
Breast
Other benign tumors
Nipple adenoma


Copyright: 2003-2025, PathologyOutlines.com, Inc.
PubMed Search: Nipple adenoma


- Nipple adenoma is a benign epithelial proliferation with a variety of morphological patterns that arise near the collecting ducts of the nipple and may be continuous with the overlying epidermis
- Benign, often florid, epithelial proliferation with retained myoepithelial cell layer involving superficial ducts of the nipple; the proliferation may extend and replace the overlying squamous epithelium resulting in erosion, hemorrhage and inflammation
- Histologic patterns include a mix of sclerosing adenosis, papillary hyperplasia and usual ductal hyperplasia
- Synonym: nipple duct adenoma
- Not recommended: florid papillomatosis of the nipple, erosive adenomatosis of the nipple, papillomatosis of the nipple, superficial papillary adenomatosis, papillary adenoma of the nipple
- Rare; occurs in males and females
- Most common in women in the fifth decade of life but has a wide age range (5 months to 89 years)
- Breast; superficial duct orifices of the nipple, the associated stroma and often the adjacent overlying epidermis
- Unknown
- Detected when small due to skin changes
- Clinically, epidermal involvement mimics the appearance of Paget disease
- On physical examination, small, palpable dermal nodule
- Nipple may appear eroded and erythematous as glandular epithelium replaces squamous epithelium
- Bleeding and exudative crust may be interpreted as nipple discharge
- If left untreated for years, may develop into large pedunculated mass (World J Surg Oncol 2014;12:91)
- Diagnosis can be made on biopsy (often of the skin due to clinical presentation) or cytology specimen and confirmed on excision
- Imaging findings are generally nonspecific (see Radiology description)
- Mammography: undetected in 33% of cases due to superficial location and small size (World J Surg Oncol 2014;12:91)
- Ultrasound: nonspecific; may detect a circumscribed mass for larger lesions, with or without cystic components, hypervascular on Doppler (Chin Med J (Engl) 2016;129:2386)
- MRI: nipple may show enhancement (J Comput Assist Tomogr 2006;30:148)
Images hosted on other servers:



Mammography, ultrasound and MRI of palpable left nipple mass with clear nipple discharge

Mammography, sonography and MRI images of nipple adenoma
- Can recur if not completely excised
- Risk of developing a subsequent breast cancer is comparable to other proliferative lesions of the breast (Am J Surg Pathol 1986;10:87)
- 22 year old woman with a papillomatous nodule on the left nipple from childhood (Clin Case Rep 2020;8:3254)
- 46 year old woman with pedunculated papillomatous mass on top of the nipple of the right breast (BMJ Case Rep 2019;12:e231516)
- 49 year old woman with a reddish nodule with surface crust on the nipple of the right breast (Dermatol Online J 2021;27)
- 82 year old woman with small painful mass in the right axilla (Diagn Pathol 2012;7:162)
- Surgical excision depending on the size and extent of lesion (ANZ J Surg 2015;85:444)
- Alternative treatments:
- Mohs micrographic surgery (Dermatol Surg 2016;42:684)
- Cryotherapy (Breast J 2016;22:584, Ann Dermatol 2021;33:182)
Images hosted on other servers:

Nipple erythema and induration

Eroded crusted nipple adenoma

Nipple nodule with erosion

Pedunculated papillomatous nipple adenoma

Accessory breast nipple adenoma

Erosion and bloody discharge

Nipple adenoma, preoperative and postconservative excision
- Rubbery; white to gray; 0.5 cm to > 4 cm
Images hosted on other servers:

Complete nipple resection
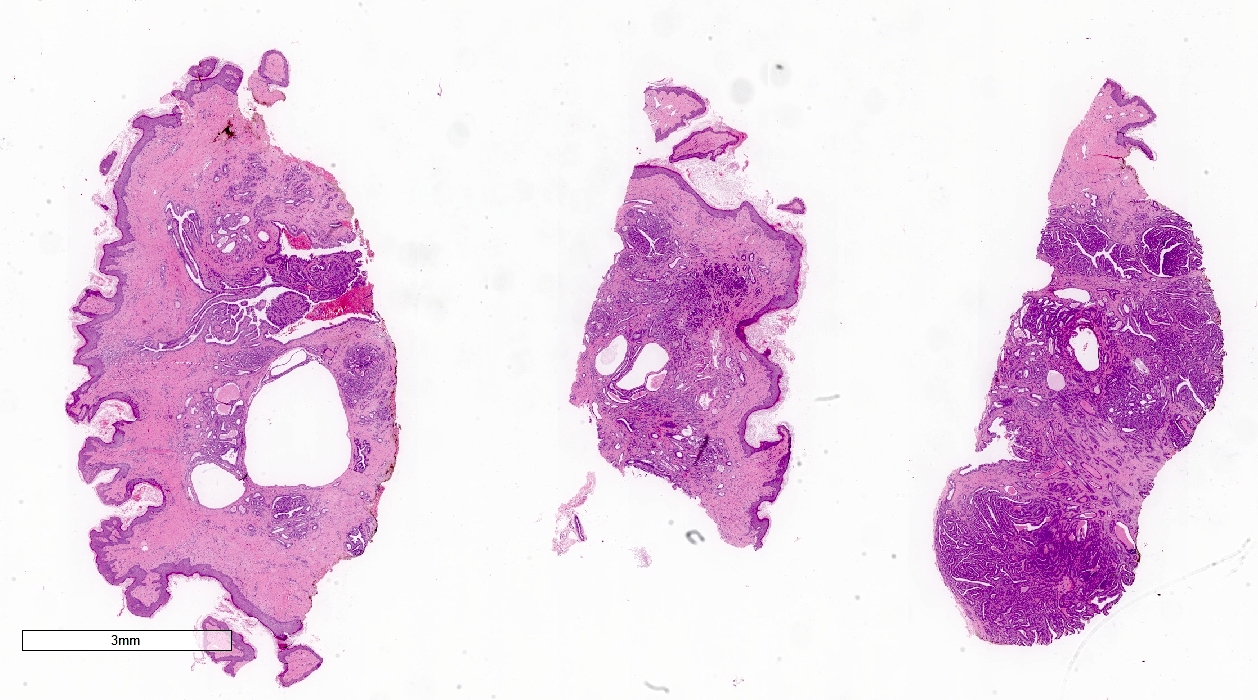
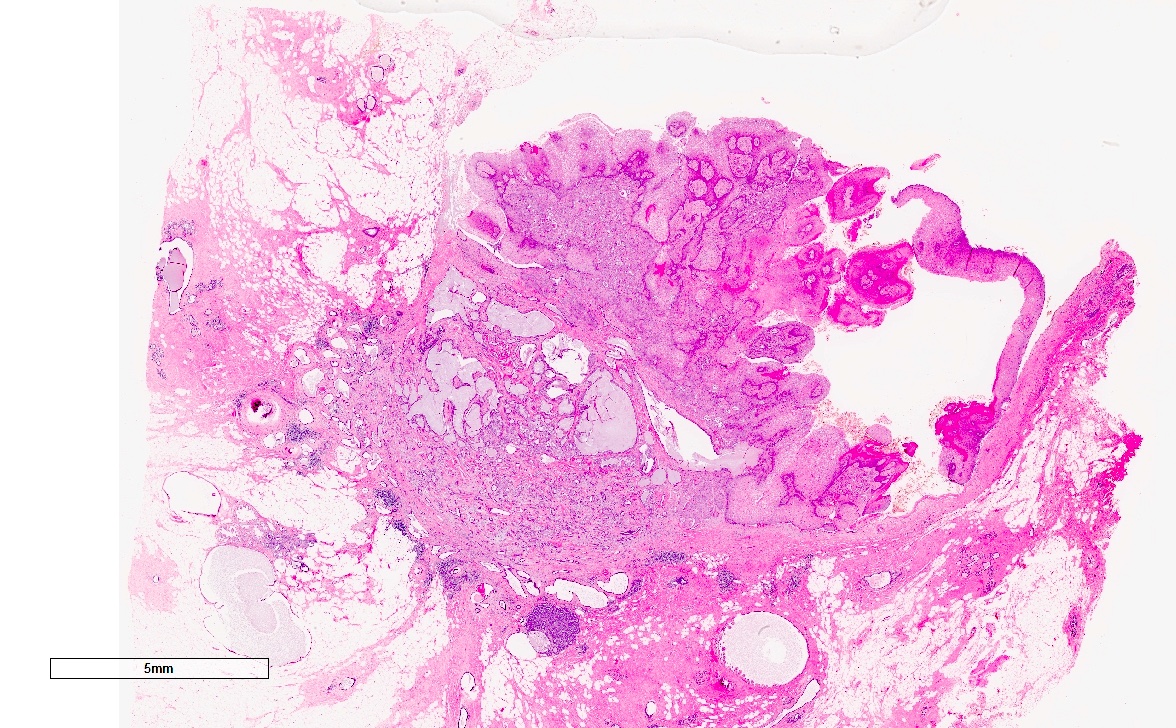
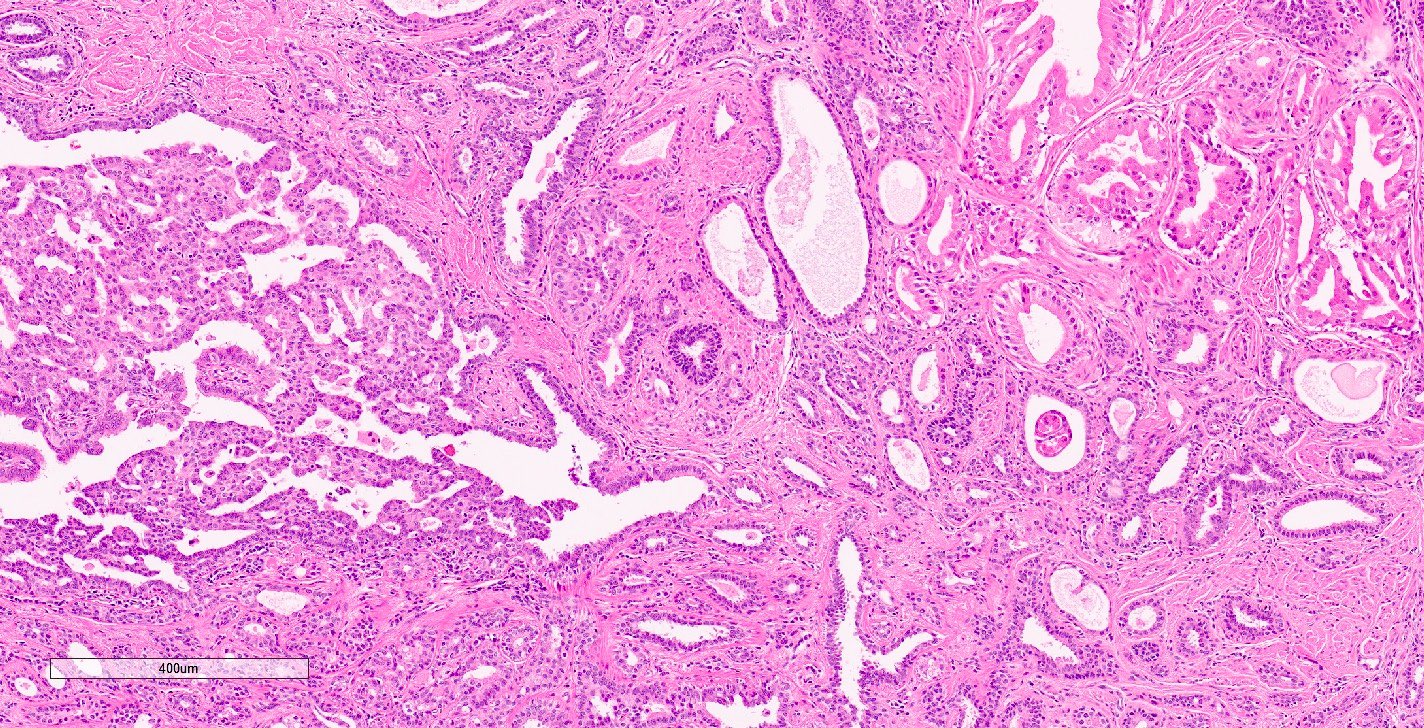
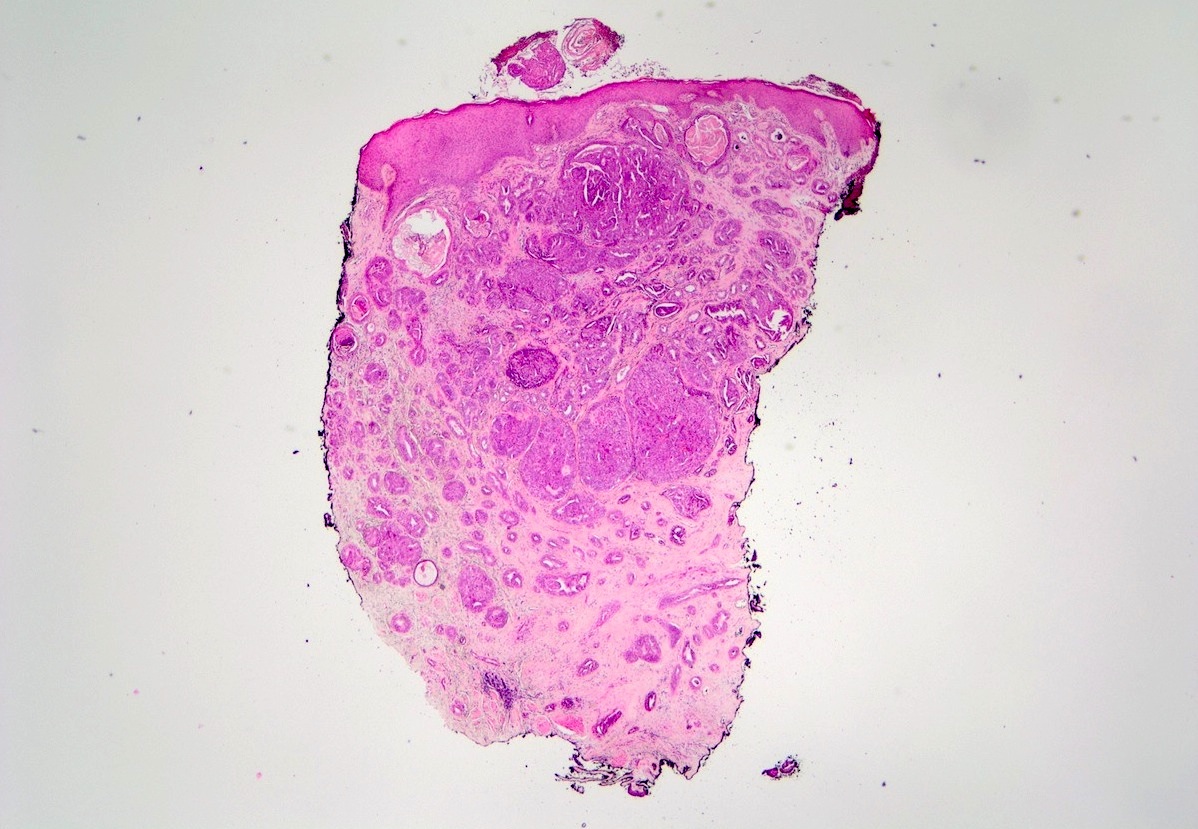
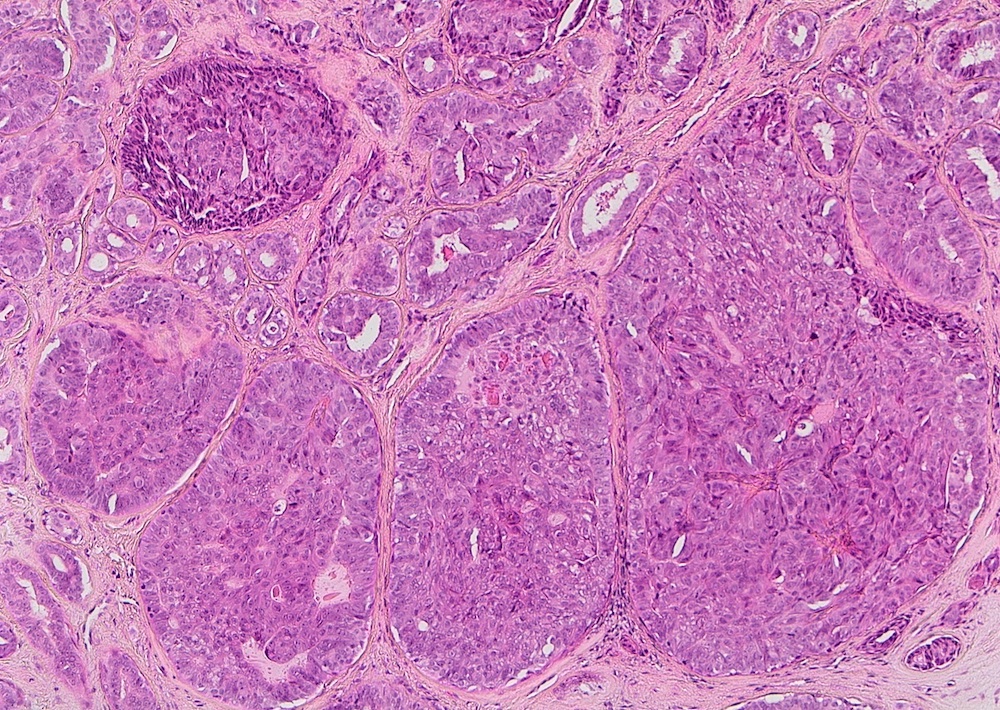
- Glandular nests of various sizes with diffuse growth within ducts lined by myoepithelial cells; complex and irregular structure may falsely mimic invasion (Chin Med J (Engl) 2007;120:630)
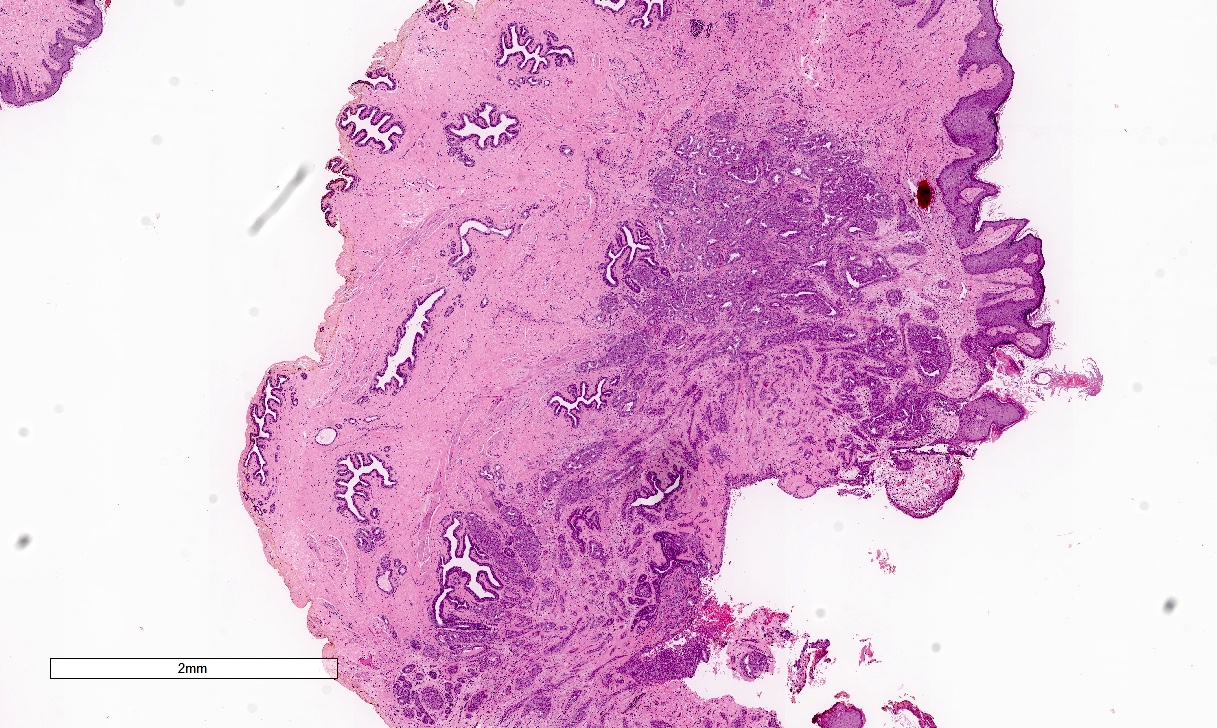
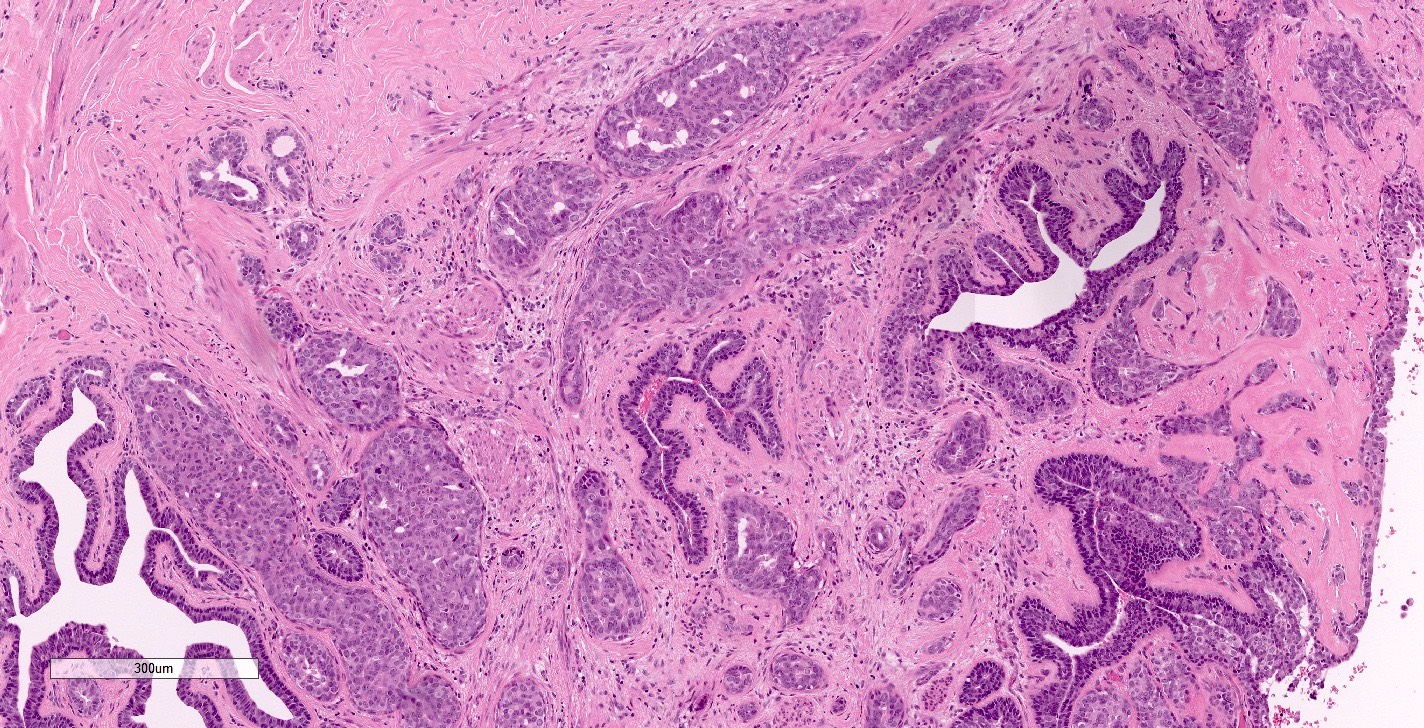
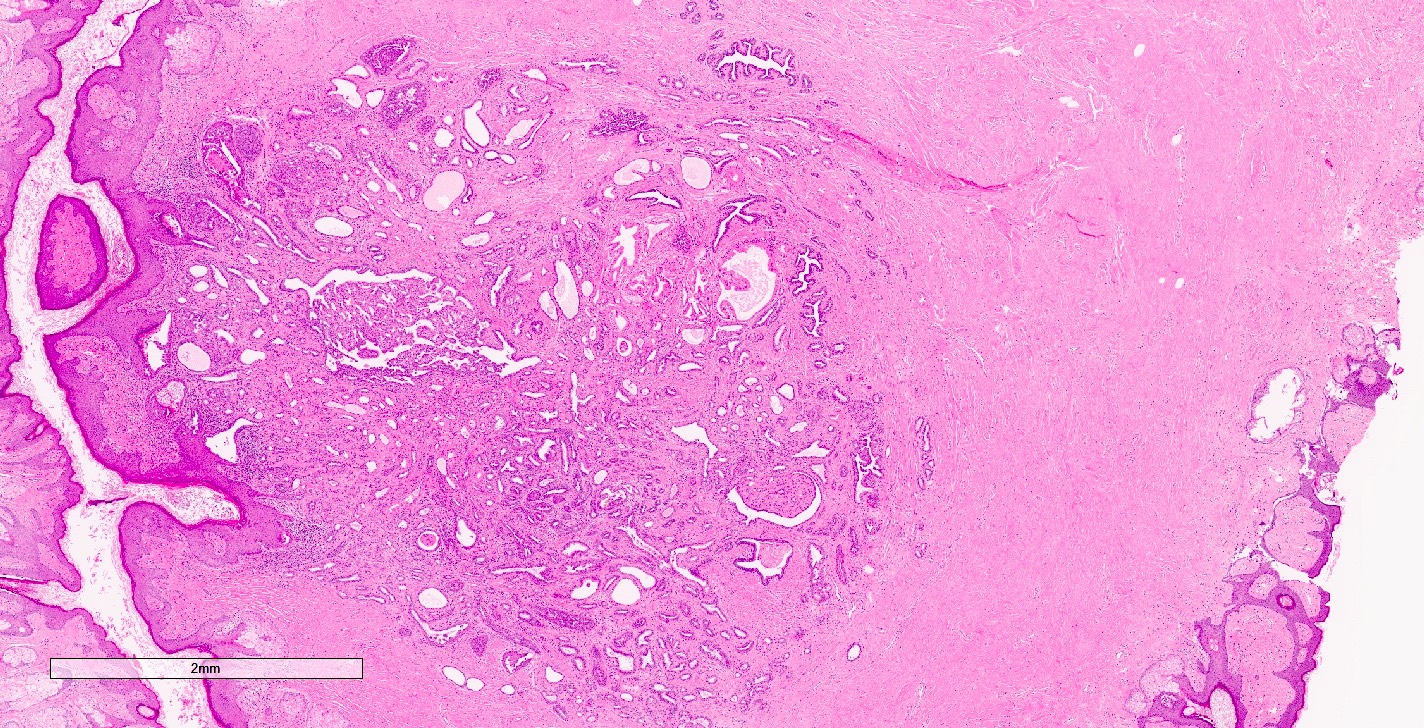
- Nodular florid epithelial proliferation of the lactiferous ducts of the nipple with papillary hyperplasia / adenosis / sclerosis / mixed pattern
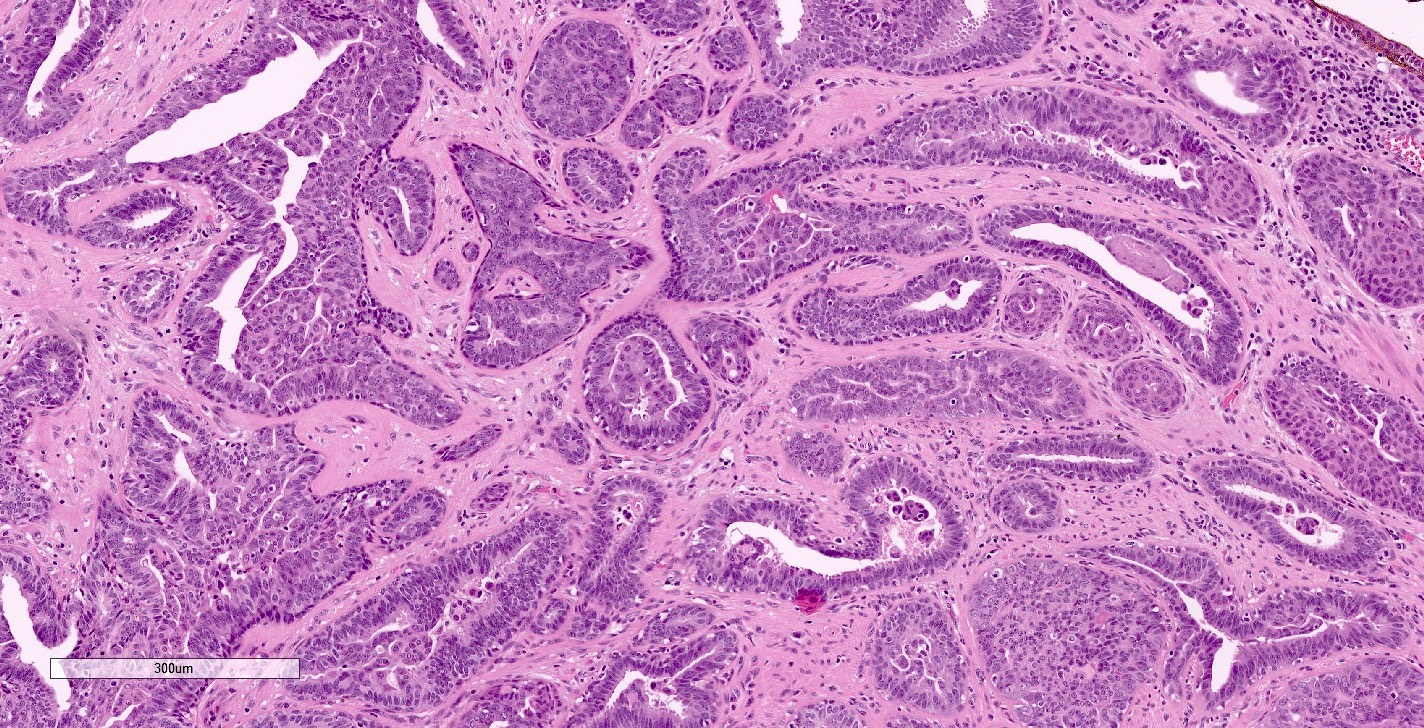
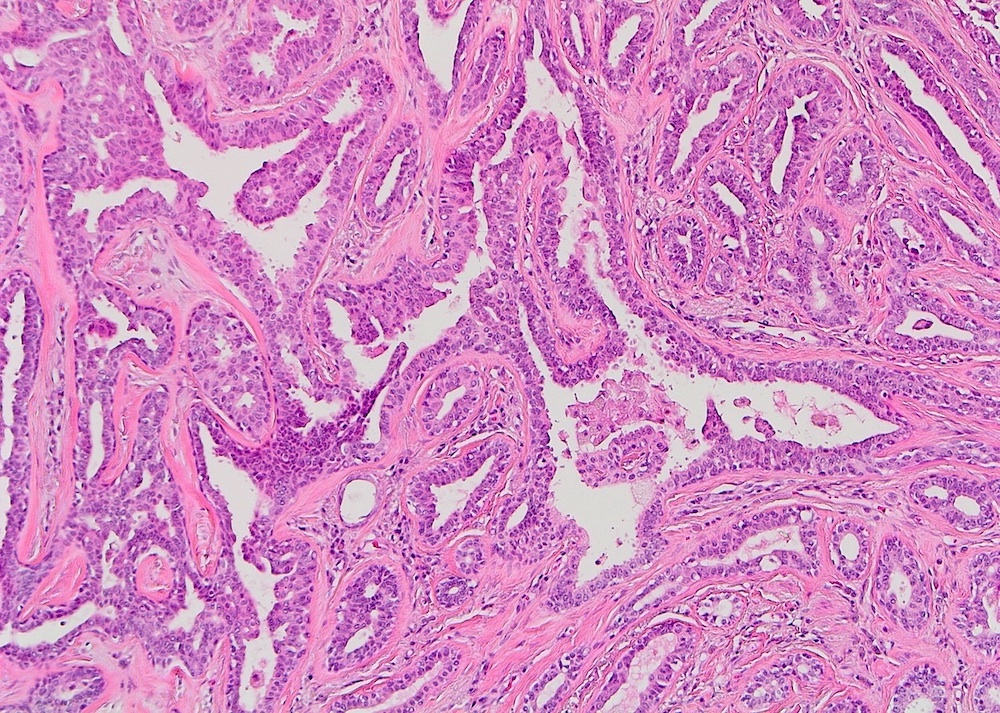
- Epithelium is cytologically bland
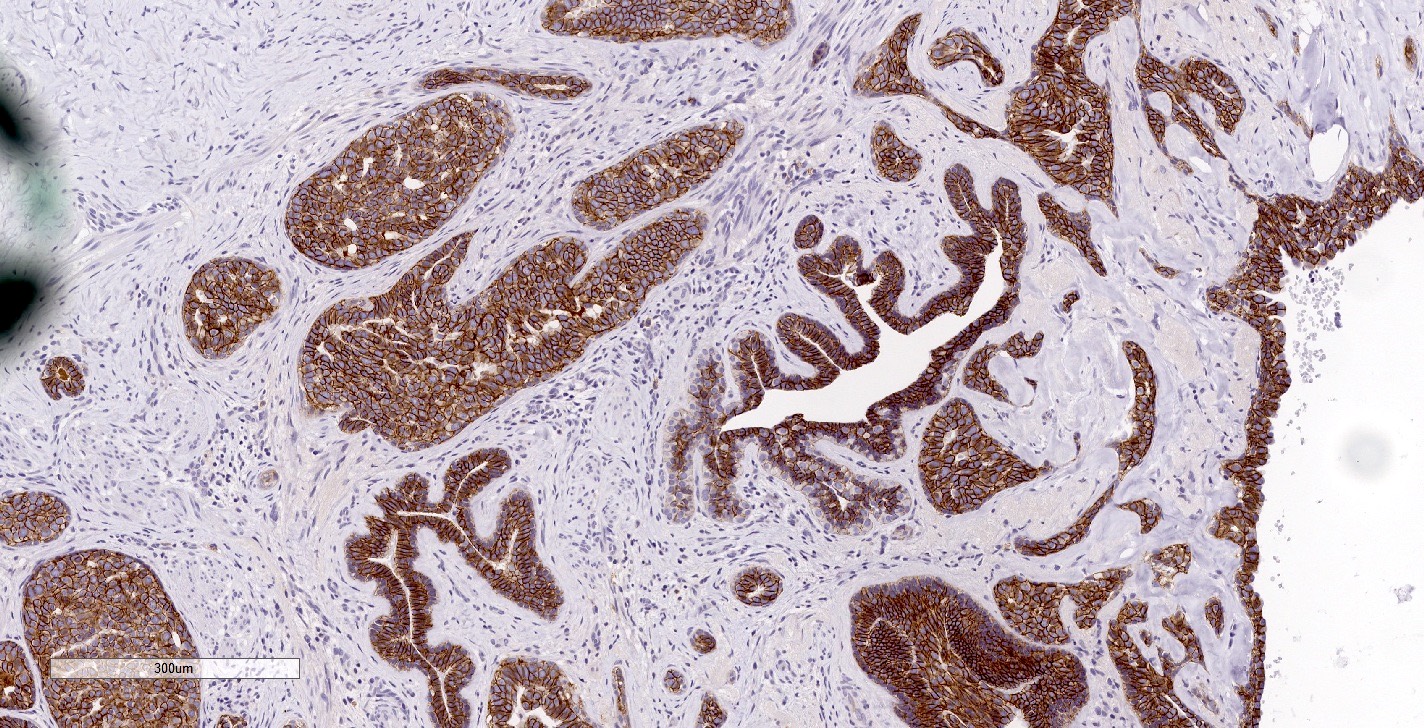
- Myoepithelial cell layer is preserved uniformly (Mod Pathol 1990;3:288)
- 4 major morphologic patterns:
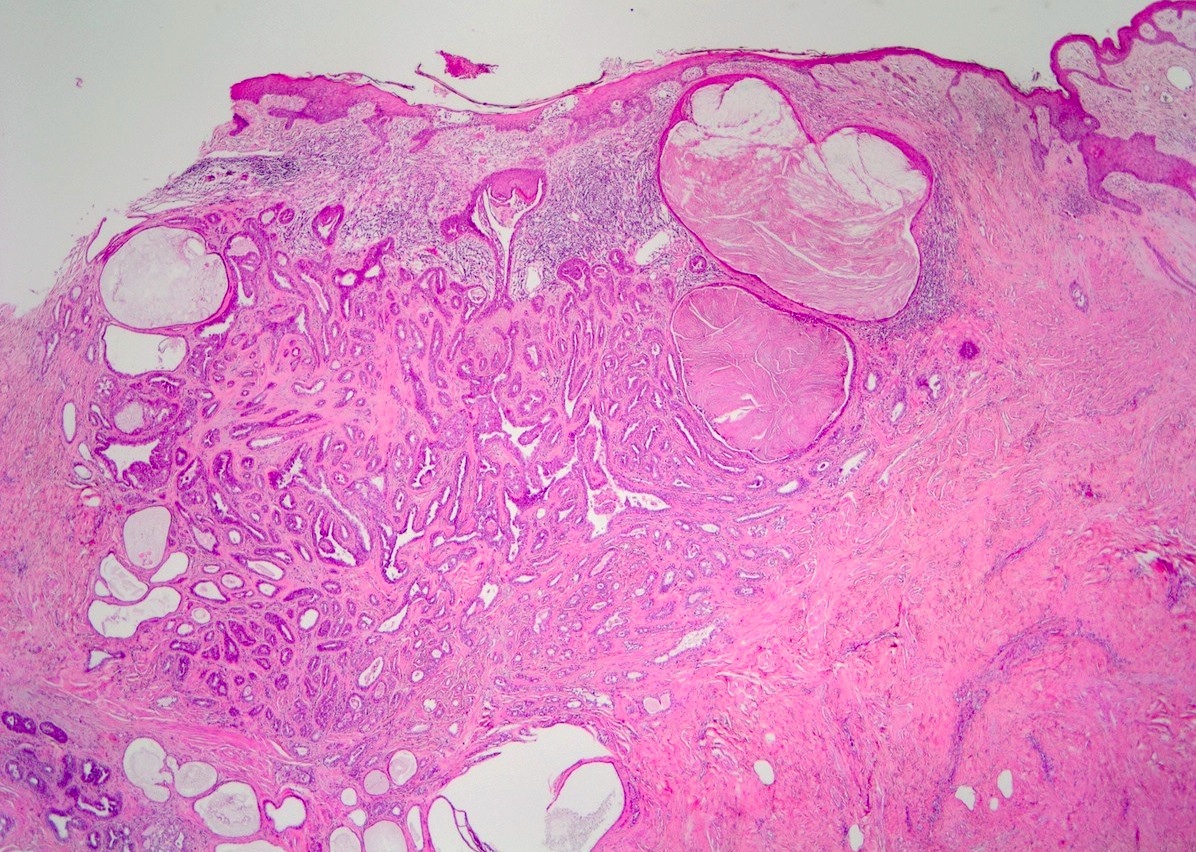
- Sclerosing papillary hyperplasia pattern:
- Intraductal papillary growth with prominent stromal proliferation (collagenous bands, myxoid change or elastosis)
- Focal central necrosis may be present
- Squamous cysts can be present in duct orifices
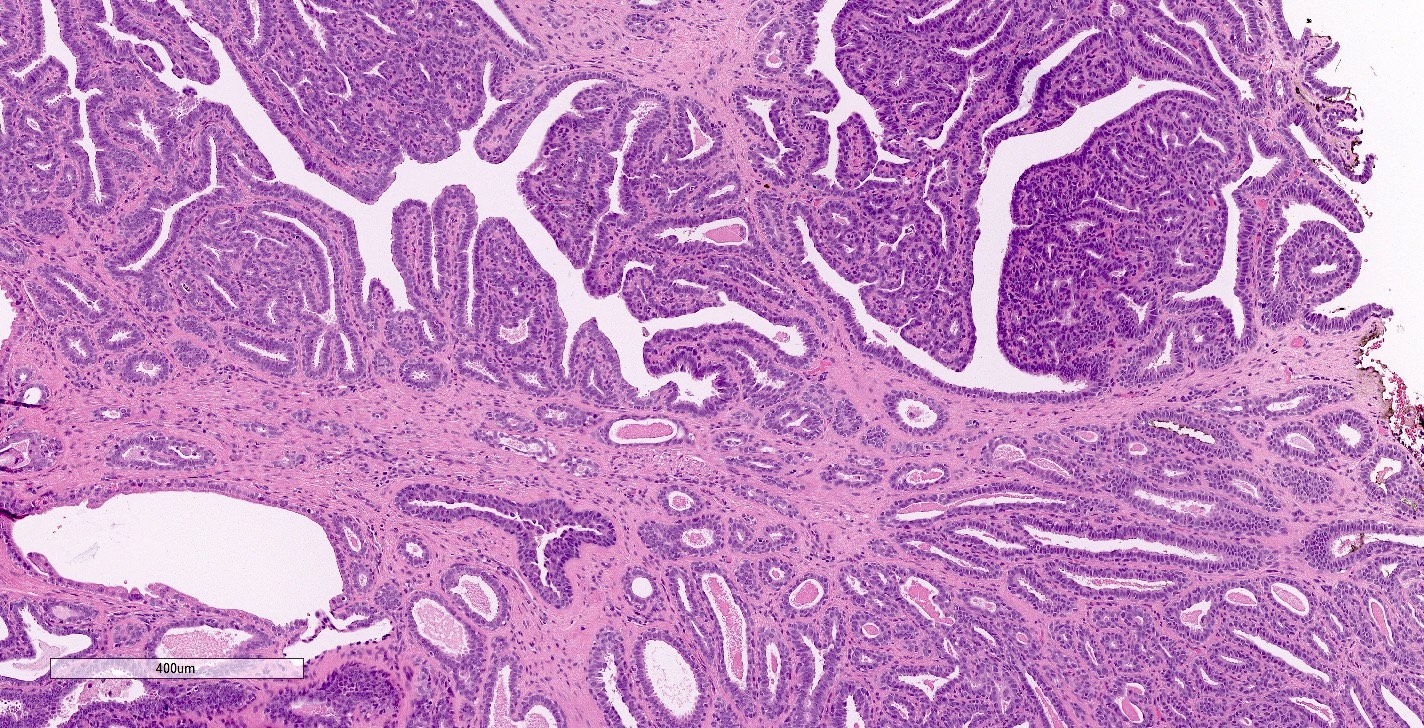
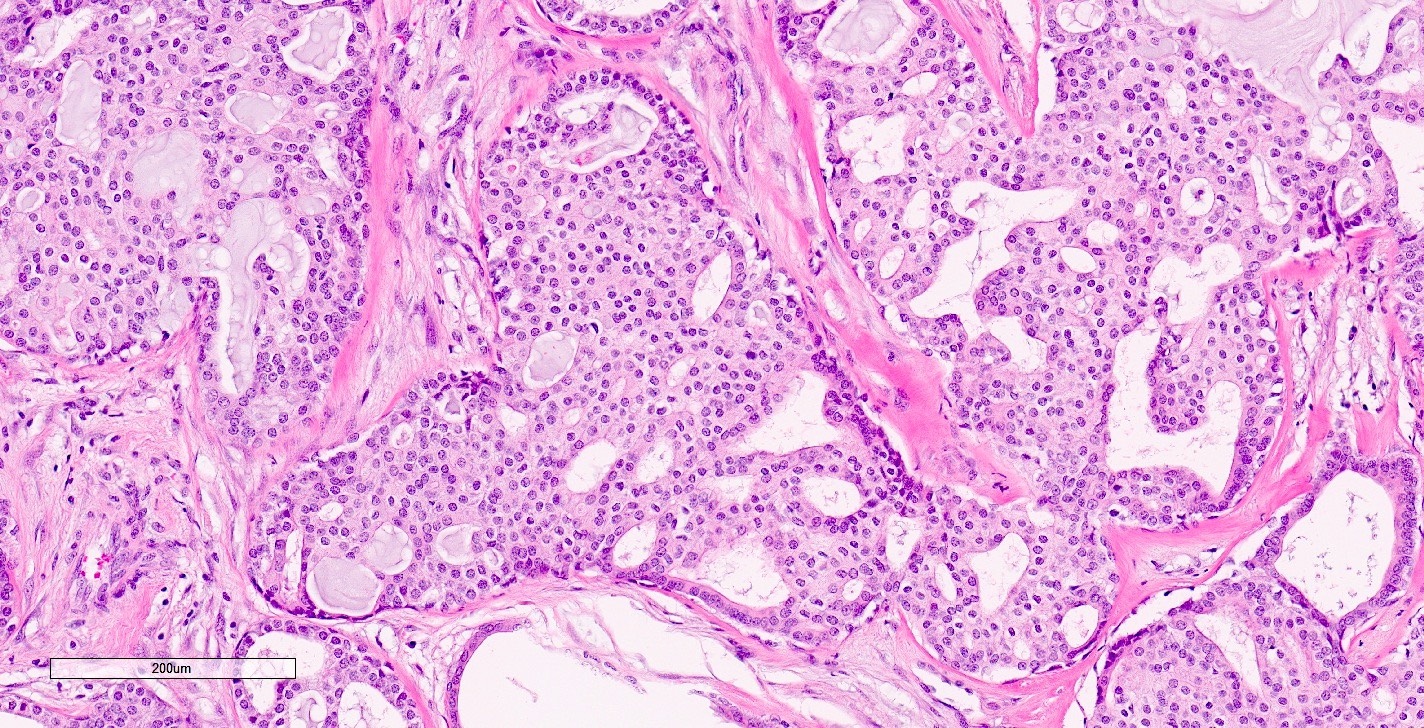
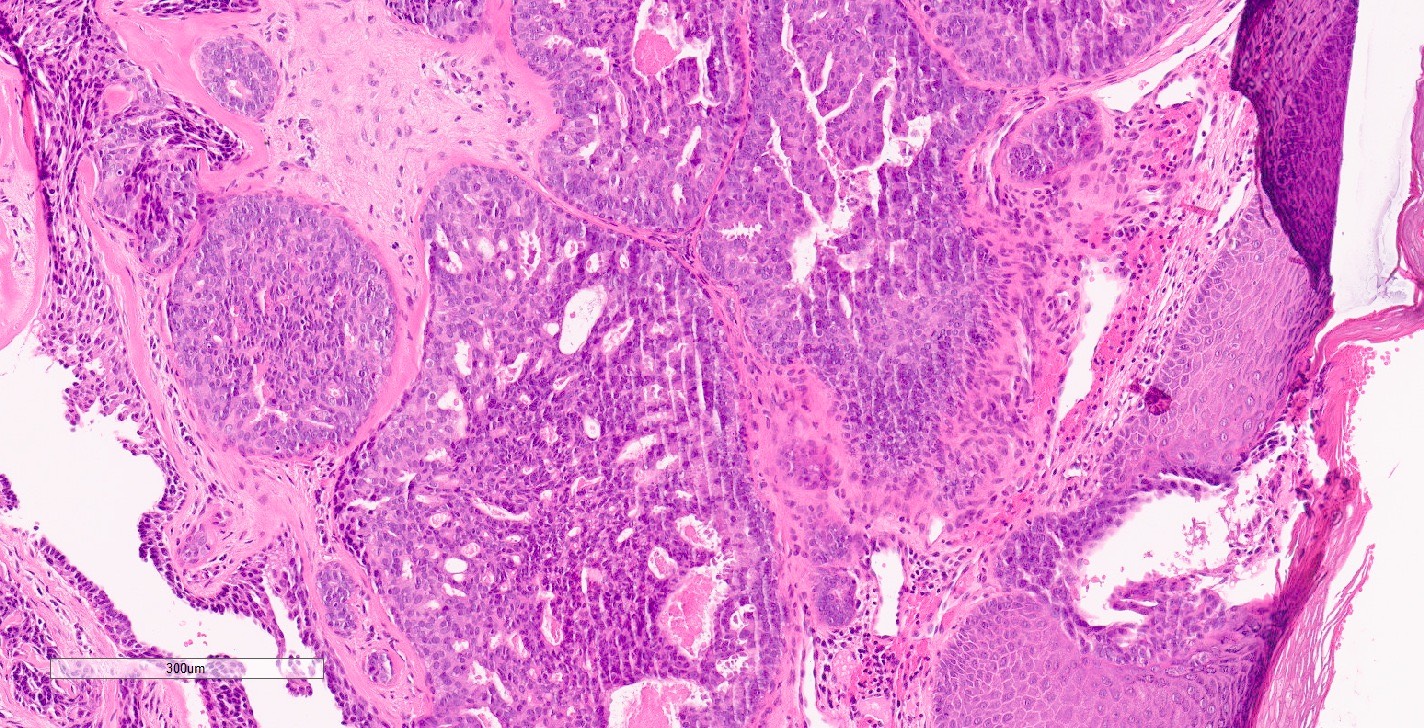
- Papillary hyperplasia pattern:
- Papillary growth in large ducts with less prominent stromal proliferation and focal necrosis
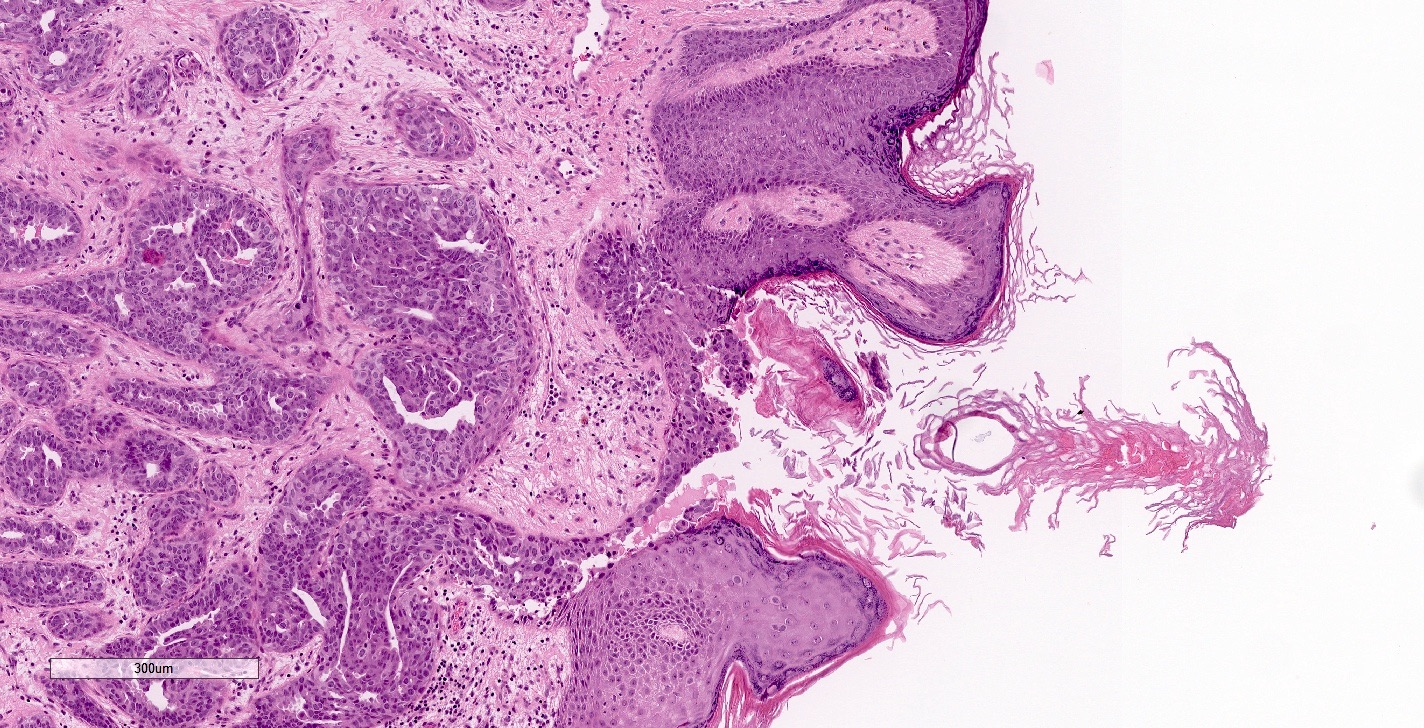
- Replacement of epidermis with glandular epithelium
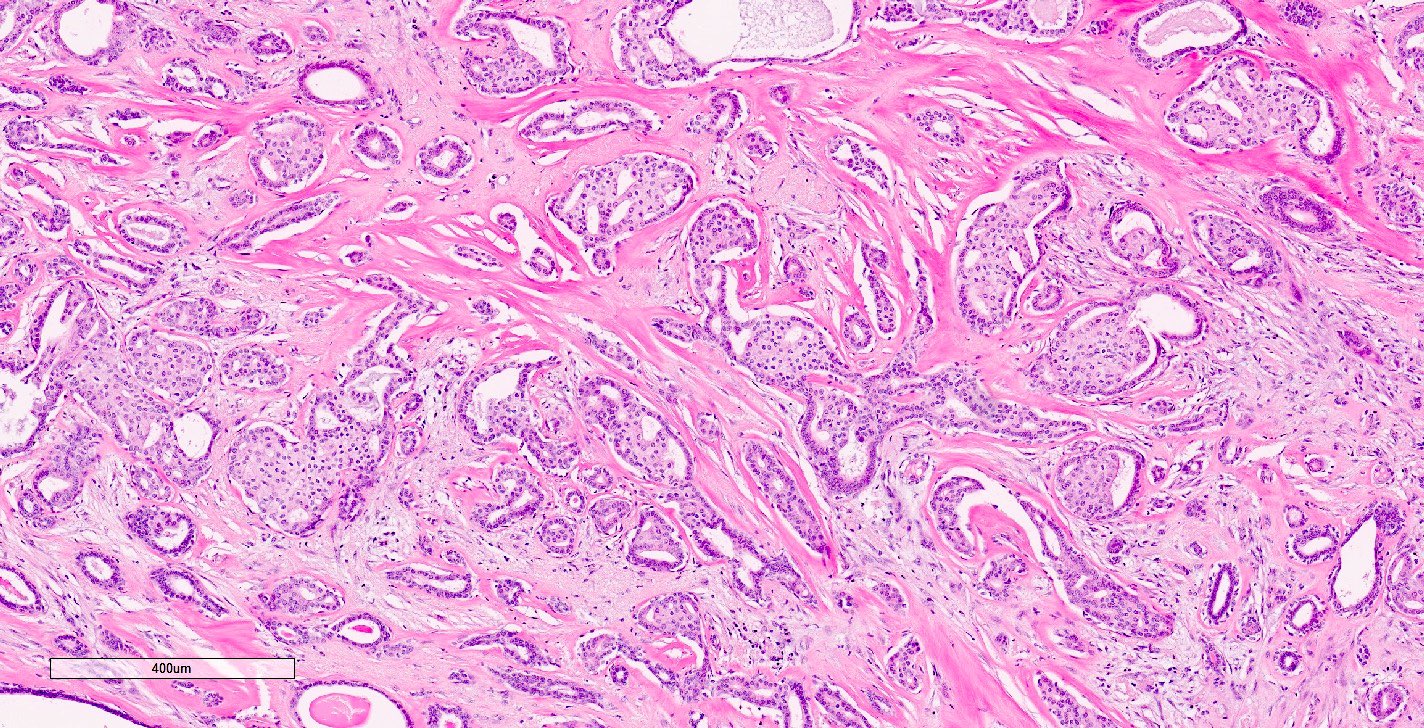
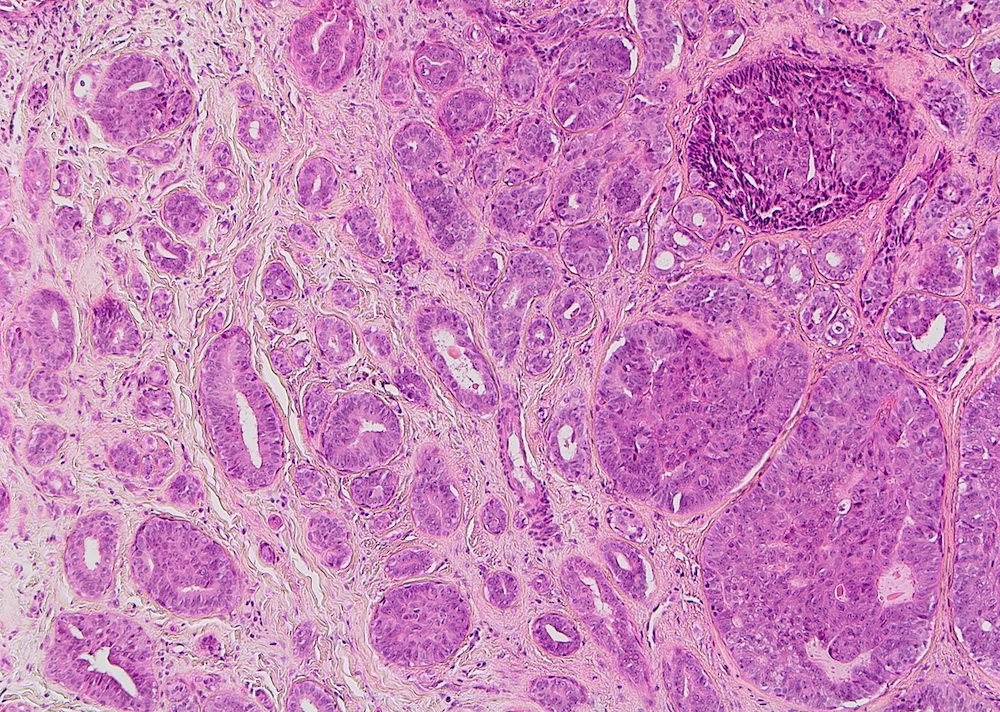
- Adenosis pattern:
- Small duct proliferation with a pattern resembling sclerosing adenosis and may be pseudoinfiltrative
- Necrosis is uncommon
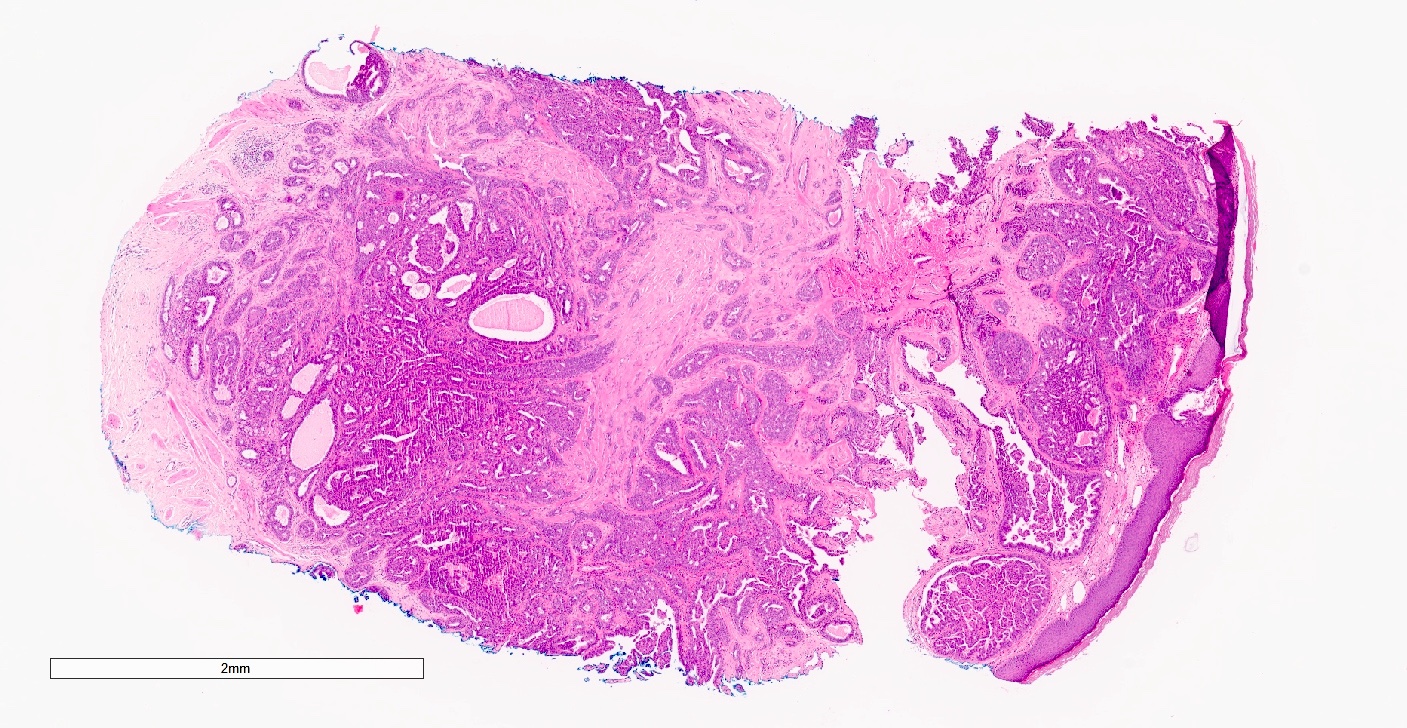
- Mixed pattern:
- Any combination of the above described patterns (Am J Surg Pathol 1986;10:87)
- Sclerosing papillary hyperplasia pattern:
- May be in continuity with the skin surface, which may appear eroded or ulcerated
- Fairly well circumscribed but unencapsulated (Br Med J 1963;1:563)
- Other features often seen:
- Squamous metaplasia and superficial keratin cysts
- Acanthosis
- Toker cell hyperplasia in the epidermis
- Multinucleated giant cells
- Apocrine metaplasia (Oncol Lett 2014;7:1839)
- In rare cases, ductal carcinoma in situ involving an adenoma or a contiguous invasive carcinoma have been reported (Mod Pathol 1995;8:633)
Contributed by Hal Berman, M.D., Ph.D., Miralem Mrkonjic, M.D., Ph.D. and Mary Ann Gimenez Sanders, M.D., Ph.D.
Epidermal involvement
Focal ulceration
Shave biopsy of nipple
Nipple duct involved by benign papillary proliferation

Well circumscribed epithelial proliferation
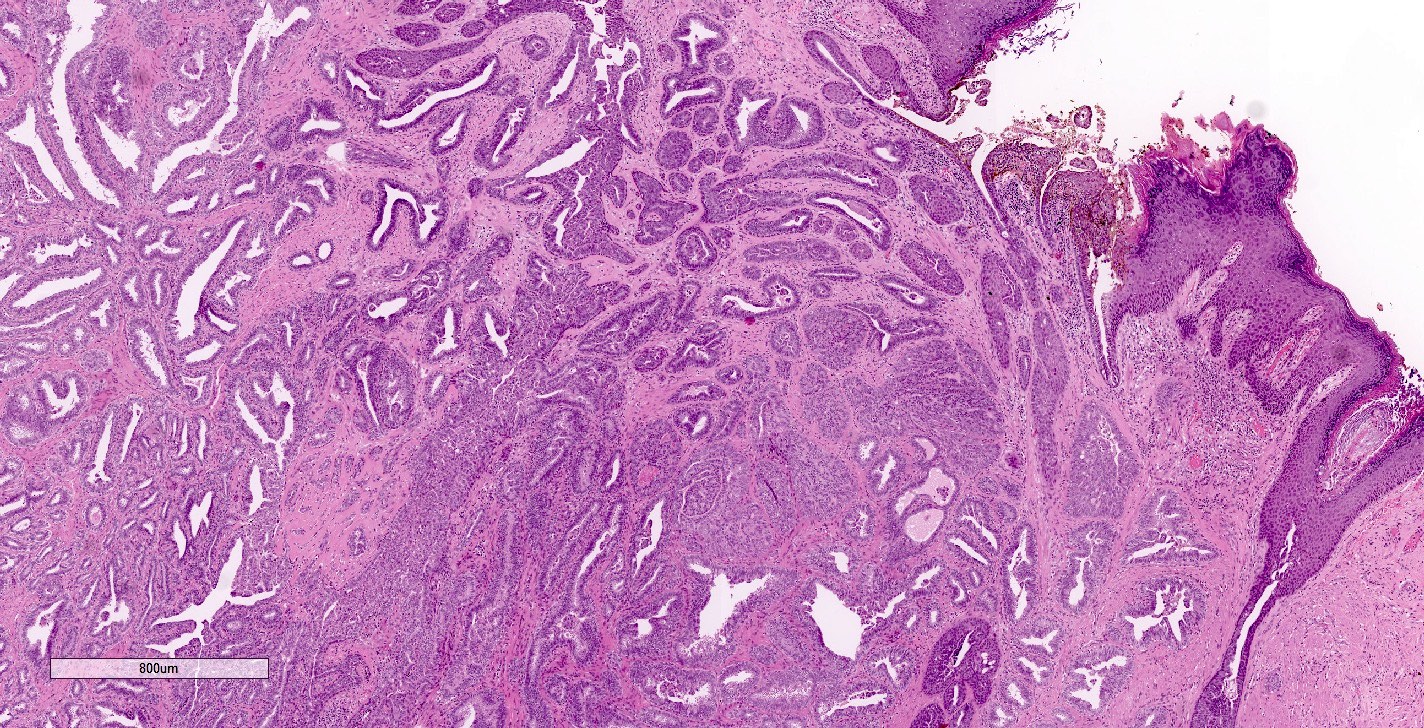
Epithelial hyperplasia and epidermal ulceration
Usual ductal hyperplasia with focal squamous metaplasia
Prominent squamous hyperplasia
Ductal carcinoma in situ
Prominent epithelial
proliferation with
papillary architecture
and tufting
Nipple section
Mixed pattern on mastectomy

Sclerosing adenosis
Papillary growth within ducts
Mixed pattern on punch biopsy
Florid usual ductal hyperplasia
Small tubules
Prominent epithelial proliferation
Images hosted on other servers:

Nipple adenoma sclerosing

Nipple adenoma adenosis pattern

Nipple adenoma papillomatous pattern

Nipple adenoma florid usual ductal hyperplasia
- Obtained by fine needle aspiration (FNA), brush cytology or tumor imprint cytology
- Reported features vary; benign when myoepithelial cells are detected
- FNA:
- Large cell clusters with a papillary or sheet structure, as well as small clusters and solitary epithelial cells in a necrotic background
- Duct epithelial and myoepithelial 2 cell pattern in the clusters
- Round to oval or spindle nuclei, fine and bland chromatin
- Brush cytology (Diagn Cytopathol 2015;43:664):
- Small papillary clusters with attached myoepithelial cells and solitary epithelial cells in a hemorrhagic or neutrophilic background
- Round to oval nuclei, with smooth contour, bland and granular chromatin
- Squamous metaplasia-like cells present
- Cytology often classified as atypical or suspicious, especially in the presence of coagulative necrosis (ANZ J Surg 2015;85:444)
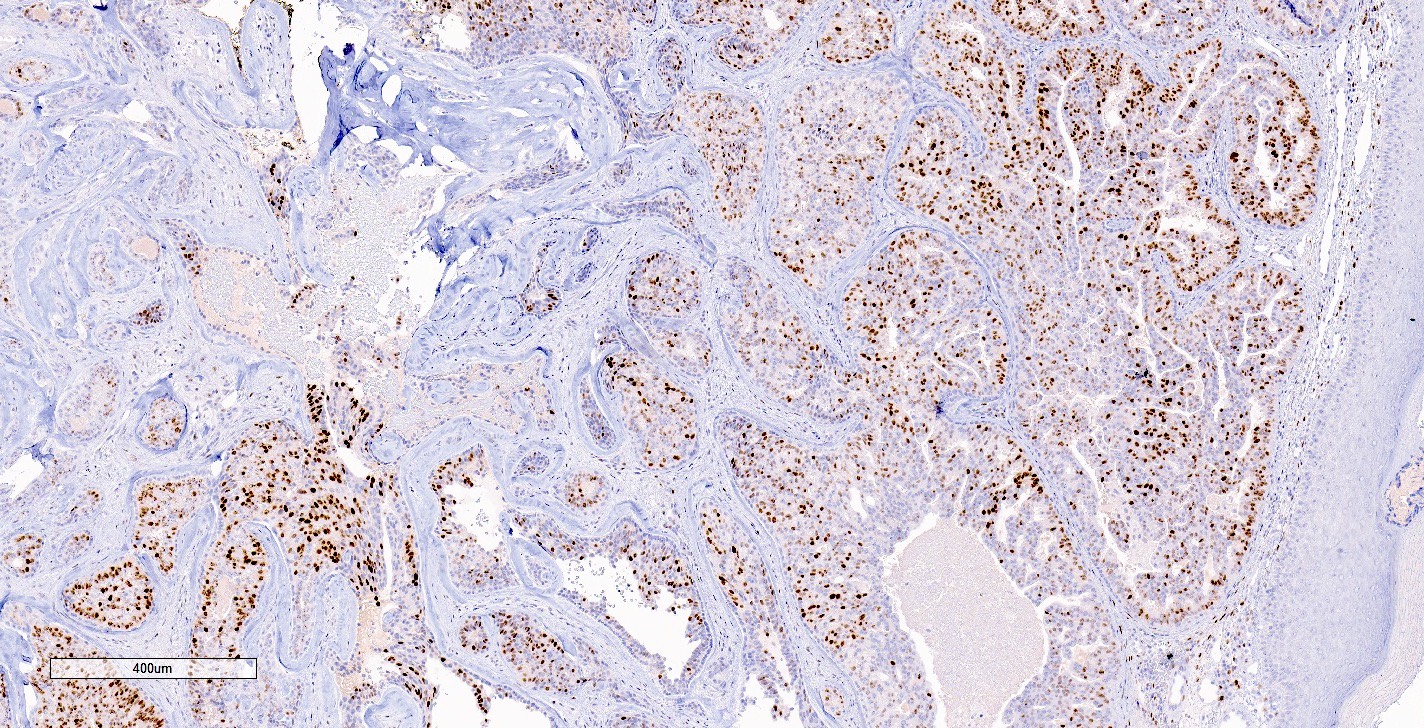
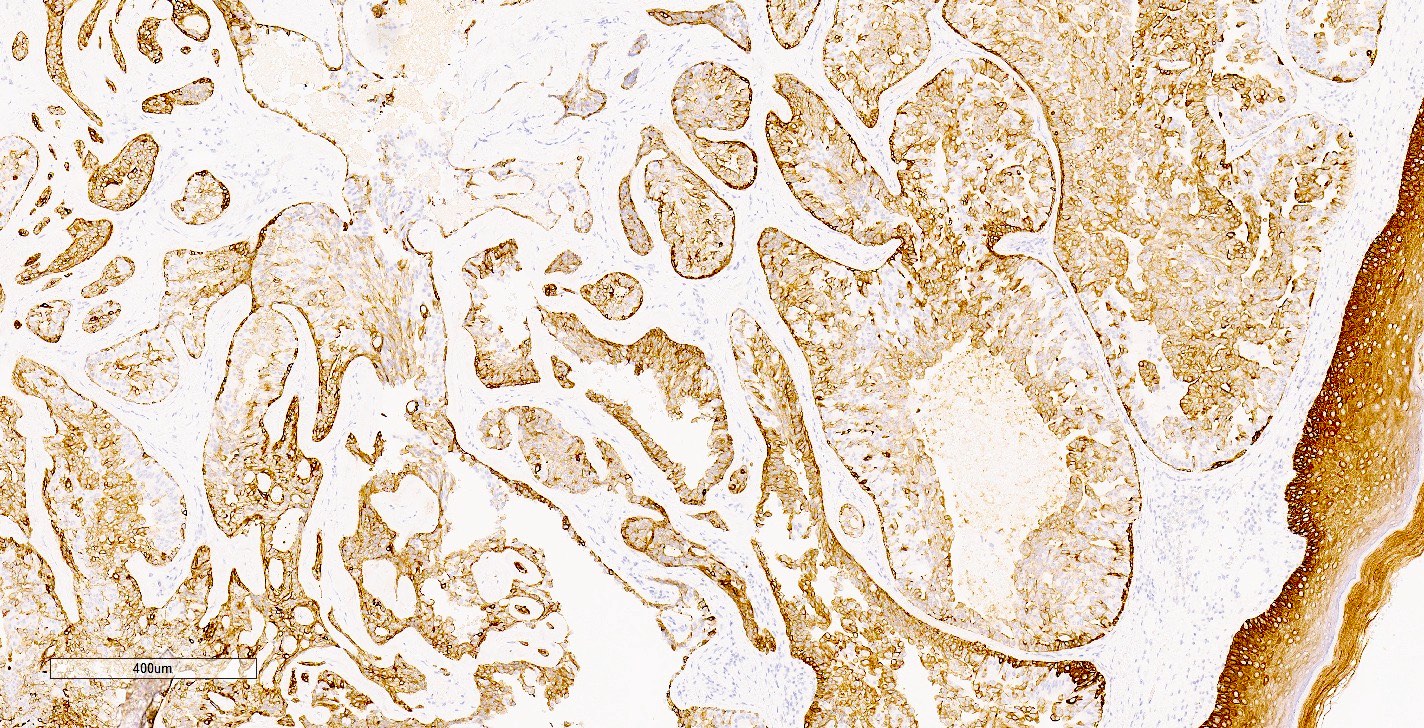
- AE1 / AE3, CK7: positive in epithelium (Mod Pathol 2003;16:893, Oncol Lett 2014;7:1839)
- p63, smooth muscle myosin, calponin: positive in myoepithelium (Oncol Lett 2014;7:1839, Am J Surg 2010;200:e39)
- ER and CK5/6: heterogeneous, mosaic type staining of the epithelium with florid usual ductal hyperplasia (Am J Surg Pathol 2010;34:896, Oncol Lett 2014;7:1839)
- Activating PIK3CA mutations reported in 12/24 cases
- KRAS (1/24 cases) and BRAF mutations (2/24 cases) (Histopathology 2017;70:195)
Dr. Jerad Gardner presents normal nipple histology and 2 cases of nipple adenoma
3 minute overview of the presentation and histology of nipple adenomas
- Right breast (nipple), punch biopsy:
- Nipple adenoma (see comment)
- Comment: Sections show ductal proliferation involving a large nipple duct with areas of papillary growth and usual ductal hyperplasia in continuity with the epidermis. Ductal epithelial cells are cuboidal to columnar with eosinophilic cytoplasm and bland nuclei. Focal areas of stromal sclerosis are identified. Immunohistochemistry for smooth muscle myosin and p63 highlights the myoepithelial cell layer while ER and CK5/6 show heterogeneous staining patterns of epithelial cells. Taken together, the histomorphology and immunohistochemistry are consistent with a nipple adenoma.
- Syringomatous tumor:
- Ducts with teardrop, comma and branching shapes
- Infiltrative growth with desmoplastic stroma, may see perineural invasion
- Does not involve the epidermis
- Invasive ductal carcinoma, no special type (low grade):
- Negative for myoepithelial cell markers (p63, smooth muscle myosin, calponin)
- Infiltrative growth pattern
- DCIS:
- Intraductal papilloma:
- Similar to nipple adenoma
- Papillary projections with fibrovascular cores
- Arises below the skin surface, involves lactiferous ducts within deeper breast parenchyma and is unlikely to be a palpable subdermal mass
- Tubular adenoma:
- Well circumscribed
- Uniform glands with scant stroma
- Encapsulated papillary carcinoma:
- Circumscribed mass found deeper in the breast compared with nipple adenomas
- Cytologic atypia
- Myoepithelial cells absent in papillae and along the periphery
A punch biopsy of the nipple was performed to sample a nodular lesion associated with skin changes in a 48 year old woman. What is the diagnosis?
- Ductal adenoma
- Intraductal papilloma
- Nipple adenoma
- Paget disease of the breast
- Tubular adenoma
Comment Here
Reference: Nipple adenoma
- CK7
- ER
- HER2
- p53
- p63
Comment Here
Reference: Nipple adenoma
- HER2 positivity is an essential characteristic of nipple adenomas
- Myoepithelial cells are absent in nipple adenoma
- Sclerosing adenosis, papillary hyperplasia and epithelial hyperplasia can be seen in mixed patterns in a nipple adenoma
- The presence of necrosis excludes nipple adenoma in the differential diagnosis
- The skin changes that can be seen in nipple adenoma are clinically distinct from Paget disease
Comment Here
Reference: Nipple adenoma
