
Breast
Fibrocystic changes
Sclerosing adenosis
Author: Julie M. Jorns, M.D.
Editorial Board Member: Gary Tozbikian, M.D.
Editor-in-Chief: Debra L. Zynger, M.D.

Last author update: 9 July 2021
Last staff update: 27 March 2024
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Sclerosing adenosis


Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Positive stains | Videos | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Jorns JM. Sclerosing adenosis. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/breastsclerosingadenosis.html. Accessed April 1st, 2025.
Definition / general
- Adenosis or lobulocentric processes with increase in glandular elements of terminal duct lobular unit (TDLU) with stromal fibrosis / sclerosis that distorts and compresses glands
- Preserved 2 cell layer (inner epithelial and outer myoepithelial cells)
Essential features
- Enlarged terminal duct lobular unit with distortion by stromal fibrosis / sclerosis
Terminology
- Nodular adenosis / adenosis tumor:
- Palpable mass (AJR Am J Roentgenol 2000;175:31)
- Coalescent foci of typical sclerosing adenosis
- Myoepitheliosis:
- Rare; sclerosing adenosis with predominance of myoepithelial cells, presents as multifocal microscopic lesions (Am J Surg Pathol 1991;15:554)
ICD coding
Epidemiology
- Most frequent in third to fourth decades but occurs over a wide age range
- Found in 12 - 28% of all benign and 5 - 7% of malignant biopsies (J Ultrasound Med 2013;32:2029)
Sites
- Terminal duct lobular unit; otherwise, no specific location within the breast
Pathophysiology
- Unknown
Etiology
- Unknown
Clinical features
- Considered a part of the spectrum of fibrocystic changes
- Often an incidental finding or detected by screening
- Can present as a palpable mass if nodular adenosis / adenosis tumor
- Reference: Schnitt: Biopsy Interpretation of the Breast, 3rd Edition, 2017
Diagnosis
- Histologic examination of tissue with or without immunohistochemistry
Radiology description
- Variable depending on the size / extent of breast involvement
- If focal, may not be visualized (i.e. incidental finding on histologic examination)
- Amorphous or pleomorphic clustered microcalcifications; architectural distortion or circumscribed to spiculated mass on mammogram (Diagn Interv Radiol 2011;17:311, Mol Clin Oncol 2017;6:157)
- Associated with increased mammographic breast density (Breast Cancer Res 2017;19:134)
- Heterogeneous echogenicity, irregular and ill defined mass, focal acoustic shadowing may be seen on ultrasound (Mol Clin Oncol 2017;6:157)
- Small (< 1 cm) mass with benign kinetics on MRI (Breast J 2019;25:143)
Radiology images
Contributed by Julie M. Jorns, M.D.
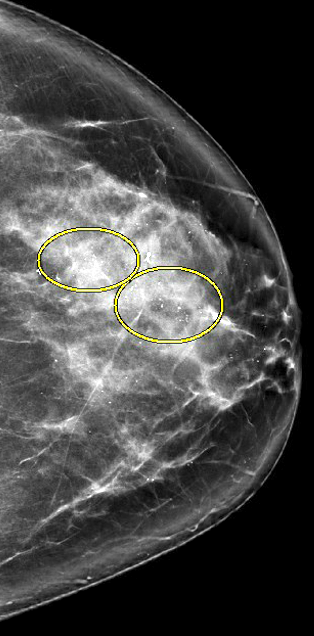
Calcifications, craniocaudal view
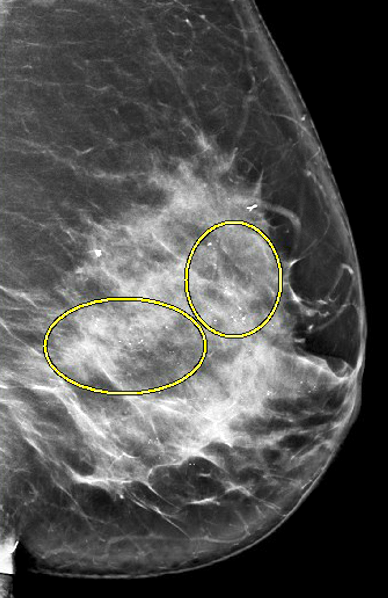
Calcifications, mediolateral oblique view
Prognostic factors
- As a single feature, increased risk of cancer of 1.5 - 2x, as seen with proliferative fibrocystic changes (Cancer 1989;64:1977)
- 2x higher risk of breast cancer with increased Ki67 proliferation index in sclerosing adenosis or associated normal background breast tissue (Breast Cancer Res Treat 2015;151:89)
- Does not provide further risk stratification in the presence of other proliferative disease / atypical hyperplasias (Breast Cancer Res Treat 2014;144:205)
- Rarely involved by lobular carcinoma in situ and mistaken for invasive carcinoma (Mod Pathol 1991;4:1)
- Ductal carcinoma in situ arising in sclerosing adenosis has a higher frequency of bilaterality (Clin Breast Cancer 2012;12:398, Breast Cancer 2014;21:732)
- Can mimic malignancy clinically and radiologically
Case reports
- 46 year old woman with sclerosing adenosis with mammogram and cytology mimicking malignancy (J Cytol 2013;30:49)
- 73 year old woman with sclerosing adenosis and coexisting ductal carcinoma in situ (Int J Surg Case Rep 2018;45:9)
- 82 year old woman with sclerosing adenosis in sentinel axillary lymph nodes (Arch Pathol Lab Med 2008;132:1439)
Treatment
- Presence of sclerosing adenosis alone in a core biopsy does not require surgical excision
- Coexisting atypia will typically prompt surgical consultation
Gross description
- Variable depending on extent of involvement and calcifications
- May be indistinguishable from surrounding breast tissue
- Multinodular, ill defined, cuts with increased resistance due to fibrosis
- Gritty due to frequent calcifications but no chalky yellow white foci or streaks as seen in fat necrosis
- Circumscribed to ill defined white, fibrotic mass if nodular adenosis / adenosis tumor
- Reference: Schnitt: Biopsy Interpretation of the Breast, 3rd Edition, 2017
Microscopic (histologic) description
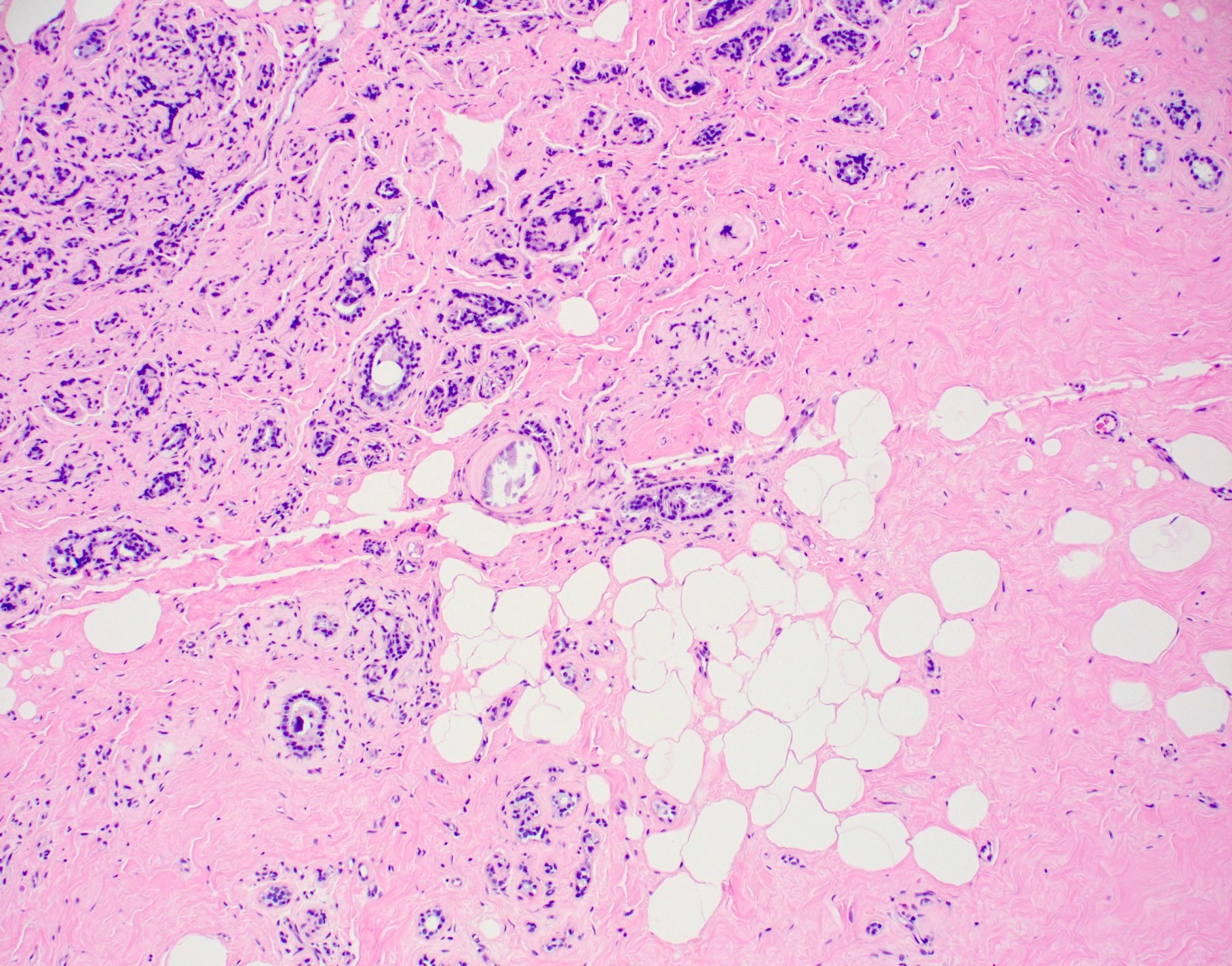
- Low power: increase in glandular elements plus stromal fibrosis / sclerosis that distorts and compresses glands
- Maintains lobular architecture at low power with rounded and well defined nodules
- Centrally is more cellular with distorted and compressed ductules; peripherally has more open or dilated ductules
- Often has microcalcifications, due to calcification of entrapped secretions
- Often has associated fibrocystic changes of other types, such as apocrine metaplasia
- Preservation of luminal epithelium and peripheral myoepithelium (2 cell layer) with surrounding basement membrane
- Myoepithelial cells may vary from being prominent to indistinct on routine H&E staining
- Myoepithelial cells are readily apparent via immunohistochemistry, even if difficult to identify on H&E
- Rarely penetrates walls of blood vessels or perineural spaces
- No necrosis, no pleomorphism
- Apocrine adenosis: variant of sclerosing adenosis with prominent apocrine features
- Epithelium may be involved by proliferative, atypical lesions or in situ carcinoma
- Can mimic malignancy:
- If involved by atypia or in situ carcinoma
- If florid and overtly non-lobulocentric / (pseudo) infiltrative into fat or stroma
- Conspicuous myoepithelial cells with attenuated epithelial cells can appear like stands of single cells and mimic invasive lobular carcinoma
- Atypical apocrine metaplasia: nuclear atypia / rare mitosis (Mod Pathol 1991;4:1)
- (Pseudo) perineural invasion
Microscopic (histologic) images
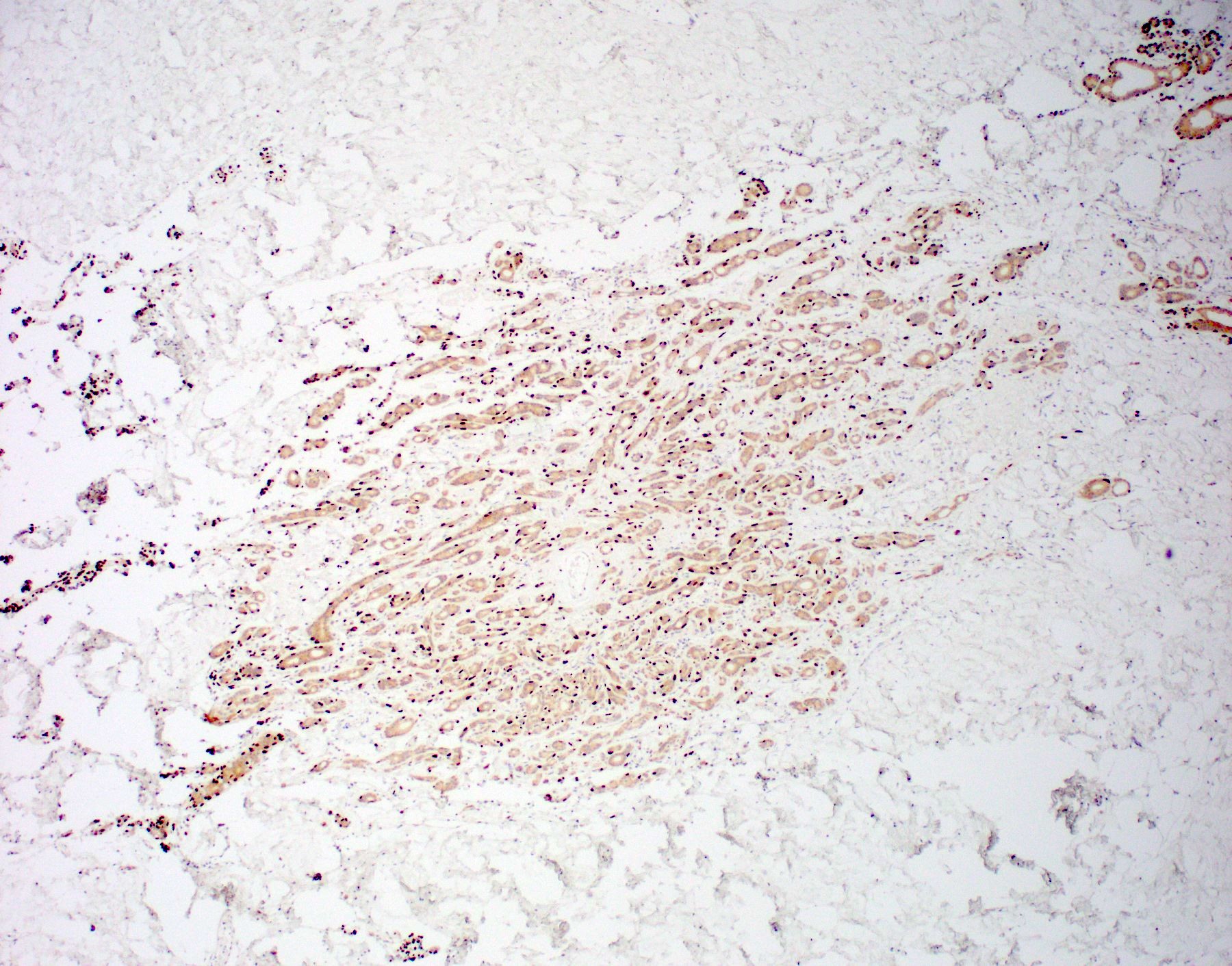
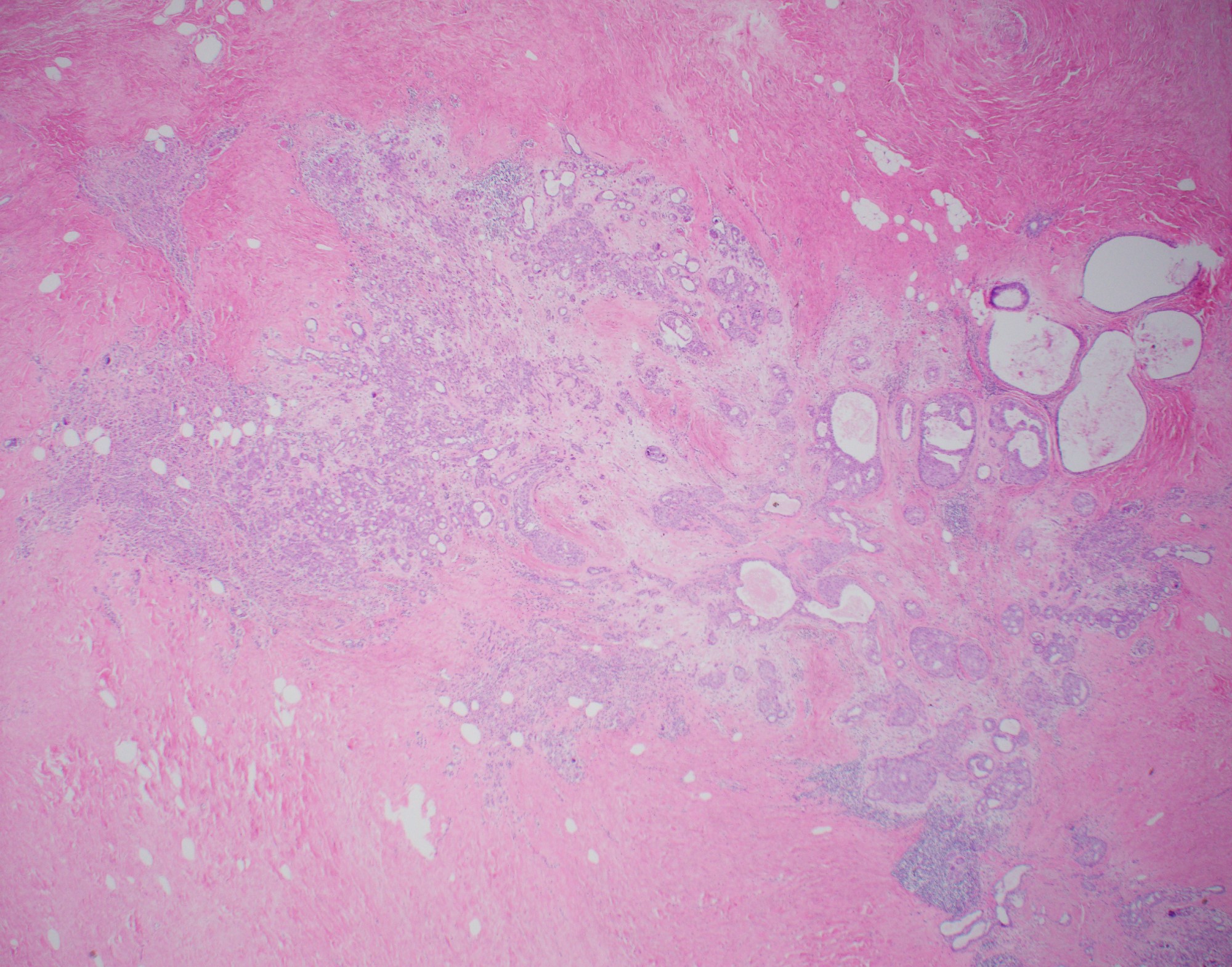
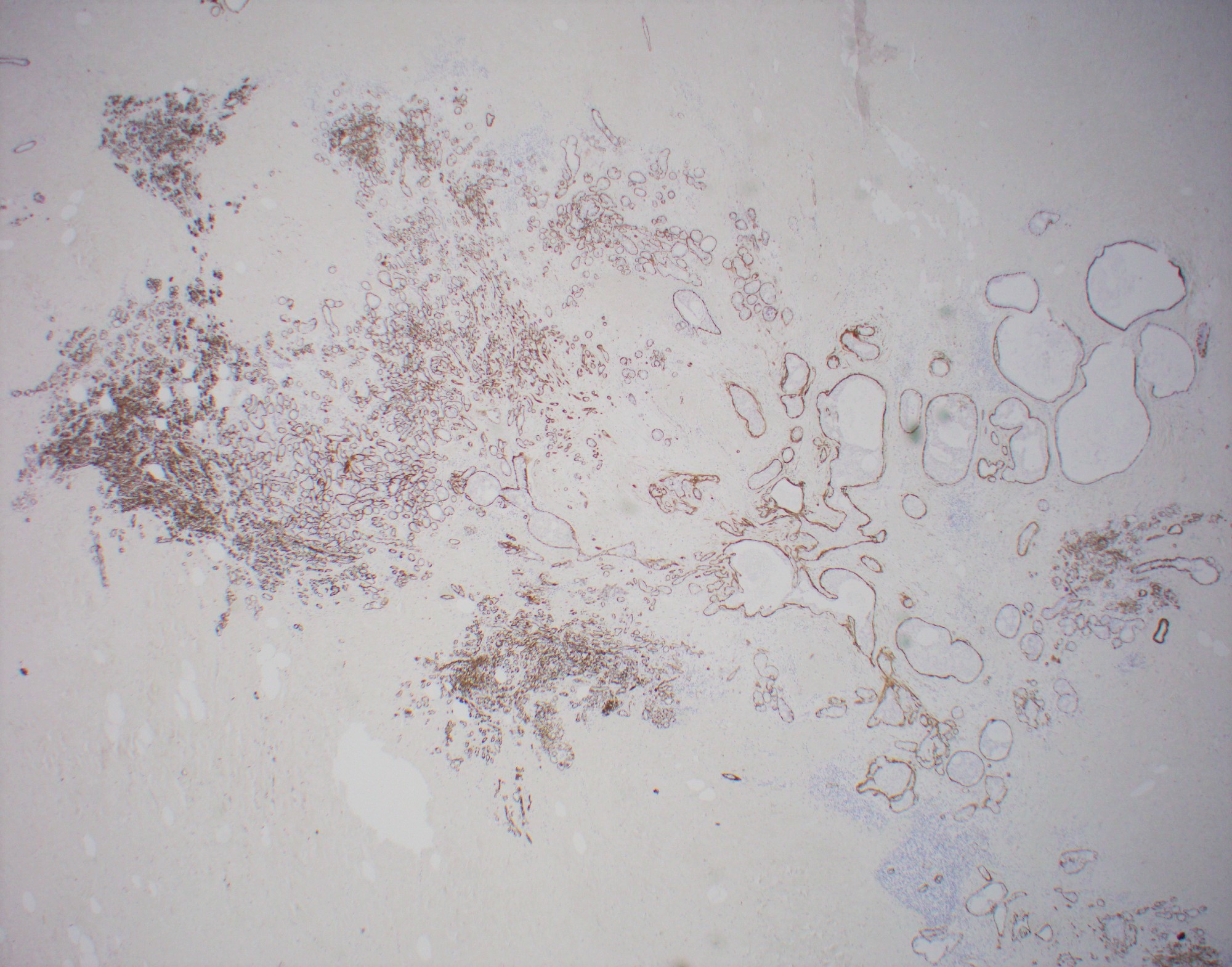
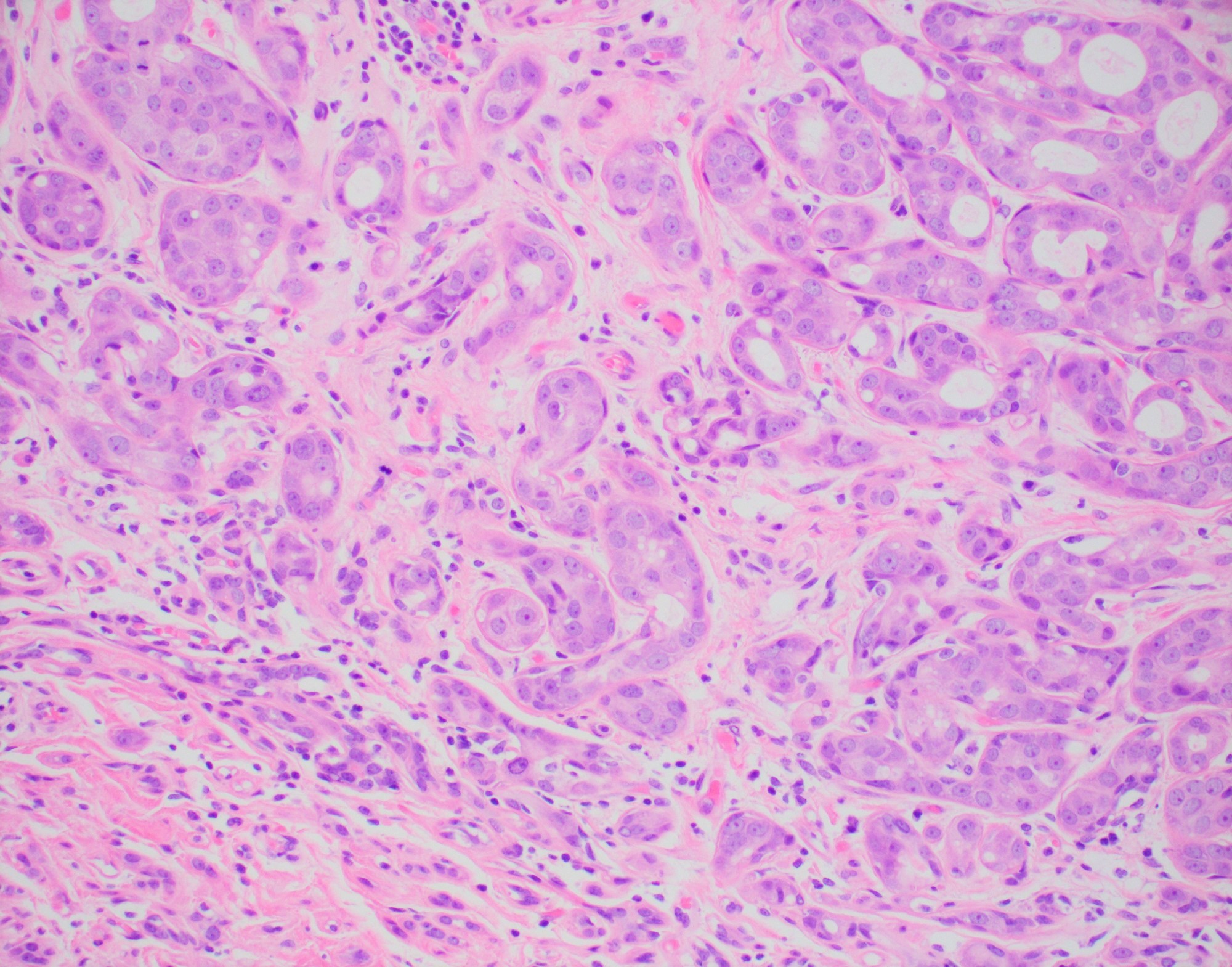
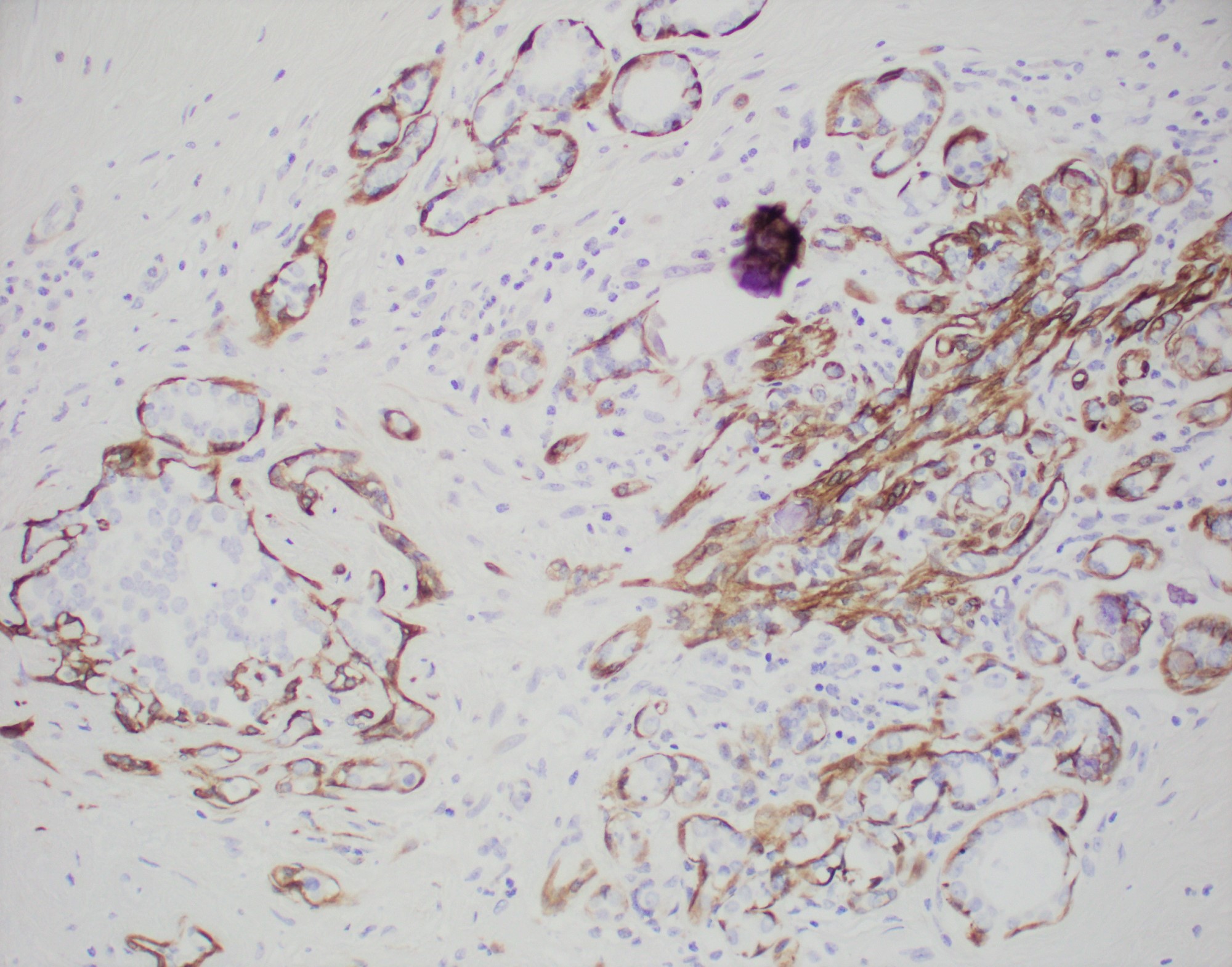
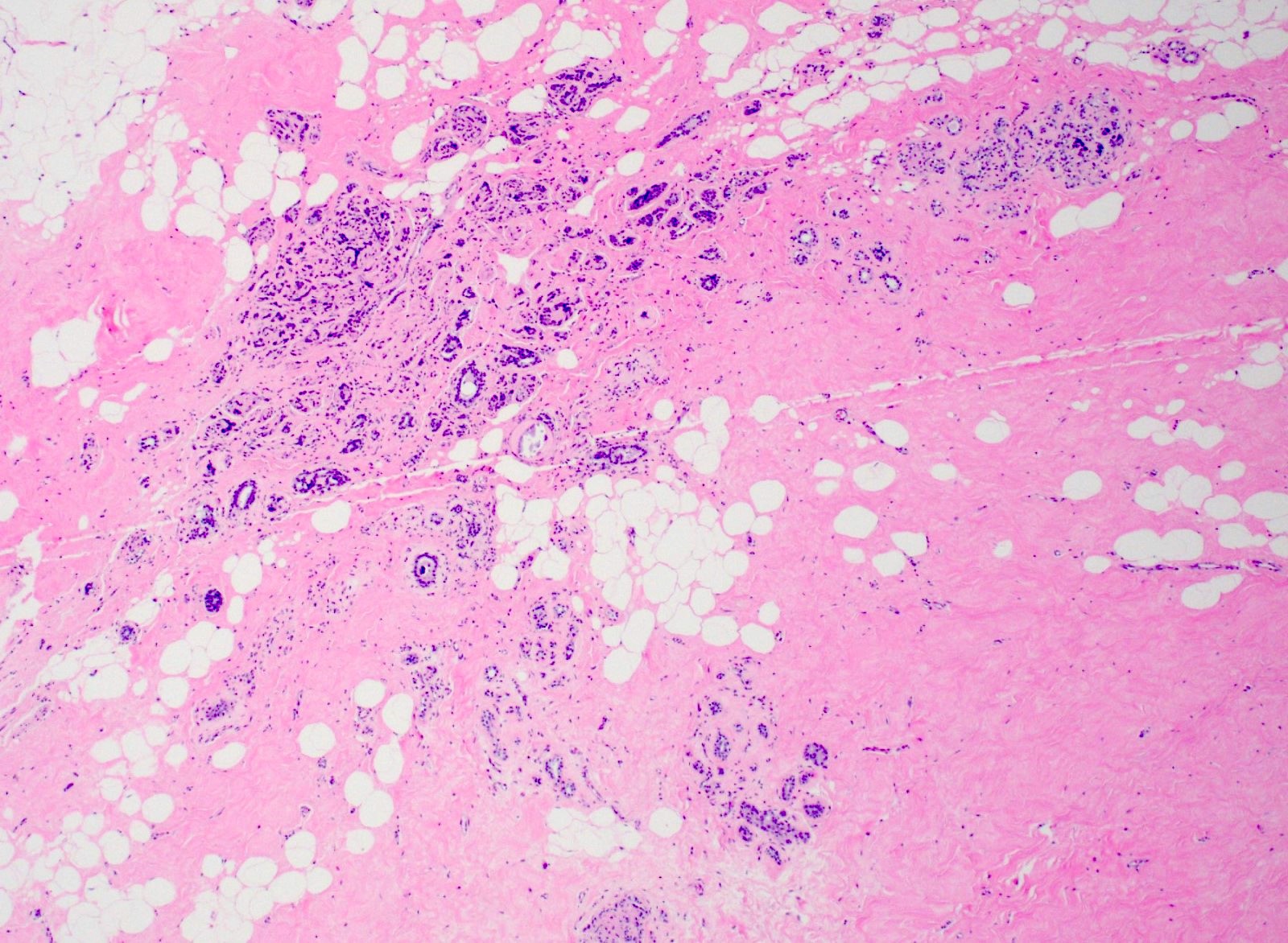
Contributed by Julie M. Jorns, M.D.
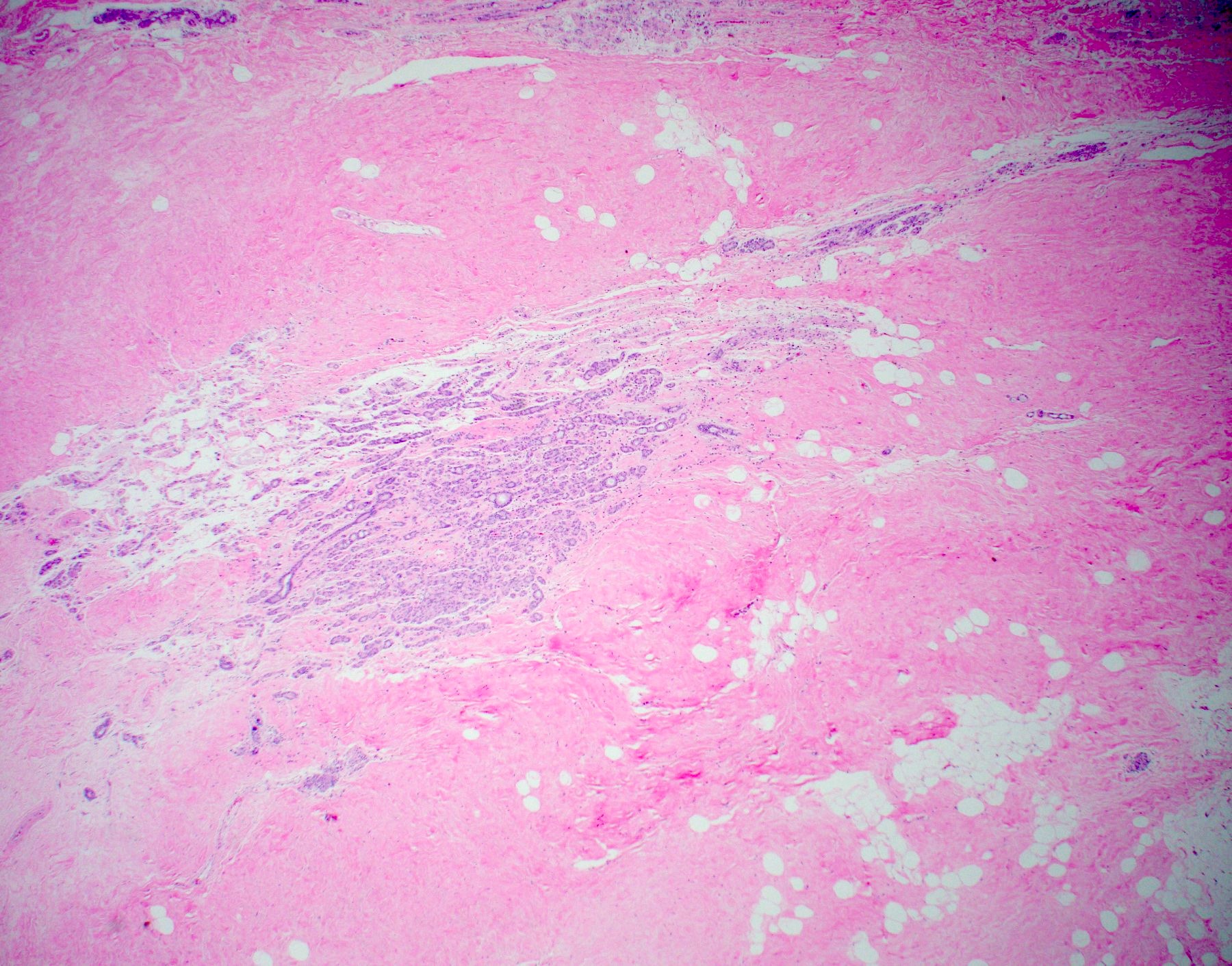
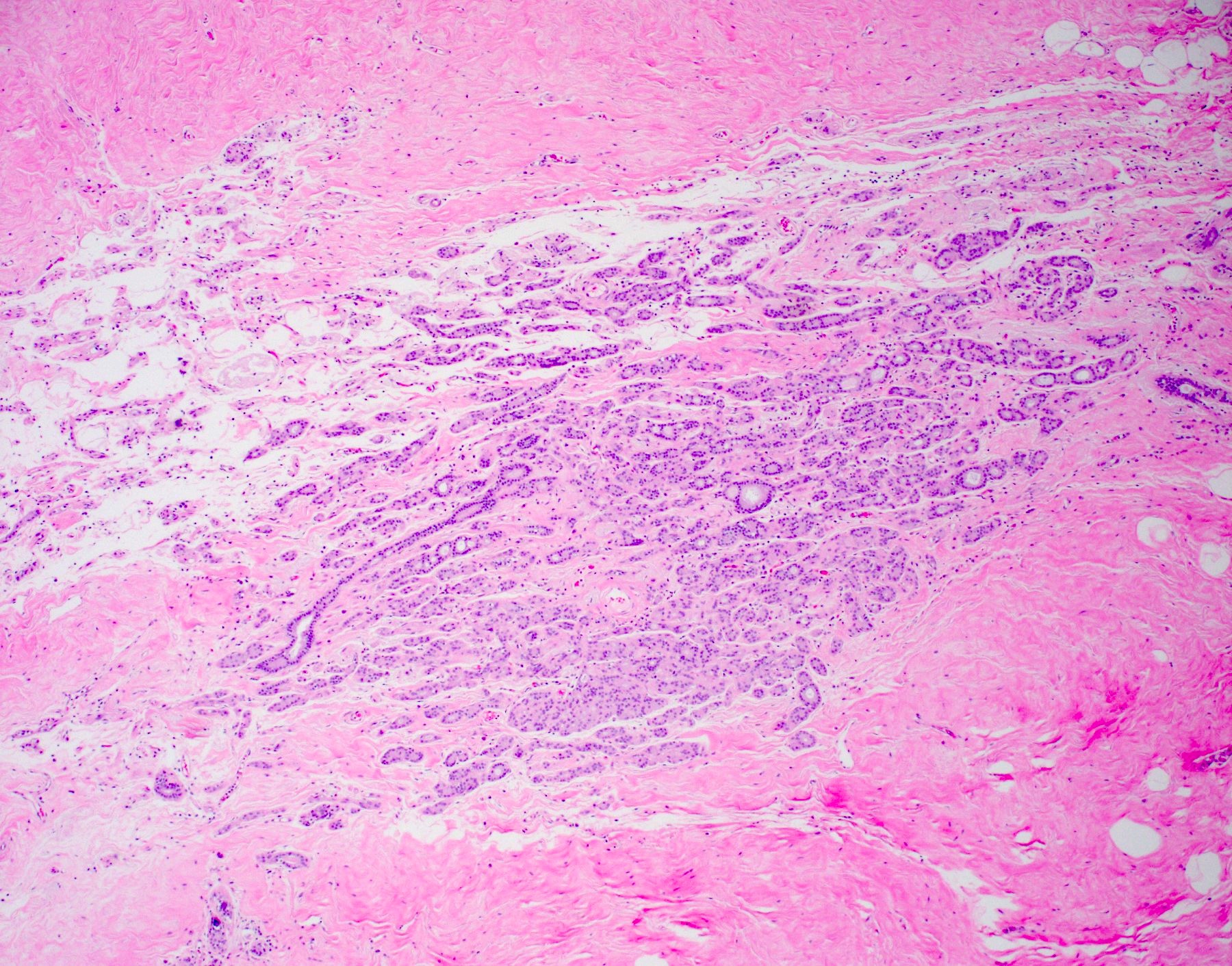
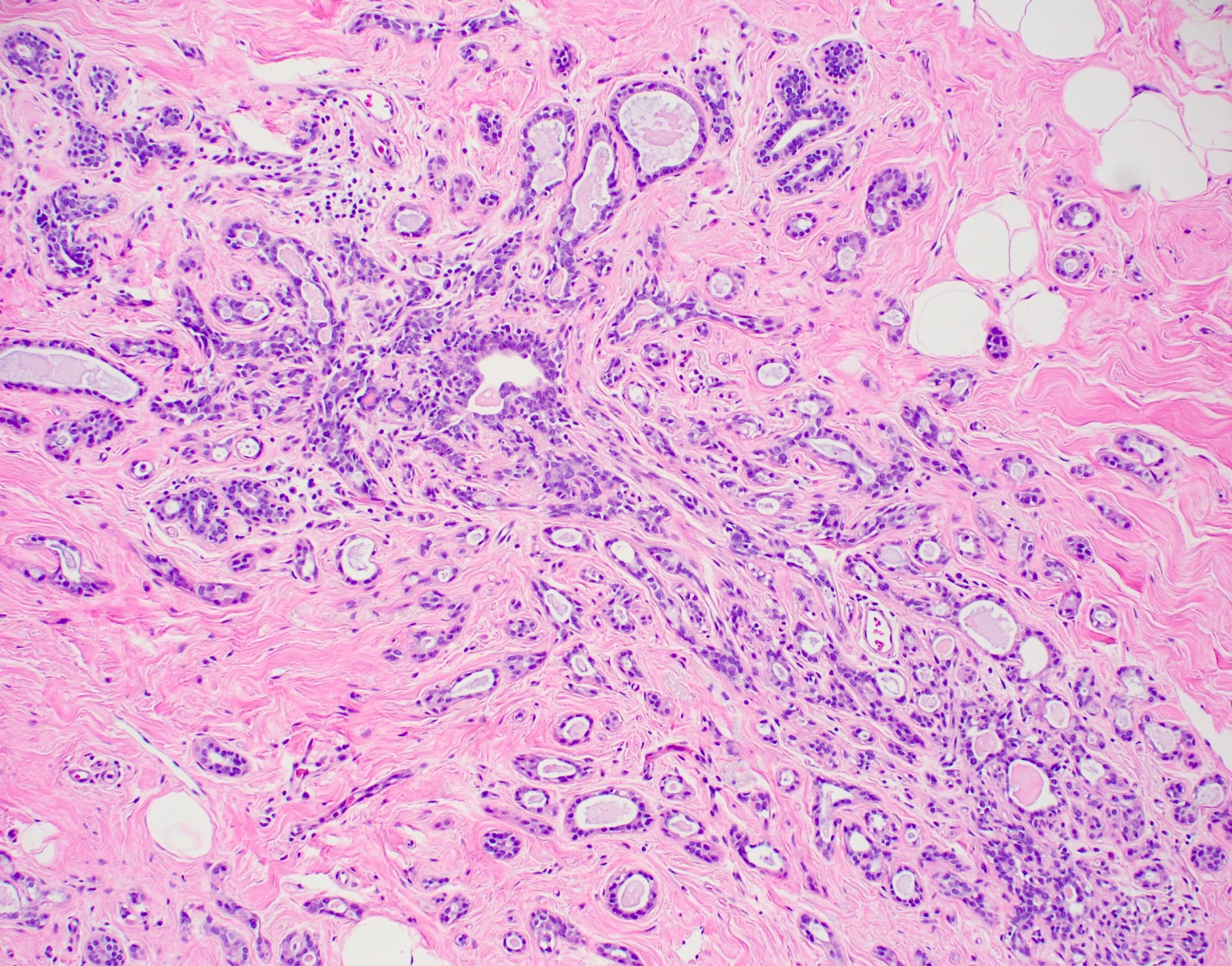
Lobule with distortion
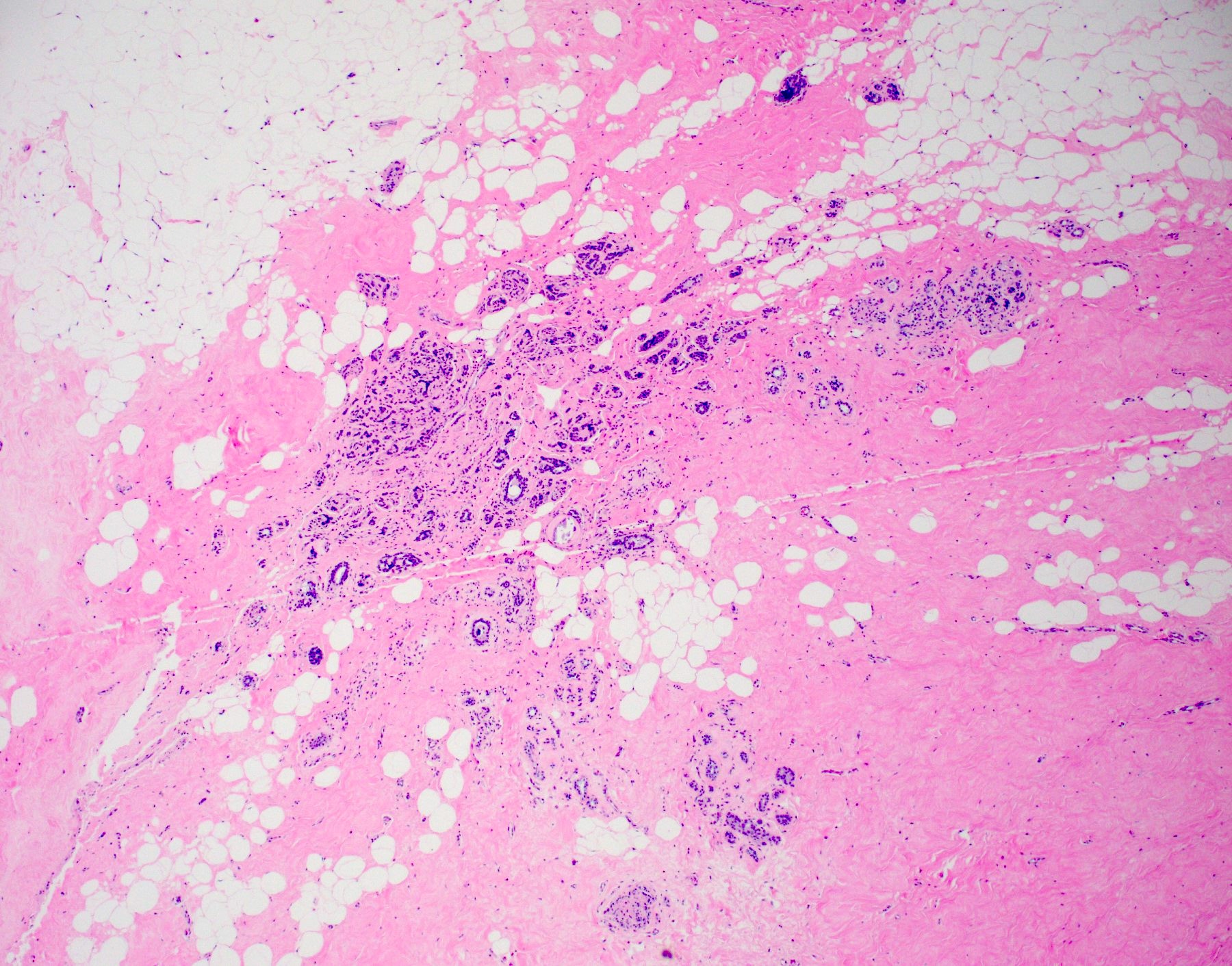
Calcifications and drag
Drag mark
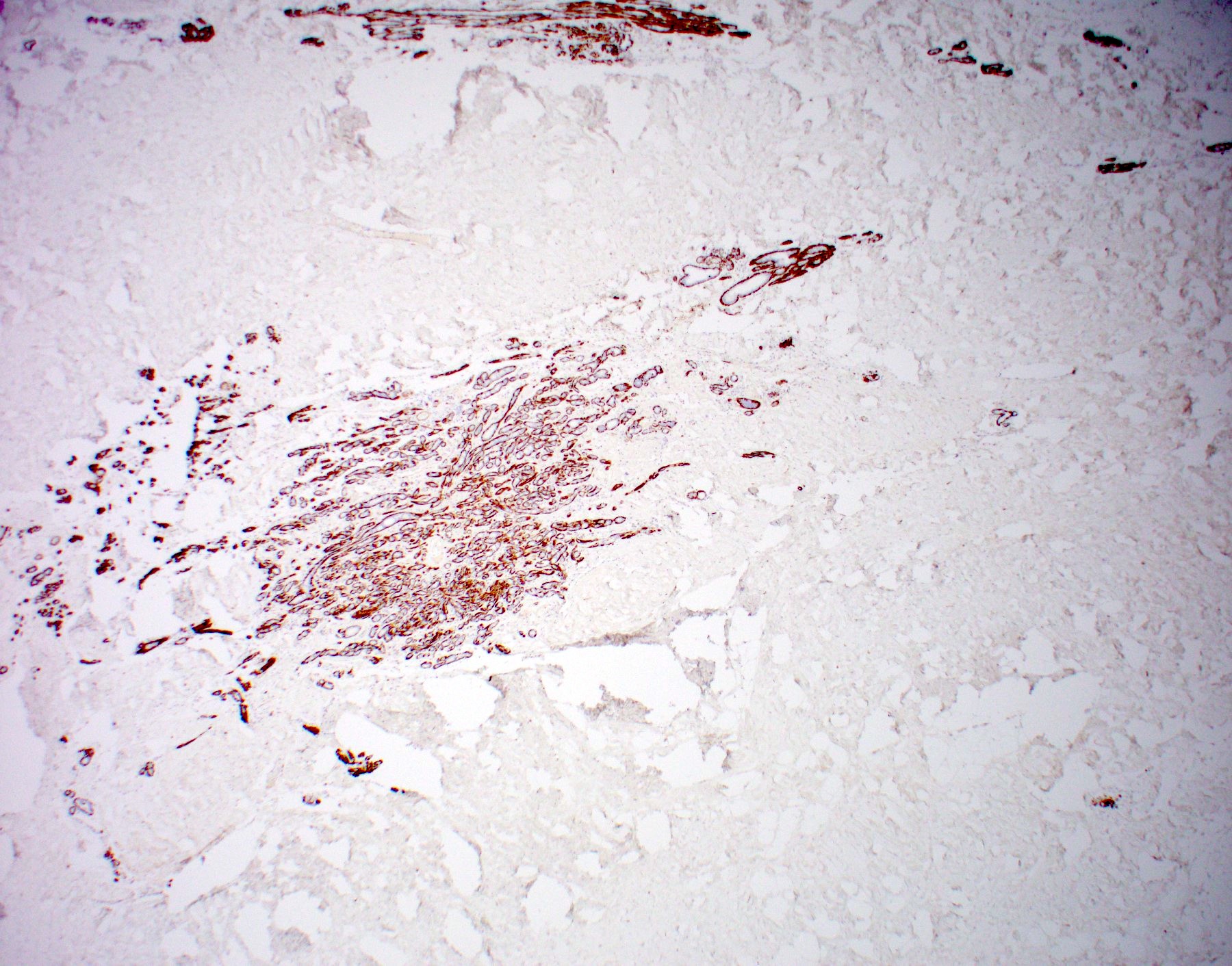
Calponin
p63
Sclerosing adenosis with DCIS
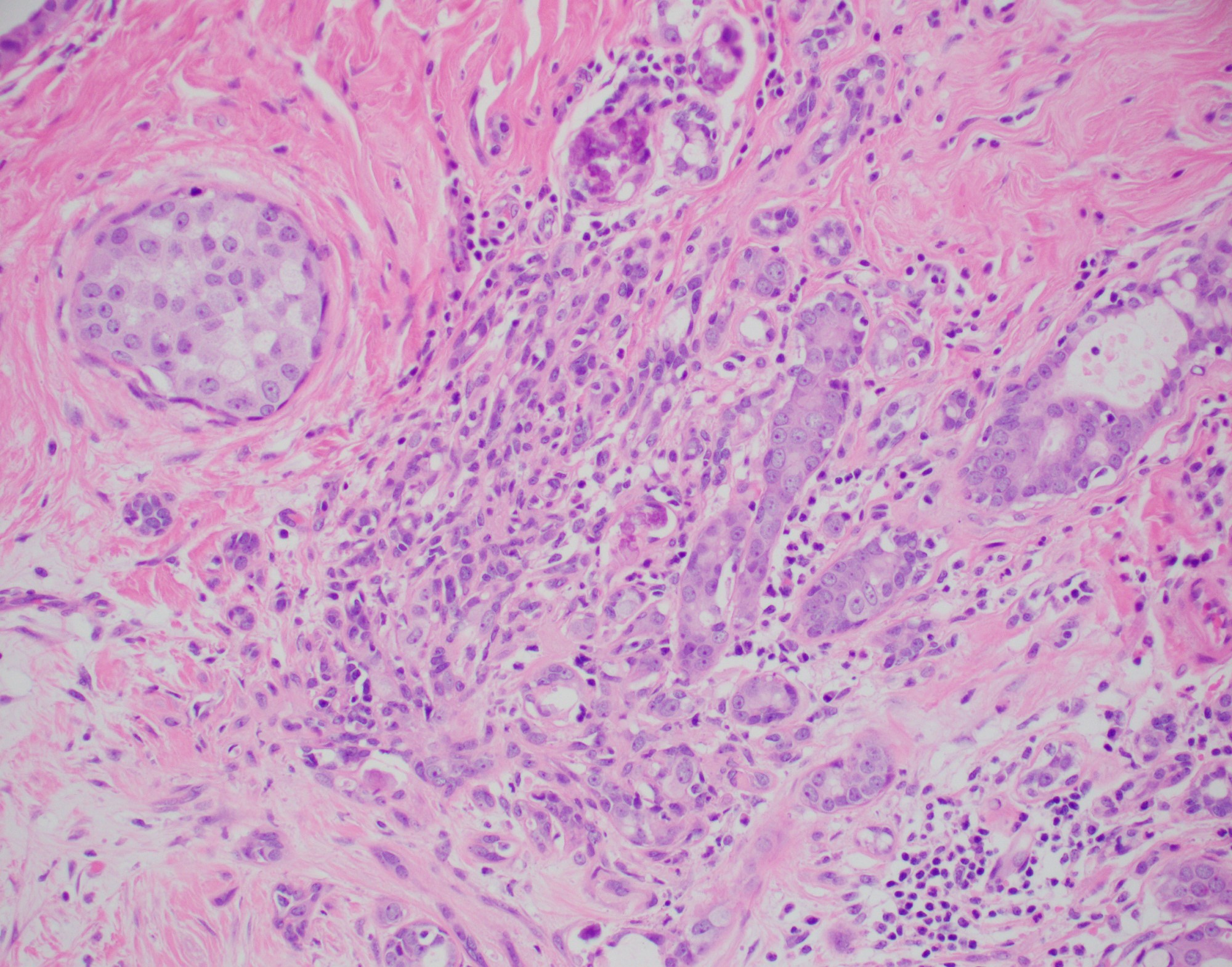
Sclerosing adenosis with DCIS
Cytology description
- Moderate to markedly cellular, with small to large groups of benign epithelial cells in acinar sheets / cohesive groups / tubules and scattered individual epithelial cells
- Also small foci of dense hyalinized stroma (Acta Cytol 2001;45:353, Diagn Cytopathol 2008;36:496)
- Tubules may have an angular configuration (Am J Clin Pathol 2012;138:96)
Positive stains
- Epithelial cells: CK7
- Myoepithelial cells: p63, CK5/6, calponin, alpha smooth muscle actin
- Basement membrane (surrounds tubules): laminin, type IV collagen
- Reference: Schnitt: Biopsy Interpretation of the Breast, 3rd Edition, 2017
Videos
Pathology mini tutorial
Sample pathology report
- Left breast, core biopsy:
- Fibrocystic changes including sclerosing adenosis with microcalcifications
Differential diagnosis
- Microglandular adenosis:
- Haphazardly distributed glands (lacks lobulocentric pattern)
- Lacks myoepithelium but has intact basement membrane
- Tubular adenoma:
- Well circumscribed
- Nodular growth may mimic nodular adenosis / adenosis tumor
- Uniform, closely packed tubules (lacks significant distortion by fibrosis)
- Invasive carcinoma:
- May be difficult to morphologically distinguish from florid sclerosing adenosis with marked distortion and/or involvement by atypia or DCIS
- Displays desmoplastic stromal response
- Lacks myoepithelium
- Invasive tubular carcinoma:
- More widely spaced tubules with single epithelial layer
- Displays desmoplastic stromal response
Additional references
Board review style question #1
A premenopausal woman underwent breast biopsy for screening detected microcalcifications showing the pictured lesion. This lesion typically is associated with
- Abundant cytologic atypia
- Clinically palpable mass
- Lack of myoepithelium
- Variable imaging features
Board review style answer #1
D. Variable imaging features. The pictured lesion is sclerosing adenosis, a benign breast lesion characterized by expansion of glands (with preserved 2 cell layers: inner epithelial and outer myoepithelial cells) within the terminal duct lobular unit with distortion by fibrosis / sclerosis. Most of the time, sclerosing adenosis lacks cytologic atypia. Sclerosing adenosis frequently has calcifications due to entrapped secretions. However, when abundant, sclerosing adenosis may present as a distortion or mass on imaging. Sometimes sclerosing adenosis clinically presents as a palpable mass, as with nodular adenosis / adenosis tumor. However, sclerosing adenosis can often be an incidental finding when there is another indication for biopsy. Thus, imaging findings are variable, depending on size and extent of the lesion.
Comment Here
Reference: Sclerosing adenosis
Comment Here
Reference: Sclerosing adenosis
Board review style question #2
Sclerosing adenosis of the breast (without atypia) imparts what risk for future breast cancer?
- No increased risk
- 1.5 - 2x increased risk
- 4 - 5x increased risk
- 8 - 10x increased risk bilaterally
- 8 - 10x increased risk ipsilaterally
Board review style answer #2
B. 1.5 - 2x increased risk. Sclerosing adenosis is considered part of the spectrum of proliferative fibrocystic changes, which imparts a 1.5 - 2x increased risk for future breast cancer. This is opposed to nonproliferative fibrocystic change which has no increased risk and atypical ductal hyperplasia (ADH) with 4 - 5x, ductal carcinoma in situ (DCIS) with 8 - 10x (unilateral: ipsilateral side) and lobular carcinoma in situ (LCIS) with 8 - 10x (bilateral) increased risk for breast cancer.
Comment Here
Reference: Sclerosing adenosis
Comment Here
Reference: Sclerosing adenosis
