
Breast
Fibrocystic changes
Microcysts
Author: Kristen E. Muller, D.O.
Editorial Board Members: Julie M. Jorns, M.D., Gary Tozbikian, M.D.

Last author update: 19 April 2021
Last staff update: 23 October 2024
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Breast [title] Microcysts


Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Cytology images | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Muller KE. Microcysts. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/breastcysts.html. Accessed April 2nd, 2025.
Definition / general
- Round to ovoid fluid filled structures of variable size lined by bland epithelium, part of nonproliferative fibrocystic changes
Essential features
- Very common nonproliferative fibrocystic change
- Round to ovoid fluid filled cysts lined by flat, cuboidal or columnar cells that may be attenuated and denuded
- Cysts alone do not increase risk of breast cancer
Terminology
- Blue dome cysts: based on gross appearance
- Type 1 cysts:
- Na/K ratio of 3 or less: increased breast cancer risk; associated with higher levels of estrogen, melatonin, epidermal growth factor and DHEA-S and lower levels of TGF-B2 than type 2 cysts (Breast Cancer Res Treat 2007;103:331)
- Type 2 cysts:
- Na/K above 3: reduced breast cancer risk, although patients may have both types of cysts and type 2 cysts can be associated with cancer (Breast 2005;14:37)
- Microcysts: seen during imaging or microscopic exam; not palpable
- Macro or gross cysts: large enough to be palpated
Note:
- Type 1 and type 2 terminology is not commonly used
ICD coding
Epidemiology
- Most common nonproliferative change in breast along with metaplastic changes
- Any age
- 20 - 25% of palpable breast abnormalities that underwent fine needle aspiration were simple cysts (Cancer 2001;93:263)
- Prevalence estimated between 50 - 90% (Breast Cancer Res Treat 2006;97:115)
Sites
- Usually multifocal and bilateral
Pathophysiology
- Arises in the terminal ductal lobular unit (TDLU) → dilation and coalescence of lobular acini
- Gross cysts defined by Haagensen are palpable (Cancer 1989;63:2156)
Etiology
- Unknown
Clinical features
- Large cysts may present as a palpable mass
Diagnosis
- Fine needle aspiration:
- Mass disappears after aspiration and the fluid is nonbloody, yellow or green and serous, no further workup necessary (Can Fam Physician 2012;58:1240)
- Further workup starting with imaging required after aspiration if no fluid, bloody or tenacious fluid or mass persists (Am Fam Physician 2003;68:1983)
- Bloody or cloudy or turbid fluid should be sent for cytopathology review
Radiology description
- Mammography: low density, circumscribed, round, oval or occasionally lobulated masses
- Amorphous, round microcalcifications may be present (Radiol Clin North Am 2010;48:931)
- Ultrasound: avascular, anechoic, oval or round mass with posterior enhancement, cyst flattens with compression, thin septations may be present (Radiol Clin North Am 2010;48:931)
- MRI: no contrast enhancement, hypointense on T1 and hyperintense on T2 (Radiol Clin North Am 2010;48:931)
Radiology images
Contributed by Kristen E. Muller, D.O.
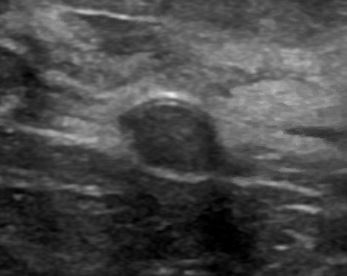
Hypoechoic mass, ultrasound
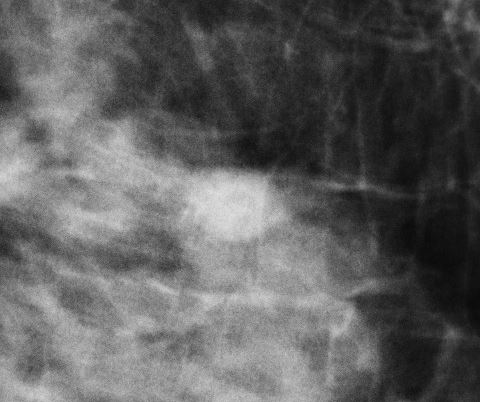
Circumscribed mass, mammogram
Prognostic factors
- Cysts alone: no increased risk of breast cancer (J Natl Cancer Inst 1978;61:1055, Arch Pathol Lab Med 1998;122:1053, N Engl J Med 1985;312:146)
- Cysts and family history of breast cancer, relative risk = 2.7 times higher (N Engl J Med 1985;312:146)
- Gross cysts: may be associated with slight (relative risk = 1.6) increased risk of breast cancer (N Engl J Med 1985;312:146, J Natl Cancer Inst 2004;96:616)
Case reports
- 37 year old man with breast cyst (Cureus 2019;11:e4814)
- 58 year old man with breast cyst (J Radiol Case Rep 2011;5:35)
- 3 family members with autosomal dominant polycystic kidney disease and breast cysts (Iran J Kidney Dis 2009;3:246)
Treatment
- Aspiration / decompression if symptomatic or for diagnostic purposes (See Diagnosis section)
Gross description
- Variable size, usually visible grossly, contains clear, straw colored or brown fluid
- Larger intact cysts may appear blue (blue domed cyst) (Breast Cancer Res Treat 2006;97:115)
Gross images
Contributed by Kristen E. Muller, D.O. and AFIP images
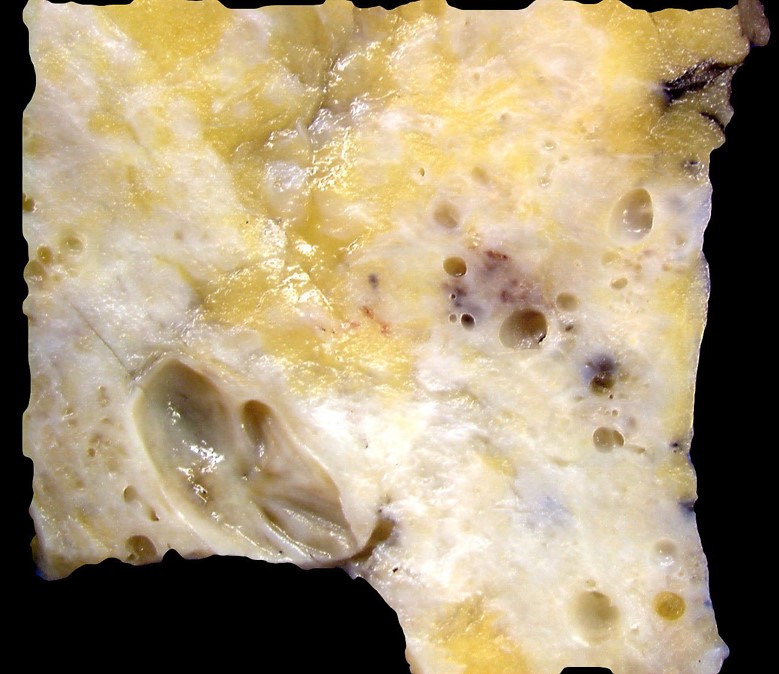
Numerous grossly visible cysts
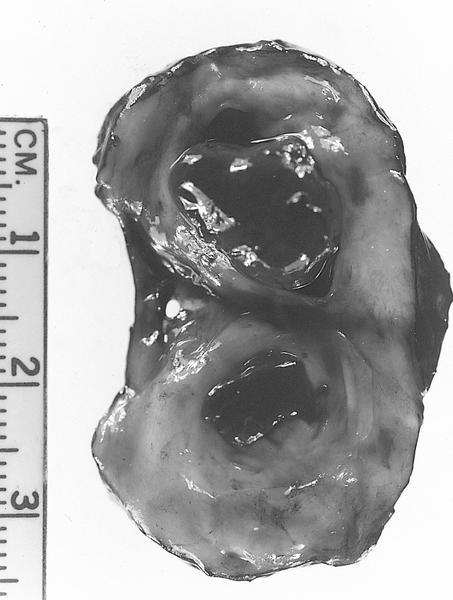
Large hemorrhagic cysts
Images hosted on other servers:


Unopened cyst

Extensive cystic disease
Microscopic (histologic) description
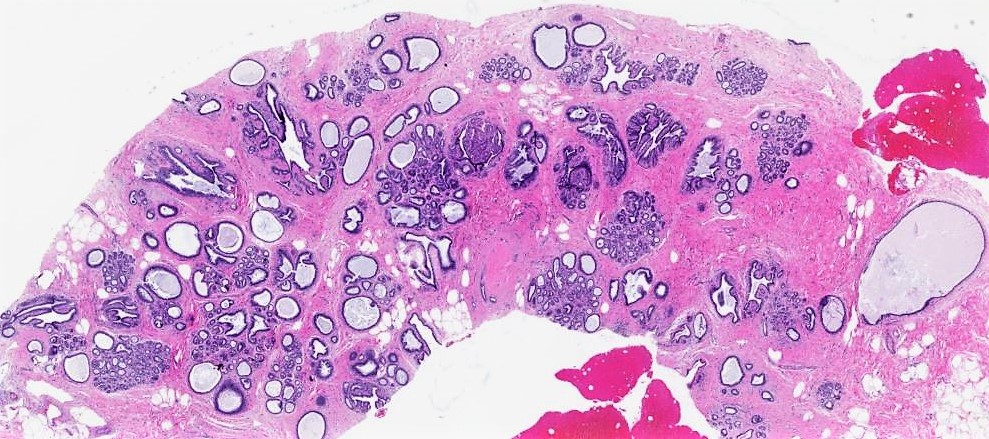
- Dilated glands lined by flat cuboidal or columnar cells
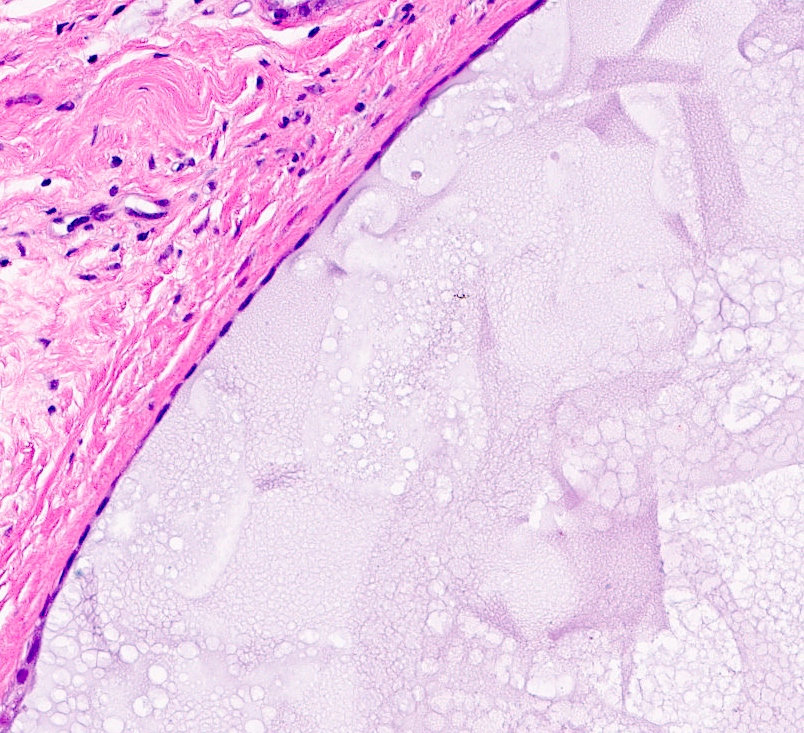
- Epithelium layer may be attenuated or absent
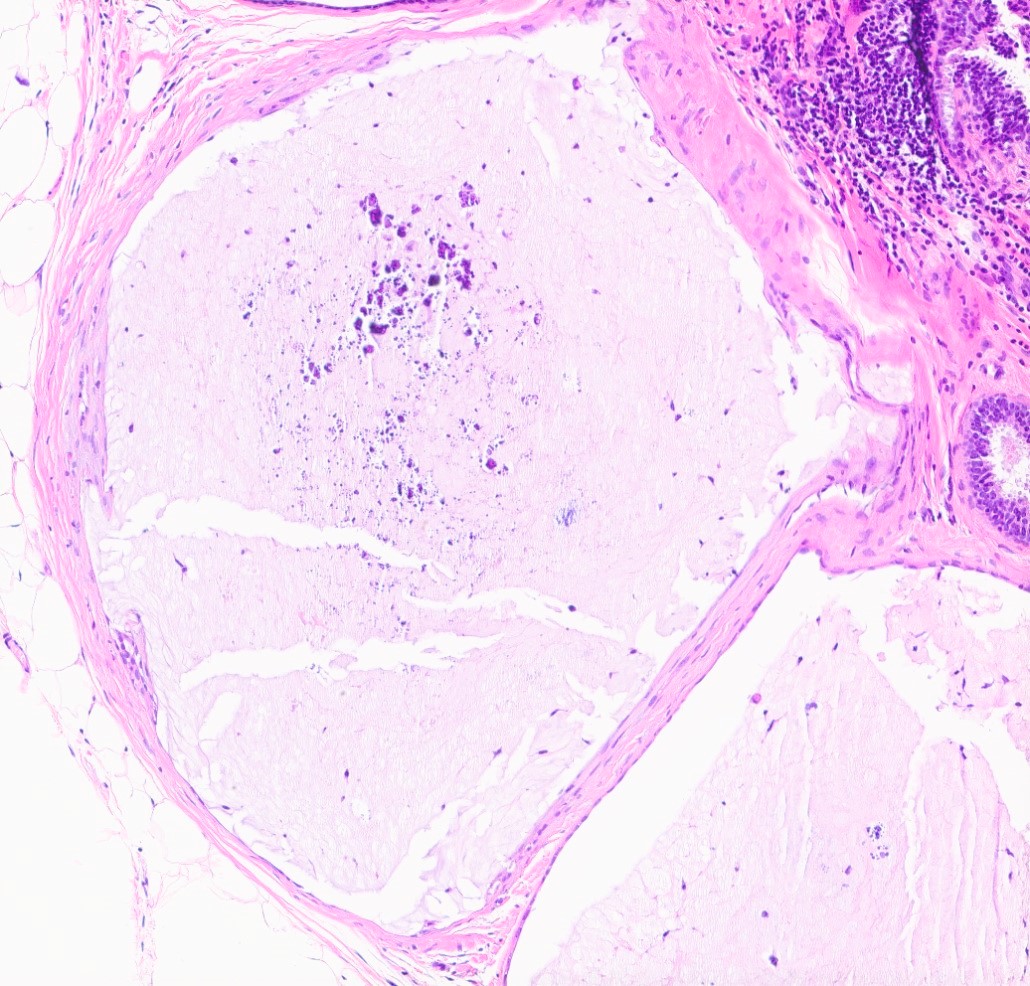
- Cyst wall may show dense fibrosis and scattered inflammatory cells
- May rupture and elicit inflammatory response with foamy macrophages, cholesterol clefts and fibrosis (Breast Cancer Res Treat 2002;75:213, Breast Cancer Res Treat 2006;97:115)
Microscopic (histologic) images
Contributed by Kristen E. Muller, D.O.
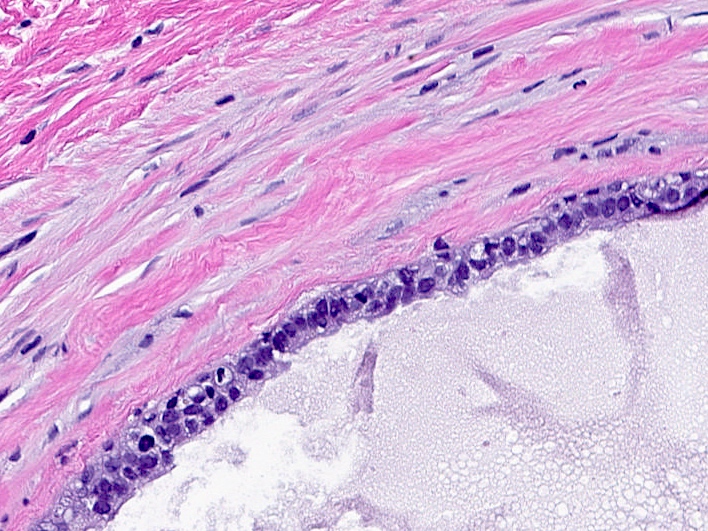
Simple epithelial lining
Flattened epithelial lining
Denuded epithelial lining

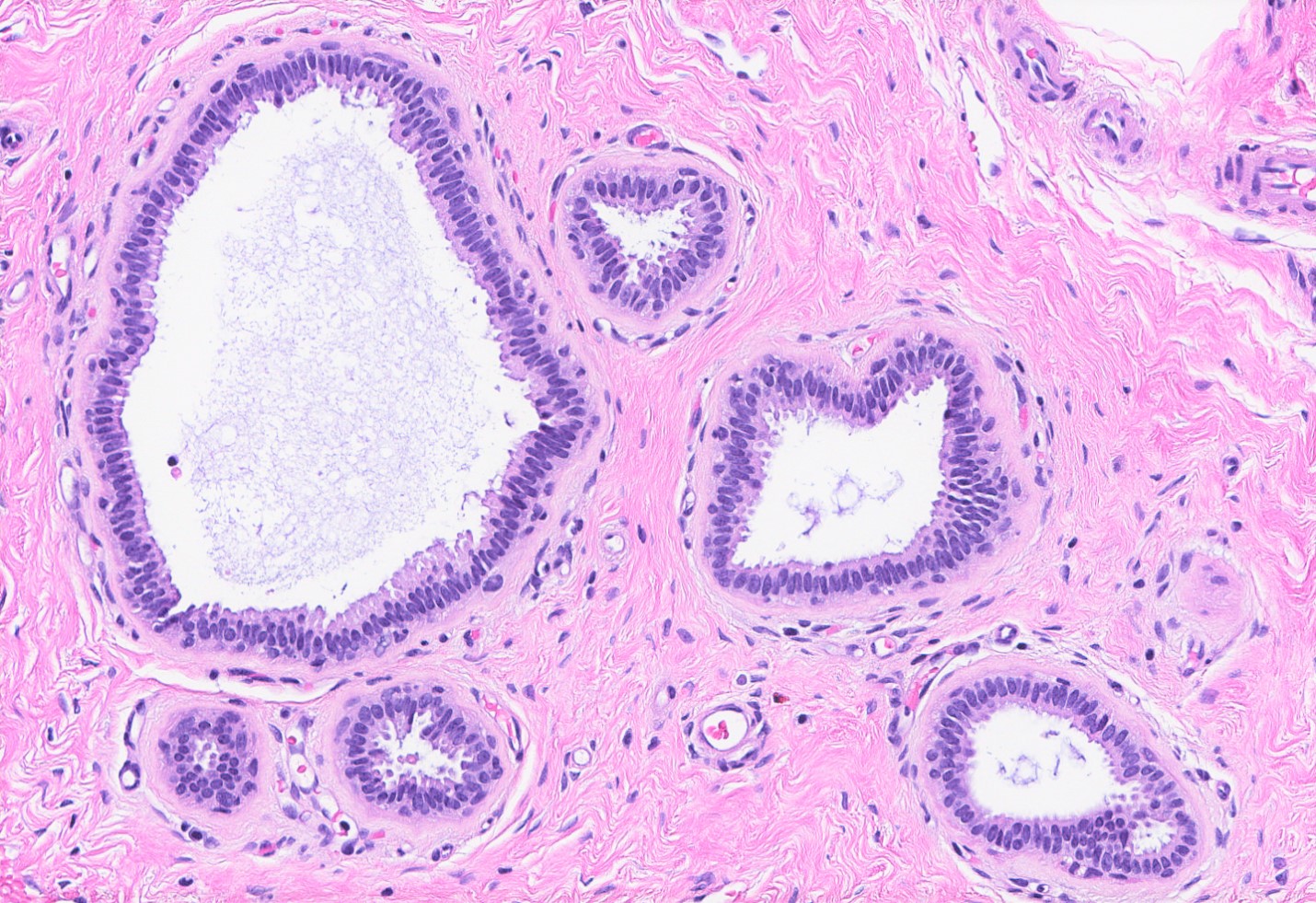
Cysts, columnar cell change
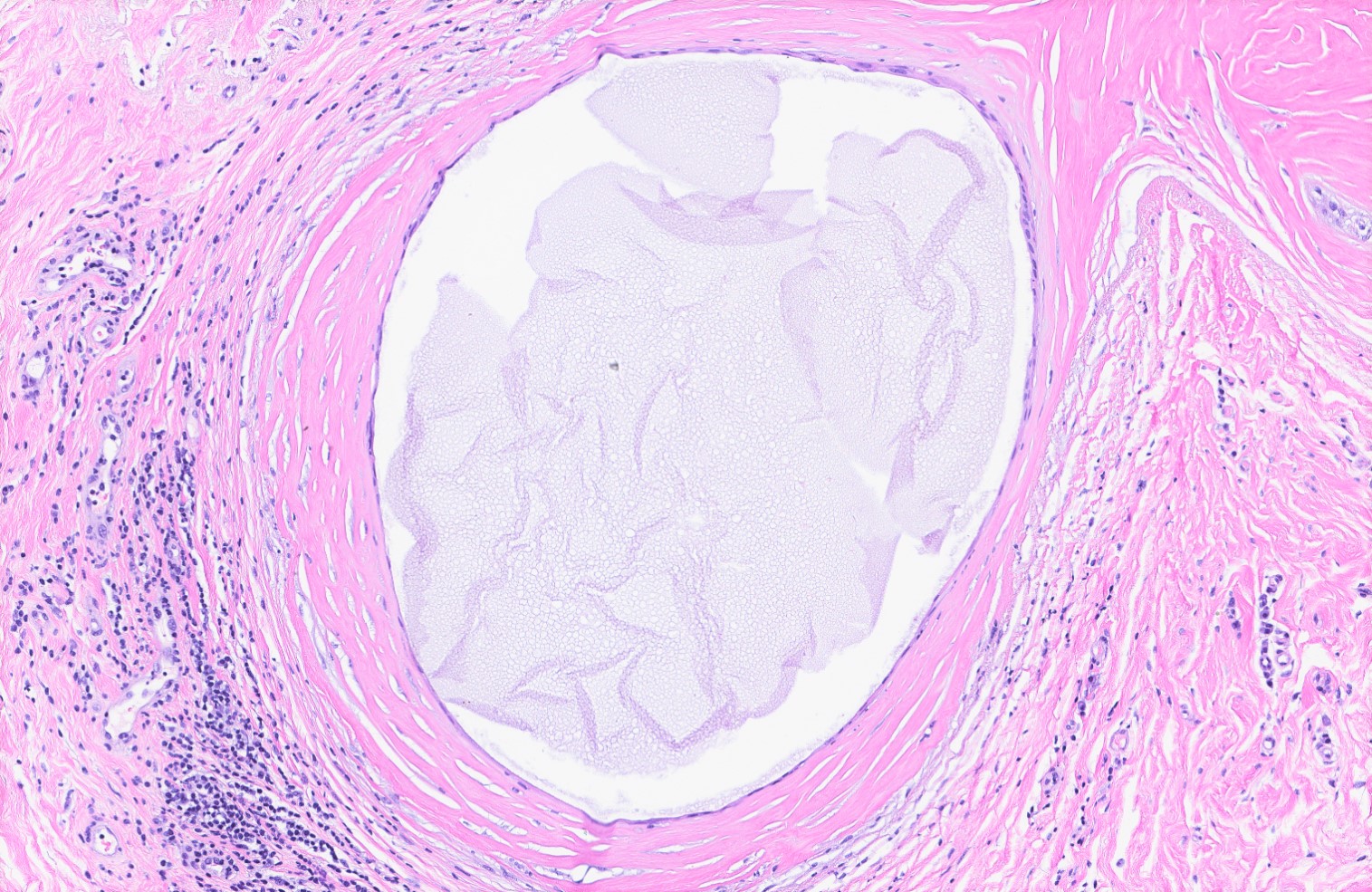
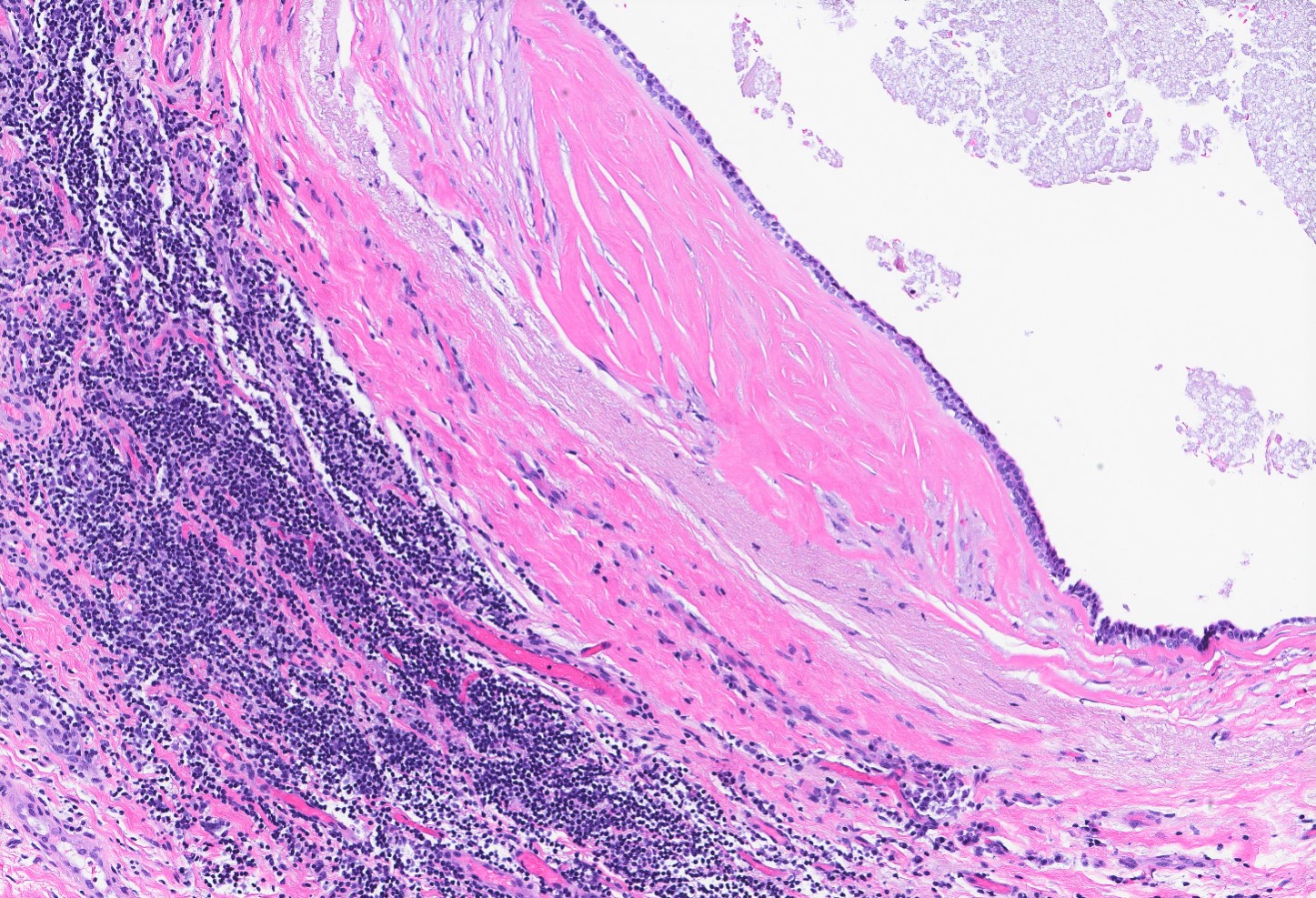
Surrounding fibrosis and inflammation
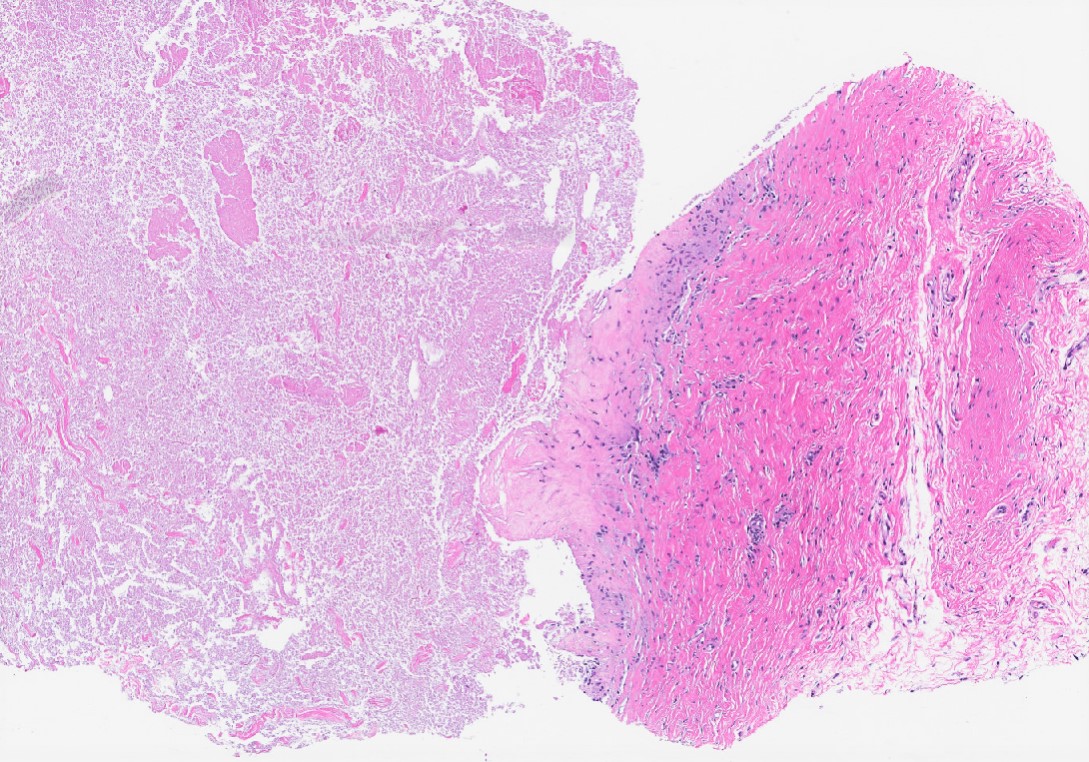
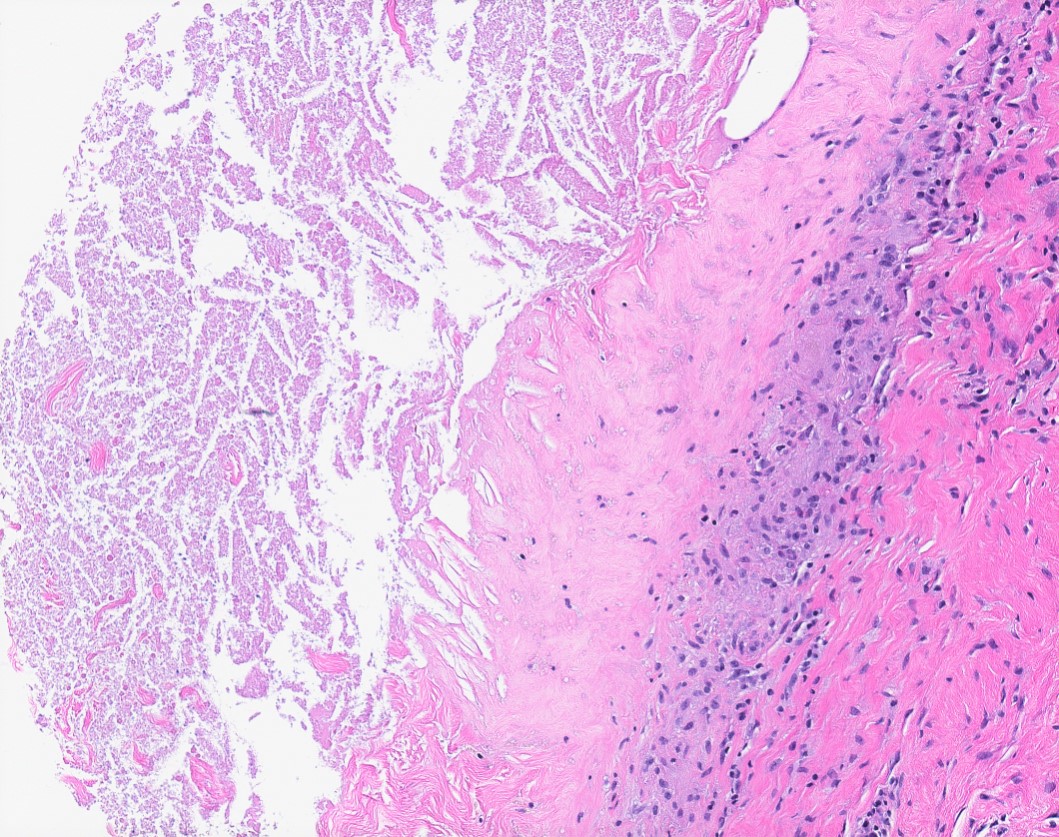
Ruptured cyst

Cluster of microcysts
Cytology description
- Hypocellular aspirate, macrophages with other inflammatory cells, with or without few clusters of benign ductal epithelial and myoepithelial cells (Patholog Res Int 2011;2011:547580)
- Prior rupture of the cyst may result in turbid or milky fluid, degenerated cells and debris in an abundant background of inflammatory cells (Patholog Res Int 2011;2011:547580)
Cytology images
Contributed by Kristen E. Muller, D.O.
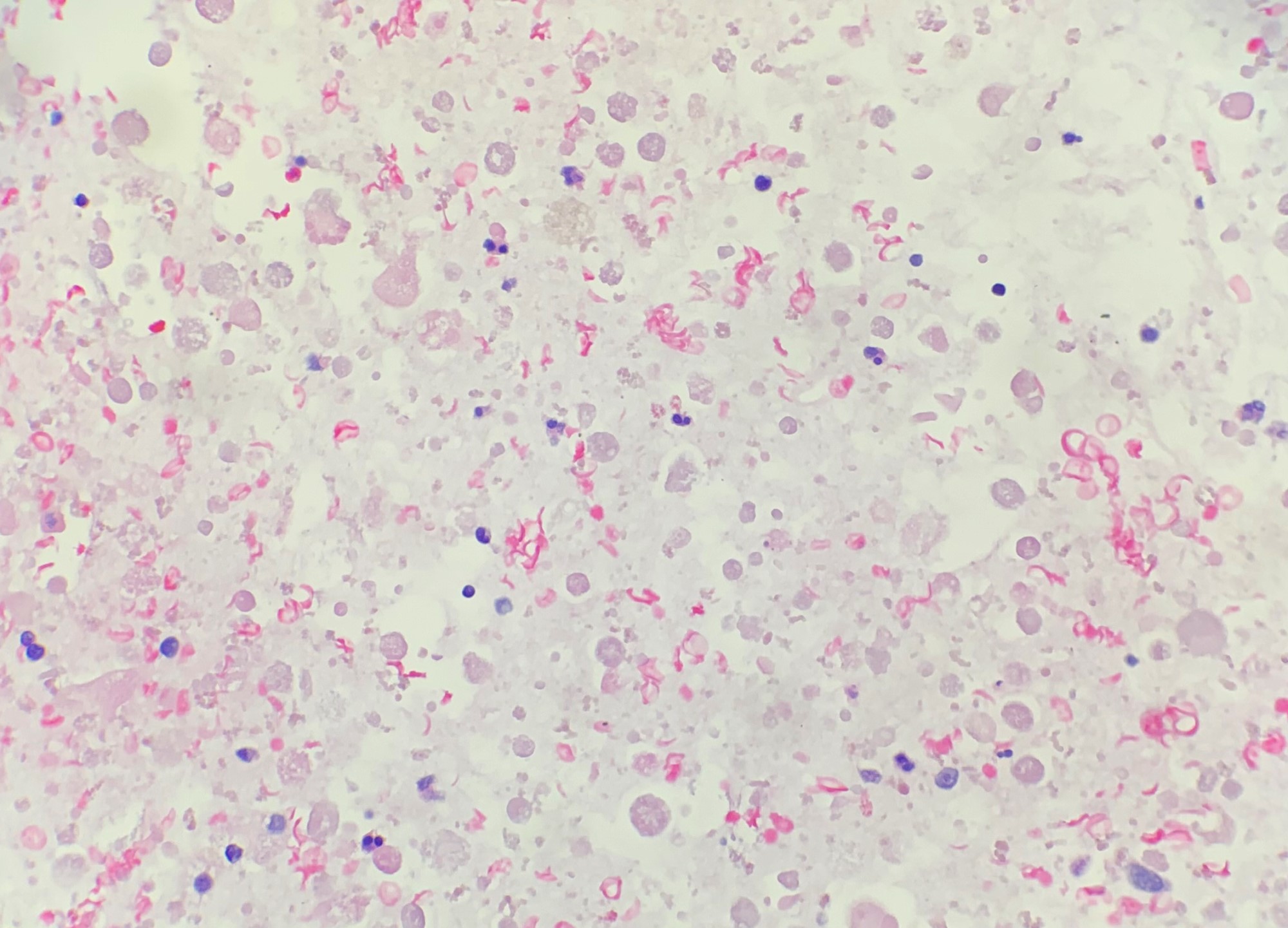
Predominantly debris, cell block
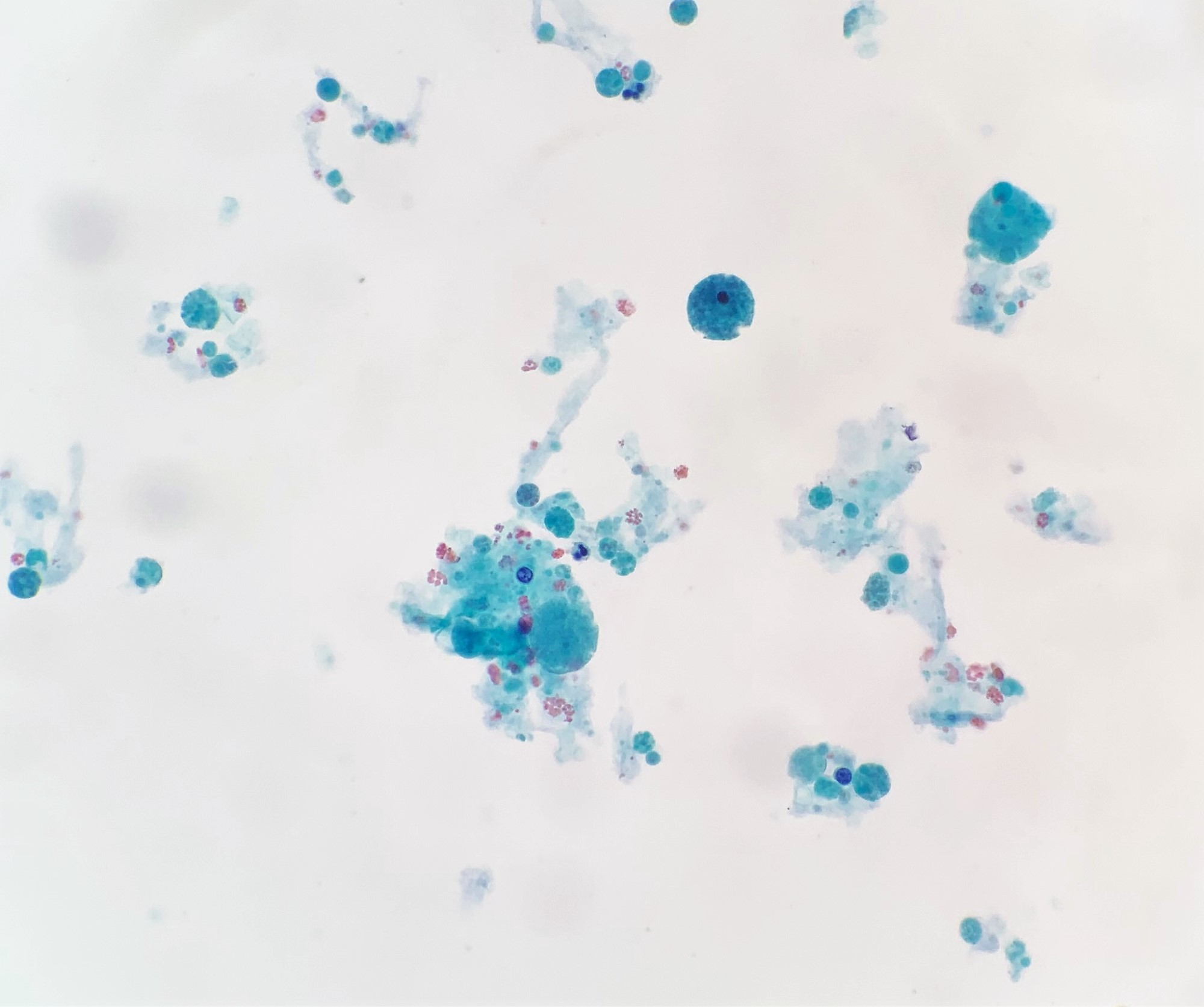
Hypocellular specimen, LBP
Sample pathology report
- Left breast, 2 o’clock, 1 cm from nipple, core needle biopsy:
- Benign breast tissue with fragments of cyst wall with surrounding fibrosis and chronic inflammation
Differential diagnosis
- Flat epithelial atypia:
- Low grade monomorphic cytologic atypia, cells lack polarity, apical tufting, increased N/C ratios, round nuclei with variably prominent nucleoli
- Cystic hypersecretory hyperplasia:
- Colloid-like secretions
- Duct ectasia:
- Elastic tissue in wall, macrophages in lumen and epithelium
- Ductal carcinoma in situ, clinging type:
- Typically high grade cytologic atypia, central necrosis
- Mucocele-like lesion:
- Cysts and dilated ducts are filled with mucin frequently with extravasated acellular mucin in periductal stroma
- May be associated with ADH
- Juvenile papillomatosis:
- Microcysts may be present, however, in addition, there is florid epithelial hyperplasia and papillomatosis
Board review style question #1
The findings pictured are from a 38 year old woman with a cystic breast mass. What is the diagnosis?
- Atypical ductal hyperplasia
- Cysts
- Duct ectasia
- Flat epithelial atypia
- Lymphocytic mastitis
Board review style answer #1
Board review style question #2
The findings pictured are from a 67 year old woman with a palpable breast mass. Ultrasound showed a complex cystic and solid mass. What is the diagnosis?
- Duct ectasia
- Ductal carcinoma in situ
- Granulomatous mastitis
- Ruptured cyst wall
Board review style answer #2
