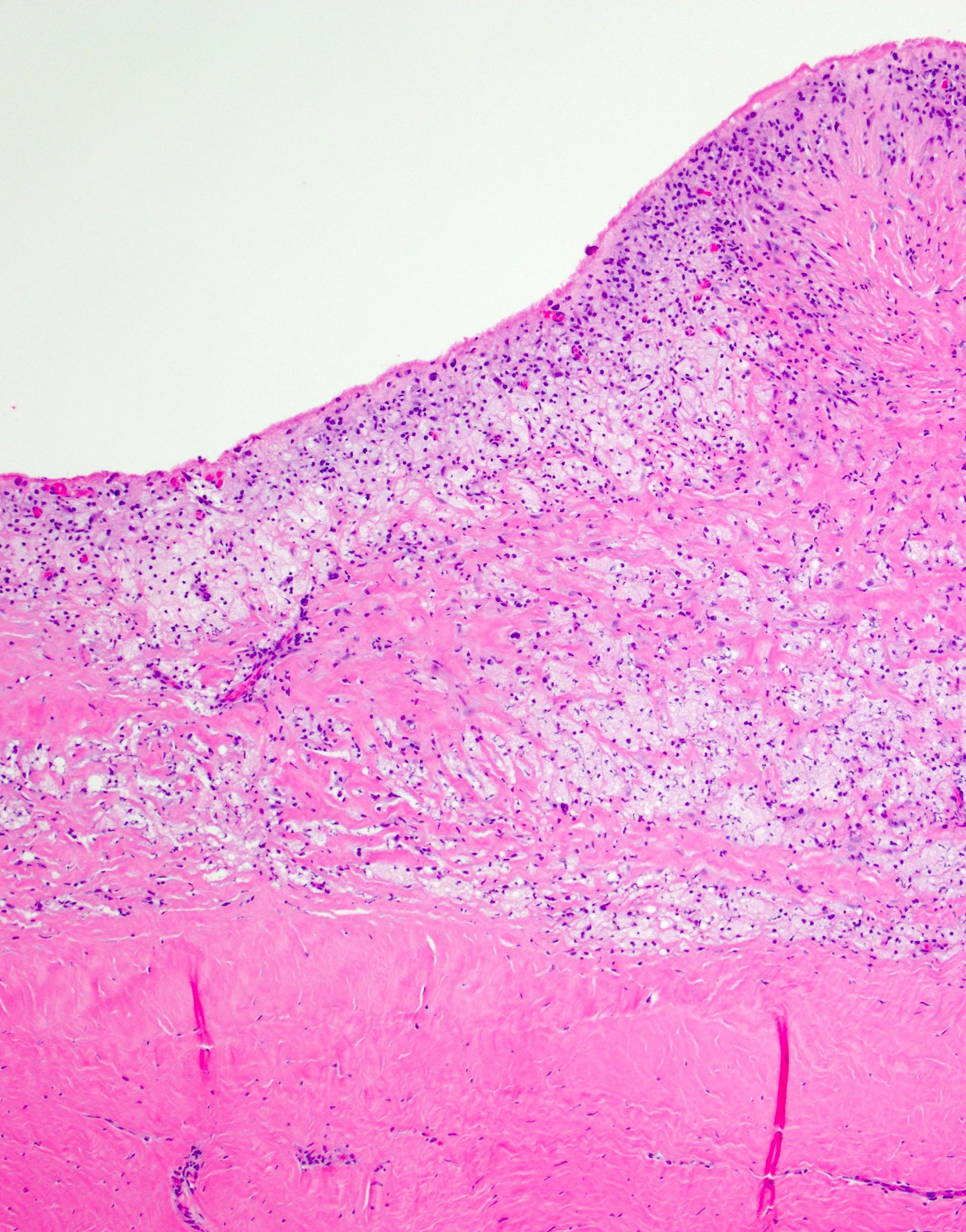
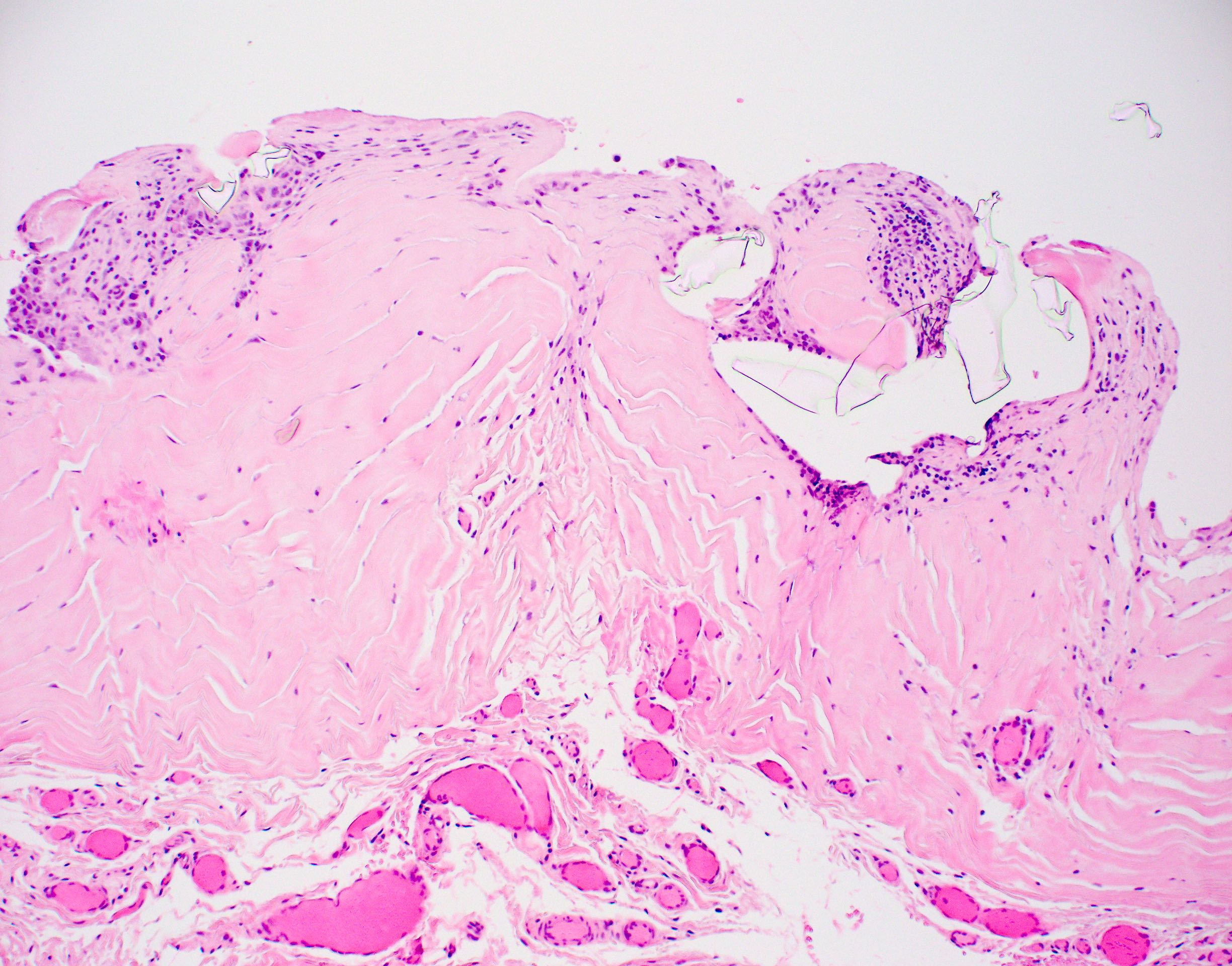
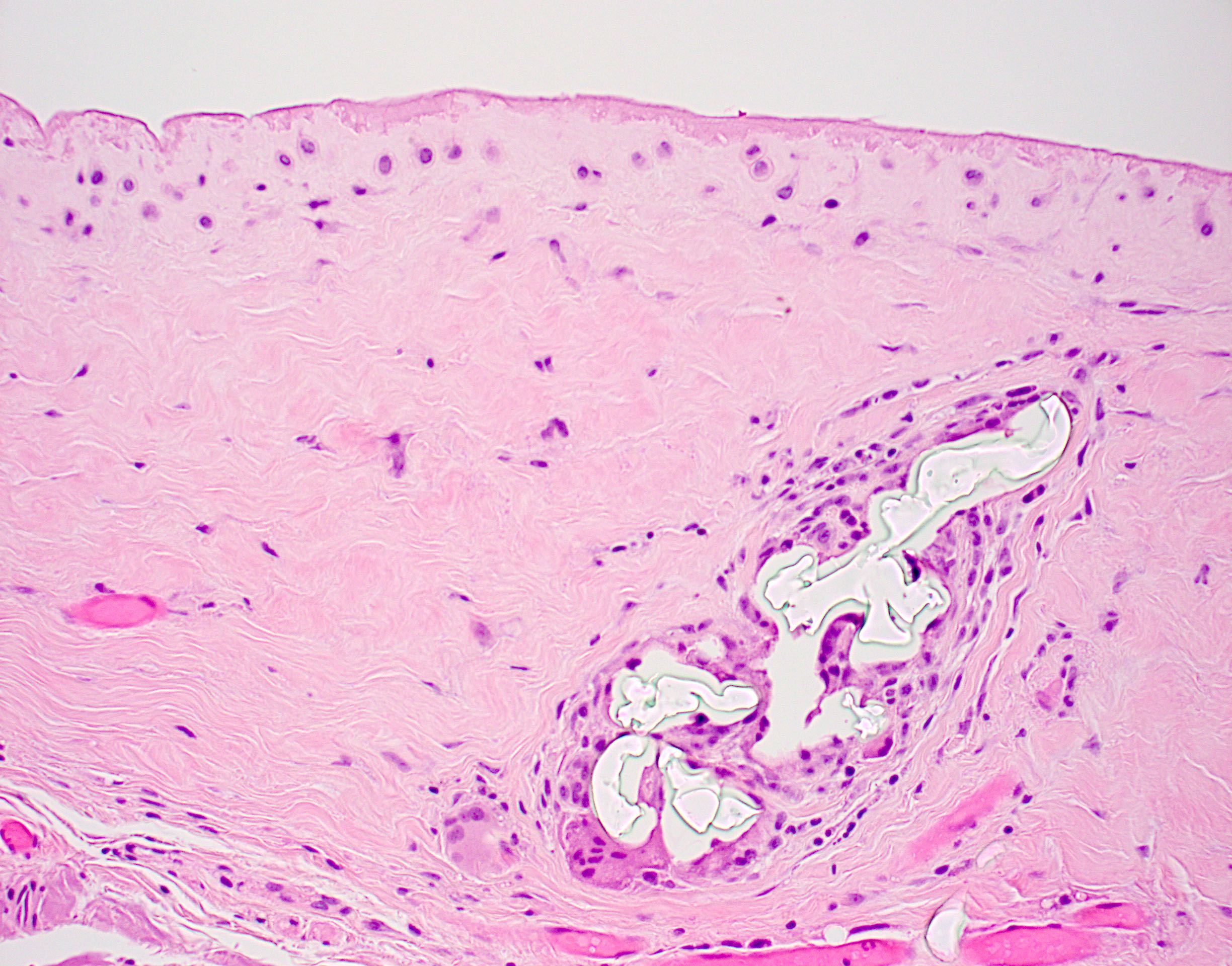
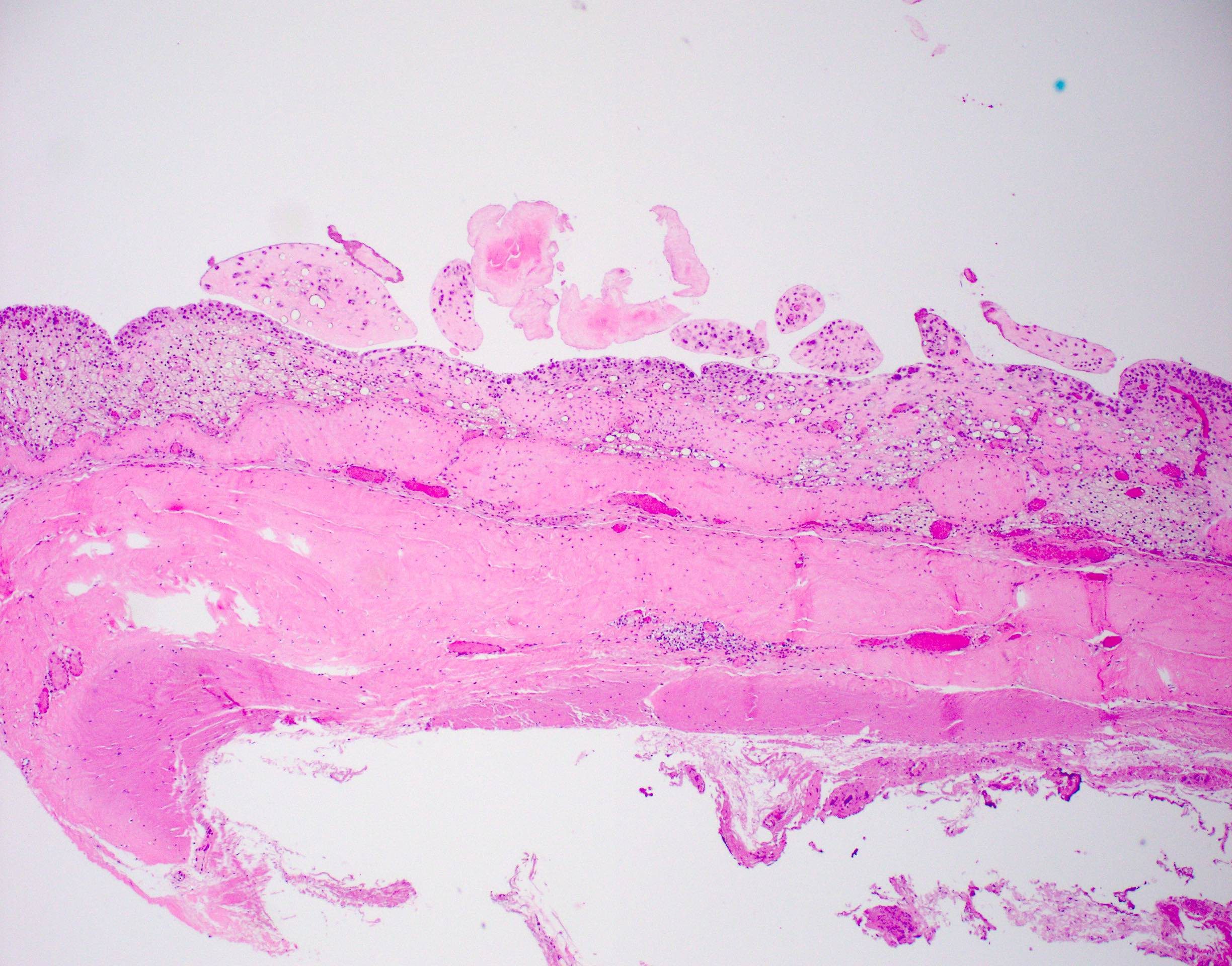
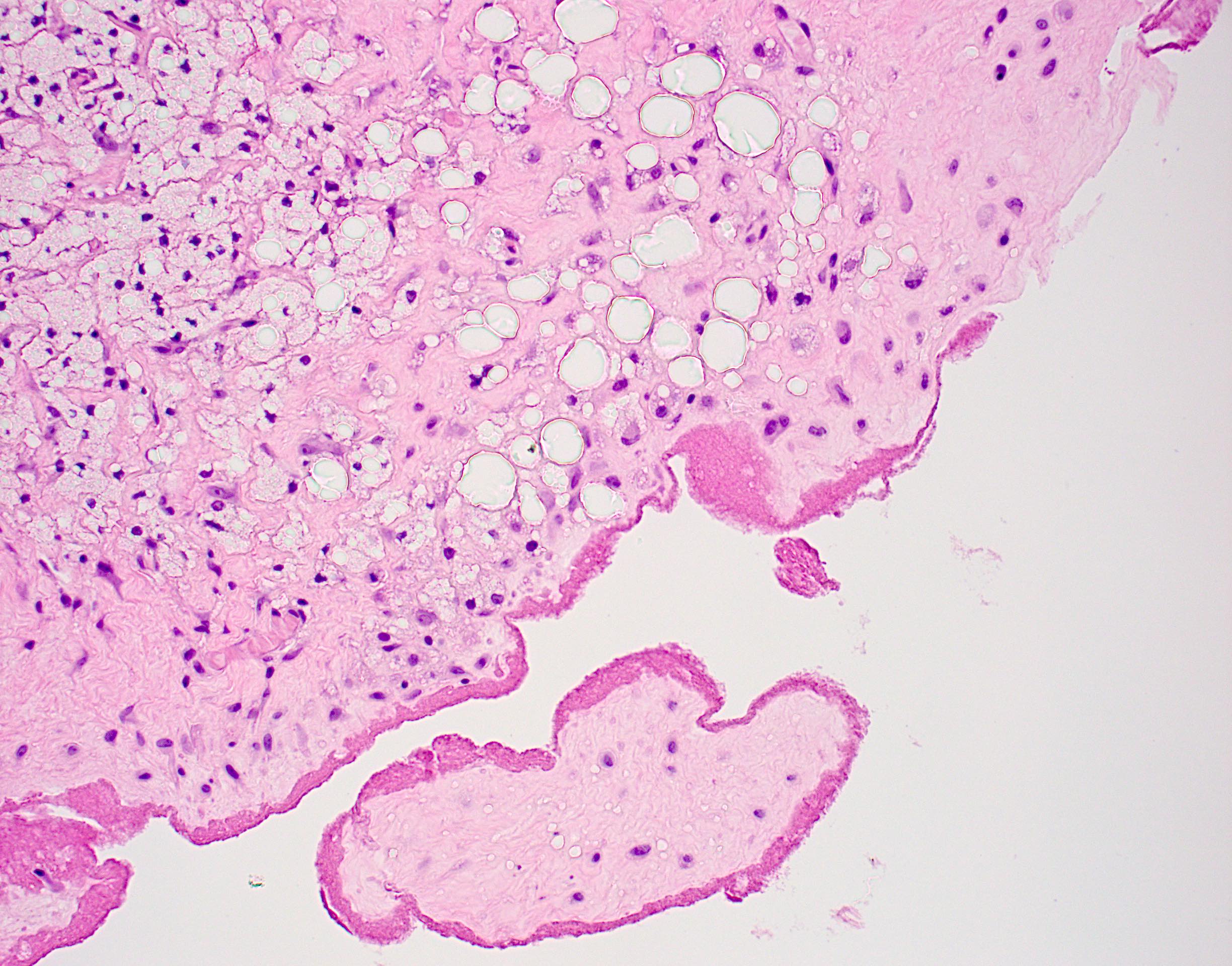
Microscopic (histologic) description
- Features are not specific:
- Chronic inflammatory cells, foreign body giant cell reaction and fibrosis
- Fat necrosis → histiocytes containing clear, refractile, nonpolarizable material within cytoplasmic vacuoles
- Extracellular silicone can also be seen as nonbirefringent crystals or particles within empty spaces
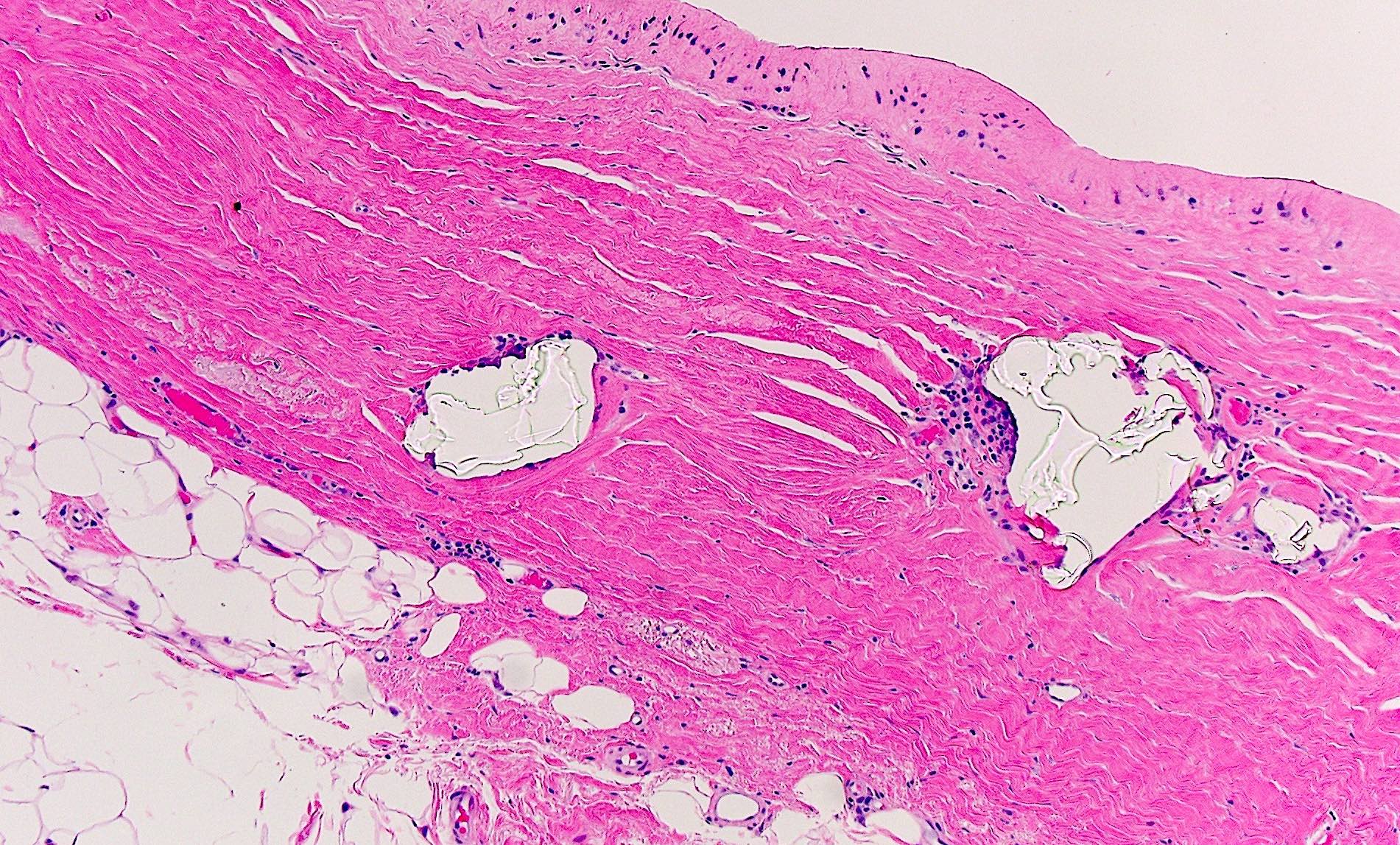
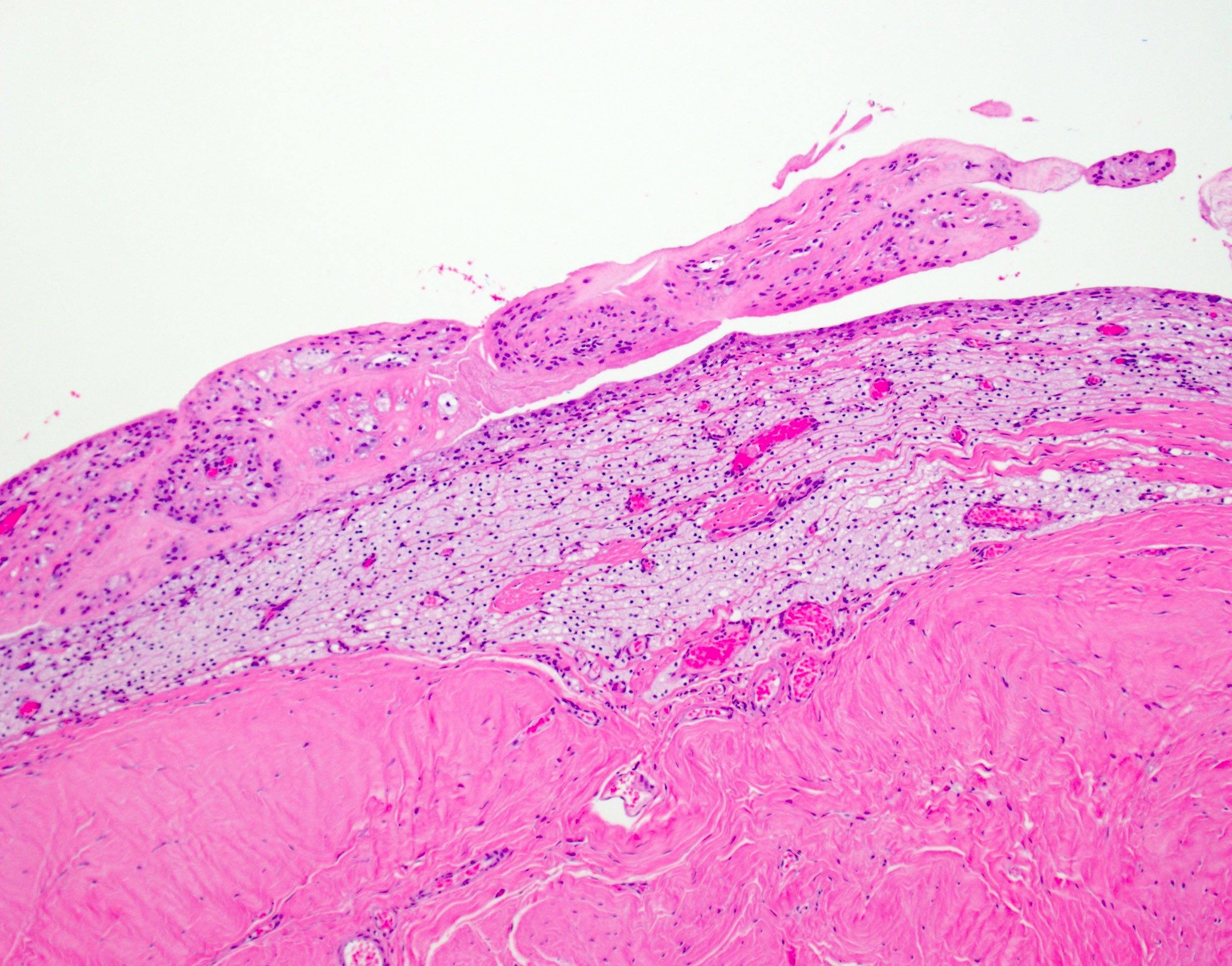
- Later features include:
- Fibrous capsule or bursa: well defined band of collagenized fibrous tissue and mixed chronic inflammatory cells
- Calcifications in the capsule or around: globular aggregates, may have bone formation
Microscopic (histologic) images
Contributed by Syed Hoda, M.B.B.S. and Julie M. Jorns, M.D.
Capsule with silicone
Silicone and synovial metaplasia
Foamy histiocytes
Clinically ruptured silicone implant
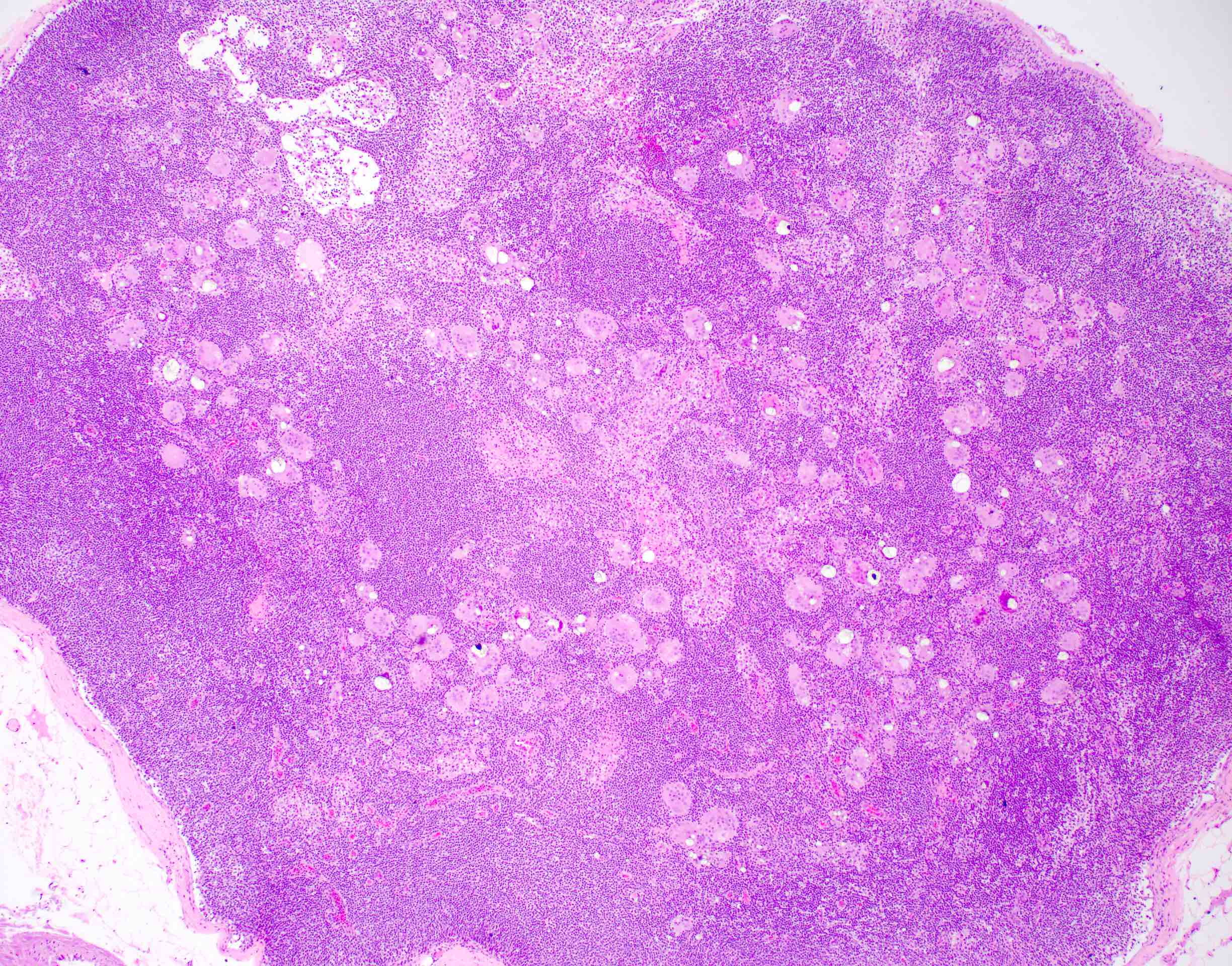

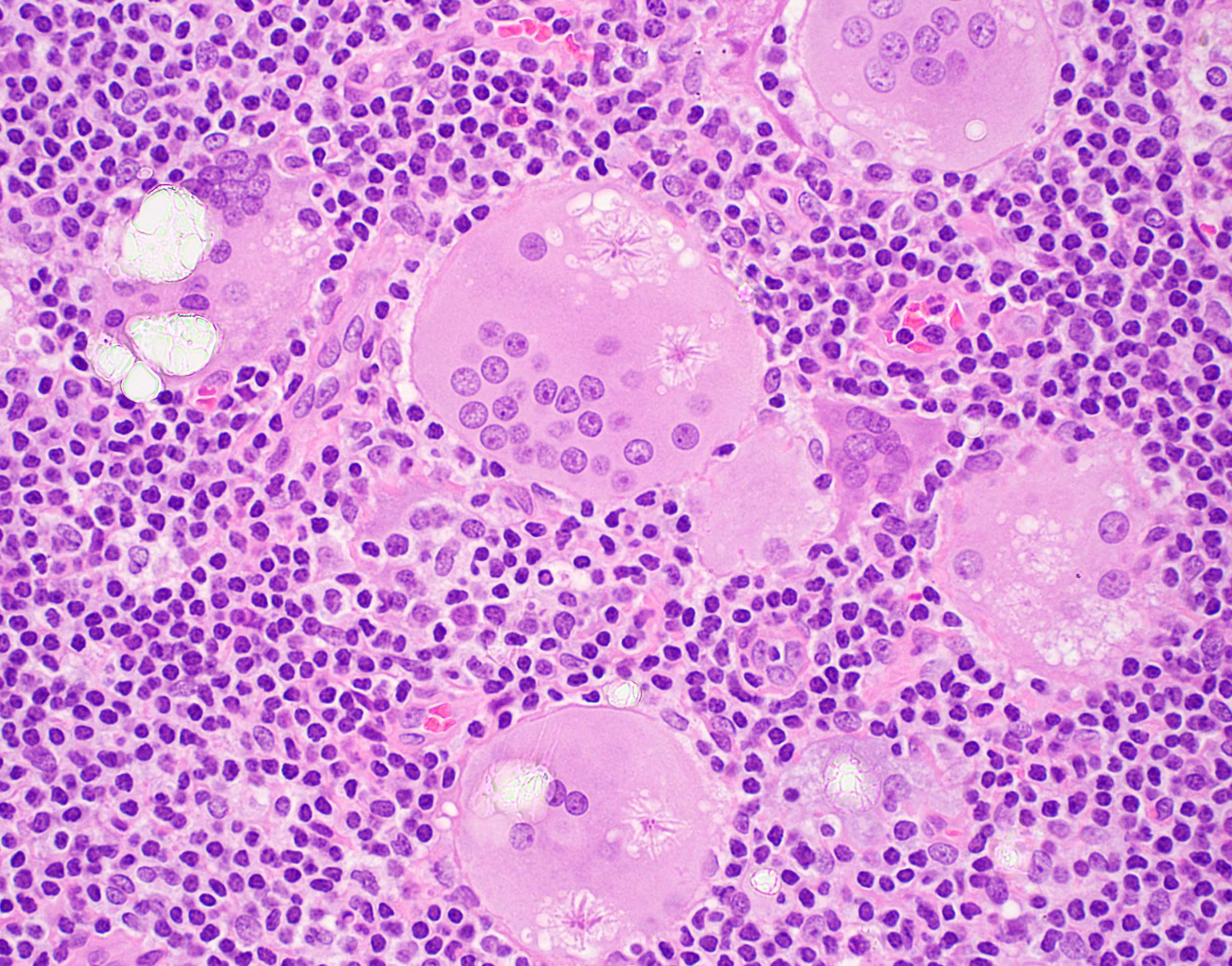
Silicone lymphadenitis
Implant with associated seroma
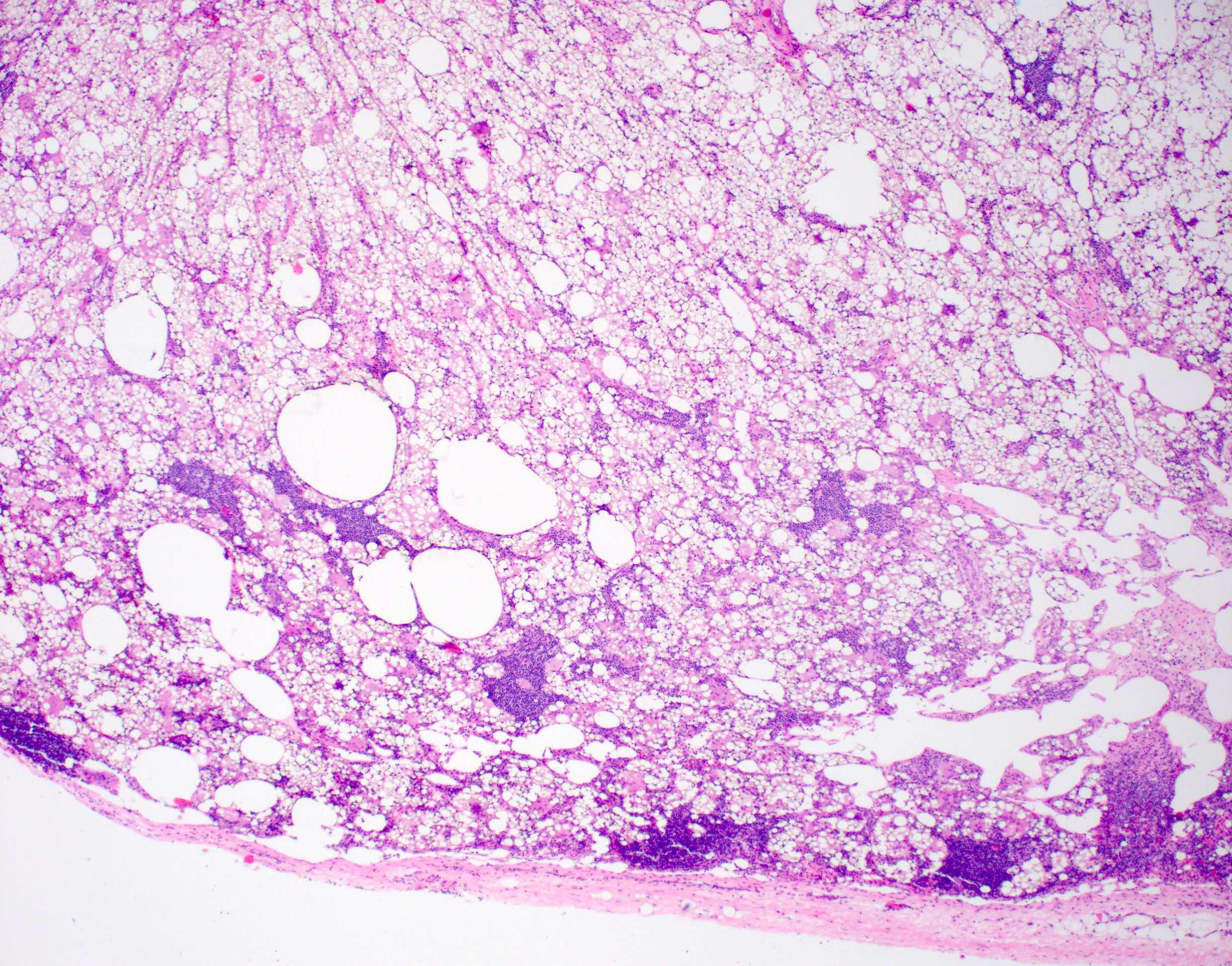

Silicone lymphadenitis
Virtual slides
Images hosted on other servers:

Breast, silicone granuloma

Lymph node, silicone lymphadenopathy
Cytology description
- Papillary synovial spherules consisting of an extracellular matrix and bland looking cells (Diagn Cytopathol 2018;46:769)
- Vacuolated histiocytes containing refractile particles (Acta Cytol 1990;34:10)
Positive stains
- Macrophages and foreign body giant cells: CD11b, CD44, CD68, CD163 (J Histochem Cytochem 2006;54:763, Cell Rep 2015;13:1937)
Negative stains
Electron microscopy description
- Calcifications are composed of hydroxyapatite crystals
Sample pathology report
- Left breast, core needle biopsy:
- Benign breast tissue with fibrous capsule with associated foreign body giant cell reaction to silicone, chronic inflammation and fat necrosis
Differential diagnosis
- Sinus histiocytosis with massive lymphadenopathy:
- Fever, leukocytosis, anemia
- Usually no history of breast implant
- Large histiocytes with emperipolesis, plasma cells
- No foreign body giant cell reaction
- No foreign material
- Fat necrosis:
- Usually secondary to injury or previous procedures
- No history of breast implant
- May have foreign material from prior procedure(s) but is morphologically different from silicone
- Abscess / acute mastitis:
- Associated with lactation in most cases
- Neutrophils are predominant
- Bacteria are usually present (gram positive)
- No foreign material
- Cystic neutrophic granulomatous mastitis:
- Fever, leukocytosis, anemia
- Granulomatous inflammation with cystic spaces rimmed by neutrophils
- Coryneform bacteria is present in cystic spaces (gram positive, culture or molecular testing)
- No foreign material
Additional references
Board review style question #1
A 34 year old nulliparous female presented with a unilateral breast mass 8 years after bilateral breast augmentation with silicone implants. On examination, the patient was afebrile but her breast was tender with a focal deformity. Which of the following histomorphological features is associated with her condition?
- Caseating granulomas
- Cystically dilated ducts with inspissated material
- Gram positive bacteria
- Histiocytes with refractile material
Board review style answer #1
Board review style question #2
Which of the following features is seen in silicone lymphadenitis?
- Crystals
- Emperipolesis
- Fungal hyphae
- Langhans giant cells
Board review style answer #2
