
Breast
Other invasive carcinoma subtypes, WHO classified
Tubular
Editorial Board Member: Kristen E. Muller, D.O.
Deputy Editor-in-Chief: Gary Tozbikian, M.D.


Last author update: 23 March 2023
Last staff update: 23 December 2024
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Tubular carcinoma breast


Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Virtual slides | Cytology description | Positive stains | Negative stains | Electron microscopy description | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Jain PV, Jorns JM. Tubular. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/breastmalignanttubular.html. Accessed April 2nd, 2025.
Definition / general
- Special subtype of invasive breast carcinoma with favorable prognosis
- Composed of distinct, well differentiated angular tubular structures (> 90%) with open lumina, lined by a single layer of low grade malignant epithelial cells, with a fibrous / desmoplastic stromal response
Essential features
- > 90% of the tumor is composed of ovoid or angular tubules with open lumina lined by a single layer of epithelial cells with low grade nuclei and sparse mitoses (grade 1)
- ER positive and HER2 negative
Terminology
- Tubular carcinoma
- Invasive tubular carcinoma
ICD coding
Epidemiology
- 1.6% of invasive breast carcinomas
- Postmenopausal women, median age at presentation is 63 years
- Slightly higher incidence in white women than black women in the U.S.
Sites
- Breast, with no specific site of predilection
Pathophysiology
- Luminal A molecular subtype of breast cancer
- Hypothesis: may arise due to a sequence of events starting with flat epithelial atypia
- Co-occurrence of columnar cell lesions, atypical ductal hyperplasia / ductal carcinoma in situ and pure form of tubular carcinoma with the same cytologic nuclear morphology has been observed (J Urol 1992;147:322)
- Rosen triad: tubular carcinoma, lobular carcinoma in situ, columnar cell lesions (Adv Anat Pathol 2008;15:140)
Etiology
- No specific etiology: see etiologies associated with low grade, ER positive invasive breast cancer of no special type (NST)
Clinical features
- Can be multifocal / multicentric (20 - 55%) (Am J Surg Pathol 1997;21:653)
- May have family history of breast carcinoma (40%)
- Usually presents as early stage, pT1 and pN0 disease (Int J Radiat Oncol Biol Phys 2009;75:1304)
Diagnosis
- Histologic examination of tissue
Radiology description
- Mammography: may present as a discrete or ill defined mass with well demarcated or spiculated, irregular margins, respectively or as an architectural distortion, with variable calcifications (Radiol Med 2006;111:773)
- Ultrasonography: hypoechoic mass with poorly defined margins and posterior acoustic shadowing (Tumori 2003;89:417)
- MRI: enhancing mass, enhancing focus or non mass enhancement (Egyptian J Radiol Nuc Med 2018;49:281)
Radiology images
Contributed by Julie M. Jorns, M.D.
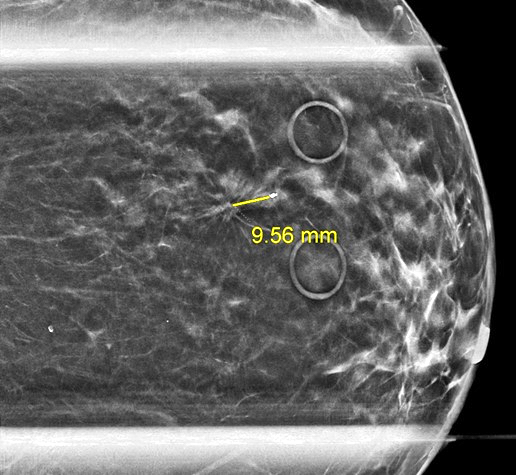
Diagnostic mammogram
Prognostic factors
- Well differentiated variant with very favorable prognosis (low rates of recurrence and metastasis) (Am J Surg 2009;197:674)
- Longer disease free and breast cancer specific survival with tubular carcinoma (n = 102) as compared to grade 1 invasive ductal carcinoma of no special type (n = 212) (J Clin Oncol 2010;28:99)
- Higher disease free survival was seen with pure tubular histology as well as if 3 criteria were met (≥ 70% tubules, pure grade 1 nuclei and no / rare mitoses) in a cohort of grade 1 - 2 tubular (n = 32) and invasive ductal (n = 115) carcinomas (Am J Clin Pathol 2004;122:728)
- Mixed with invasive ductal carcinoma of no special type has a worse prognosis (Hum Pathol 1983;14:694)
- Cause specific survival of 97% at 10 years (Eur J Surg Oncol 2005;31:9)
- 10 - 27% have axillary metastases, often micrometastases but still have excellent prognosis (Eur J Surg Oncol 2006;32:488, Breast J 2003;9:298)
Case reports
- 39 and 74 year old women who presented with tubular carcinoma in retroareolar and deep parasternal locations, respectively (Medicine (Baltimore) 2021;100:e24977)
- 46 year old woman with tubular carcinoma presenting as non mass enhancement (Egyptian J Radiol Nuc Med 2018;49:281)
- 63 year old woman with tubular carcinoma that spontaneously shrank from 9 mm to 4 mm on breast imaging during the 6 year interval from first identification to diagnostic biopsy (Radiol Case Rep 2015;1:68)
Treatment
- Surgery, either breast conserving surgery (lumpectomy) or mastectomy, with or without radiation therapy depending on surgery and clinical features (Breast Cancer Res Treat 2005;93:199, Breast J 2005;11:129)
- Axillary lymph node staging, including sentinel lymph node excision, may be safely omitted (Eur J Surg Oncol 2013;39:248, Ann Surg Oncol 2023;30:1042)
- May be offered anti-endocrine therapies
- Adjuvant chemotherapy is contraindicated
Gross description
- Spiculated tumor with a firm consistency; may have gritty texture if there are calcifications
- Mean size is 1.2 cm
- White, tan or gray in color
Gross images
Images hosted on other servers:

Yellow-white sclerotic mass
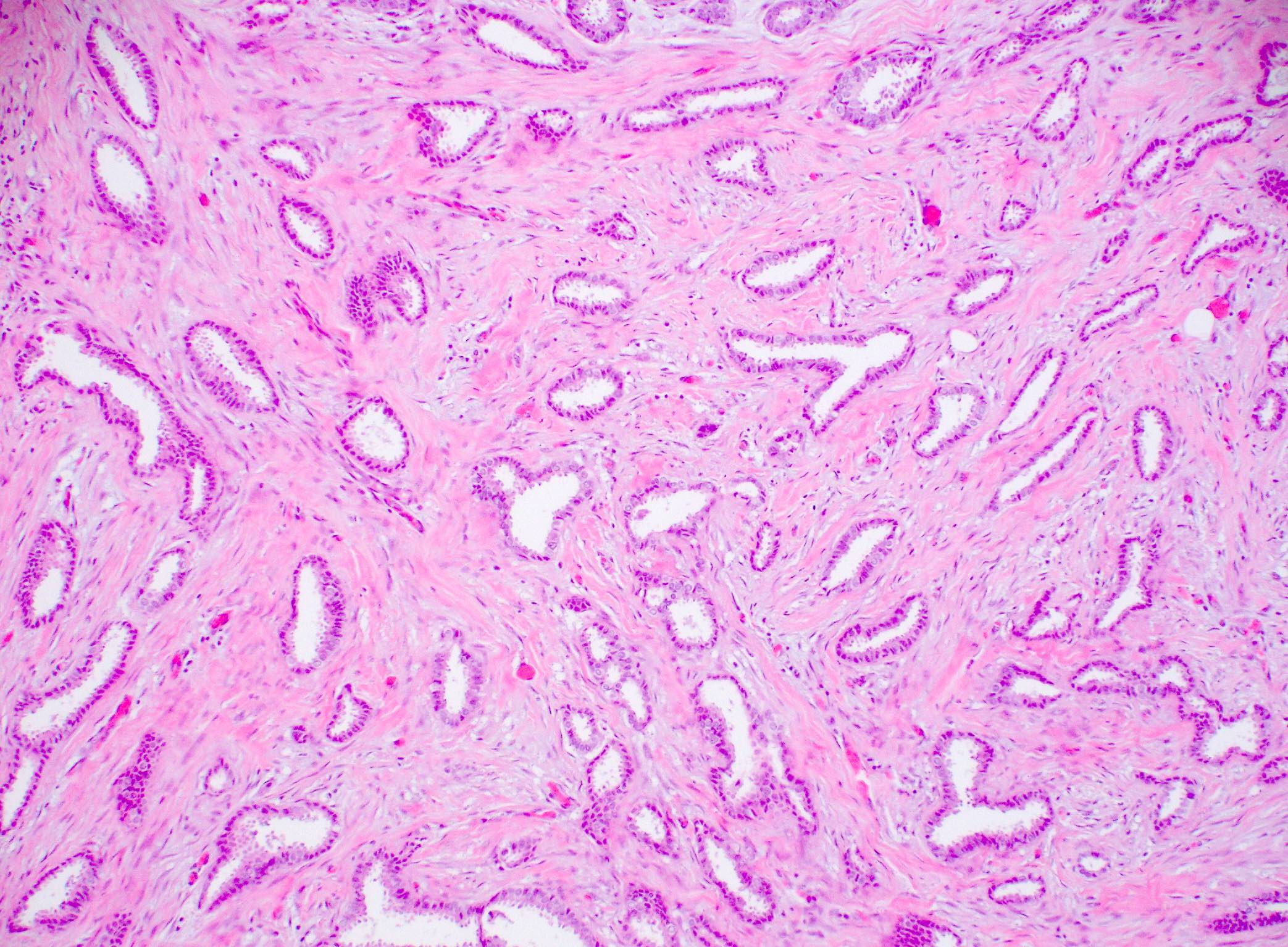
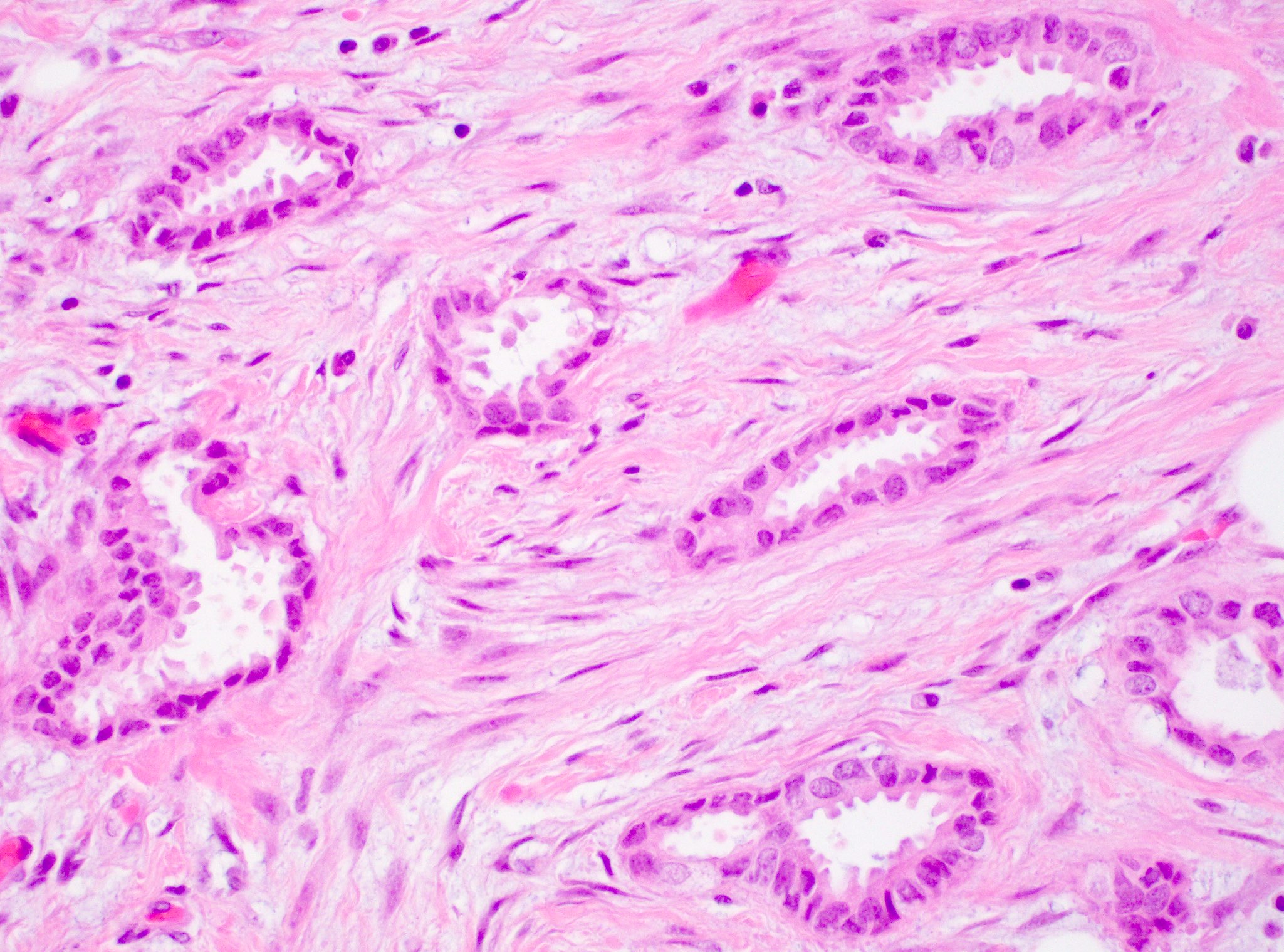
Microscopic (histologic) description
- Invasive breast cancer with infiltrative growth pattern, often with invasion into adipose tissue and with an associated fibrous or desmoplastic stromal response
- No myoepithelium surrounding the tubules
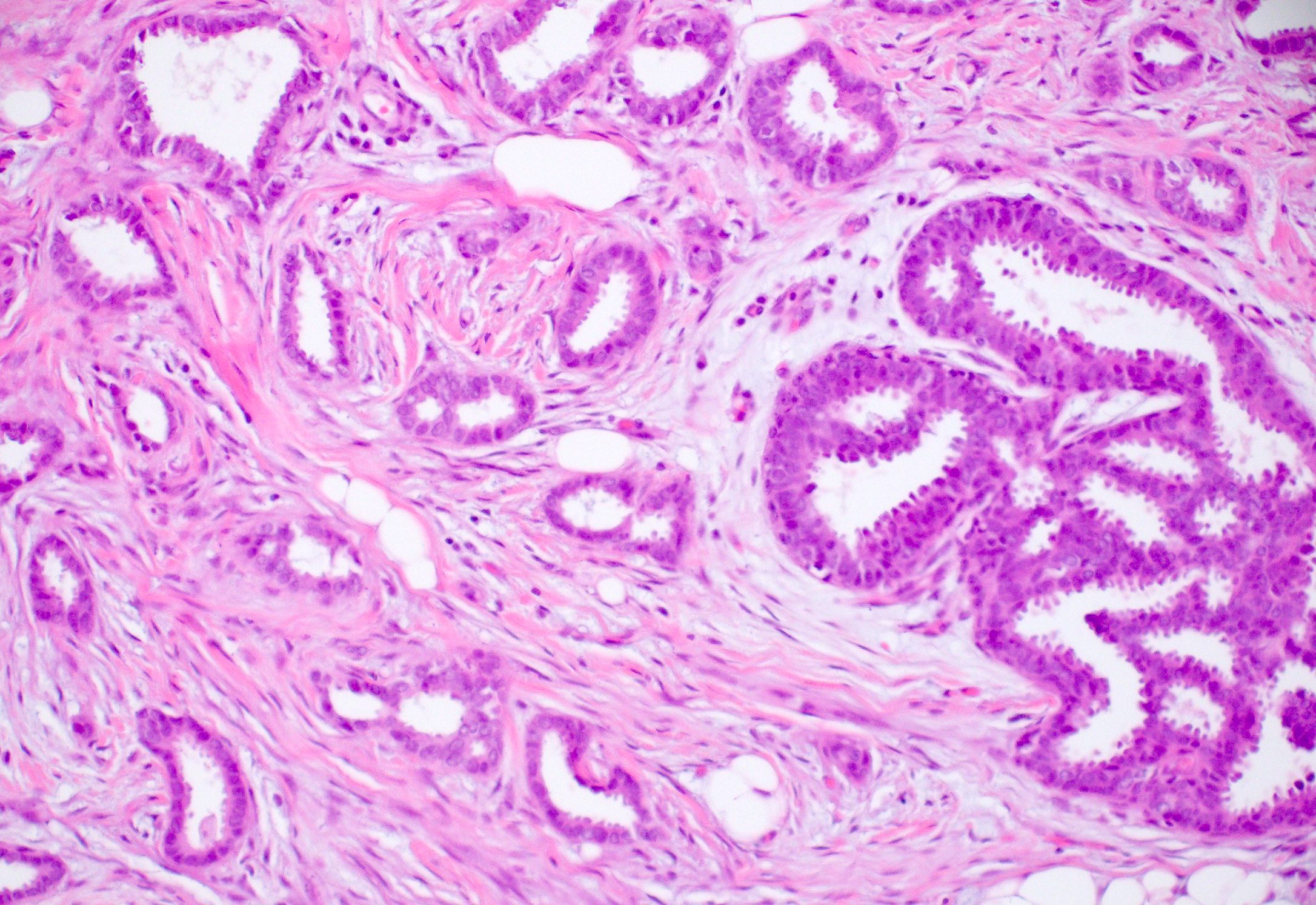
- > 90% of the tumor is composed of small, ovoid or angulated tubules with open lumina
- Tubules are lined by a single layer of epithelial cells with low grade nuclei and sparse mitoses (grade 1)
- Tumor cells often have apical cytoplasmic tufting or snouts
- Cells lining the neoplastic tubules are cuboidal to columnar with uniform, small to intermediate sized nuclei
- No significant cytologic atypia, multilayering or high mitotic activity (the presence of these would rule out tubular carcinoma)
- There may be luminal secretions or calcifications
- Tumor cells are ER positive and HER2 negative
- Recent study shows that the actual structure is not tubular, instead it simulates a beaded necklace
- 2 dimensional microscopy and 3 dimensional modeling studies revealed that structure resembled a necklace formed by a string of beads with the tubules visualized as blebs bridged together by solid cords of cells; continuous or branching tubules were not seen (Histopathology 2006;48:556)
- Desmoplastic or fibroelastotic stroma
- Frequent presence of associated nonobligate precursors:
- Columnar cell lesions (95%), in particular flat epithelial atypia (Am J Surg Pathol 2007;31:417, Pathol Int 2008;58:620)
- Atypical ductal hyperplasia
- ER positive low grade DCIS
- Rosen triad: tubular carcinoma, lobular carcinoma in situ, columnar cell lesions (Adv Anat Pathol 2008;15:140)
Microscopic (histologic) images
Contributed by Julie M. Jorns, M.D., Mark R. Wick, M.D. and AFIP
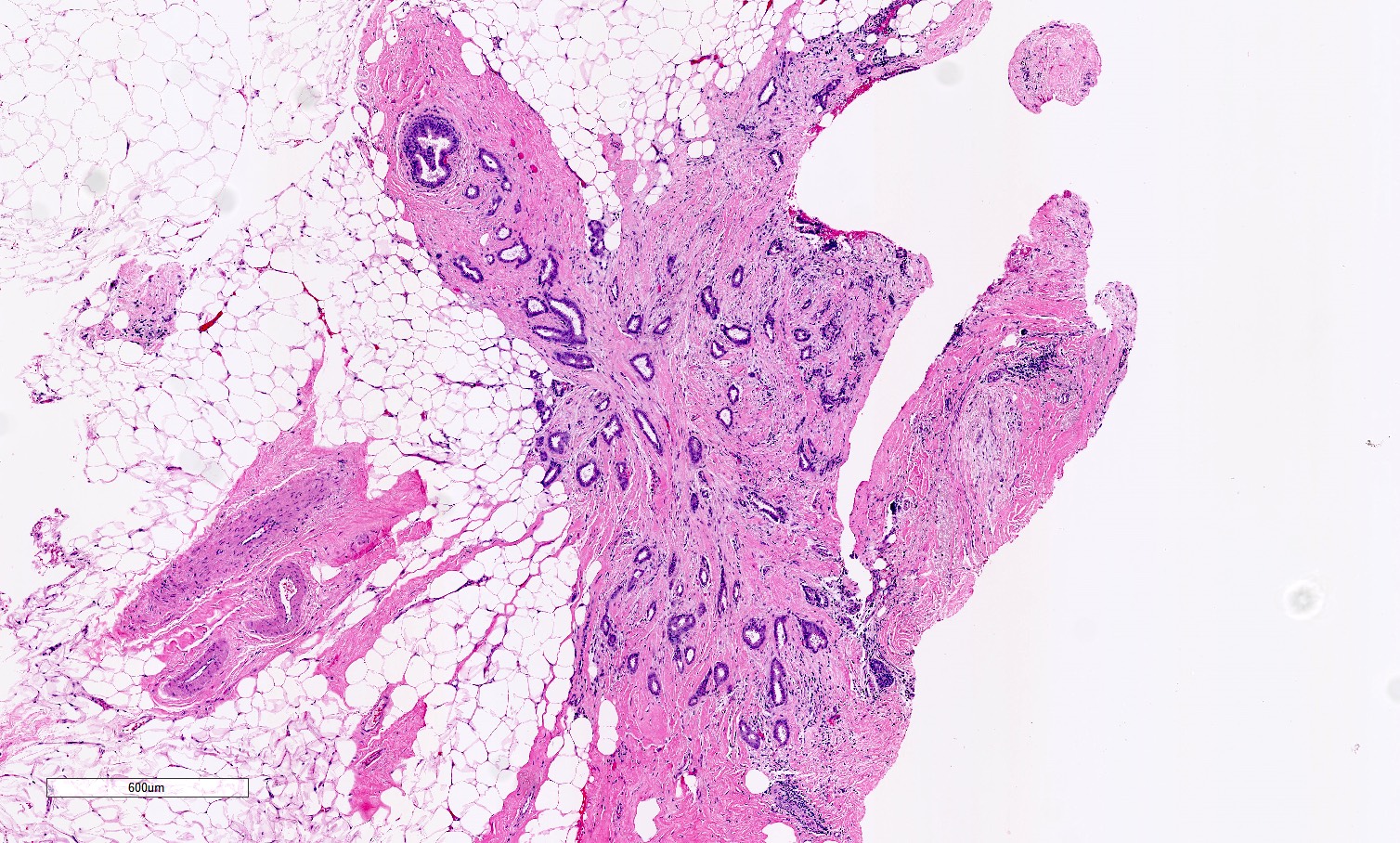
Infiltrative angulated tubules
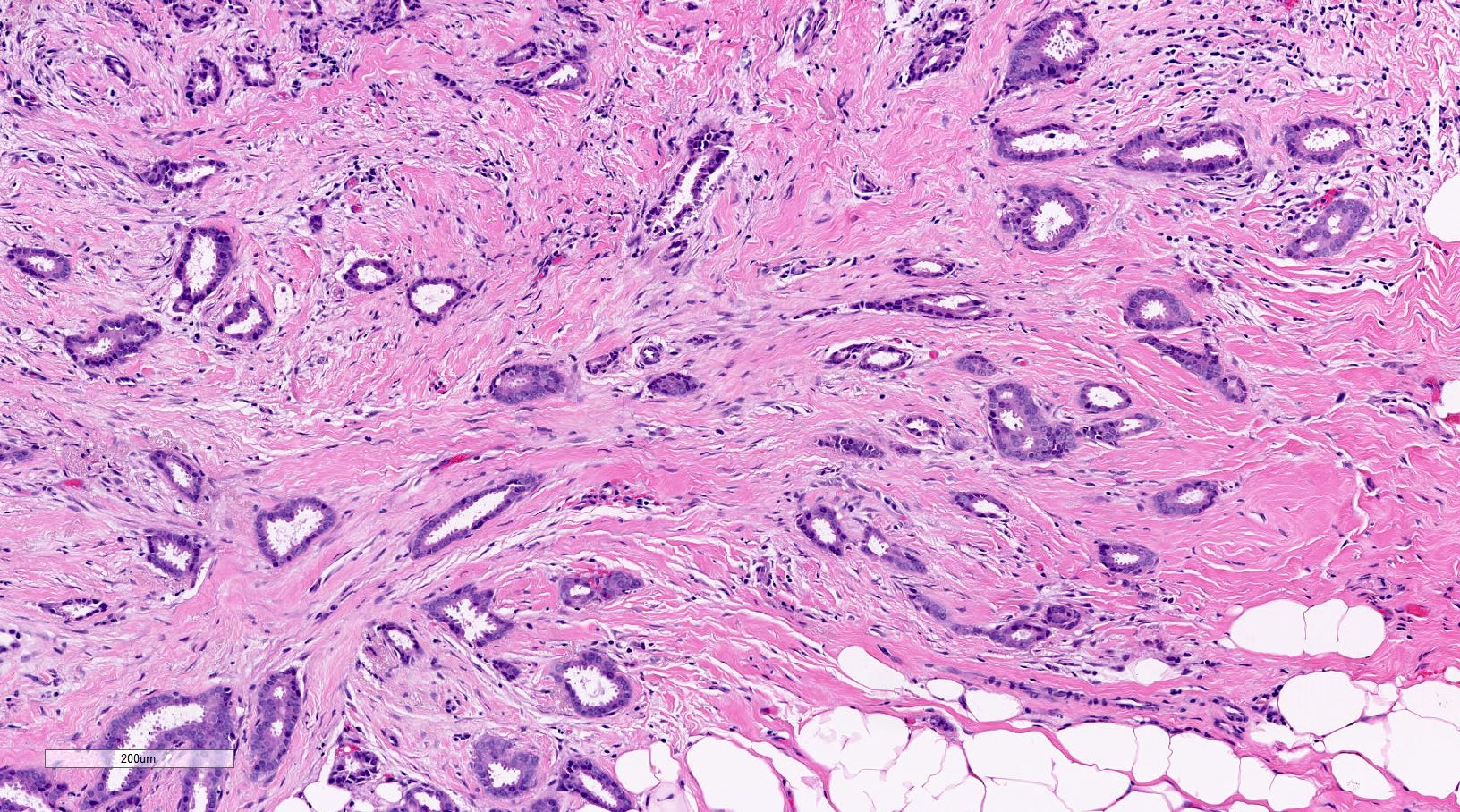
Angulated tubules
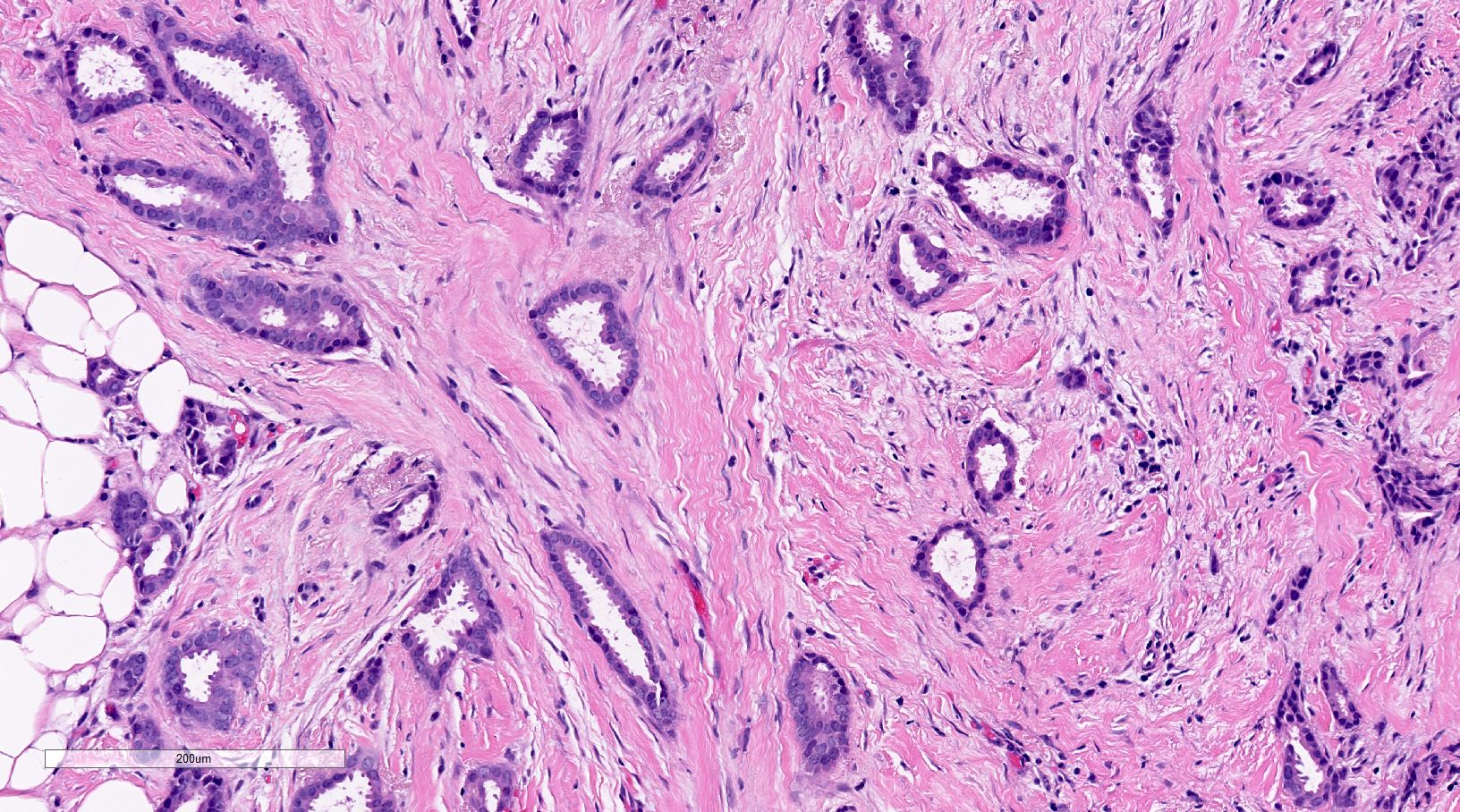
Apical tufting
Desmoplasia
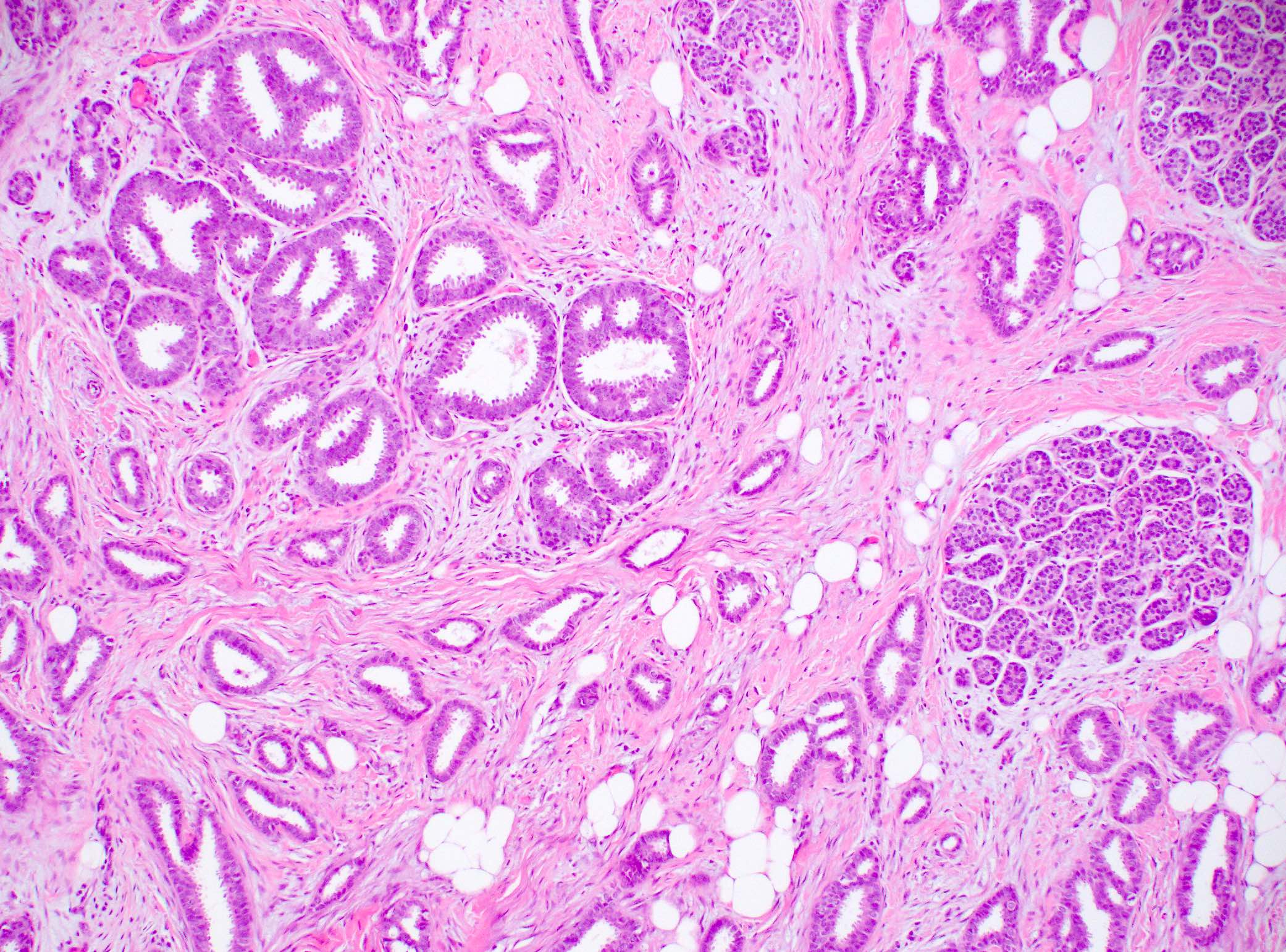
Associated ADH, FEA and ALH
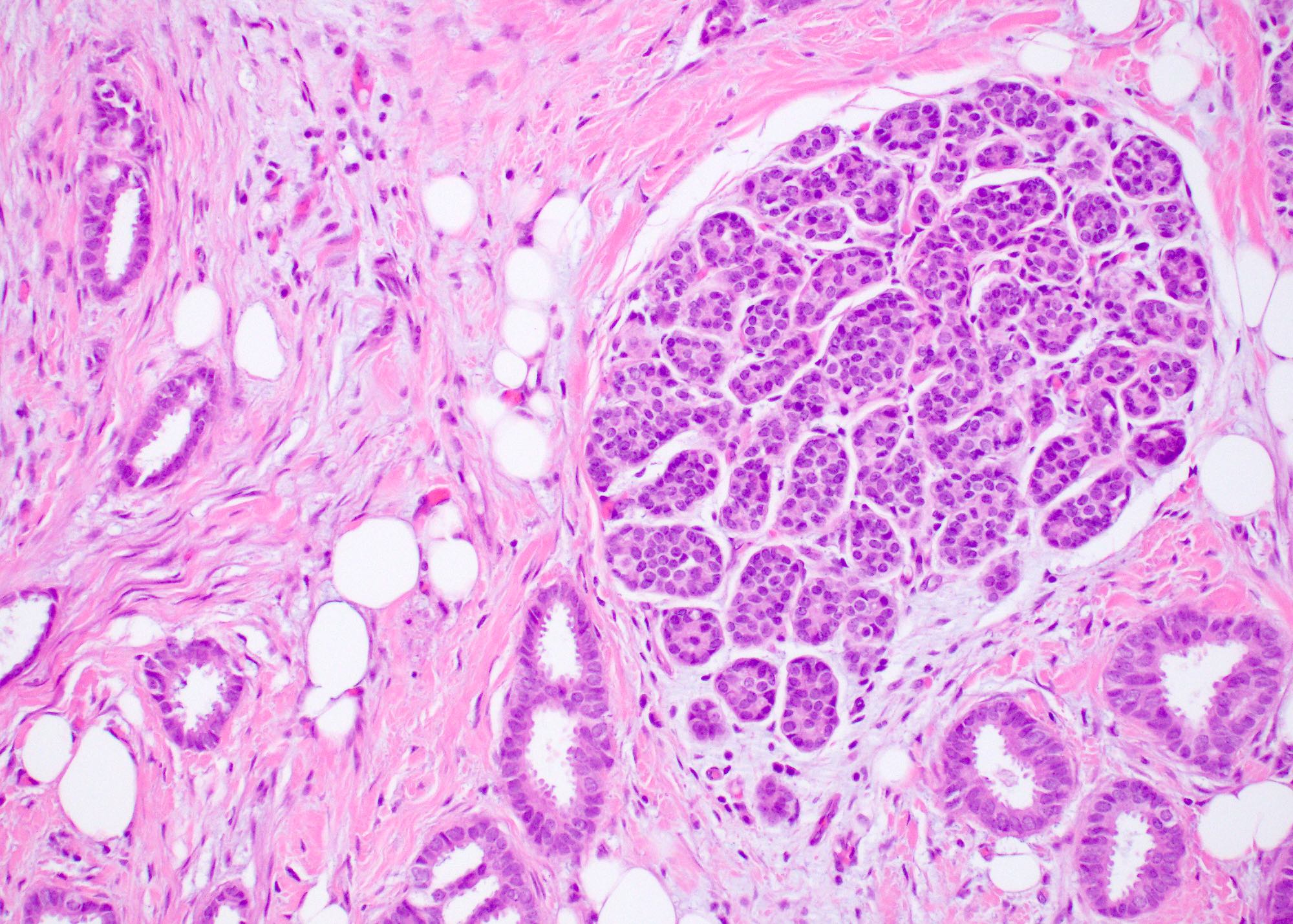
Associated atypical lobular hyperplasia
Associated atypical ductal hyperplasia / flat epithelial atypia
Apical tufting
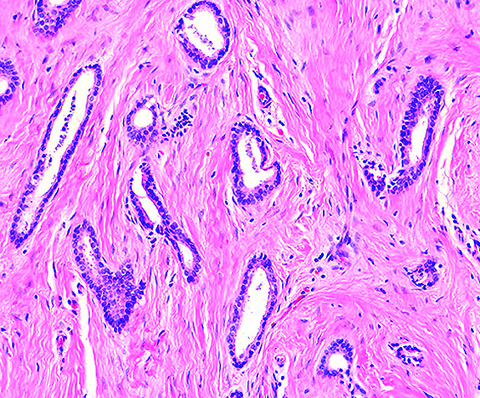
Open tubules
Angular glands with cytoplasmic snouts
Virtual slides
Images hosted on other servers:

Invasive tubular carcinoma
Cytology description
- Increased cellularity, somewhat angular or irregular or small tubular epithelial clusters and single epithelial cells
- Cells are bland and orderly with variable atypia and a variable number of prominent myoepithelial cells
- Features of malignancy such as nuclear atypia, absence of myoepithelial cells and cellular dissociation are subtle and hence diagnosis on cytology can be challenging (Acta Cytol 1997;41:1139, Am J Clin Pathol 1994;101:488)
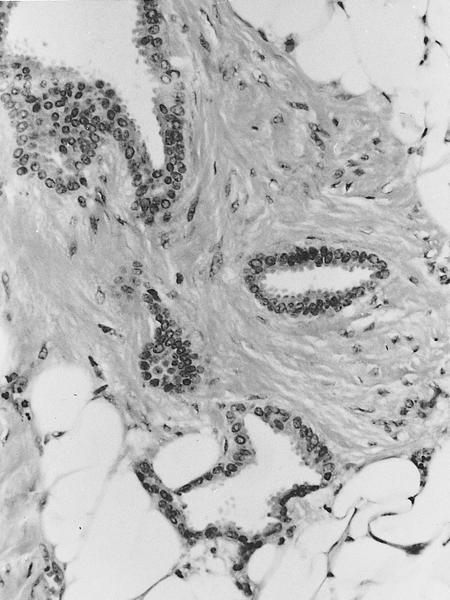
Positive stains
- ER, PR and E-cadherin
- CK8, CK 8/18 (luminal phenotype)
Negative stains
- HER2 (ERBB2), HER1 (EGFR), p53 (Am J Clin Pathol 2006;126:55)
- Myoepithelial markers (p63, CD10, smooth muscle actin, CK5/6)
- P-cadherin
- CK5 / CK14 (luminal phenotype)
Electron microscopy description
- Ductal differentiation, no myoepithelial cells and no basement membrane
Molecular / cytogenetics description
- ER positive pathway alterations
- Frequent alterations: loss of 16q (78 - 86%), gains of 1q (50 - 62%), both usually occur concurrently
- Infrequent alterations: 16p gain, loss of 8p, 3p (the FHIT gene locus) and 11q (the ATM gene locus)
- Fewer overall chromosomal changes than invasive ductal carcinoma of no special type (Hum Pathol 2001;32:222)
- Clonally related to flat epithelial atypia and low grade DCIS (Am J Surg Pathol 2009;33:1646)
Sample pathology report
- Right breast, ultrasound guided core biopsy:
- Invasive mammary carcinoma with tubular features, preliminary modified Bloom-Richardson grade 1 (1+2+1) (see comment)
- Estrogen receptor: (91 - 100%, strong) positive
- Progesterone receptor: (91 - 100%, strong) positive
- HER2 / neu: (1+) negative for overexpression
- Comment: The carcinoma in this biopsy has entirely tubular features. If there is similar morphology in > 90% of the tumor on resection it would be best classified as an invasive tubular carcinoma.
Differential diagnosis
- Sclerosing adenosis:
- Overall lobular architecture but with distortion by fibrosis, compression of glands with 2 layers (inner epithelial and outer myoepithelial)
- Positive for myoepithelial markers (Appl Immunohistochem Mol Morphol 2006;14:71)
- Radial scar:
- Desmoplastic / elastotic stroma, bland tubules
- Does not infiltrate at the periphery
- Often has intermixed fibrocystic changes such as cysts and usual ductal hyperplasia
- Retained myoepithelial cell layer
- Microglandular adenosis:
- More rounded (not angulated) tubules with intraluminal colloid-like secretory material (Am J Surg Pathol 1982;6:401)
- Lacks myoepithelium but basement membrane material is present
- ER negative and S100 positive
- Mixed tumors with a combination of tubular carcinoma and another subtype of cancer:
- Should be reported when the tumor mass shows 10 - 90% tubular carcinoma (common) or ≥ 90% is tubular carcinoma and remaining tumor shows nuclear grade 3 (rare)
- Tubulolobular carcinoma:
- Mixed tubular and lobular components
- Not an entity in WHO
- Thought to be a variant of tubular carcinoma as they share similar architectural and growth patterns (tubulolobular carcinoma also resembles a beaded necklace but with longer connecting strands of single cells)
- Both show E-cadherin positivity
- Both show indolent clinical behavior
- Low grade adenosquamous carcinoma:
- Squamous differentiation
- Less uniformity (open and compressed tubules, nests)
- Often ER negative
- Low grade invasive ductal carcinoma of no special type:
- Similar low grade cytologic features to tubular carcinoma, with or without prominent apical cytoplasmic tufting but with more complex architecture
- Tumor shows multilayering, stratification, glandular fusion or branching and may have > 10% ribbons or cords
- ER expression is often high but may be of lower intensity in tubular carcinoma (i.e., third quartile or > 50 - 75%, expression) than in well differentiated invasive ductal carcinoma (i.e., fourth quartile or > 75 - 100%, expression) (Arch Pathol Lab Med 2014;138:1507)
Additional references
Board review style question #1
A postmenopausal woman presented with a breast mass measuring 0.8 cm. Biopsy and resection showed the morphology seen in the image above in > 90% of the tumor. What is the expected immunoprofile?
- ER / PR positive, HER2 negative
- ER / PR positive, HER2 positive
- ER / PR negative, HER2 positive
- ER / PR negative, HER2 negative
Board review style answer #1
A. ER / PR positive, HER2 negative. The tumor consists of infiltrative small, angulated tubules with a single layer of low grade neoplastic epithelium with prominent apical tufting, features diagnostic of tubular carcinoma. Tubular carcinoma is a luminal A breast carcinoma and thus is ER / PR positive and HER2 negative.
Comment Here
Reference: Tubular carcinoma of breast
Comment Here
Reference: Tubular carcinoma of breast
Board review style question #2
A core biopsy of a breast mass shows an invasive carcinoma with tubular features. What are the essential criteria to diagnose this tumor as tubular carcinoma?
- > 90% tubules lined by highly pleomorphic epithelial cells and brisk mitosis
- > 90% tubules lined by low grade epithelial cells with sparse mitosis
- < 90% tubules lined by highly pleomorphic epithelial cells and brisk mitosis
- < 90% tubules lined by low grade epithelial cells with sparse mitosis
Board review style answer #2
B. > 90% tubules lined by low grade epithelial cells with sparse mitosis. The diagnosis of tubular carcinoma or any special subtype of invasive breast carcinoma, requires that > 90% of the tumor show the specific diagnostic features of the special subtype. Thus, in the case of tubular carcinoma, > 90% of the tumor must have small, angulated tubules lined by a single layer of low grade malignant epithelium and sparse to absent mitoses. Because the patient underwent core biopsy, which is only a sampling of the tumor, the designation as tubular carcinoma should be reserved until the tumor is fully evaluated on subsequent resection. In such cases, a note or comment can be helpful (please see Sample pathology report for an example).
Comment Here
Reference: Tubular carcinoma of breast
Comment Here
Reference: Tubular carcinoma of breast
