
Breast
Other invasive carcinoma subtypes, WHO classified
Acinic cell carcinoma


Copyright: 2001-2024, PathologyOutlines.com, Inc.
PubMed search: Acinic cell carcinoma


- Acinic cell carcinoma is a malignant epithelial neoplasm characterized by clear and granular cells that may contain zymogen granules in the cytoplasm and shows microglandular and solid growth patterns
- Granular eosinophilic and basophilic cytoplasm with intracytoplasmic granules that are positive for periodic acid-Schiff with diastase (PASD)
- Infiltrative microglandular and solid growth patterns
- Positive immunohistochemical staining for EMA and markers of serous acinar differentiation
- Acinar cell carcinoma
- Rare carcinoma of the breast affecting females (20 - 80 years old); 1 case has been reported in a male, 68 cases reported in the literature (2022) (Breast Cancer 1998;5:77, Breast 2022;66:208)
- Breast, with no site predilection (Pathology 2017;49:215)
- Breast glands may show acinic differentiation that could possibly give rise to acinic cell carcinoma (Histopathology 2009;54:262)
- Acinic cell carcinoma shows similar mutations and DNA copy numbers to conventional triple negative breast carcinomas or those associated with microglandular adenosis (J Pathol 2015;237:166, Mod Pathol 2017;30:69)
- Morphologic and genetic relationship with microglandular adenosis has been reported and discussed (Mod Pathol 2017;30:1504, Mod Pathol 2017;30:1505)
- Breast acinic cell carcinomas have different mutation profiles from salivary gland acinic cell carcinomas, suggesting the entities are unrelated (Histopathology 2015;67:529)
- Unknown
- Presentation is similar to invasive breast carcinoma of no special type, palpable mass (Pathology 2017;49:215)
- Histologic and immunohistochemical examination of lesional tissue (Pathology 2017;49:215)
- Poorly defined lump / mass with microcalcifications, although may vary in clinical and radiological appearance (Breast 2022;66:208)
Contributed by Miralem Mrkonjic, M.D., Ph.D.
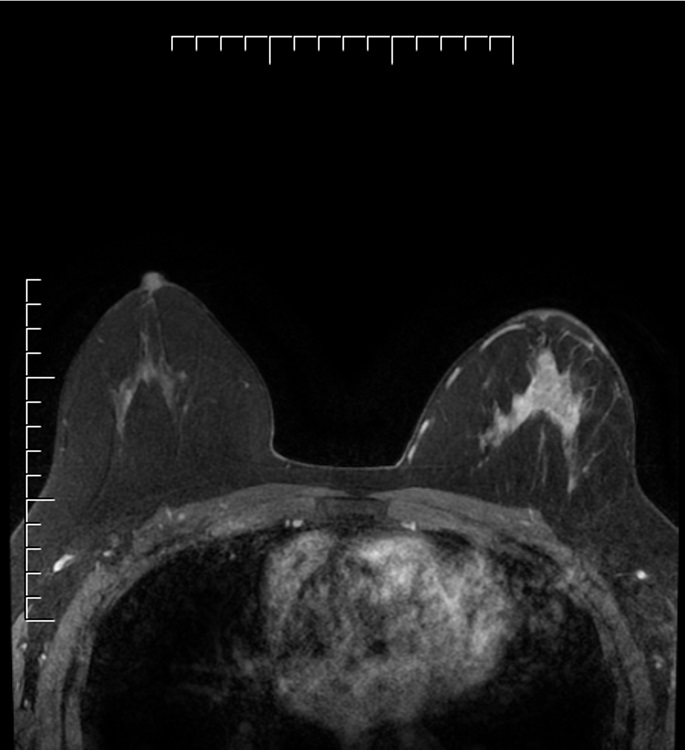
Left breast mass with nonmass enhancement
Images hosted on other servers:

Doppler ultrasound, molybdenum target

MRI and PET / CT
- Knowledge about prognosis is limited, thought to be a triple negative tumor with intermediate aggressive potential
- Molecular evidence suggests that it could be the precursor of more aggressive forms of triple negative breast carcinoma (J Pathol 2015;237:166)
- Axillary lymph node metastases are rare, reported in 11 of 68 reports (Breast 2022;66:208)
- Potential for distant metastases to liver, bone and lung (Histopathology 2004;45:645, J Clin Pathol 2002;55:545, Ann Diagn Pathol 2011;15:84)
- Peritoneal metastases have also been reported (Mol Clin Oncol 2022;16:43)
- 26 year old woman diagnosed with acinic cell carcinoma of the breast within a fibroadenoma (Int J Surg 2014;12:S232)
- 41 year old woman with palpable right breast lump (Ann Med Surg (Lond) 2018;35:137)
- 44 year old woman diagnosed with acinic cell carcinoma of the breast and carrying a BRCA1 mutation (BMC Cancer 2013;13:46)
- 52 year old woman with palpable lump in the outer quadrant of her right breast (Medicine (Baltimore) 2017;96:e8866)
- 59 year old woman with a lump in her right breast (Mol Clin Oncol 2022;16:43)
- Breast conserving surgery or mastectomy, generally with sentinel lymph node excision or axillary lymph node dissection; with or without neoadjuvant or adjuvant chemotherapy and radiotherapy, hormonal therapy (if ER positive) (Breast 2022;66:208)
- Poorly defined, gray-brown, rubbery, slightly lobulated appearance (J Breast Cancer 2011;14:160)
Images hosted on other servers:

Ill defined, slightly lobulated mass

Gray-brown rubbery tumor
- Cells with serous differentiation containing zymogen granules in the cytoplasm that stain with PASD
- Predominantly solid or microglandular growth but may be cystic, trabecular or show other growth patterns (Breast 2022;66:208)
Contributed by Miralem Mrkonjic, M.D., Ph.D.
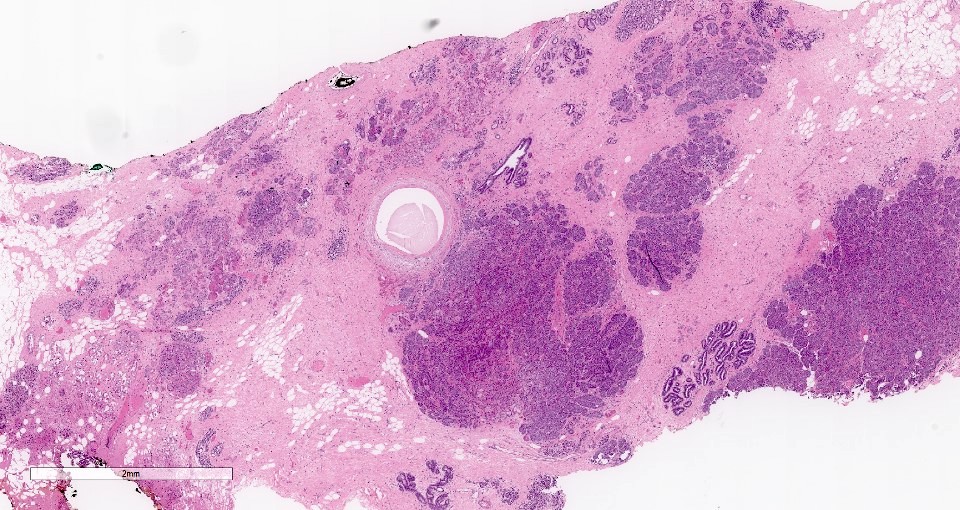
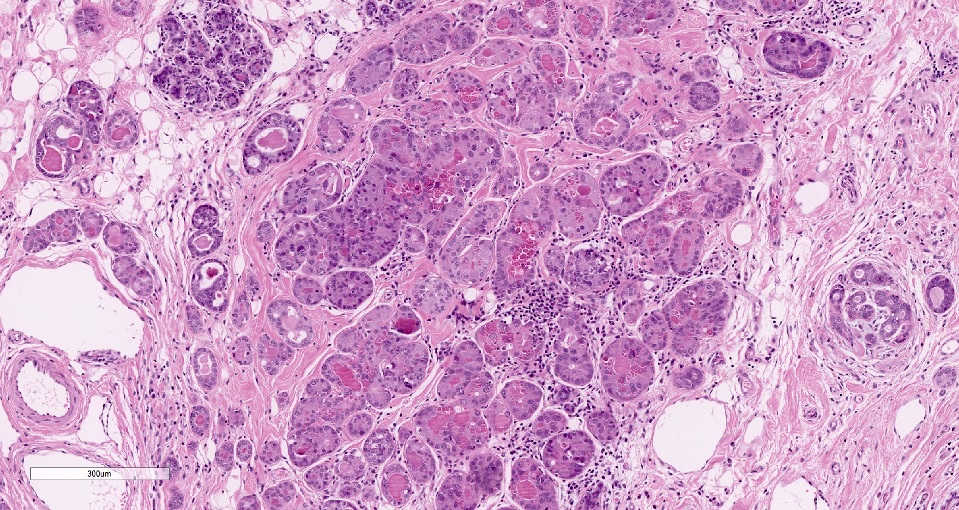
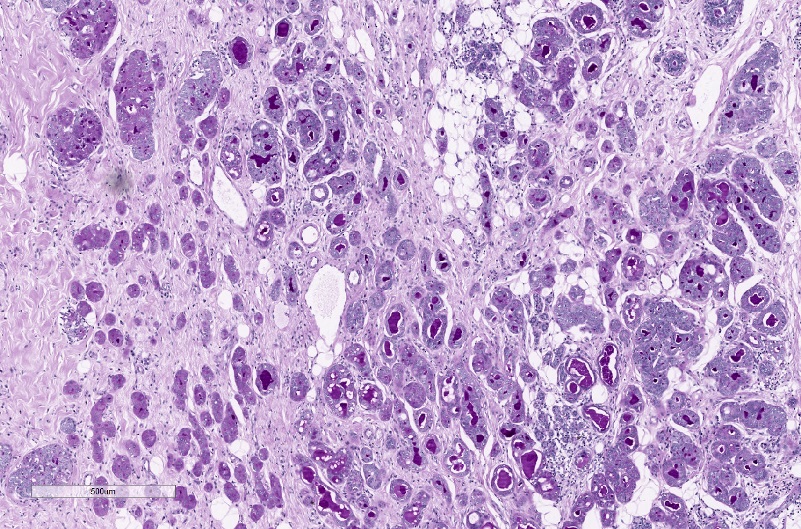
Infiltrative growth pattern
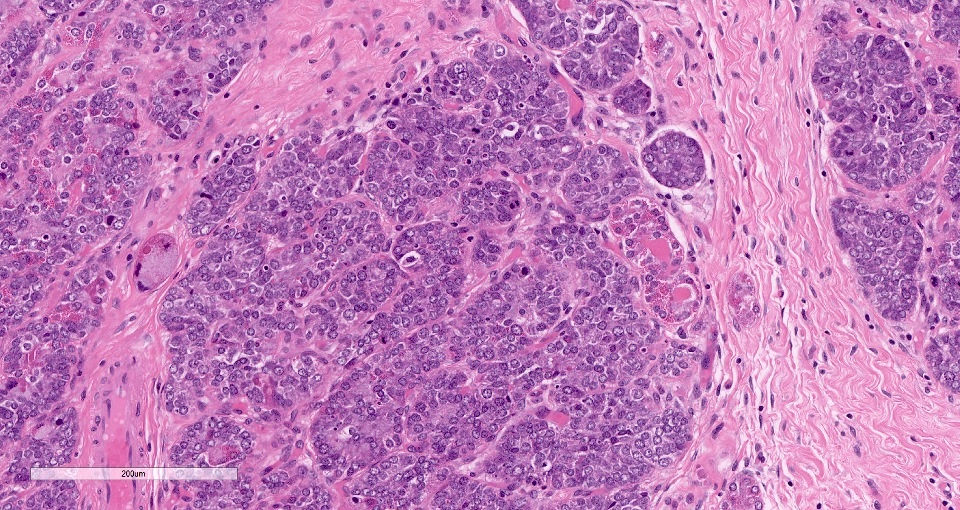
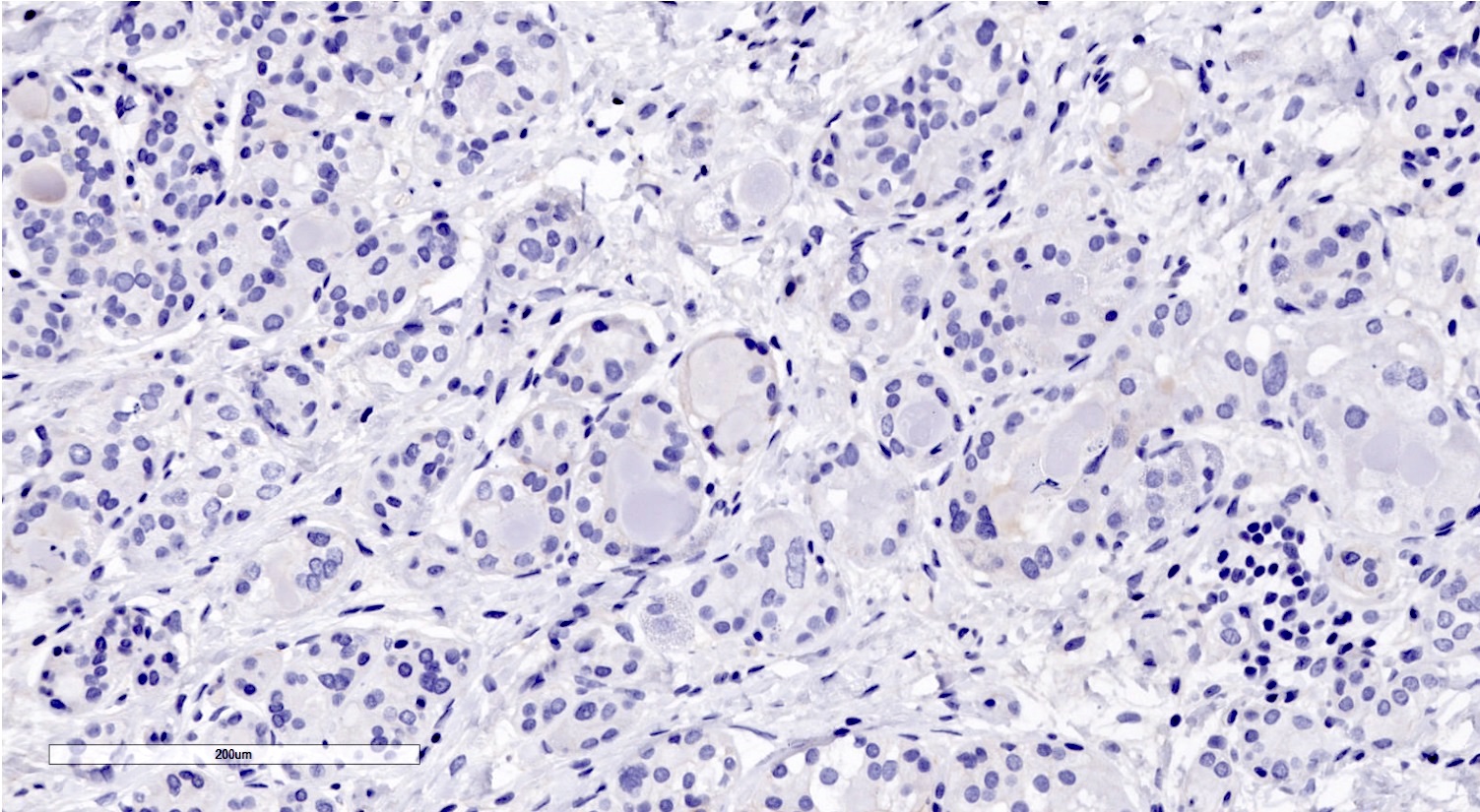
Microglandular architecture

Microglandular architecture and eosinophilic cytoplasm
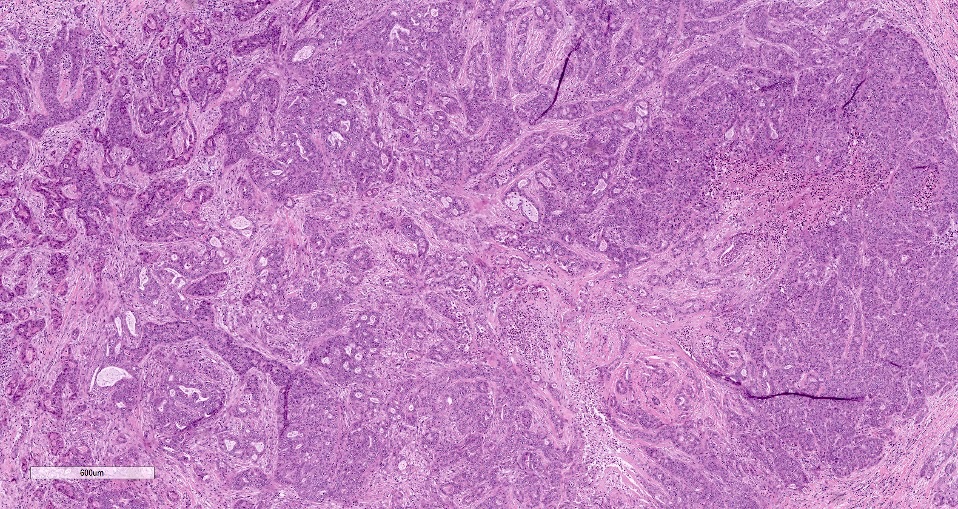
Areas resembling
invasive ductal
carcinoma of no
special type
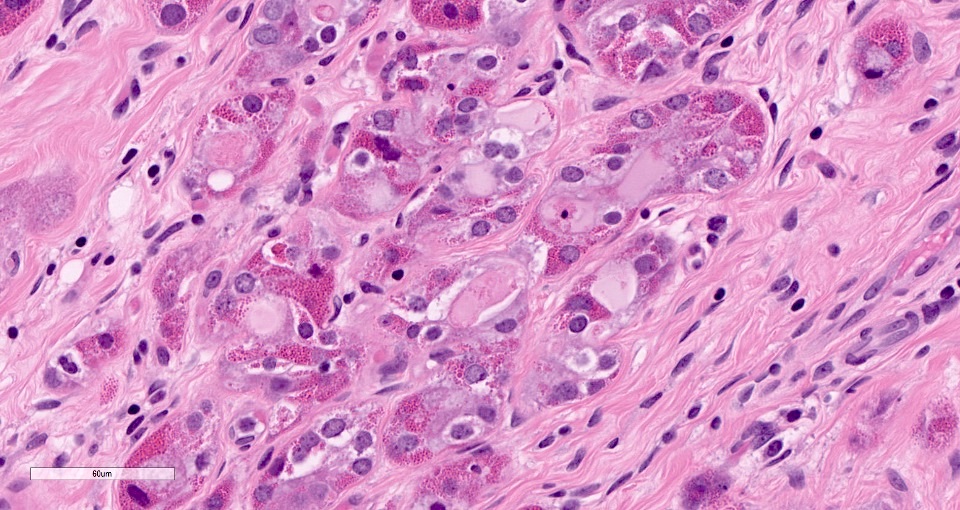
Prominent cytoplasmic eosinophilic granules
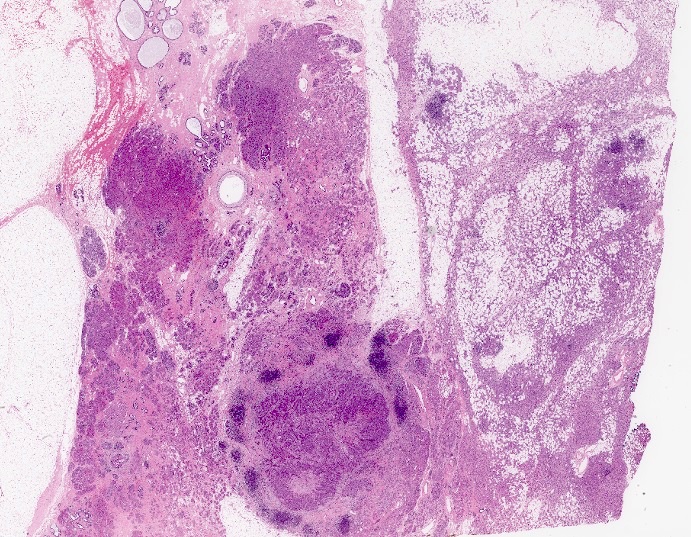
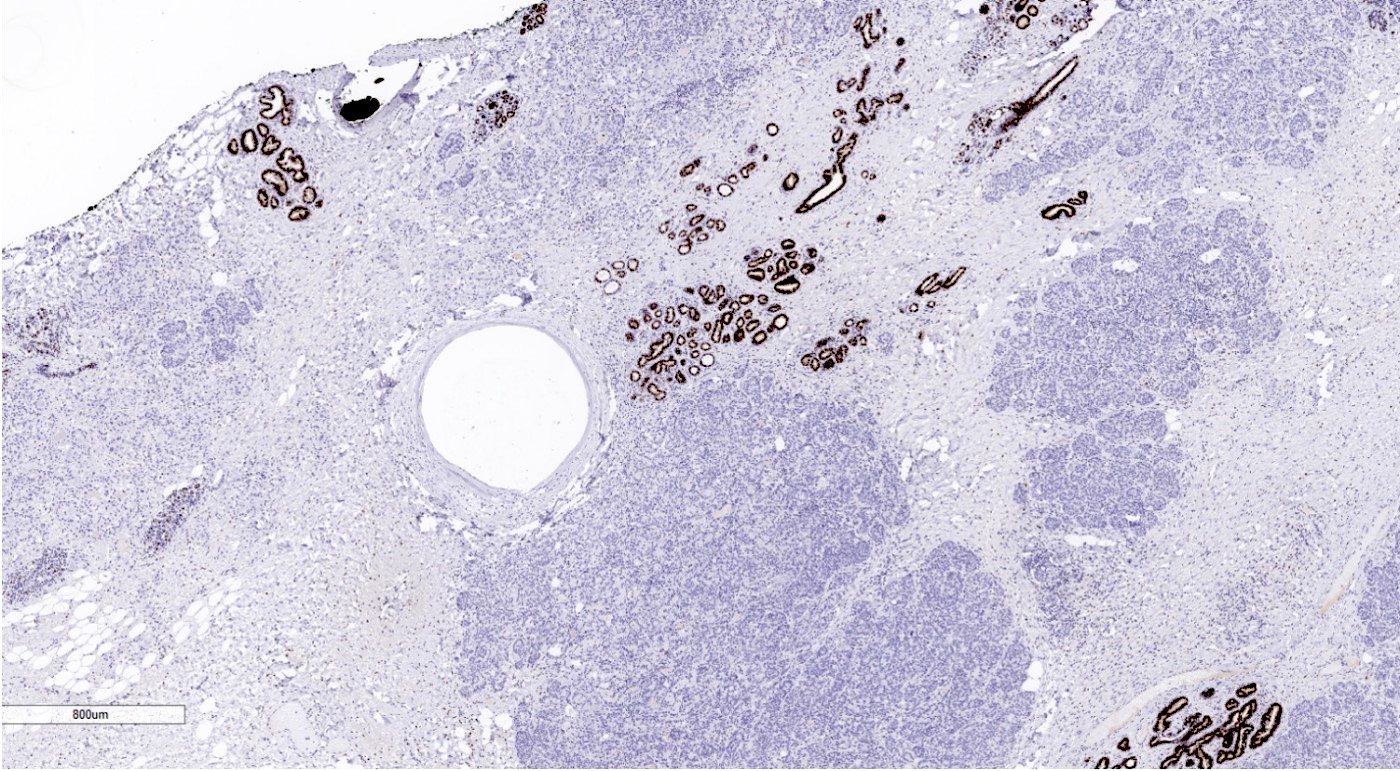
Background of extensive MGA and AMGA
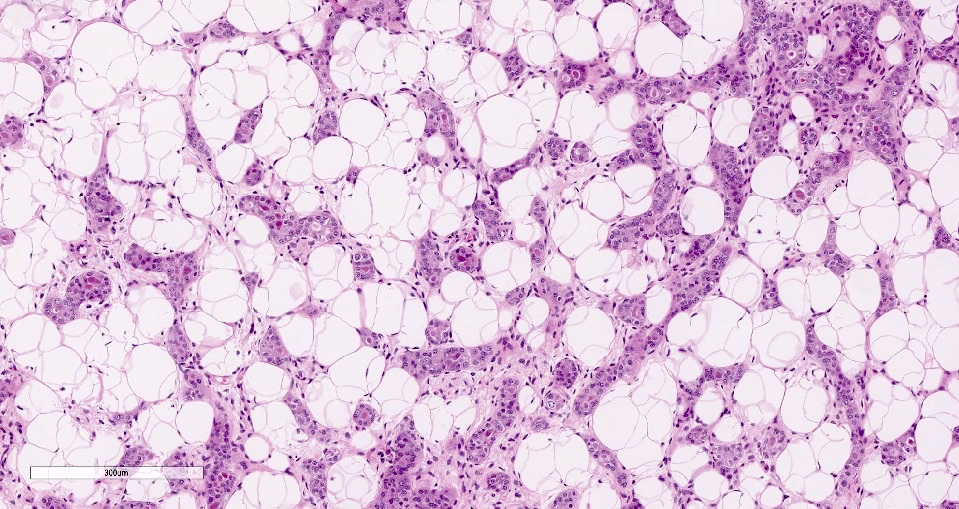
MGA in the adipose tissue
Nuclear atypia in MGA
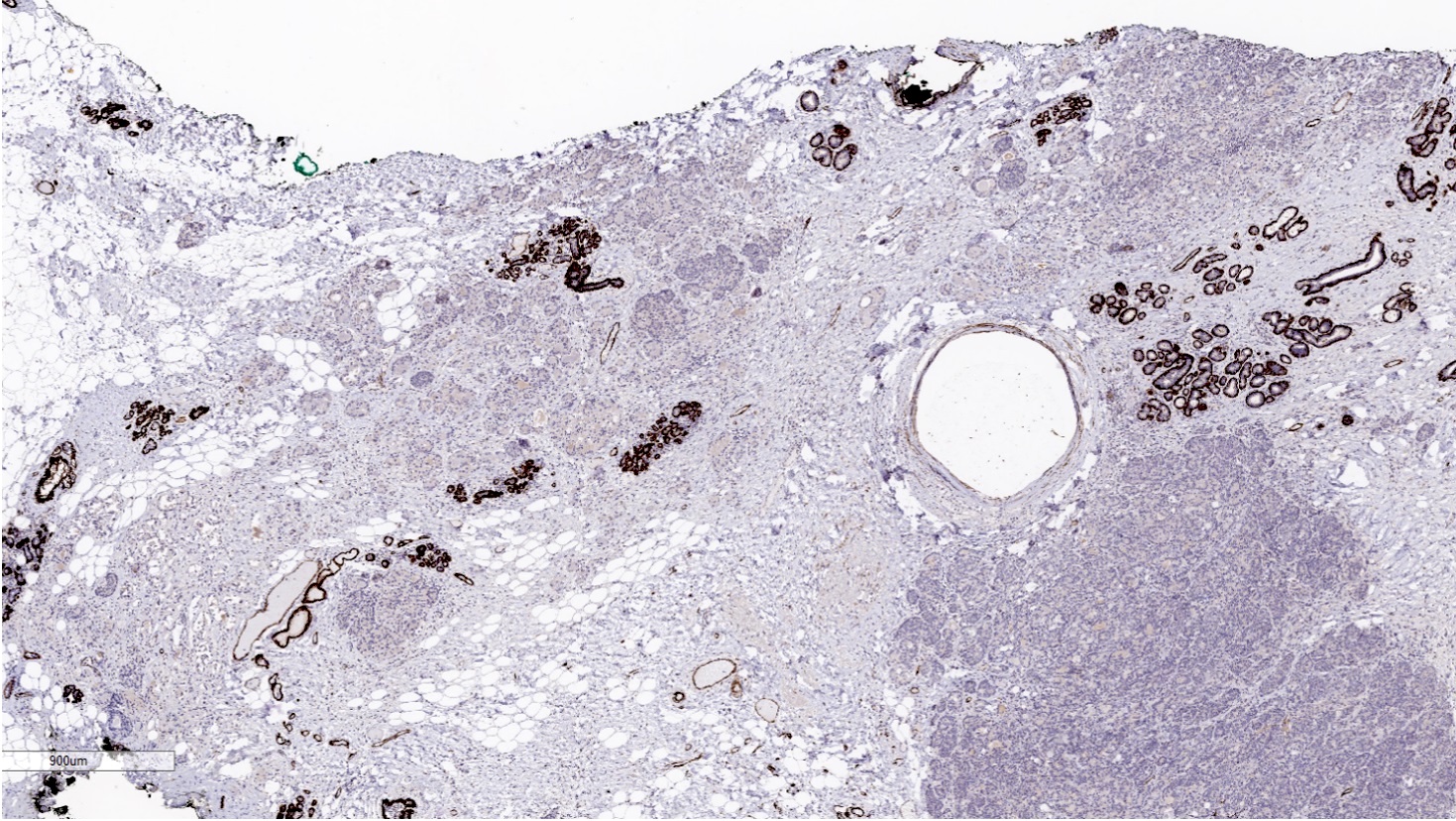
Absence of staining around invasive carcinoma
Invasive carcinoma is negative for ER
Invasive carcinoma is negative for HER2
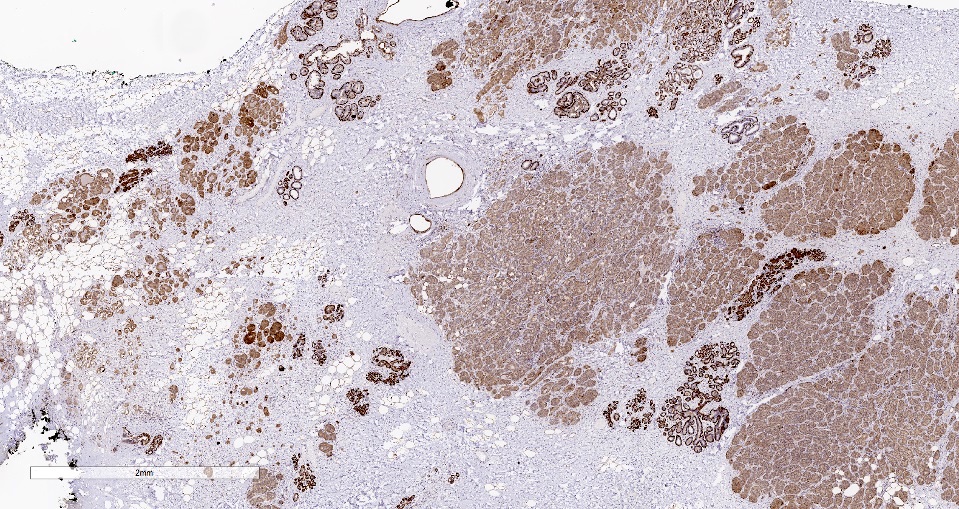
Invasive carcinoma is positive for S100
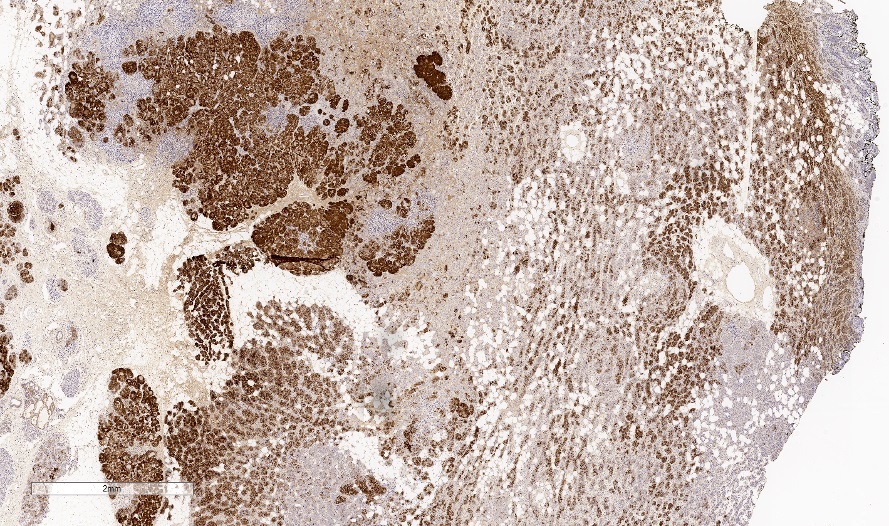
Invasive carcinoma is positive for lysozyme
PASD cytoplasmic staining
- Fine needle aspiration: hypercellular, atypical cells in sheets, round to oval nuclei, single nucleoli, mild pleomorphism in size, moderately increased N:C ratio, intercellular cystic spaces, acinic pattern, cytoplasmic vacuoles and granules visible on Papanicolaou and Giemsa stains (Cytopathology 2013;24:403)
- PASD
- EMA (100% positive, 29/29 cases)
- S100 (93% positive, 50/54 cases)
- Lysozyme (95% positive, 39/41 cases)
- Alpha-1-antichymotrypsin / trypsin (96% positive, 25/26 cases)
- Amylase (94% positive, 17/18 cases)
- E-cadherin (100% positive, 7/7 cases)
- CK7 (100% positive, 9/9 cases)
- Ki67 (range 5 - 30% most commonly reported)
- GCDFP-15 (56% positive, 14/25 cases)
- Reference: Breast 2022;66:208
- Cells with vacuolated cytoplasm containing many electron dense granules of varying size and a prominent rough endoplasmic reticulum (RER) (J Breast Cancer 2011;14:160)
Images hosted on other servers:

Cytoplasmic electron dense granules

Dilation of RER

Acinar cell granules, prominent RER
- No pathognomonic genomic alterations have been described
- Has a similar molecular profile to triple negative breast carcinoma and does not share the genomic rearrangement seen in salivary gland acinic cell carcinoma (Histopathology 2019;75:931)
- TP53 mutations are the most consistent molecular event (Breast 2022;66:208)
- PIK3CA and other mutations have been described in a subset of cases (Mod Pathol 2017;30:69)
- BRCA1 gene alterations have also been described (BMC Cancer 2013;13:46, Histol Histopathol 2023;38:91)
- Breast (right), lumpectomy:
- Acinic cell carcinoma (see comment)
- Comment: Sections show breast tissue involved by acinic cell carcinoma in solid nests and acini of polygonal cells with granular eosinophilic cytoplasm. These tumor cells display round, uniform nuclei with prominent nucleoli. Periodic acid-Schiff with diastase (PASD) staining demonstrates the presence of zymogen-like granules in the cytoplasm, confirming the acinar differentiation characteristic of this tumor.
- Lactational changes:
- Cytoplasmic vacuolization and secretory material
- Microglandular adenosis:
- Intact basal lamina
- Adenoid cystic carcinoma:
- Dual cell population showing positivity for myoepithelial markers like SMA
- Mucoepidermoid carcinoma:
- Presence of intracellular and extracellular mucin
- Mucicarmine positive
A premenopausal woman presents with a painless, palpable, slow growing mass in her left breast. Histological examination reveals cells with abundant eosinophilic and basophilic cytoplasm with large coarse PASD+ intracytoplasmic granules and centrally located nuclei with prominent nucleoli, showing an infiltrative microglandular growth pattern. What is the most likely diagnosis?
- Acinic cell carcinoma
- Angiolipoma
- Burkitt lymphoma
- Fibroadenoma
- Invasive lobular carcinoma
Comment Here
Reference: Acinic cell carcinoma
Which immunostain expression would be the most helpful to support the suspected diagnosis?
- E-cadherin+
- HER2+ (3+)
- Lysozyme+
- Ki67 > 90%
- S100+
Comment Here
Reference: Acinic cell carcinoma
- ER+, PR+, HER2+
- ER+, PR+, HER2-
- ER+, PR-, HER2-
- ER-, PR-, HER2+
- ER-, PR-, HER2-
Comment Here
Reference: Acinic cell carcinoma

