
Breast
Other carcinoma subtypes, not WHO classified
Tubulolobular carcinoma
Authors: Hafsa Nebbache, M.D., S. Emily Bachert, M.D.
Editorial Board Member: Kristen E. Muller, D.O.
Deputy Editor-in-Chief: Gary Tozbikian, M.D.

Last author update: 16 April 2024
Last staff update: 16 April 2024
Copyright: 2001-2025, PathologyOutlines.com, Inc.
PubMed Search: Tubulolobular carcinoma


Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Etiology | Clinical features | Diagnosis | Radiology description | Prognostic factors | Case reports | Treatment | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Positive stains | Negative stains | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1Cite this page: Nebbache H, Bachert SE. Tubulolobular carcinoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/breastmalignanttubulolobular.html. Accessed April 1st, 2025.
Definition / general
- Carcinoma with mixed histologic features of both tubular carcinoma and invasive lobular carcinoma (Virchows Arch 2006;448:500)
Essential features
- Carcinoma with areas of tubular carcinoma and invasive lobular carcinoma
- Most are estrogen receptor (ER) positive and HER2 negative
- Not synonymous with invasive carcinoma with ductal and lobular features
Terminology
- In the 5th edition of the WHO Classification of Breast Tumours, tubulolobular carcinoma is considered a histologic variant of invasive lobular carcinoma; however, many authors consider this histological pattern a variant of invasive breast carcinoma of NST (Diagnostics (Basel) 2022;12:2658)
ICD coding
- ICD-11: XH3RK9 - tubulolobular carcinoma
Epidemiology
- Rare; 1 - 2% of all invasive breast carcinomas
- Predominantly in women; has been reported in men
- Mean age is 59 - 60 years (range: 43 - 79) (Zhonghua Bing Li Xue Za Zhi 2012;41:681, Am J Surg Pathol 2004;28:1587)
Sites
- Breast
- Single case report in the anogenital region (Am J Surg Pathol 2006;30:1193)
Etiology
- Etiology is multifactorial: genetics, hormones, diet, age and reproductive factors are risk factors (WHO 5th edition)
- ER positive pathway of breast cancer development characterized by gains of 1q and losses of 16q (WHO 5th edition)
- See etiologies associated with low grade, ER positive invasive breast cancer of no special type (NST)
- Expression of E-cadherin supports ductal differentiation, despite a dominant lobular growth pattern (Am J Surg Pathol 2004;28:1587)
Clinical features
- Can be multifocal (~20%) (Am J Surg Pathol 1997;21:653)
- Presence of palpable mass (85%) (Eur J Radiol 2006;60:418)
- Usually presents at early pathologic stage, pT1 and N0 disease (75%) (Mod Pathol 2007;20:130)
Diagnosis
- Diagnosis can be made on core needle biopsy or resection specimens
Radiology description
- Most common finding on mammography and ultrasound is an irregular mass (Eur J Radiol 2006;60:418)
- Dense stroma may aid in the early detection of these tumors (Am J Surg Pathol 2004;28:1587)
Prognostic factors
- Intermediate prognosis between that of classic invasive lobular carcinoma and pure tubular carcinoma (Breast Care (Basel) 2008;3:423)
- 25% of patients present with stage II disease or higher (compared with 0% for tubular carcinomas and 60% for invasive lobular carcinomas) (Mod Pathol 2007;20:130)
- Multifocal disease and positive axillary lymph nodes are more common in tubulolobular carcinoma (60%) compared with tubular carcinomas (33%) (Mod Pathol 2007;20:130, Am J Surg Pathol 2004;28:1587)
Case reports
- 60 year old woman with tubulolobular carcinoma of the breast with focal targetoid pattern (Int J Med Sci Public Health 2014;3:1018)
- 64 year old woman with mammary type tubulolobular carcinoma of the anogenital area (Am J Surg Pathol 2006;30:1193)
- 67 year old woman with tubulolobular carcinoma of the breast with periglandular collagen IV immunostaining (Breast Care (Basel) 2008;3:423)
- 69 year old woman with tubulolobular carcinoma of the breast with grooved and cerebriform nuclei (Diagn Cytopathol 2011;39:54)
- 70 year old woman with tubulolobular carcinoma of the breast with metastases to the colon (Onco Targets Ther 2014;7:435)
Treatment
- Localized excision / mastectomy
- Choice of treatment is based on the size and the tumor stage: localized excision, radical or modified radical mastectomy, hormone therapy and adjuvant therapy (Mod Pathol 2007;20:130)
Gross description
- Ill defined, firm, gray tumor, usually measuring < 2 cm in greatest dimension, ranging in size from 0.5 cm to 2.5 cm (median, 1.4 cm) (Am J Surg Pathol 2004;28:1587)
Microscopic (histologic) description
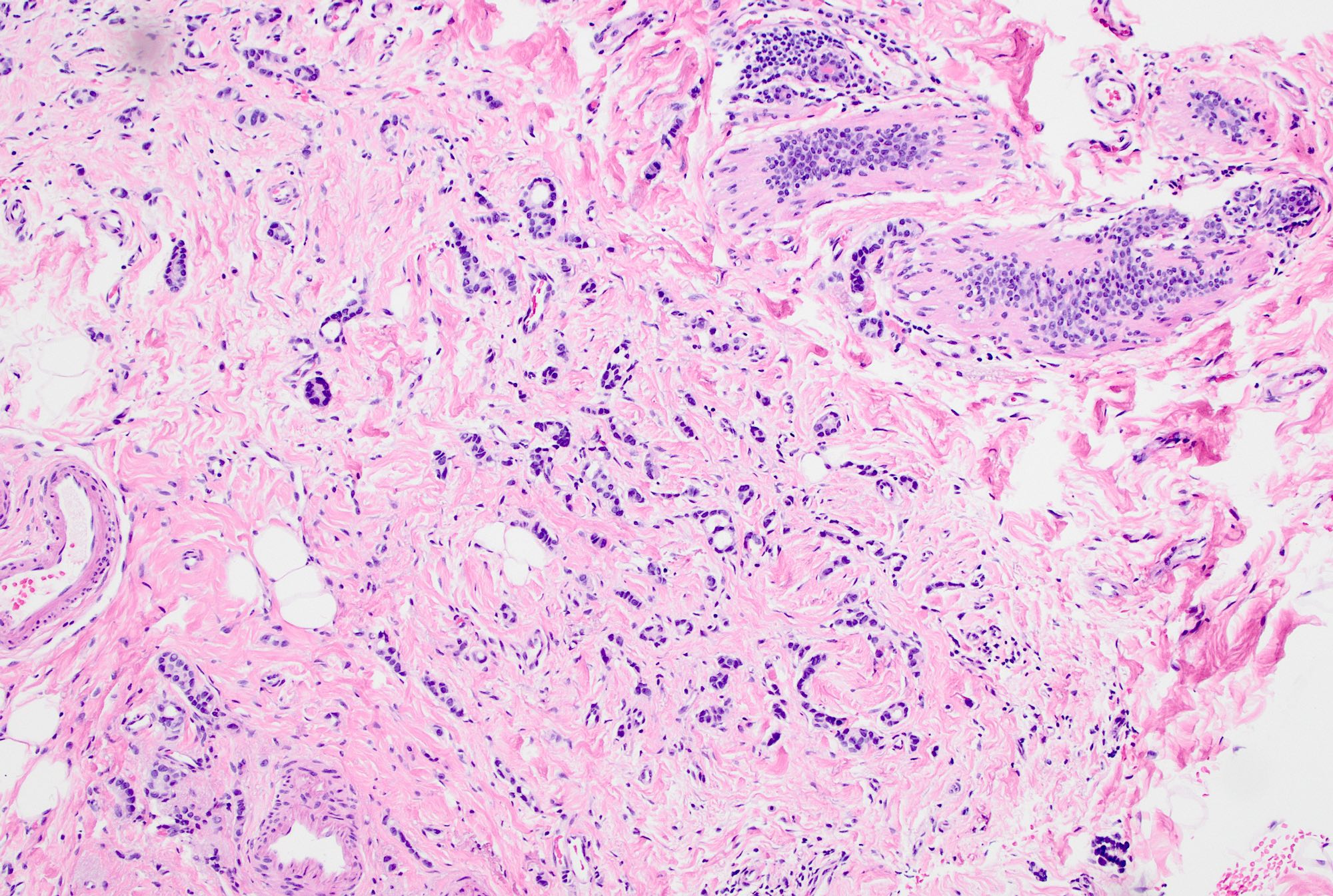
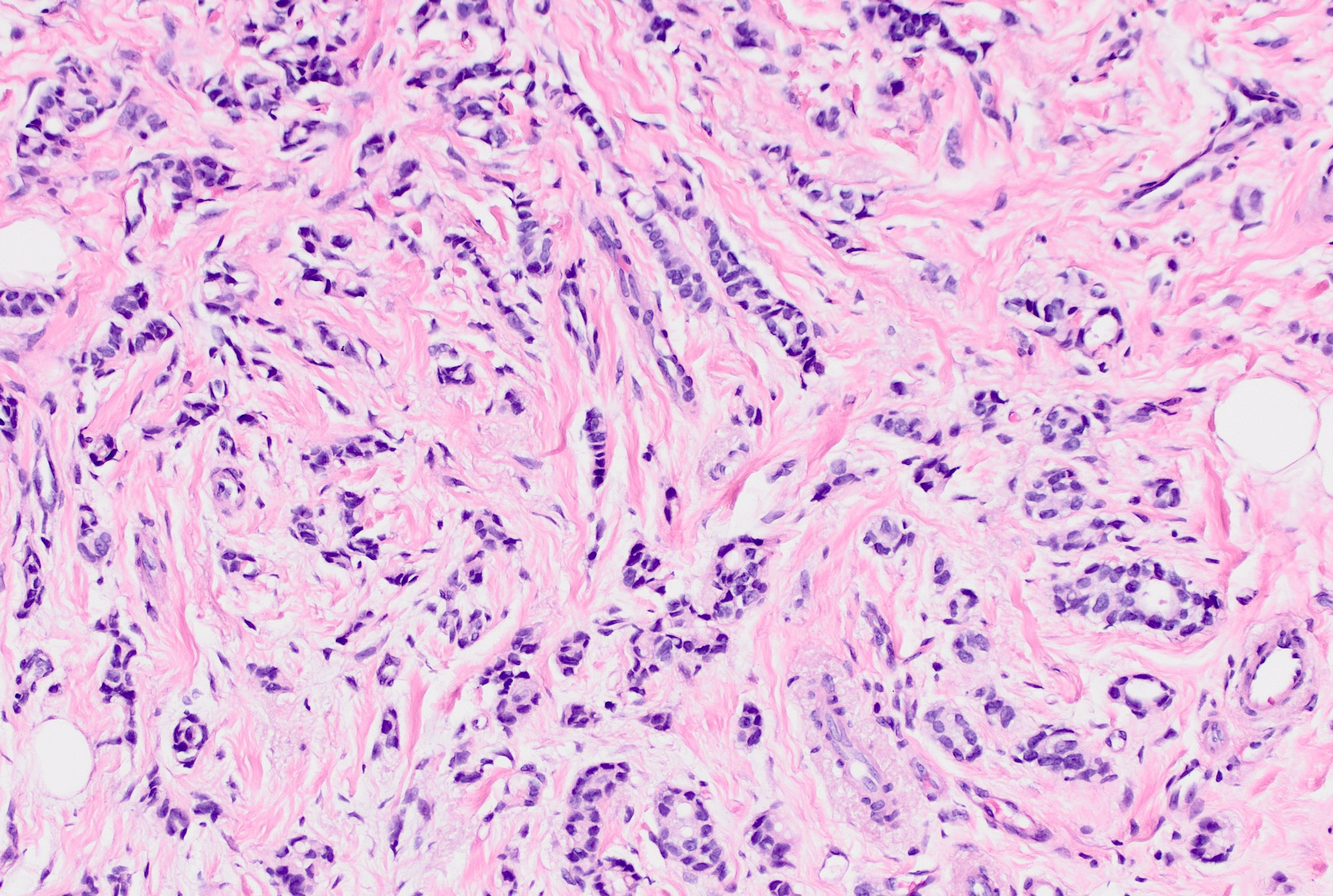
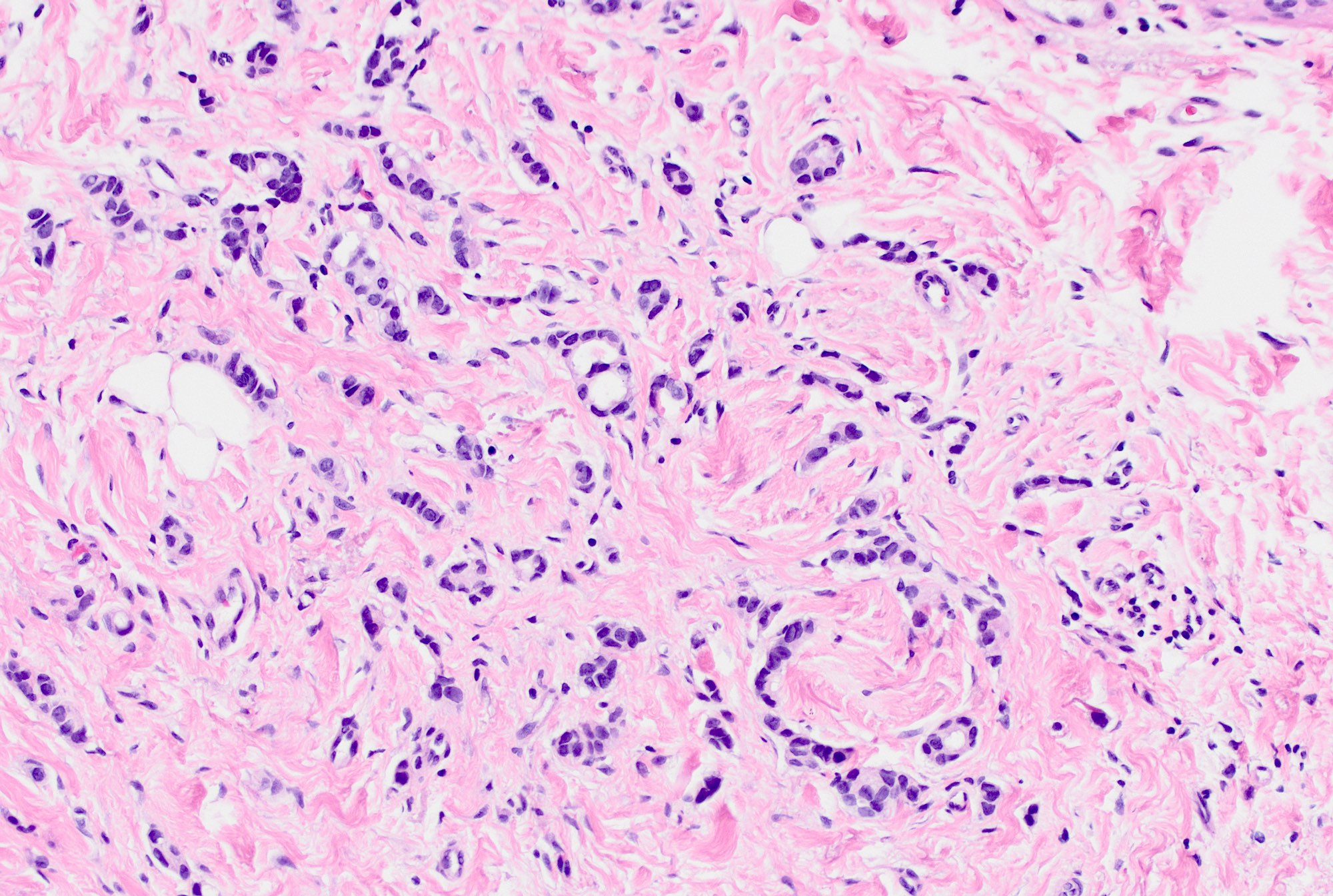
- Invasive tumor with mixed pattern of small tubules with a lobular pattern of infiltration within a dense collagenous stroma often with prominent elastosis
- Tubular component: small, round to angulated tubules with low grade nuclei and variable apical snouts
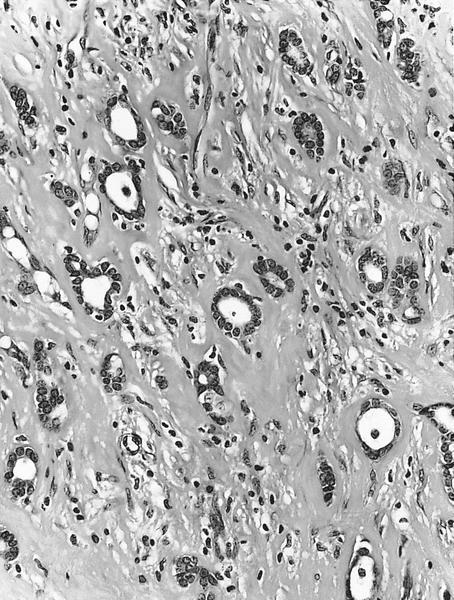
- Lobular component: single cells, single file cords of cells, often displaying targetoid growth around benign ducts
- Cells are uniform and display low grade nuclear atypia (nuclear grade 1 or 2) with inconspicuous nucleoli and minimal amphophilic cytoplasm
- Cells with lobular growth pattern may show occasional intracytoplasmic lumina and rare signet ring morphology
- Can have variable proportion of tubular and lobular components
- Usually well differentiated (grade 1); can be moderately differentiated
- Nuclear score can be grade 1 - 2
- May have associated ductal carcinoma in situ (DCIS) or lobular carcinoma in situ (LCIS)
- Lacks surrounding myoepithelial cell layer
- References: Mod Pathol 2007;20:130, Am J Surg Pathol 2004;28:1587, Breast Care (Basel) 2008;3:423
Microscopic (histologic) images
Contributed by S. Emily Bachert, M.D. and AFIP
Haphazard arrangement
Infiltrative pattern
Tubular and lobular components
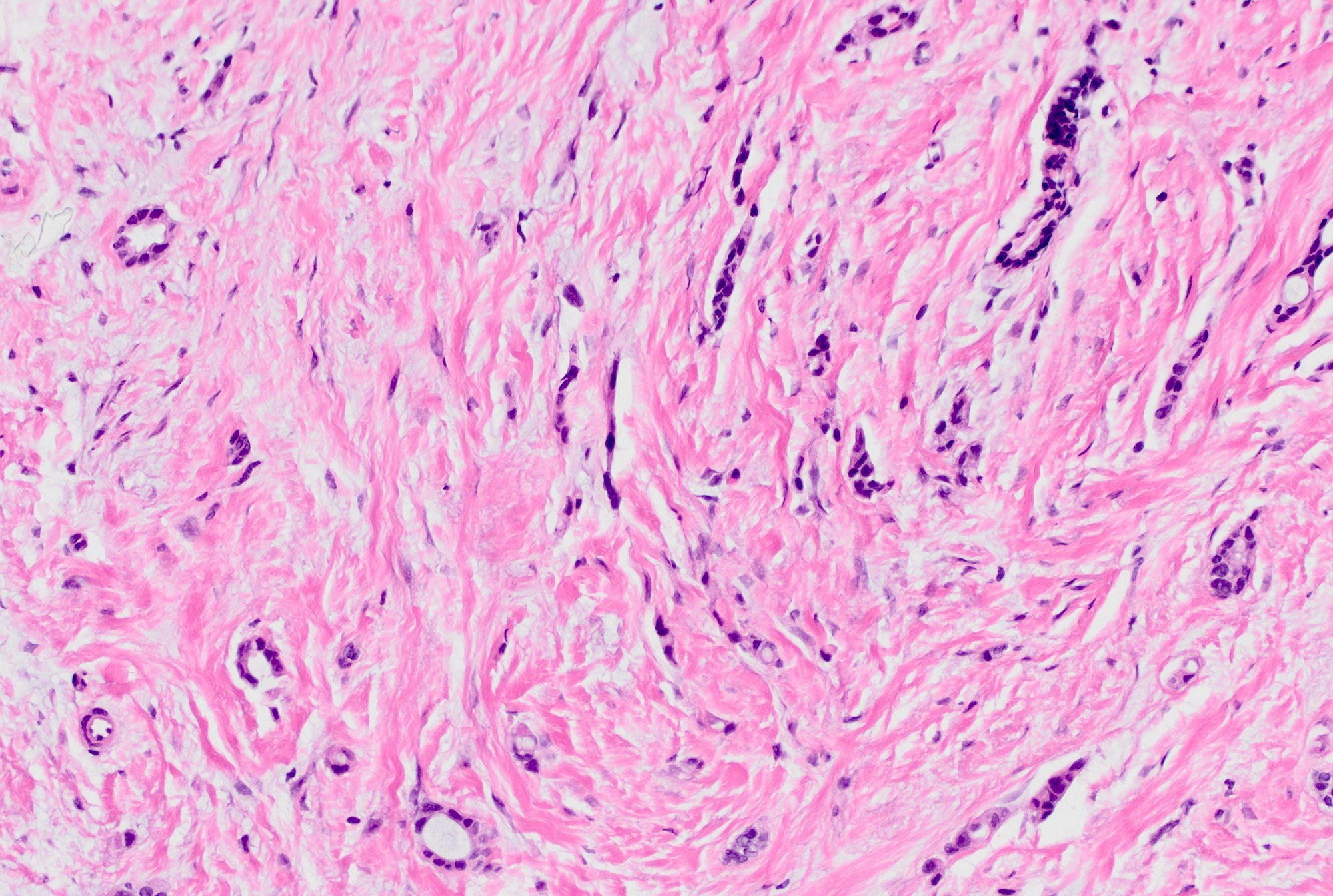
Fibrous stroma
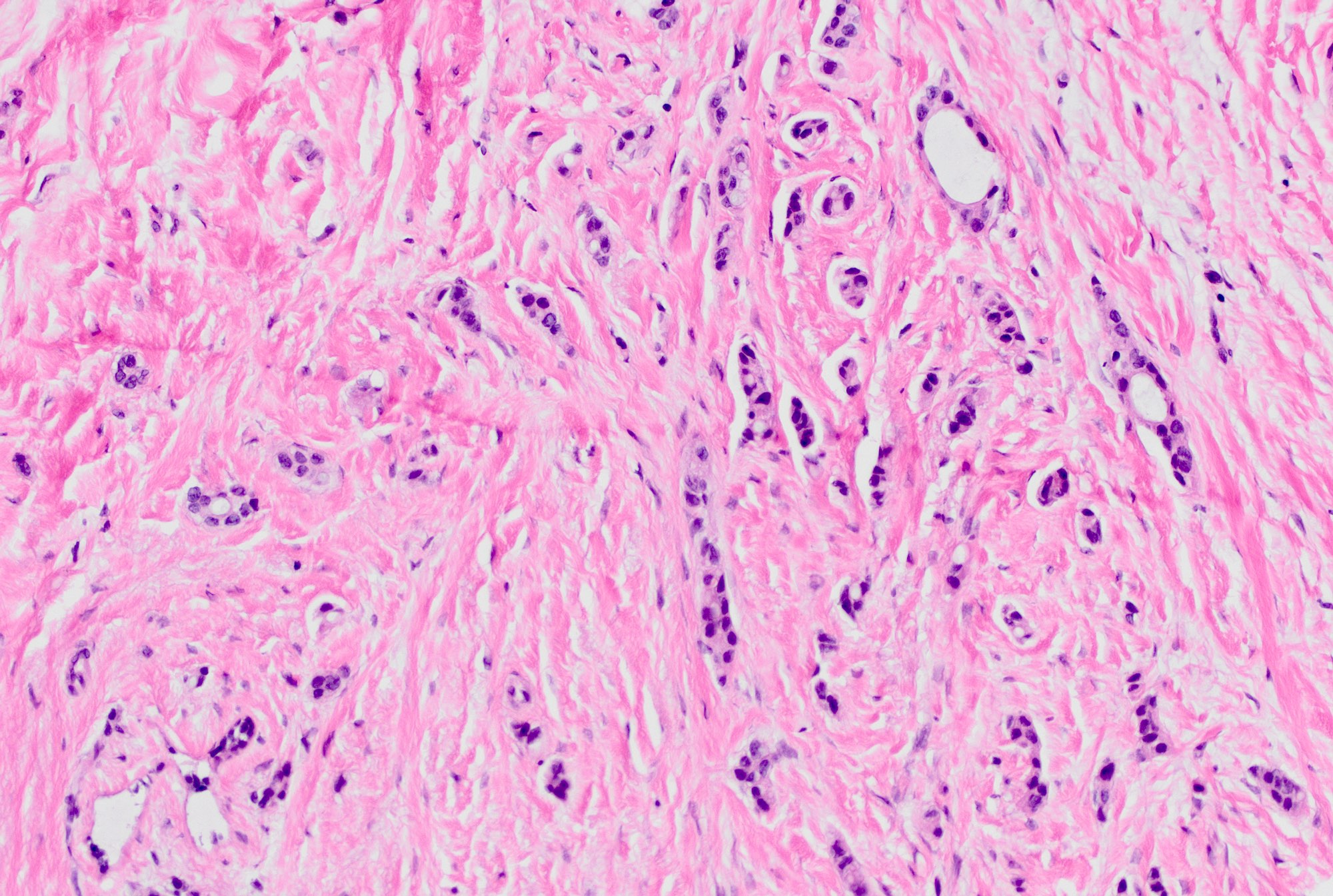
Predominantly lobular component
Infiltrative tubules

Single file cells
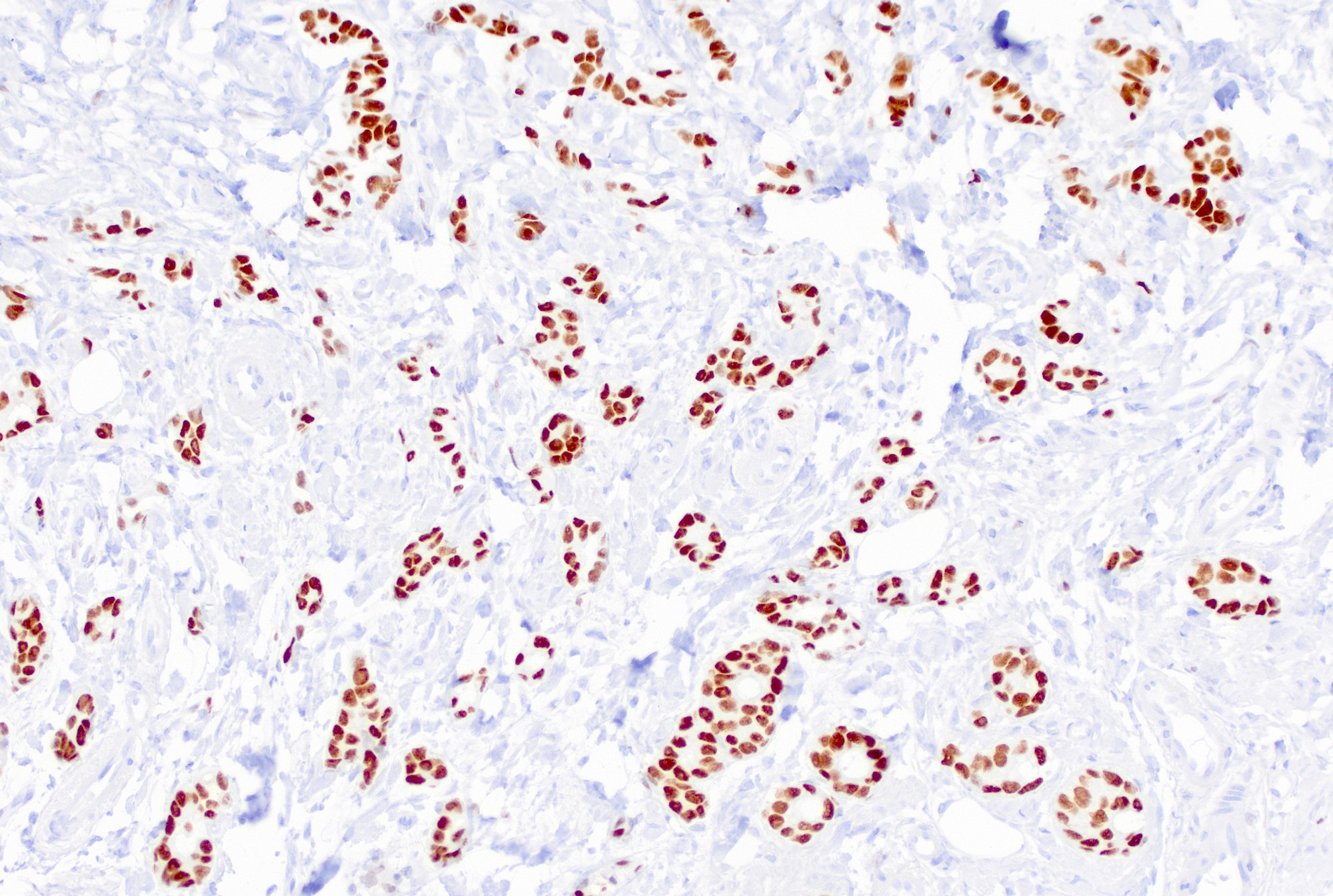
ER+
Cytology description
- Diagnosis can be suggested but not definitively made on cytologic preparations
- Single filing of cells and tubular structure formation
- Low nuclear grade
- Low mitotic rate
- Intracytoplasmic vacuoles and rare nucleoli (Acta Cytol 1996;40:465)
Positive stains
- Almost all are ER+ and PR+
- E-cadherin (75 - 100%), high molecular weight keratin 34 beta E12 (93%) and catenins (alpha, beta or gamma membranous staining in 100%), p120 (100%)
- GATA3, mammaglobin, GCDFP-15
- References: Mod Pathol 2007;20:130, Am J Surg Pathol 2004;28:1587
Negative stains
- SMMHC, p63, calponin (myoepithelial markers)
- S100
- HER2
- References: Mod Pathol 2007;20:130, Am J Surg Pathol 2004;28:1587
Sample pathology report
- Right breast, excision:
- Tubulolobular carcinoma, well differentiated, measuring 1.5 cm
- Nottingham grade I / III: tubule score = 1, nuclear score = 1, mitoses score = 1
Differential diagnosis
- Mixed ductal and lobular carcinoma:
- Lacks small, round, well formed tubules
- Invasive lobular carcinoma:
- Linear files of dyscohesive cells without tubule formation
- E-cadherin negative
- Tubular carcinoma:
- Lacks lobular component
- Microglandular adenosis:
Additional references
Board review style question #1
Which of the following is true regarding the histologic subtype of the breast carcinoma shown above?
- The tumor will most likely be ER negative and HER2 positive
- The tumor will most likely be ER positive and HER2 negative
- The tumor will most likely be negative for E-cadherin
- The tumor will most likely be positive for SMMHC and p63
Board review style answer #1
B. The tumor will most likely be ER positive and HER2 negative. The picture depicts an invasive carcinoma with small round tubules and single filing of cells, compatible with a tubulolobular carcinoma of the breast. Answer A is incorrect because the vast majority of these tumors are ER positive and HER2 negative. Answer C is incorrect because E-cadherin is usually positive in these tumors as they have tubule formation. Answer D is incorrect because these tumors will be negative for myoepithelial markers, compatible with invasive carcinomas.
Comment Here
Reference: Tubulolobular carcinoma
Comment Here
Reference: Tubulolobular carcinoma
