
Breast
Other nonneoplastic
Lactating adenoma
Editor-in-Chief: Debra L. Zynger, M.D.


Last author update: 21 April 2020
Last staff update: 27 December 2021
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Lactating adenoma [title] breast


Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Virtual slides | Cytology description | Cytology images | Positive stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Motanagh S, Muller K. Lactating adenoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/breastlactatingadenoma.html. Accessed April 1st, 2025.
Definition / general
- Well circumscribed mass, arising during or shortly after pregnancy, composed of cuboidal cells with actively secreting, closely packed glands
Essential features
- Most prevalent breast lesion in pregnant women and during postpartum period
- Must be distinguished from carcinoma, as breast cancer is the second most common malignancy during pregnancy
- Age range (19 - 34 years), female
- Benign, slow growing
- Unknown capability of malignant transformation
Terminology
- Adenomatous lactational hyperplasia, nodular lactational hyperplasia (not recommended by WHO)
ICD coding
Epidemiology
- 19 - 34 years, female, predominantly in third decade of life
- Most prevalent breast lesion in pregnant women (mostly third trimester) and during postpartum period (puerperium)
Sites
- Predominantly in breast, may develop in ectopic breast tissue along milk line extending from axilla to vulva (Radiol Case Rep 2017;12:215, Pan Afr Med J 2012;13:47)
Pathophysiology
- Unknown if de novo neoplasm or hyperplastic condition
- Some postulate may arise in a pre-existing adenoma (tubular adenoma, fibroadenoma) with superimposed lactational changes; however, lack of MED12 exon 2 mutations, frequently found in fibroadenomas, does not support this theory (Genes Chromosomes Cancer 2017;56:11)
- Increase in serum estrogen, progesterone and prolactin
Clinical features
- Painless, soft, palpable, solid, mobile discrete mass
- May be bilateral and multifocal
- Infarction may lead to pain, tenderness and rapid enlargement
Diagnosis
- Imaging: ultrasound (first line modality given increased density of pregnant / lactating breast tissue), mammogram, MRI (J Am Coll Radiol 2018;15:S263, AJR Am J Roentgenol 2013;200:3213)
- Invasive procedure: biopsy, fine needle aspiration
Radiology description
- Homogeneous, circumscribed, hypoechoic mass, with posterior acoustic enhancement and gentle lobulations (J Hum Lact 2016;32:559)
- May show hypervascularization (Breast Care (Basel) 2019;14:30)
- May appear hyperechoic or radiolucent due to milk fat
- Rarely shows irregular margins mimicking malignancy (Radiology 1998;206:271)
Radiology images
Contributed by Kristen E. Muller, D.O.
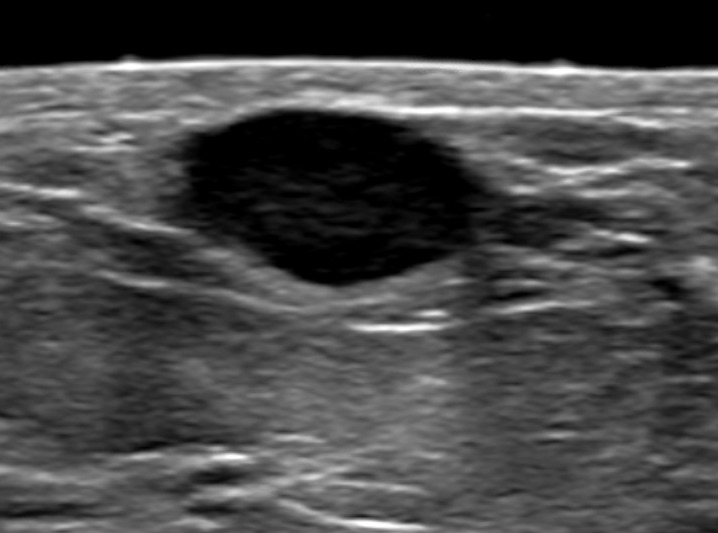
Well circumscribed hypoechoic mass
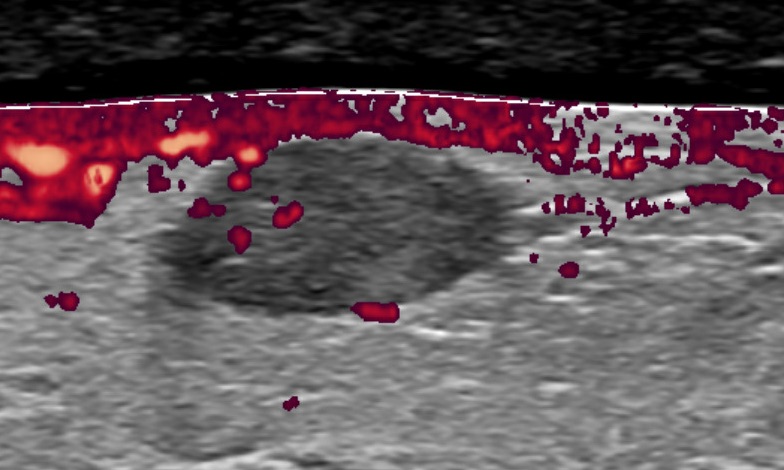
Hypoechoic mass with hypervascularity
Prognostic factors
- Slow growing, spontaneous regression
- No progression to cancer on follow up studies
- Unknown if capable of carcinogenesis or risk factor
- Coexistence of lactating adenoma with breast malignancy reported (Indian J Cancer 2015;52:585, J Clin Pathol 2005;58:87)
Case reports
- 21 year old woman with rapidly enlarging giant lactating adenoma (J Surg Case Rep 2010;2010:8)
- 22 year old woman with continuously enlarging lactating adenoma misdiagnosed as malignancy on imaging (Breast J 2019;25:1278)
- 25 year old lactating woman with co-occurrence of lactating adenoma and infiltrating ductal carcinoma (J Clin Diagn Res 2015;9:ED14)
- 33 year old woman with aggressively enlarging lactating adenoma prompting multiple biopsies (Radiol Case Rep 2017;12:215)
- 35 year old woman with lactating adenoma 6 months postpartum and continued breast feeding within 24 hours post operation (J Hum Lact 2016;32:559)
Treatment
- Observation for slow growing
- Many spontaneously regress after termination of breastfeeding
- Enucleation in cases that warrant excision (enlarging, worrisome clinical or histologic features)
Clinical images
Images hosted on other servers:

Large mass
Gross description
- Lacks true capsule, well circumscribed, lobulated, solitary or multiple, firm / rubbery mass, gray-tan cut surface, may have necrosis / infarction (Radiol Case Rep 2017;12:215)
- Size: usually < 5 cm, rare reported cases of giant lactating adenomas up to 25 cm (J Surg Case Rep 2010;2010:8, AJR Am J Roentgenol 1999;173:933)
Gross images
Contributed by Dr. Mark R. Wick
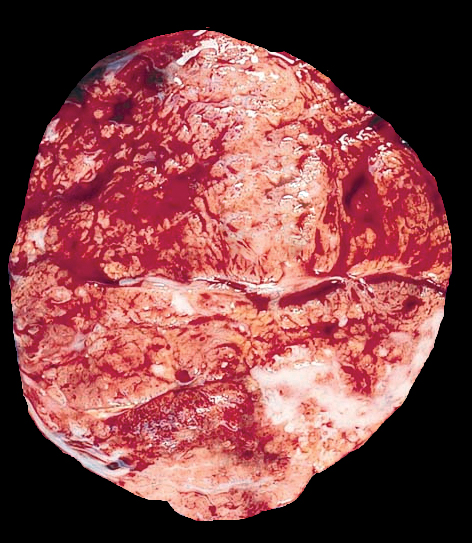
Lactating adenoma
Images hosted on other servers:

Well circumscribed mass
Microscopic (histologic) description
- Well circumscribed proliferation of hyperplastic closely packed lobules with both epithelial and myoepithelial cell layers separated by thin, delicate connective tissue
- Glands lined by actively secreting cuboidal or hobnail shaped cells with small round nuclei and granular to clear vacuolated cytoplasm
- Variably prominent small, pinpoint nucleoli may be seen but cells lack cytologic atypia
- Occasional mitoses may be seen
- Resembles pregnancy-like (pseudolactational) changes
- May resemble fibroadenoma or tubular adenoma with lactational change microscopically
Microscopic (histologic) images
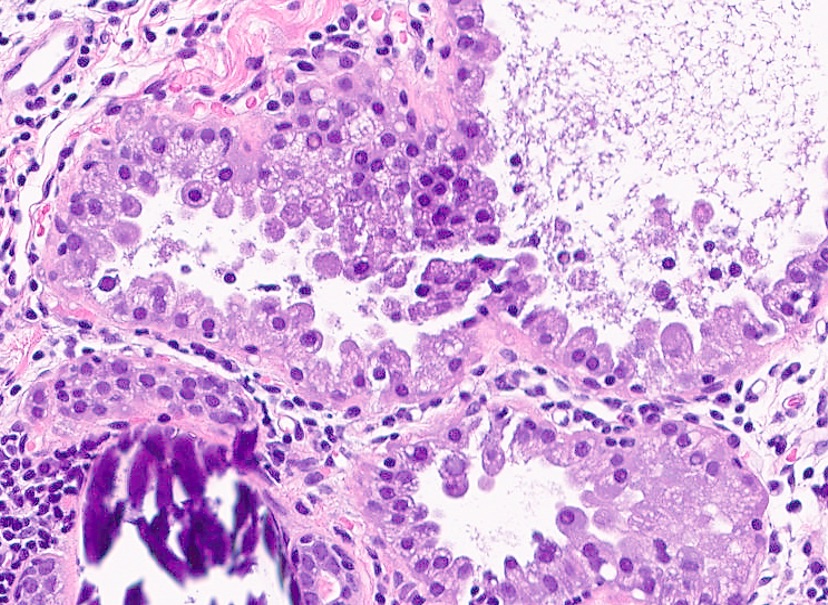
Contributed by Kristen E. Muller, D.O.
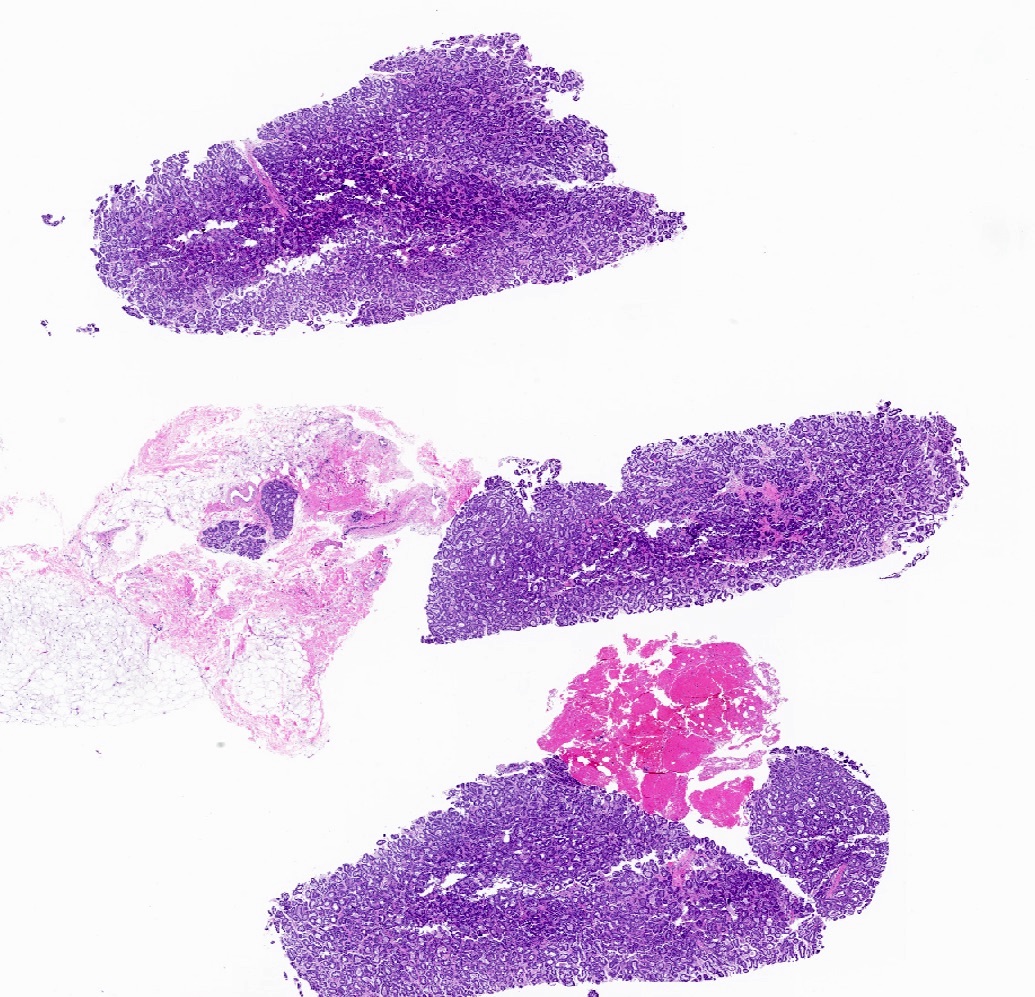
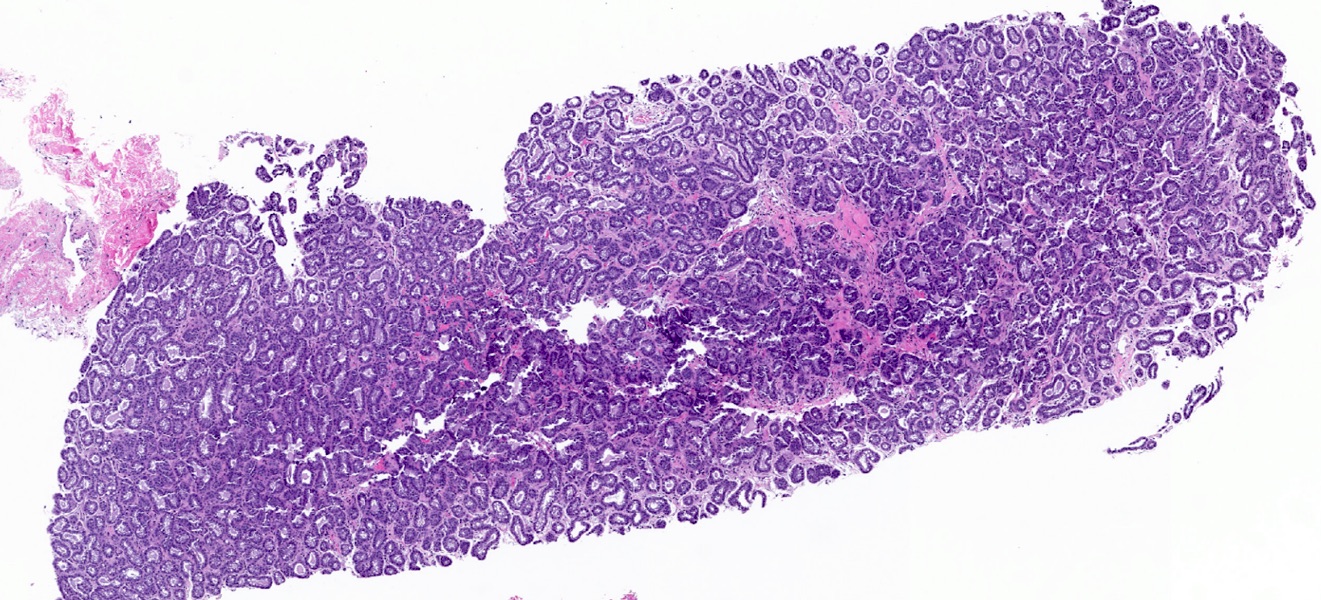
Lactating adenoma biopsy
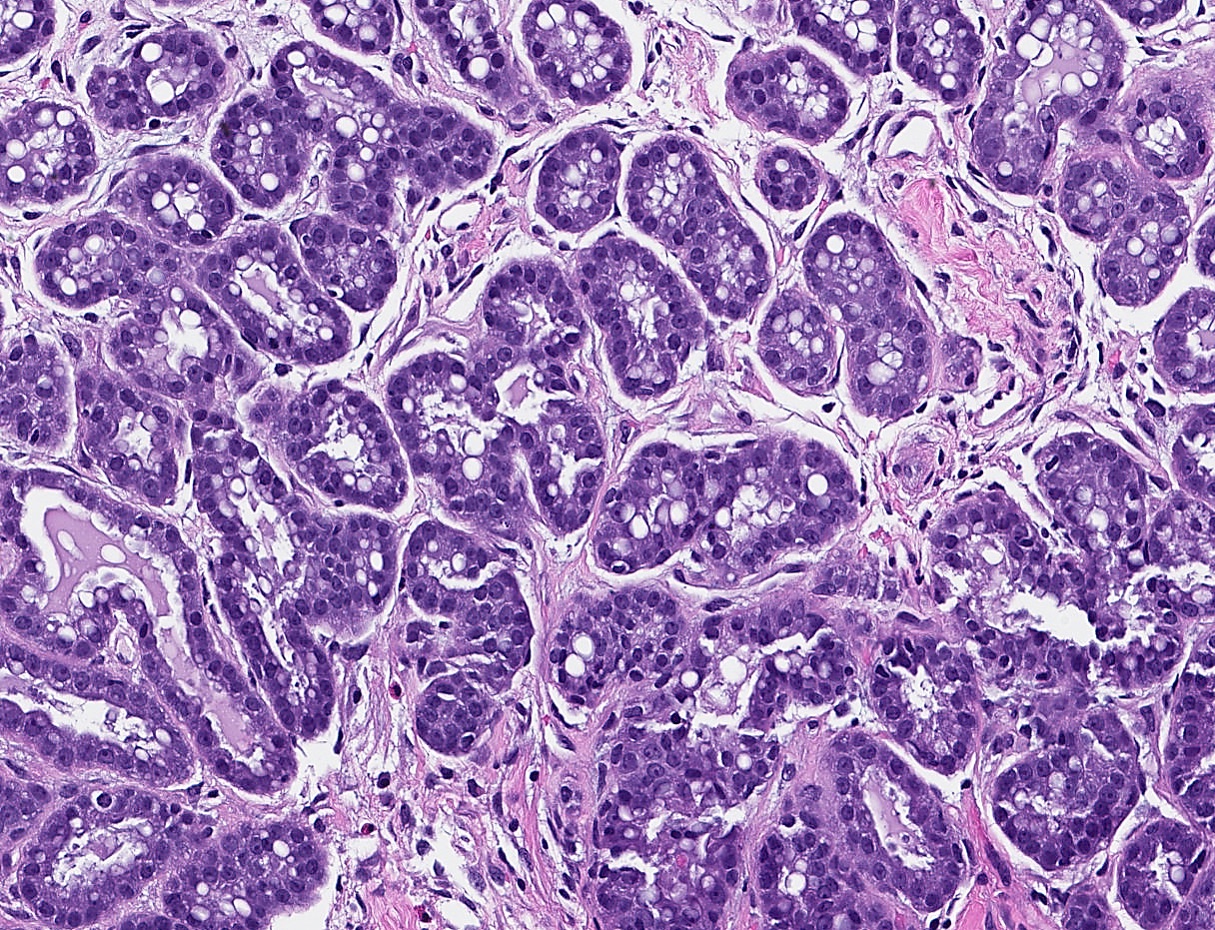
Vacuolated cytoplasm
Hypersecretory features
Delicate stroma

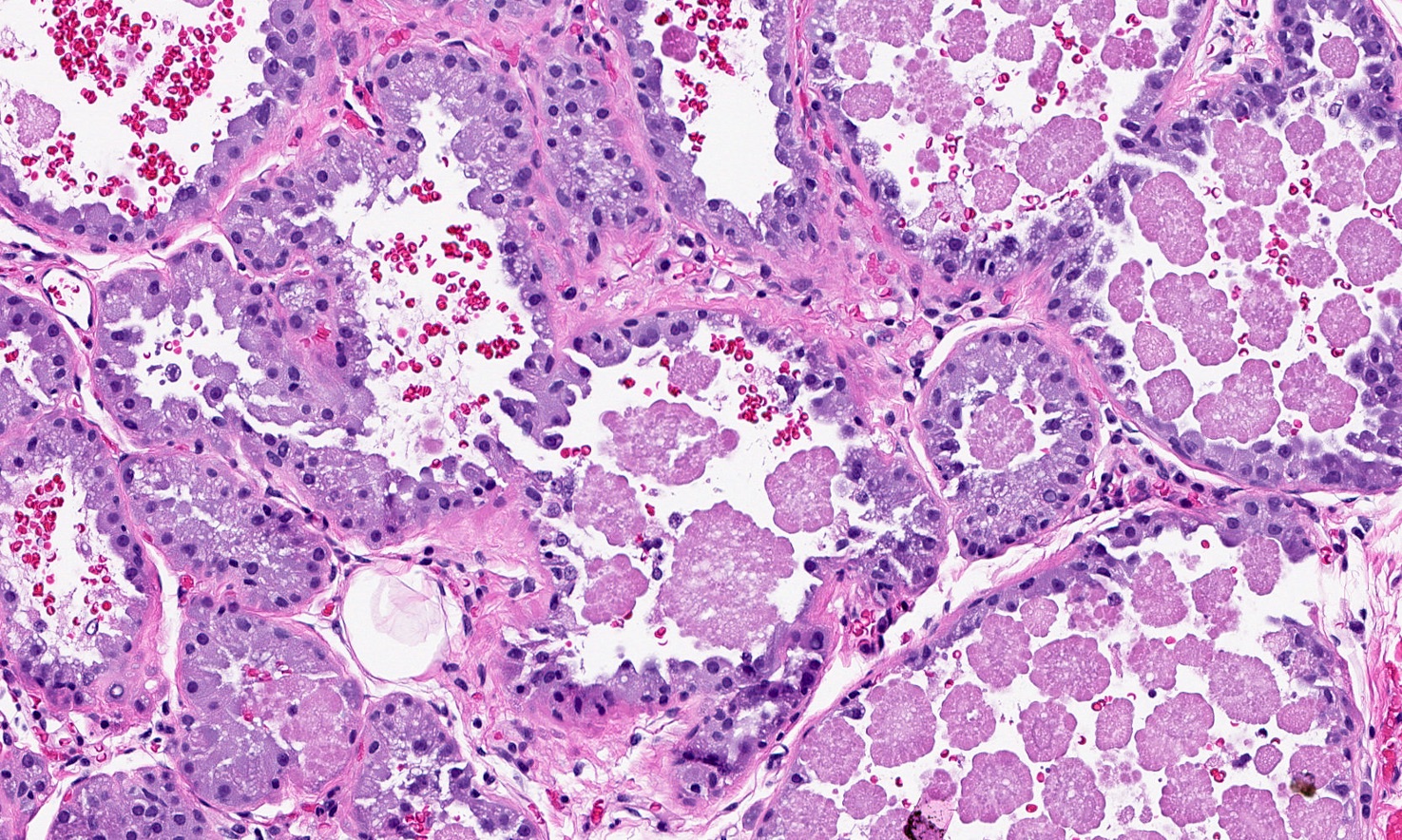
Prominent hobnailing
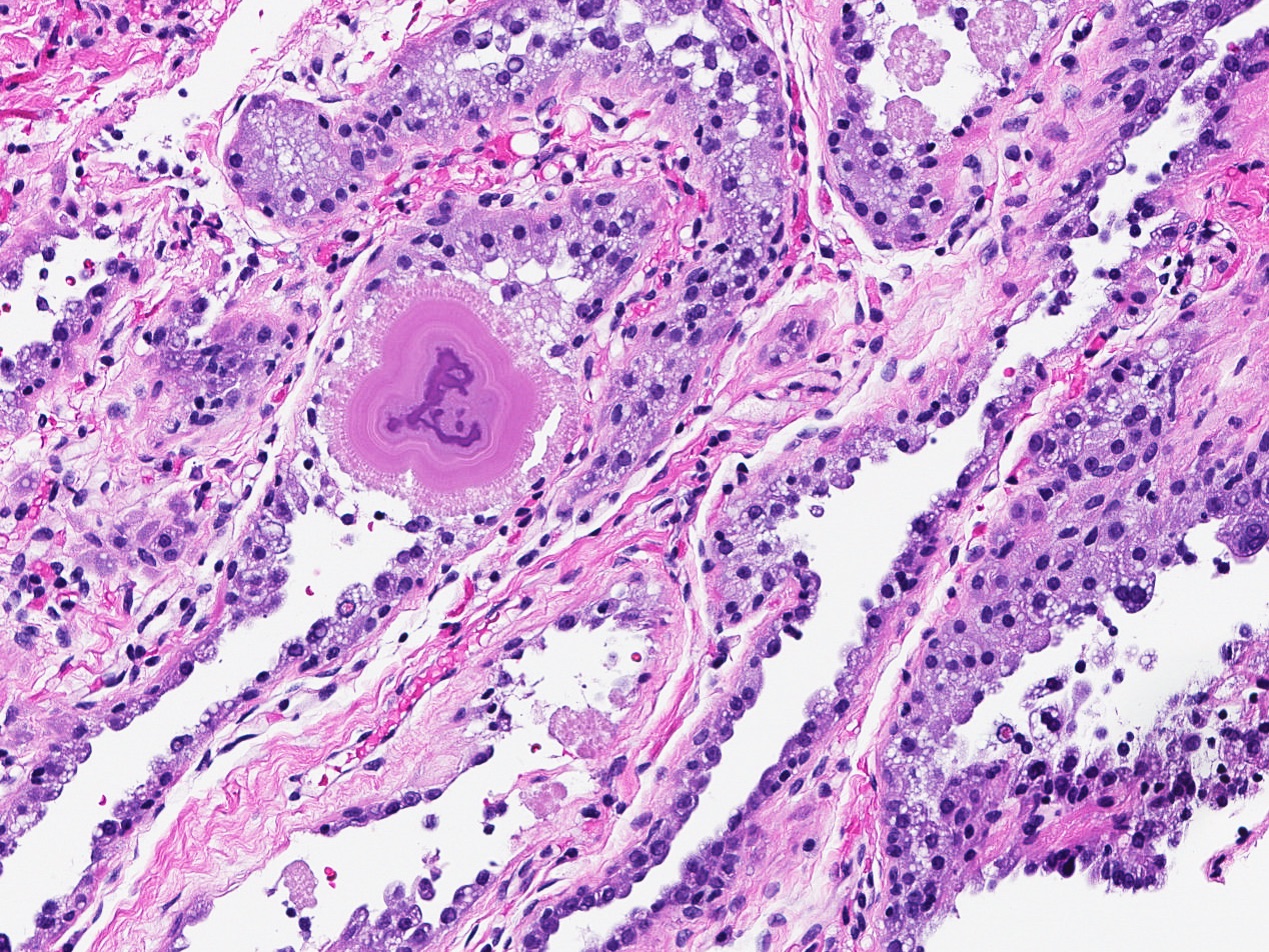
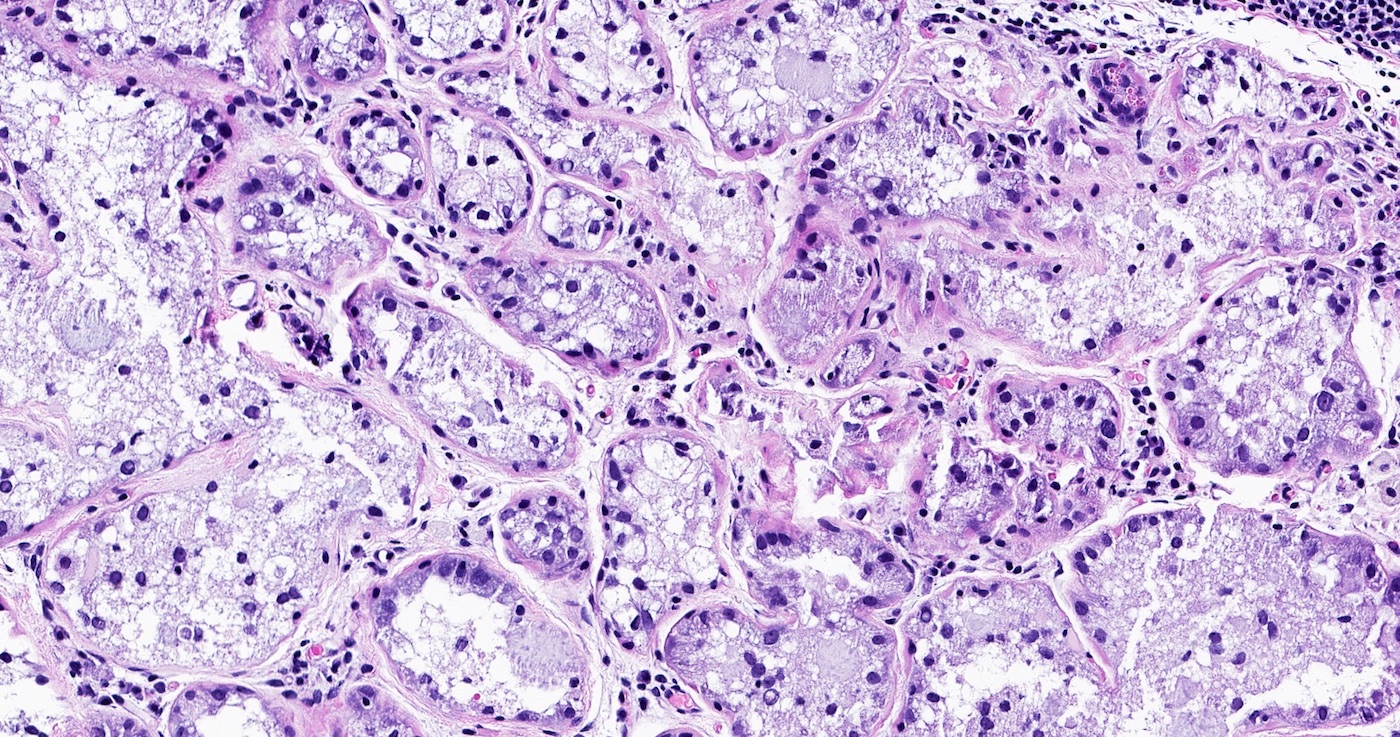
Psammomatous calcification
Virtual slides
Images hosted on other servers:

Lactating adenoma
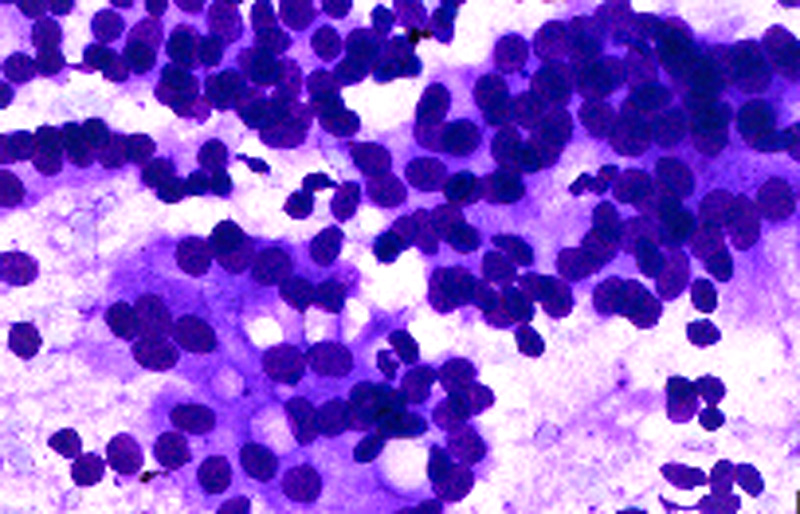
Cytology description
- Loose cohesive clusters of monomorphic cells or single cells
- Cells contain foamy to finely vacuolated cytoplasm, round uniform nuclei with fine chromatin and small nucleoli (J Clin Diagn Res 2013;7:2417)
- Background of foamy material
Cytology images
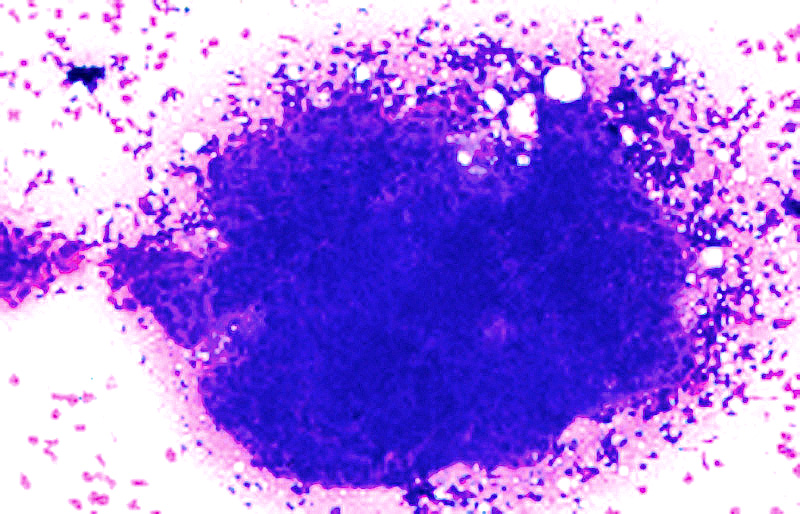
Contributed by Dr. Mark R. Wick
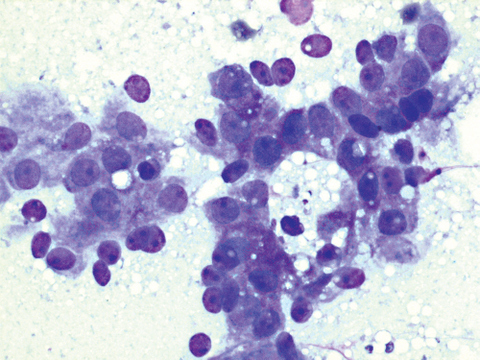
FNAB
Images hosted on other servers:
Increased lobular size
Cytoplasmic vacuoles and background foamy material
Molecular / cytogenetics description
- 50 gene NGS panel showed no mutations in three lactating adenomas in one series, including MED12 exon 2 mutations (frequently seen in fibroadenomas) (Genes Chromosomes Cancer 2017;56:11)
Sample pathology report
- Right breast mass, needle biopsy:
- Breast tissue with lactational change / lactating adenoma
- Microcalcifications associated with lactational change / lactating adenoma
Differential diagnosis
- Lobular hyperplasia (normal physiologic event in pregnancy):
- Not a well defined mass
- Delayed involution of lactation:
- Not a well defined mass
- Hyperplastic and involuting lobules
- Neutrophils, macrophages and lymphocytes in background
- More frequently associated with calcifications
- Fibroadenoma with secretory activity:
- Fibroepithelial architecture
- Prominent stroma
- Focal, not diffuse, proliferation of cells with secretory activity
Additional references
Board review style question #1
Which of the following is correct for the entity pictured from this breast biopsy from a 27 year old pregnant woman?
- Frequently shows a prominent stromal component similar to fibroepithelial lesions
- Histologically composed of closely packed glands lined by actively secreting cuboidal or hobnail shaped cells
- Never develops in ectopic breast tissue along milk line
- The glands lack a myoepithelial cell layer
- Third most prevalent breast lesion in pregnant women
Board review style answer #1
B. Histologically composed of closely packed glands lined by actively secreting cuboidal or hobnail shaped cells
Comment Here
Reference: Lactating adenoma
Comment Here
Reference: Lactating adenoma
Board review style question #2
What is the most common breast lesion in pregnant and lactating women?
- Adenomyoepithelioma
- Atypical ductal hyperplasia
- Fibroadenoma
- Invasive ductal carcinoma
- Lactating adenoma
Board review style answer #2
