
Breast
Other benign tumors
Fibromatosis
Editorial Board Member: Kristen E. Muller, D.O.
Deputy Editor-in-Chief: Gary Tozbikian, M.D.


Last author update: 15 June 2021
Last staff update: 20 March 2024
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Breast fibromatosis


Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Frozen section description | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Cytology images | Positive stains | Negative stains | Molecular / cytogenetics description | Videos | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: LaBoy C, Siziopikou KP. Fibromatosis. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/breastfibromatosis.html. Accessed April 3rd, 2025.
Definition / general
- Low grade infiltrative spindle cell neoplasm composed of fibroblasts and myofibroblasts
Essential features
- Rare low grade neoplasm with infiltrative pattern
- Bland spindle cells arranged in long intersecting fascicles within a collagenous stroma
- Characterized by alterations in WNT / beta catenin pathway
- Does not metastasize but can locally recur after surgical excision
Terminology
- Desmoid tumor, aggressive fibromatosis, desmoid type fibromatosis, extra-abdominal desmoid
ICD coding
- ICD-O: 8821/1 - desmoid type fibromatosis
- ICD-11: 2F75 & XH13Z3 - neoplasms of uncertain behavior of breast & aggressive fibromatosis
Epidemiology
- < 0.2% of tumors of the breast
- F > M, third through fifth decades
- Reference: Breast Care (Basel) 2021;16:77
Sites
- May be primary to the breast or be secondary extension into the breast from the chest wall
Pathophysiology
- Up to 95% harbor CTNNB1 activating mutation (sporadic); APC gene inactivating mutation responsible for remainder of cases (hereditary) (Cancers (Basel) 2020;12:1851)
- Through the WNT / beta catenin pathway, these mutations motivate cells to proliferate while destabilizing beta catenin that then accumulates within the nucleus (J Clin Oncol 2018;36:202)
Etiology
- Can consequently occur after surgery, trauma or rarely, after breast implants (Breast Care (Basel) 2021;16:77, Cancers (Basel) 2020;12:1851)
- Estrogen thought to influence growth (Breast Care (Basel) 2021;16:77, Indian J Surg Oncol 2020;11:71)
- Can be associated with Gardner syndrome or familial adenomatous polyposis
Clinical features
- Slow growing, often self detected firm mass
Diagnosis
- May arise as palpable mass that appears as abnormality on mammography
- Rarely presents with breast pain, nipple discharge and skin retraction (Breast Care (Basel) 2021;16:77)
Radiology description
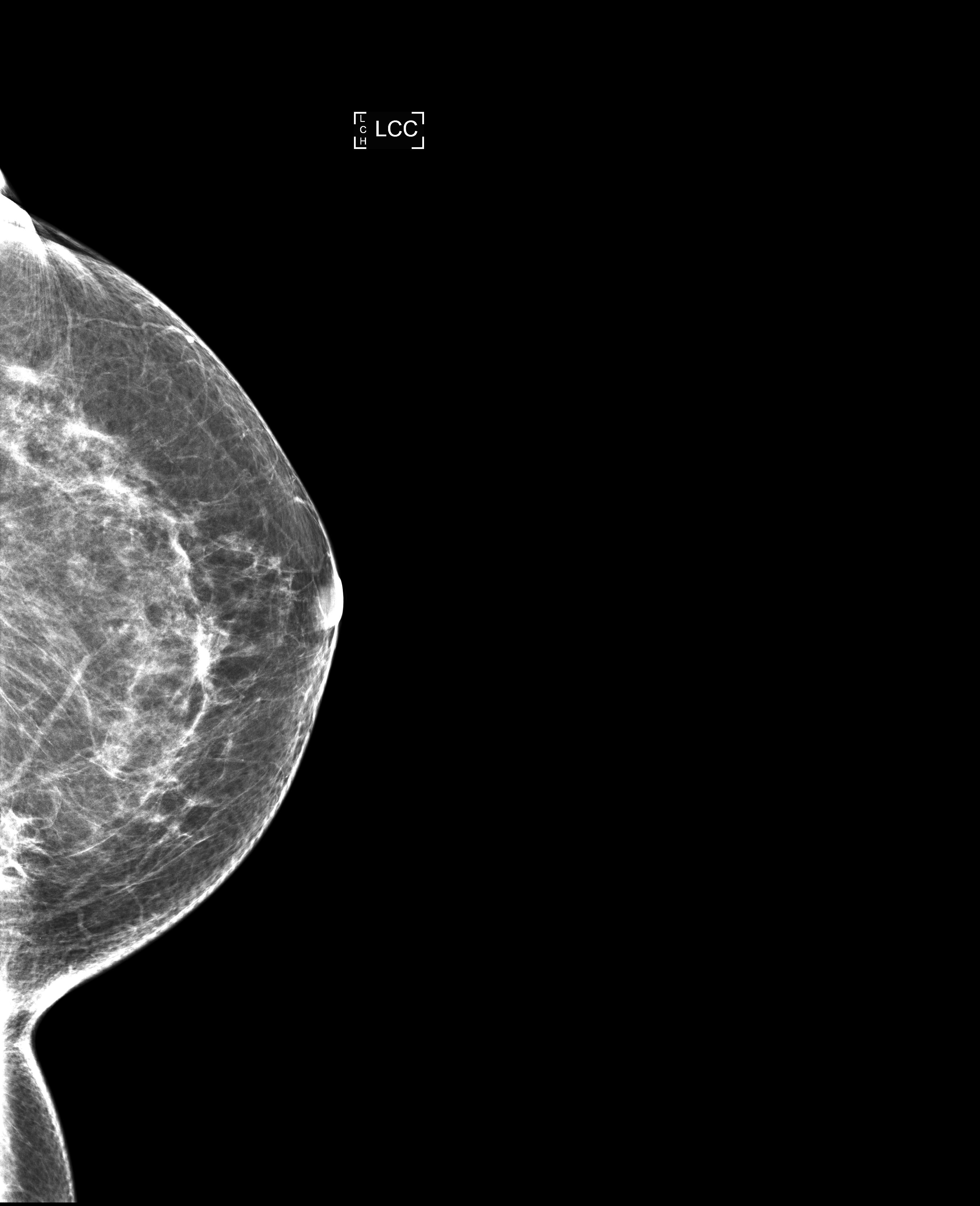
- Imaging may show well circumscribed mass or poorly defined / spiculated mass that can be mistaken for malignant process (Breast Care (Basel) 2021;16:77)
Radiology images
Contributed by Carissa LaBoy, M.D.

Mammogram of right breast

Ultrasound of right breast
Mammogram of breast mass

Ultrasound of left breast
Prognostic factors
- Does not metastasize (Pathologica 2019;111:344)
- Locally aggressive, local recurrence rates reported in 29% to as high as 40 - 50% of cases after excision (Ann Surg Oncol 2008;15:274, J Clin Oncol 2018;36:202)
- Margin status not reliable risk factor for recurrence (J Clin Oncol 2018;36:202, Cancers (Basel) 2020;12:1851)
Case reports
- 25 year old woman with indentation and pain in left inframammary fold (Radiol Case Rep 2018;13:1174)
- 31 year old woman with dimpling in the left breast (Int J Surg Case Rep 2017;41:392)
- 36 year old woman with rapidly growing lump in right breast (Oncol Lett 2017;14:1433)
- 42 year old woman with breast implants and palpable lump in left breast (Radiol Case Rep 2017;12:431)
- 60 year old man with 2 year history of right breast mass (Chirurgia (Bucur) 2019;114:664)
Treatment
- Surgical local excision
- Other options include active surveillance for asymptomatic patients and systemic therapy, such as adjuvant radiation for patients with multiple recurrences (Breast Care (Basel) 2021;16:77, Cancers (Basel) 2020;12:1851)
Gross description
- Well to poorly circumscribed mass of variable size (from < 1 cm to > 10 cm), with white-gray whorled or trabeculated cut surface
Gross images
Images hosted on other servers:

White trabeculated cut surface


Chest wall mass
Frozen section description
- Bland spindle cells seen on intraoperative frozen section would prompt benign diagnosis
Microscopic (histologic) description
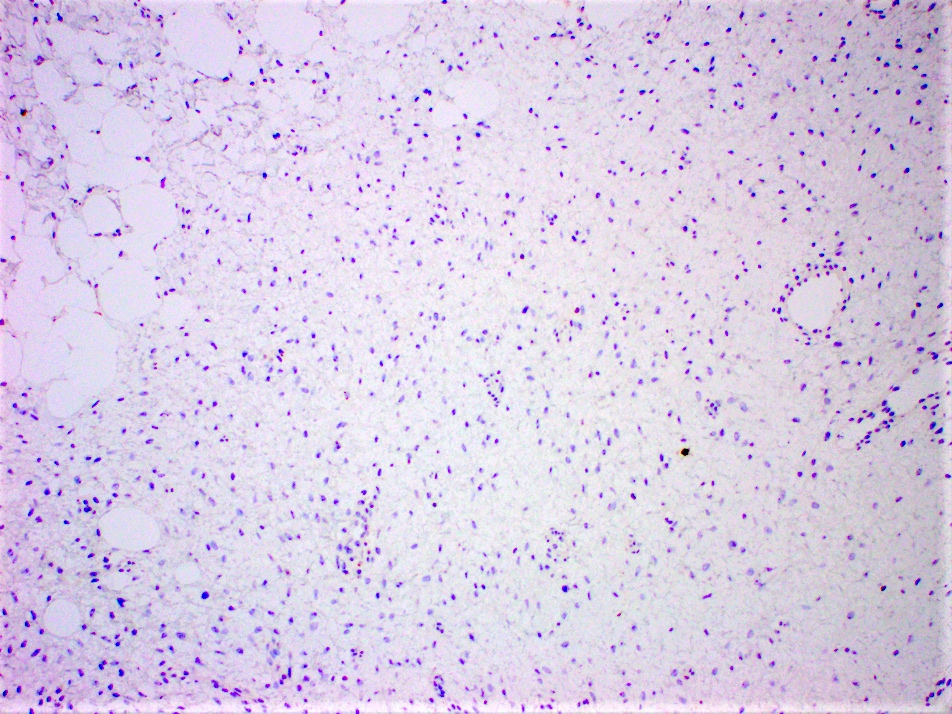
- Long intersecting fascicles composed of bland spindle cells with indistinct borders, hyperchromatic nuclei with occasional nucleoli and eosinophilic cytoplasm
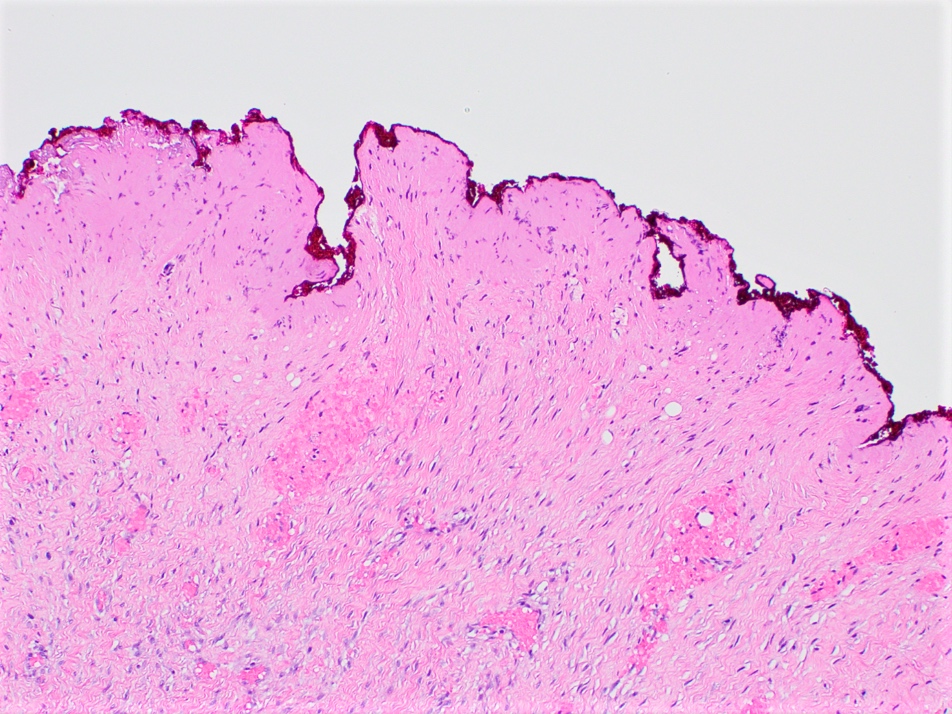
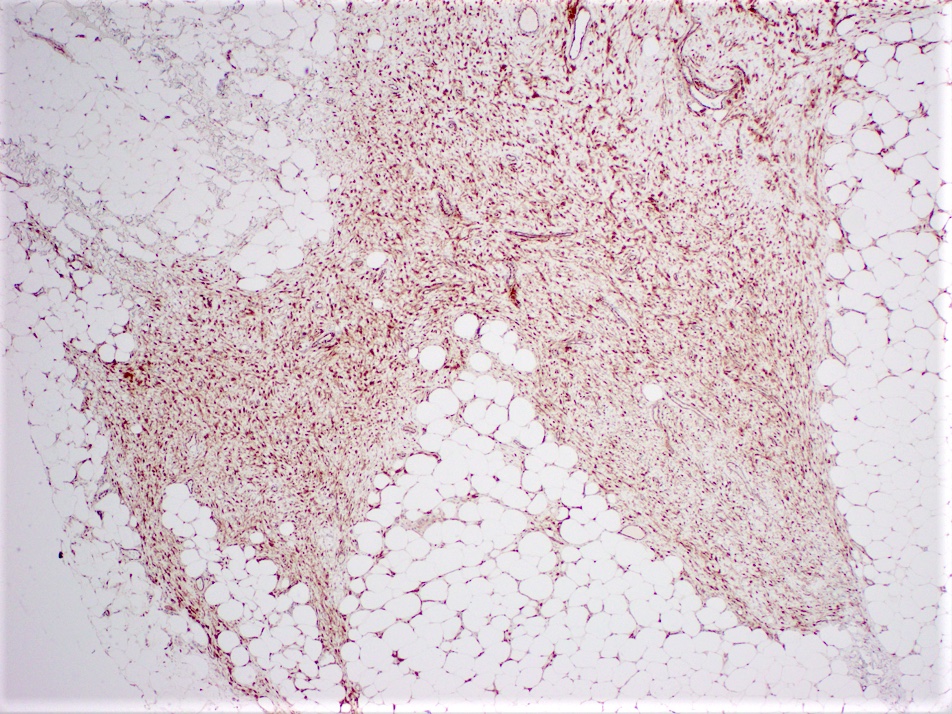
- Cells infiltrate normal ducts and lobules, adipose tissue and skeletal muscle, thus mimicking invasive process
- Mitosis is rare
- Background stroma has thickened collagen resembling keloid
- Older lesions may calcify
- Lymphoid aggregates may be seen at the periphery of the lesion
- Reference: Pathologica 2019;111:344
Microscopic (histologic) images
Contributed by Carissa LaBoy, M.D.
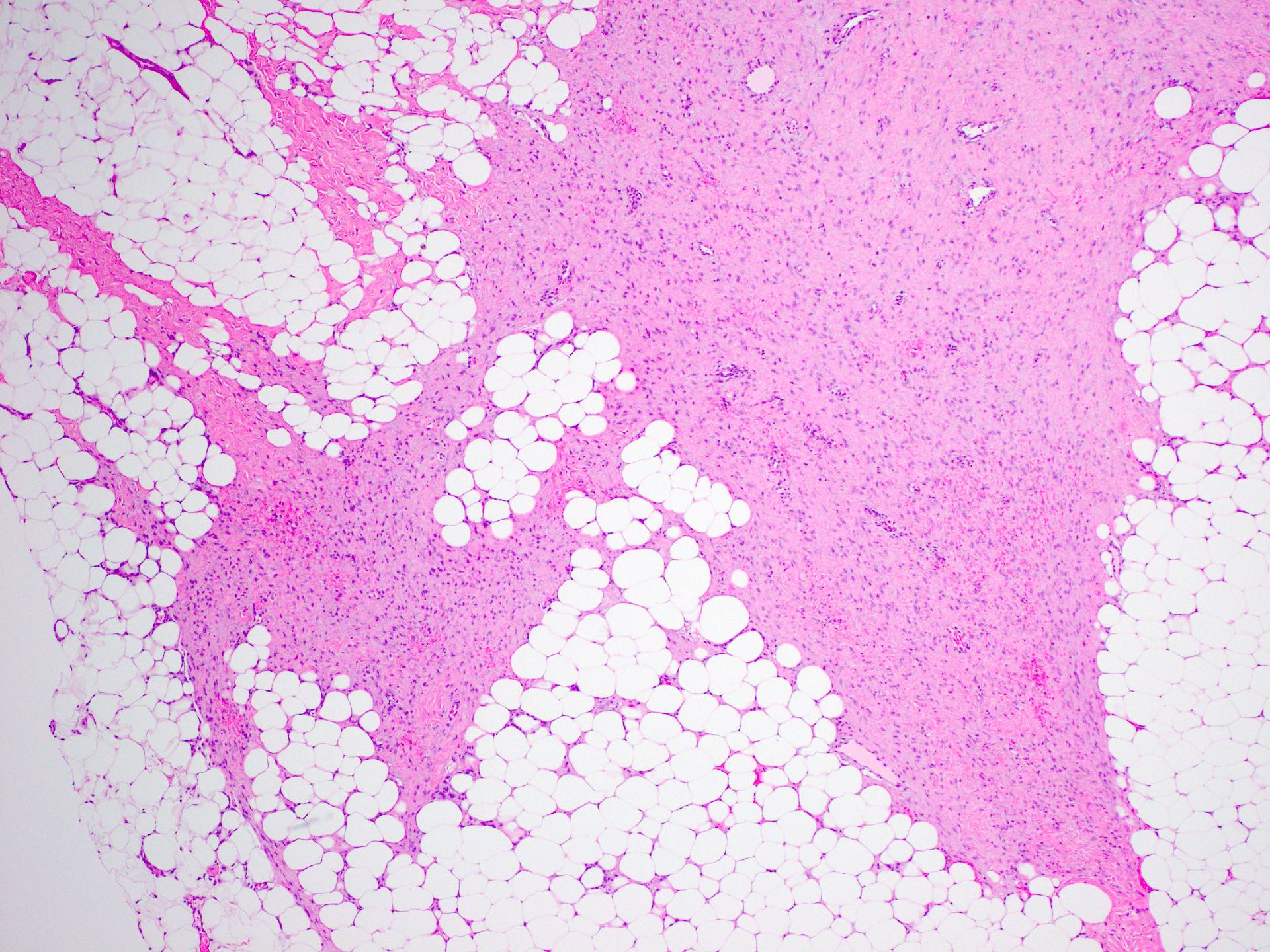
Infiltrative breast mass
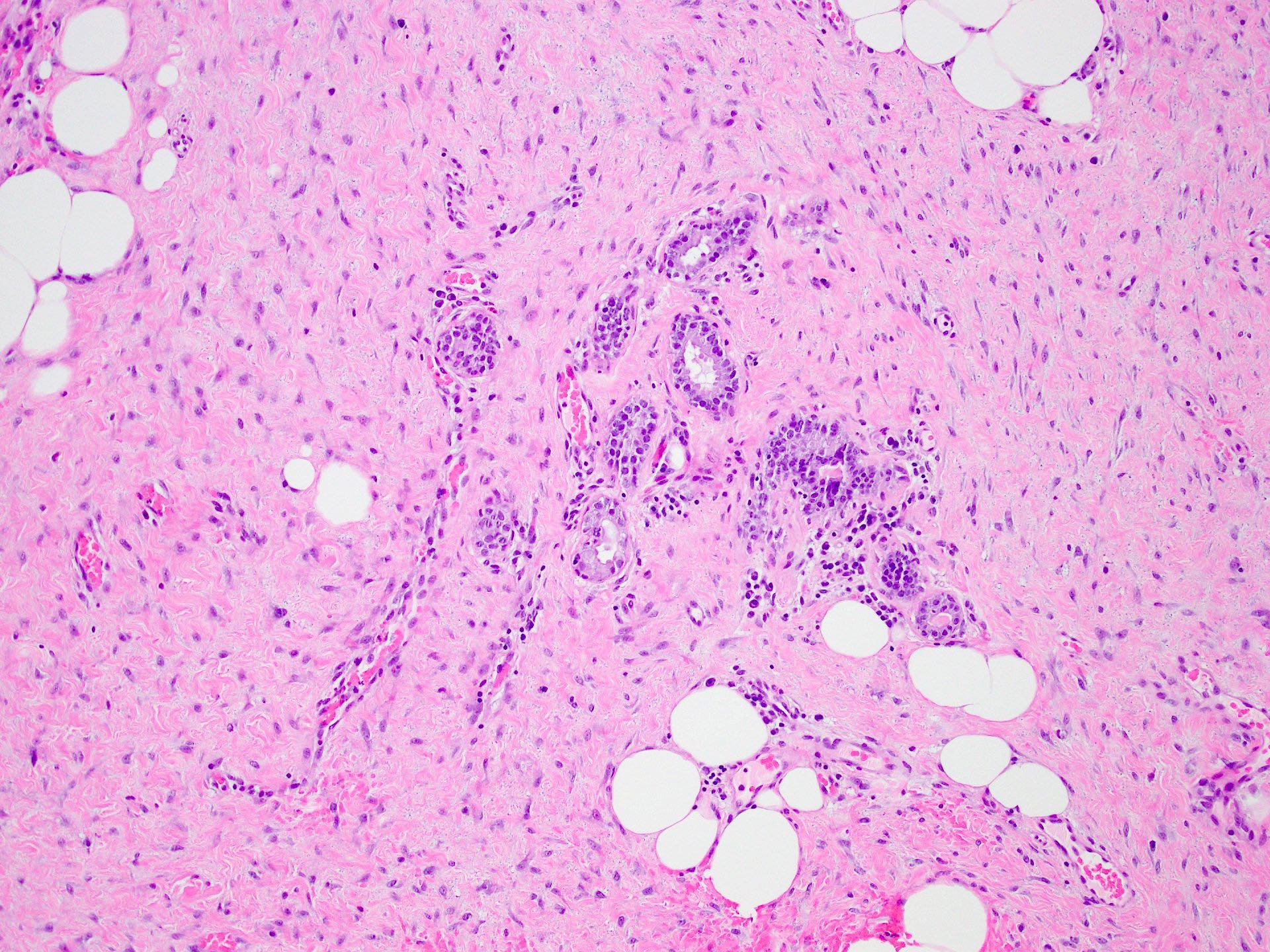
Cells entrapping normal ducts
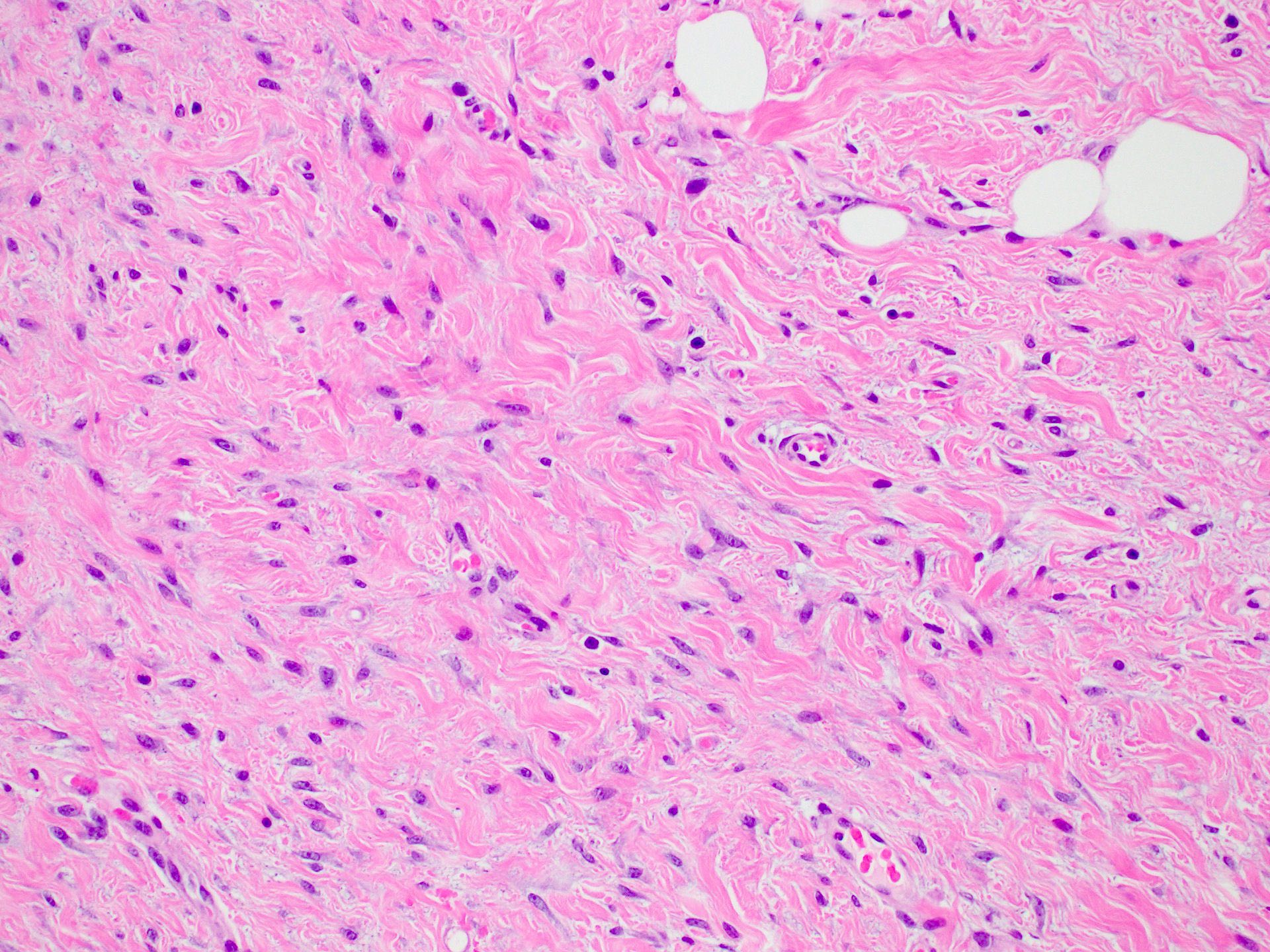
Cells in collagenous stroma
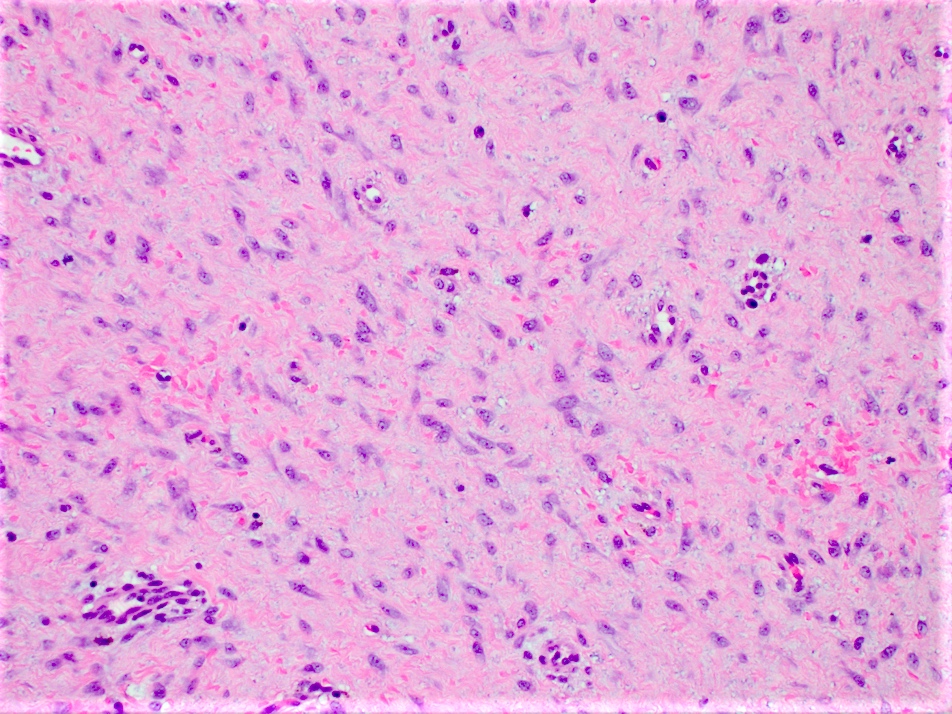
Bland spindle cells
Positive margin on excision
Beta catenin positivity
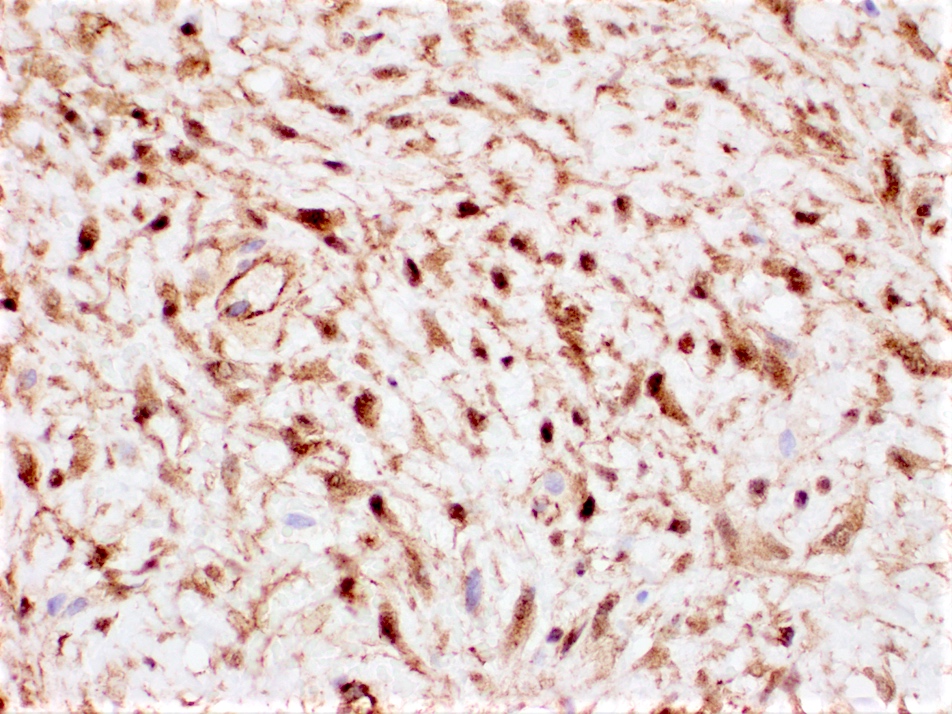
Beta catenin nuclear positivity
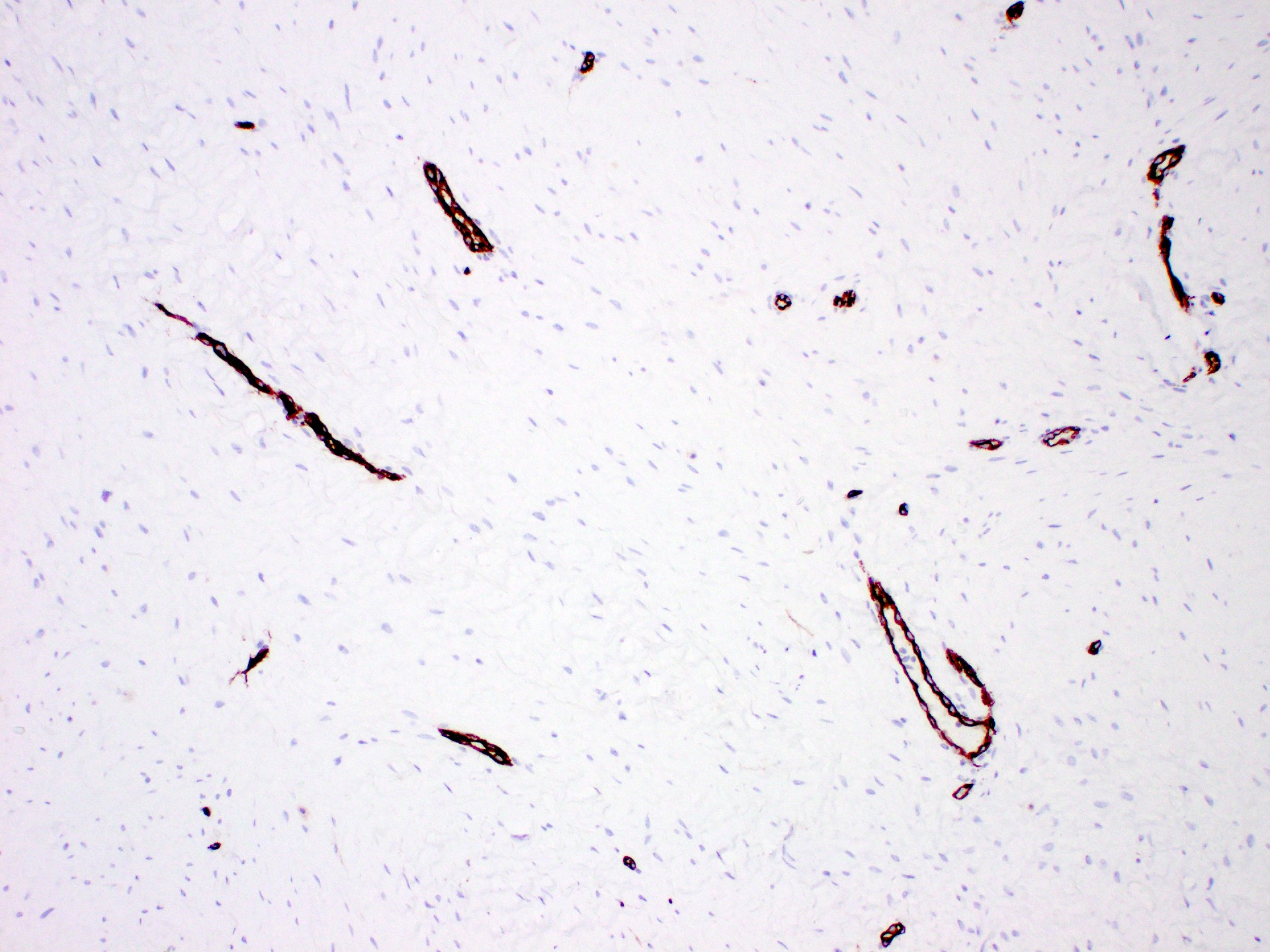
CD34 negative spindle cells
Pancytokeratin negative spindle cells
Cytology description
- Fine needle aspiration is difficult and often yields fibrous nondiagnostic material
- When successful, fine needle aspiration shows bland spindle cells with hyperchromatic nuclei and wispy cytoplasm within abundant stroma (Cancer 2007;111:166)
Cytology images
Images hosted on other servers:


Fine needle aspiration of fibromatosis


Fine needle aspiration of fibromatosis
Positive stains
- Beta catenin (80% of cases) (Pathologica 2019;111:344)
- Not specific, can also be positive in spindle cell carcinomas, metaplastic breast carcinomas and benign phyllodes tumors (Breast Care (Basel) 2021;16:77)
- SMA
- Calponin
Negative stains
- Pancytokeratin
- p63
- CD34
- ER
- PR
- HER2
- Reference: Breast Care (Basel) 2021;16:77
Molecular / cytogenetics description
- Sequencing can identify activating CTNNB1 mutation or inactivating APC mutation in 79% of cases (Hum Pathol 2002;33:39, Curr Opin Oncol 2017;29:268)
- Trisomies in chromosome 8 or 20 occur, significance is unknown (J Clin Oncol 2018;36:202)
Videos
Review of fibromatosis
Sample pathology report
- Left breast, needle localized lumpectomy:
- Fibromatosis, measuring 2.8 cm in greatest dimension
- Margins negative with tumor > 0.5 cm from all margins
Differential diagnosis
- Scar:
- Focally infiltrative lesion composed of bland spindle cells with associated histiocytes, foreign body giant cell reaction and lymphocytes
- History of prior procedure
- Nodular fasciitis:
- Focally infiltrative lesion composed of spindle cells forming short fascicles or storiform pattern with increased mitotic activity
- Does not display nuclear beta catenin staining
- Dermatofibrosarcoma protuberans:
- Focally infiltrative lesion with spindle cells in storiform growth pattern and low mitotic activity
- Low grade fibromatosis-like metaplastic carcinoma:
- Infiltrative lesion composed of spindle to epithelioid cells arranged in small clusters with low mitotic activity
- Cytokeratin and p63 positive
- Low grade myofibroblastic sarcoma:
- Focally infiltrative lesion composed of spindle cells arranged in fascicles
- Mild to moderate nuclear pleomorphism and brisk mitosis
- Myofibroblastoma:
- Spindle cells arranged in short, disorganized fascicles with intersecting thick collagen bands resembling keloid; do not typically entrap normal ducts or lobules
- Benign phyllodes tumor:
- Well circumscribed mass with hyperplastic epithelium within a hypercellular stroma composed of spindle cells with mild atypia and low mitotic activity
Board review style question #1
What is the pattern of beta catenin immunohistochemical staining for fibromatosis pictured above?
- Cytoplasmic
- Cytoplasmic and membranous
- Membranous
- Nuclear
Board review style answer #1
D. Nuclear. The pathophysiology of fibromatosis involves an activating CTNNB1 mutation in sporadic cases and an APC gene inactivating mutation in hereditary cases. Both types of mutations activate the WNT / beta catenin pathway, motivating cells to proliferate while degrading beta catenin, which then accumulates within the nucleus. This in turn yields a nuclear pattern of staining by immunohistochemistry.
Comment Here
Reference: Fibromatosis
Comment Here
Reference: Fibromatosis
Board review style question #2
Which of the following is correct regarding the histologic features and clinical behavior of breast fibromatosis?
- Chemotherapy is the preferred treatment due to high mitotic activity
- Metastasis is a common feature of this tumor
- Necrosis and pleomorphism make this a high grade tumor
- Tumor has a high frequency of local recurrence
Board review style answer #2
D. Tumor has a high frequency of local recurrence. Breast fibromatosis is a low grade tumor consisting of bland spindle cells with rare or no mitotic activity and no metastatic potential. However, due to its infiltrative nature, this tumor has a tendency to locally recur after surgical excision.
Comment Here
Reference: Fibromatosis
Comment Here
Reference: Fibromatosis
