

Breast
Other nonneoplastic
Cystic hypersecretory hyperplasia
Board of reviewers: Gary M. Tse, M.B.B.S.
Deputy Editor-in-Chief: Gary Tozbikian, M.D.


Last author update: 11 November 2024
Last staff update: 18 December 2024
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search:: Cystic hypersecretory hyperplasia


Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Prognostic factors | Case reports | Treatment | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Positive stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1Cite this page: Jones VM, Muller KE. Cystic hypersecretory hyperplasia. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/breastcystichypersecretoryhyperplasia.html. Accessed January 5th, 2025.
Definition / general
- Type of breast lesion characterized by cystically dilated ducts lined by bland cuboidal or columnar epithelium, filled with homogenous eosinophilic secretions that resemble thyroid colloid
Essential features
- Cystically dilated ducts lined by bland epithelium filled with homogenous eosinophilic secretions that resemble thyroid colloid
- Absence of cytologic and architectural atypia
- May coexist with a spectrum of cystic hypersecretory lesions, including cystic hypersecretory carcinoma (CHC)
- Background breast tissue may show lactational / pregnancy-like changes
- Excisional biopsy is recommended
Terminology
- Cystic hypersecretory hyperplasia (CHH)
- Cystic hypersecretory change
ICD coding
- ICD-11: GB20.Z - benign breast disease, unspecified
Epidemiology
- F > M
- Rare
- Age at diagnosis: 38 - 62 years (mean: 52 years) (Cancer 1988;61:1611)
- May coexist with pregnancy-like (pseudolactational) hyperplasia (PLH) observed in nonlactating, nonpregnant women (Am J Surg Pathol 2000;24:1670, Am J Surg Pathol 2004;28:789)
Sites
- Can be unifocal or multifocal and often arises in a spectrum of other cystic hypersecretory lesions
Pathophysiology
- Unknown
- Often arises in a spectrum of hypersecretory lesions, including CHC; in some cases, there may be background lactational-like / pregnancy-like change as well
Etiology
- Unknown
Clinical features
- Patients may present with palpable mass or nipple discharge (Am J Surg Pathol 2000;24:1670)
- Patients are usually otherwise asymptomatic (Arch Pathol Lab Med 2003;127:e389)
Diagnosis
- Fine needle aspiration, core biopsy, excisional biopsy (recommended)
Radiology description
- Luminal calcifications are not a prominent feature of CHH; however, calcifications are common in associated pregnancy-like hyperplasia (Am J Surg Pathol 2004;28:789)
- Magnetic resonance imaging (MRI) may show mass or nonmass findings with foci of simple enhancement (Arch Pathol Lab Med 2003;127:e389)
- Mammography may show asymmetrical density or a homogeneous mass (Cytopathology 2002;13:175, Arch Pathol Lab Med 2003;127:e389)
Prognostic factors
- Natural history is unknown due to rarity
- Considered a benign lesion
- CHH is on the spectrum of cystic hypersecretory lesions and may be a precursor to CHC (Am J Surg Pathol 2014;38:45)
- Evidence of transformation areas from CHH to CHH with atypia to CHC have been reported (Cancer 1988;61:1611)
- 70 published cases of CHC to date showed that all cases had focal CHH or CHH with atypia (South Asian J Cancer 2023;12:297)
- All 10 cases of CHC were present in a background of CHH or atypical CHH (Am J Surg Pathol 2014;38:45)
Case reports
- 45 year old woman with invasive CHC and a background of CHH (J Korean Med Sci 2004;19:149)
- 48 year old woman with CHH with cytologic atypia (Arch Pathol Lab Med 2003;127:e389)
- 60 year old woman with CHC and a background of CHH (South Asian J Cancer 2023;12:297)
Treatment
- If CHH is suspected on needle core biopsy, excisional biopsy is recommended to exclude CHH with atypia, CHC and invasive carcinoma (Autops Case Rep 2022;12:e2021375, Arch Pathol Lab Med 2003;127:e389, Am J Surg Pathol 2004;28:789)
- Excisional biopsy is generally curative for CHH alone (Arch Pathol Lab Med 2003;127:e389)
Gross description
- CHH lesions are at least 1 - 5 cm in diameter (compared to CHC, reported up to 10 cm) (Cancer 1988;61:1611)
- Individual ducts and cysts reported from 0.1 to 1.3 cm (Cancer 1988;61:1611)
- Cut surface with numerous cystic spaces filled with gelatinous, viscid, mucinous or colloid-like material (Cytopathology 2002;13:175, Cancer 1988;61:1611)
- Usually grossly indistinguishable from surrounding breast tissue (Arch Pathol Lab Med 2003;127:e389)
- Unlike juvenile papillomatosis, hypersecretory lesions are not circumscribed and do not contain yellow chalky areas (Cancer 1988;61:1611)
- Extensive sampling is necessary to thoroughly differentiate CHH with and without atypia, ductal carcinoma in situ (DCIS) of cystic hypersecretory type and invasive components
Microscopic (histologic) description
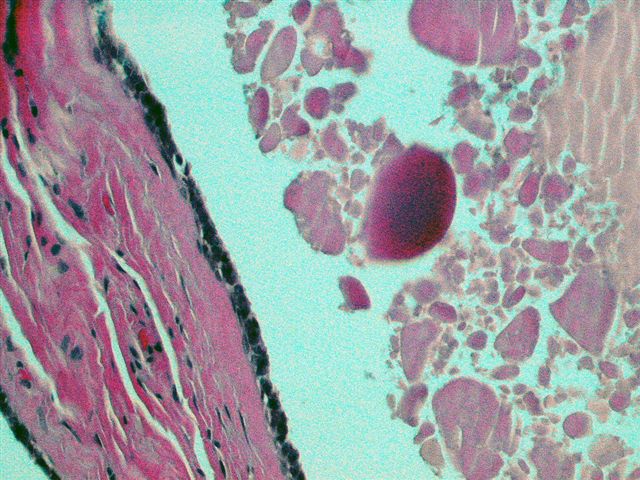
- Dilated cysts with intraluminal homogeneous thyroid-like material consisting of acellular, eosinophilic, colloid-like secretions (Arch Pathol Lab Med 2003;127:e389, Am J Surg Pathol 2000;24:1670)
- Cysts are lined by a single orderly layer of flat, cuboidal or columnar epithelium
- Epithelial lining cells are monotonous with low N:C ratios, bland nuclei, eosinophilic cytoplasm and focal secretory changes
- Frequent, artifactual shrinking / retraction of cyst contents away from the lining epithelium as well as the presence of parallel cracks in the secretion (Cancer 1988;61:1611)
- Occasional spillage of cyst contents into adjacent stroma through disrupted cyst lining, creating inflammatory milieu of lymphocytes, foamy histiocytes and focal hemorrhage (Cancer 1988;61:1611, Cytopathology 2002;13:175)
- CHH frequently merges with pregnancy-like (pseudolactational) hyperplasia (Am J Surg Pathol 2004;28:789)
- CHH / PLH cases tend to contain DCIS, usually micropapillary or cystic hypersecretory types (Am J Surg Pathol 2004;28:789)
- CHH with atypia (atypical CHH)
- Mild to moderate degree of cytologic or architectural atypia without fully attaining the level of DCIS (Am J Surg Pathol 2014;38:45)
- Nuclear pleomorphism, hyperchromasia, epithelial crowding with loss of polarity, increased N:C ratios, enlarged nucleoli, rare mitotic figures (Am J Surg Pathol 2000;24:1670, Cancer 1988;61:1611, Cytopathology 2002;13:175)
- Architectural features of atypical ductal hyperplasia, often micropapillary growth or bridge formation (Am J Surg Pathol 2014;38:45, Arch Pathol Lab Med 2009;133:722)
- Mild to moderate degree of cytologic or architectural atypia without fully attaining the level of DCIS (Am J Surg Pathol 2014;38:45)
Microscopic (histologic) images
Contributed by Victoria M. Jones, M.D., Kristen E. Muller, D.O., AFIP and Lisa Cerilli, M.D. (Case #35)

Multiple dilated cysts

Pregnancy-like changes

Colloid-like secretions

Bland, simple cuboidal epithelial lining

Atypia

Atypia


CHC (DCIS)

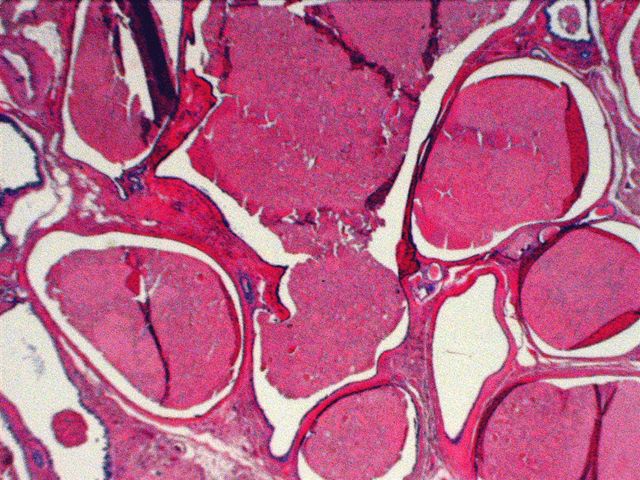
Cysts lined by flat, cuboidal epithelium
Cysts lined by flat, cuboidal epithelium


Focal atypical epithelium
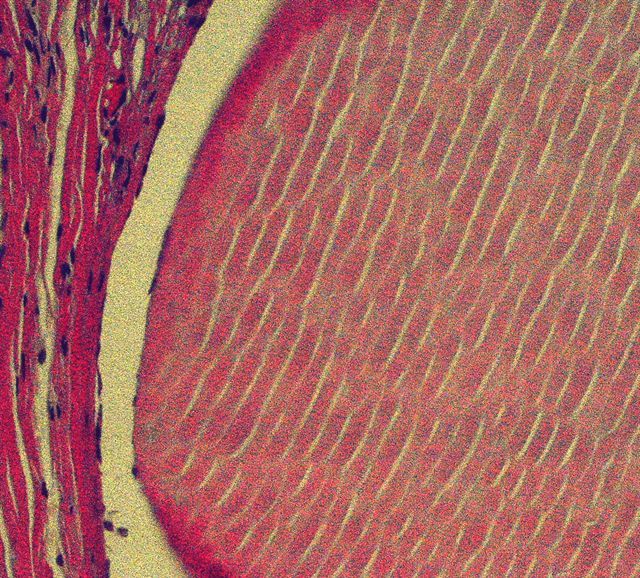
Intraluminal secretions
Cytology description
- Large clumped amounts of homogenous, eosinophilic, acellular secretions and minimal stroma (Cytopathology 2002;13:175)
- Benign and bland appearing epithelial cells in cohesive sheets, devoid of pleomorphism (Cytopathology 2002;13:175)
- CHH with atypia shows cellular and nuclear pleomorphism with some loss of cohesion (Cytopathology 2002;13:175)
- Cystic hypersecretory lesions can be diagnosed in a fine needle aspiration (FNA) specimen if the characteristic secretion is recognized (Acta Cytol 1997;41:892, Acta Cytol 1999;43:273, Arch Pathol Lab Med 1988;112:560)
- Cystic hypersecretory lesions with DCIS usually produce papillary clusters of tumor cells in an FNA specimen (Hoda: Rosen's Breast Pathology, 4th Edition, 2014)
Positive stains
- ER (Autops Case Rep 2022;12:e2021375, Am J Surg Pathol 2014;38:45)
- Secretions are PAS positive and resistant to diastase (Cytopathology 2002;13:175)
Molecular / cytogenetics description
- Unknown
Sample pathology report
- Breast, left, core biopsy:
- Cystic hypersecretory hyperplasia (see comment)
- Comment: The cores show benign breast tissue with scattered cystically dilated ducts lined by bland, cuboidal to columnar cells with abundant intraluminal eosinophilic secretions. The epithelial lining lacks evidence of cytologic atypia (epithelial crowding, hyperchromasia and conspicuous mitotic figures). The histologic findings are compatible with cystic hypersecretory hyperplasia (CHH). CHH often arises in a spectrum of hypersecretory lesions including cystic hypersecretory carcinoma. A conservative excisional biopsy is recommended to exclude a malignant process.
Differential diagnosis
- Cystic hypersecretory carcinoma (cystic hypersecretory ductal carcinoma in situ):
- Nuclear atypia, increased architectural complexity (micropapillary), mitoses, necrosis
- Microcysts:
- Lack thyroid-like colloid secretions
- Pseudolactational change:
- Not typically cystic
- Foamy, vacuolated cytoplasm with hobnailing
- Lacks thyroid-like colloid secretions
- Secretory carcinoma:
- Juvenile papillomatosis:
- Both can be mass forming with grossly visible cysts
- Lacks thyroid-like colloid secretions
- Often shows florid epithelial hyperplasia and papillomatosis
Board review style question #1
Board review style answer #1
B. Excisional biopsy. This lesion shows the characteristic features of cystic hypersecretory hyperplasia (CHH). When CHH is found on a core biopsy, excision is recommended to exclude malignancy since CHH may be associated with cystic hypersecretory carcinoma. Answer C is incorrect because, although benign, CHH can be associated with malignancy; therefore, excisional biopsy is recommended over follow up imaging. Answer D is incorrect because if malignancy is excluded upon excision, CHH is considered benign and no further treatment is necessary. Answer A is incorrect because CHH is a benign lesion and does not require chemotherapy.
Comment Here
Reference: Cystic hypersecretory hyperplasia
Comment Here
Reference: Cystic hypersecretory hyperplasia

