
Breast
Other benign tumors
Atypical vascular proliferation
Authors: Indu Agarwal, M.D., Luis Blanco, Jr., M.D.
Editorial Board Member: Julie M. Jorns, M.D.
Deputy Editor-in-Chief: Gary Tozbikian, M.D.


Last author update: 9 February 2023
Last staff update: 9 February 2023
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Atypical vascular proliferation


Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1Cite this page: Agarwal I, Blanco L. Atypical vascular proliferation. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/breastatypicalvascular.html. Accessed April 1st, 2025.
Definition / general
- Atypical vascular proliferations on irradiated skin, often small and multiple
Essential features
- Superficial dermal based growth of narrow vascular spaces
- Develops after external radiation for breast carcinoma
- Typically involves the skin overlying breast
- 2 subtypes: lymphatic type and vascular type
- Differentiated from angiosarcoma by lack of multilayering, mitosis, marked cytologic atypia, blood lakes and absence of extension into subcutaneous tissue
Terminology
- Atypical vascular lesion term coined by Fineberg and Rosen in 1994 (Am J Clin Pathol 1994;102:757)
- Acceptable terminology: atypical vascular proliferation
Epidemiology
- Wide age range has been reported but is most common in late sixth to early seventh decade (Breast Cancer Res Treat 2014;146:347, Am J Surg Pathol 2005;29:983)
- Develops 3 to 6 years after radiation treatment (Semin Diagn Pathol 2017;34:410)
Sites
- Skin of breast or anterior chest wall exposed to previous radiation
Pathophysiology
- Secondary to irradiation but precise pathogenesis is unknown
Etiology
- Directly associated with radiation treatment
- Median total administered dose: 50 Gy (Am J Surg Pathol 2005;29:983)
Clinical features
- Multiple, small papules or vesicles and erythematous plaques (Am J Surg Pathol 2002;26:328)
Diagnosis
- Requires correlation of clinical history and physical examination with microscopic features
- Complete excision of the lesion is required for definitive diagnosis
Prognostic factors
- Mostly follows a benign course (Am J Surg Pathol 2005;29:983)
- Local recurrences and development of further similar lesions may occur in the radiation field
- Progression to angiosarcoma is rare but reported (Am J Surg Pathol 2005;29:983)
Case reports
- 41 and 61 year old women with small vascular lesions of the breast diagnosed by MRI guided vacuum assisted biopsy (Radiol Case Rep 2022;17:2492)
- 43 year old woman presented with 29 atypical vascular lesions following breast conserving surgery and radiation (Cutis 2019;103:E22)
- 49 year old woman presented with postradiation atypical vascular proliferation mimicking angiosarcoma 8 months following breast conserving therapy for breast carcinoma (J Clin Aesthet Dermatol 2011;4:47)
Treatment
- Complete excision with uninvolved surgical margins and follow up (Am J Surg Pathol 2005;29:983)
Clinical images
Contributed by Anna Purdy, M.S.N.

Upper outer quadrant erythema

Axillary papules
Images hosted on other servers:

Postmastectomy


Left breast is erythematous with sclerotic tissue changes

Papules and nodules around the mastectomy scar
Gross description
- ≥ 1 circumscribed papules, bluish purple nodules, small vesicles or erythematous plaques, median of 0.5 cm
- Tends to be well demarcated, symmetric and wedge shaped (Semin Diagn Pathol 2017;34:410)
Microscopic (histologic) description
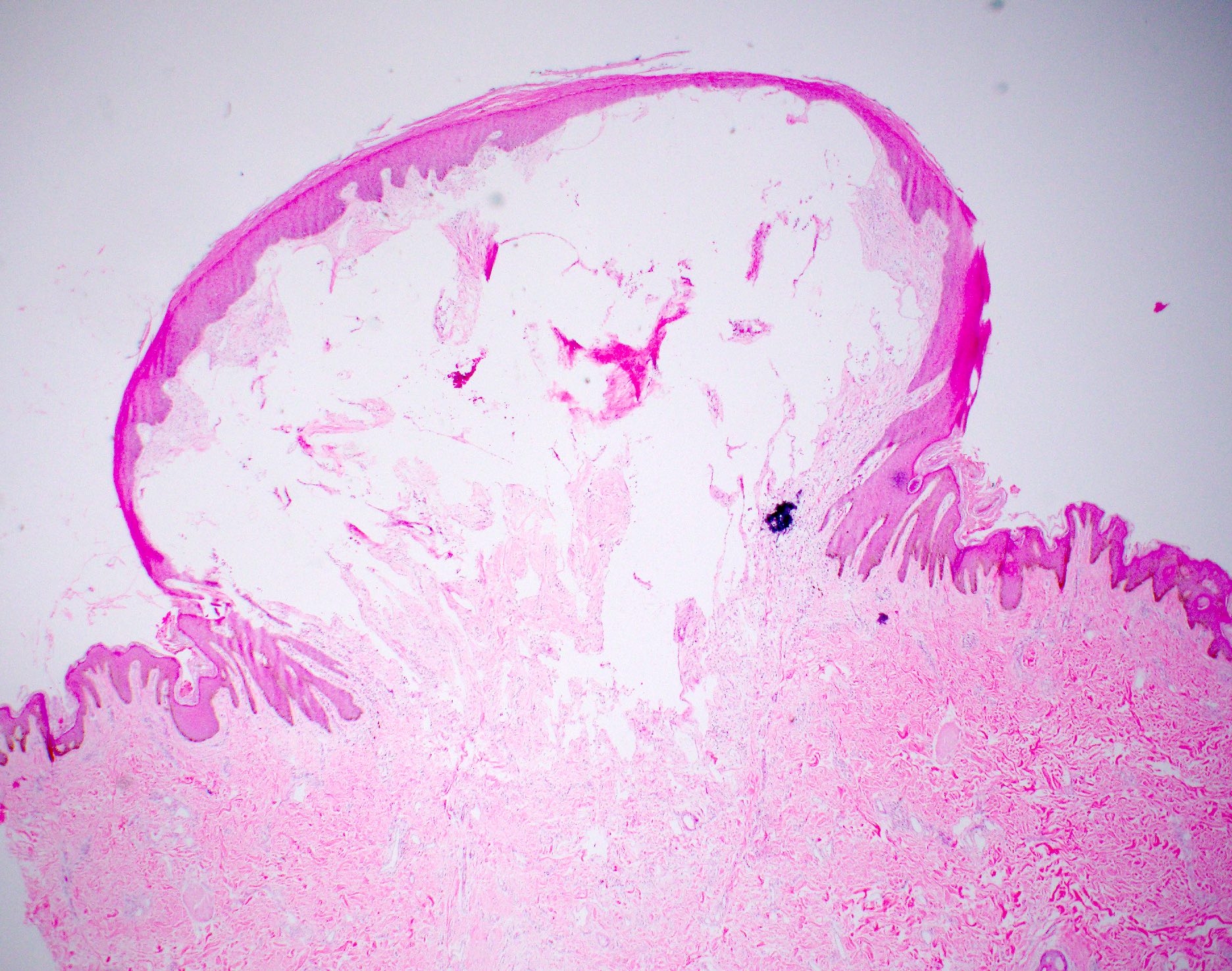
- Relatively well circumscribed lesion with a somewhat wedge shaped outline, limited to the dermis and not extending into subcutis
- 2 histologic subtypes with overlapping histologic features (Am J Surg Pathol 2008;32:943):
- Lymphatic subtype:
- More common subtype
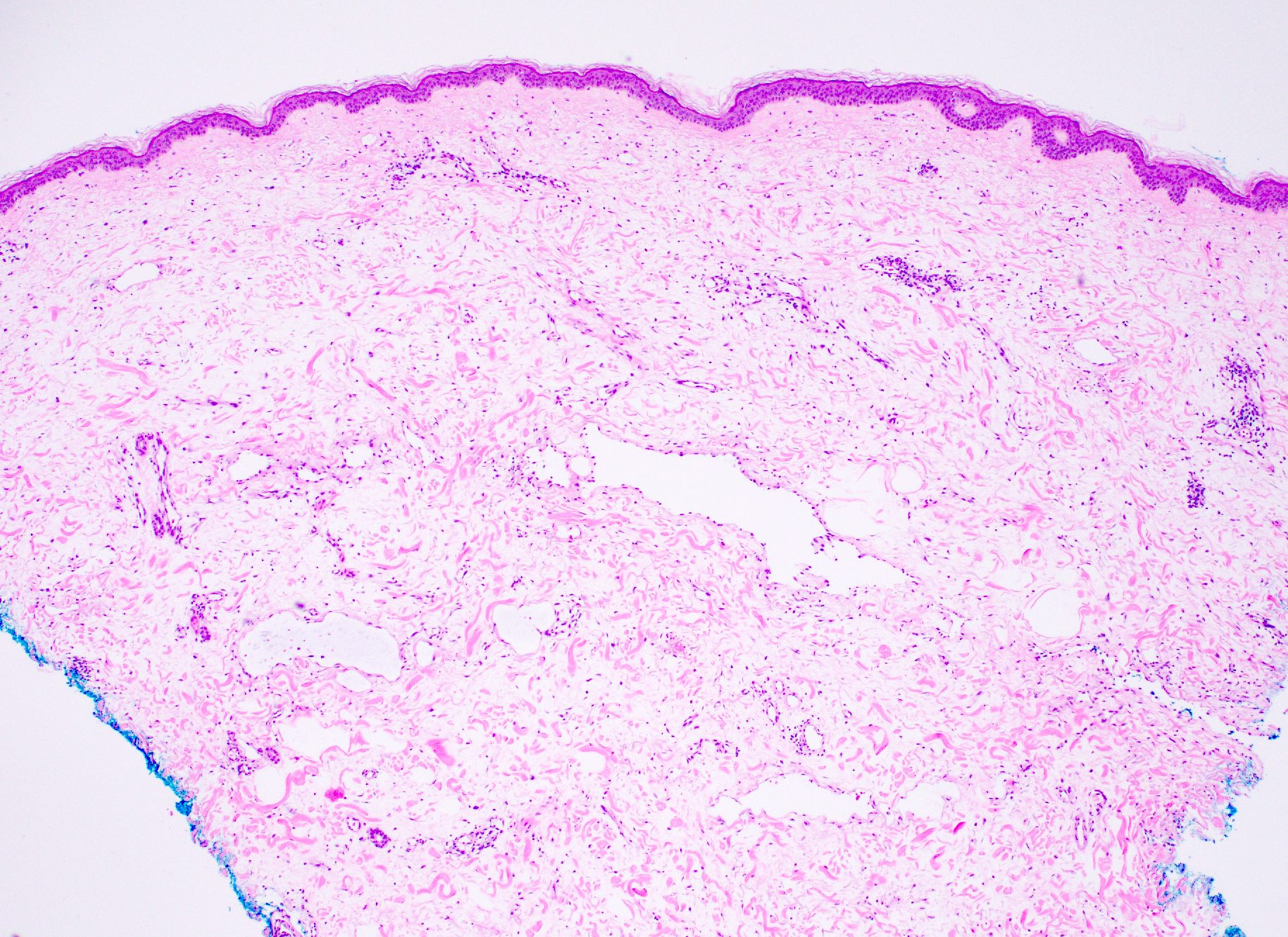
- Irregularly shaped, thin walled vascular channels with a branching and anastomosing growth
- Lymphatic valve-like structures may be evident
- Vessels lined by single layer of endothelial cells without atypia
- Hobnailing and nuclear hyperchromasia may be seen
- Vascular subtype:
- Thin capillary channels lined by flattened to hobnail endothelium, lacking lobular growth pattern
- Lymphatic subtype:
- Individual lesions may show composite features of both subtypes
Microscopic (histologic) images
Contributed by Indu Agarwal, M.D., Sharlene See, M.D. and Julie M. Jorns, M.D.
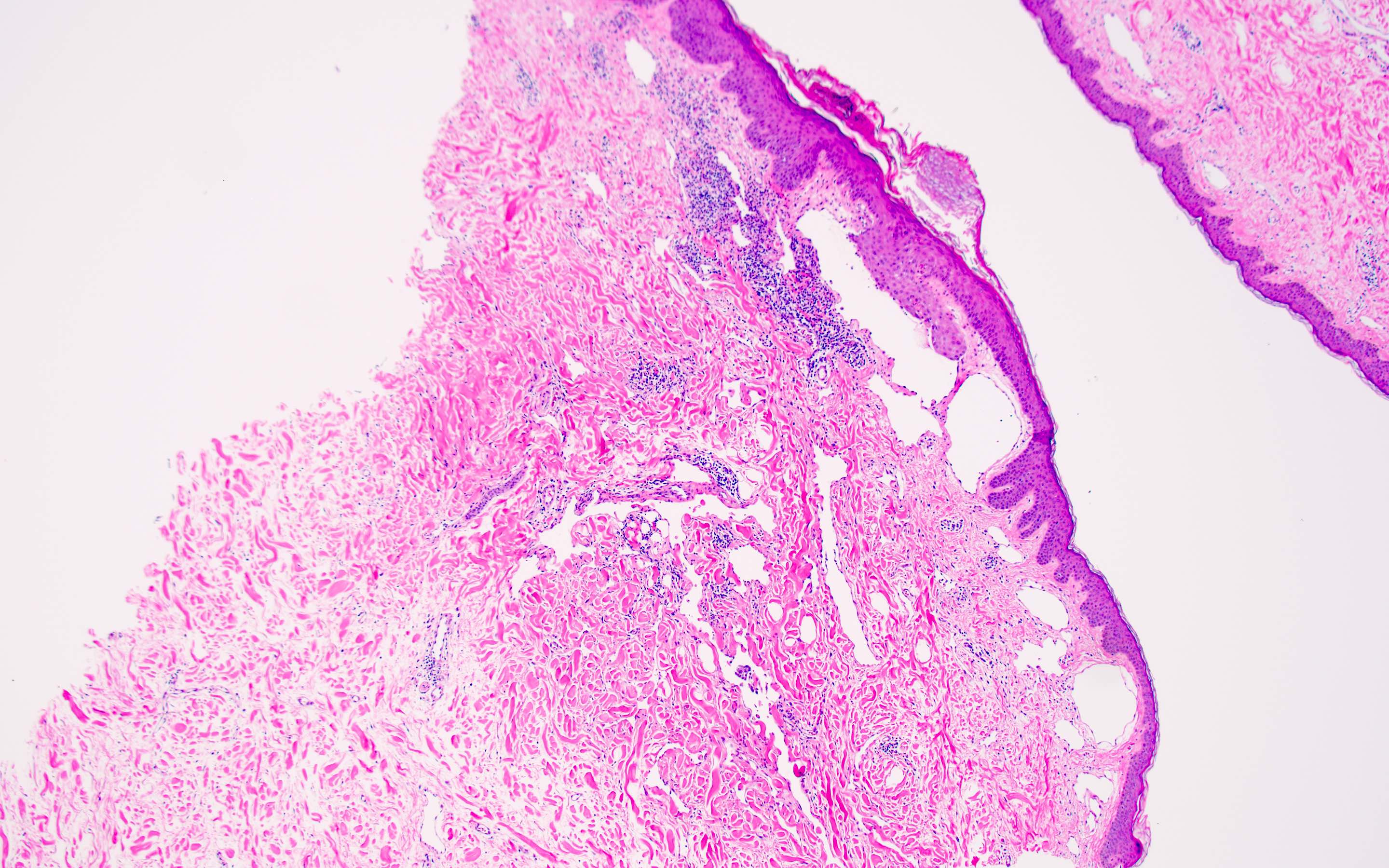
Wedge shaped outline
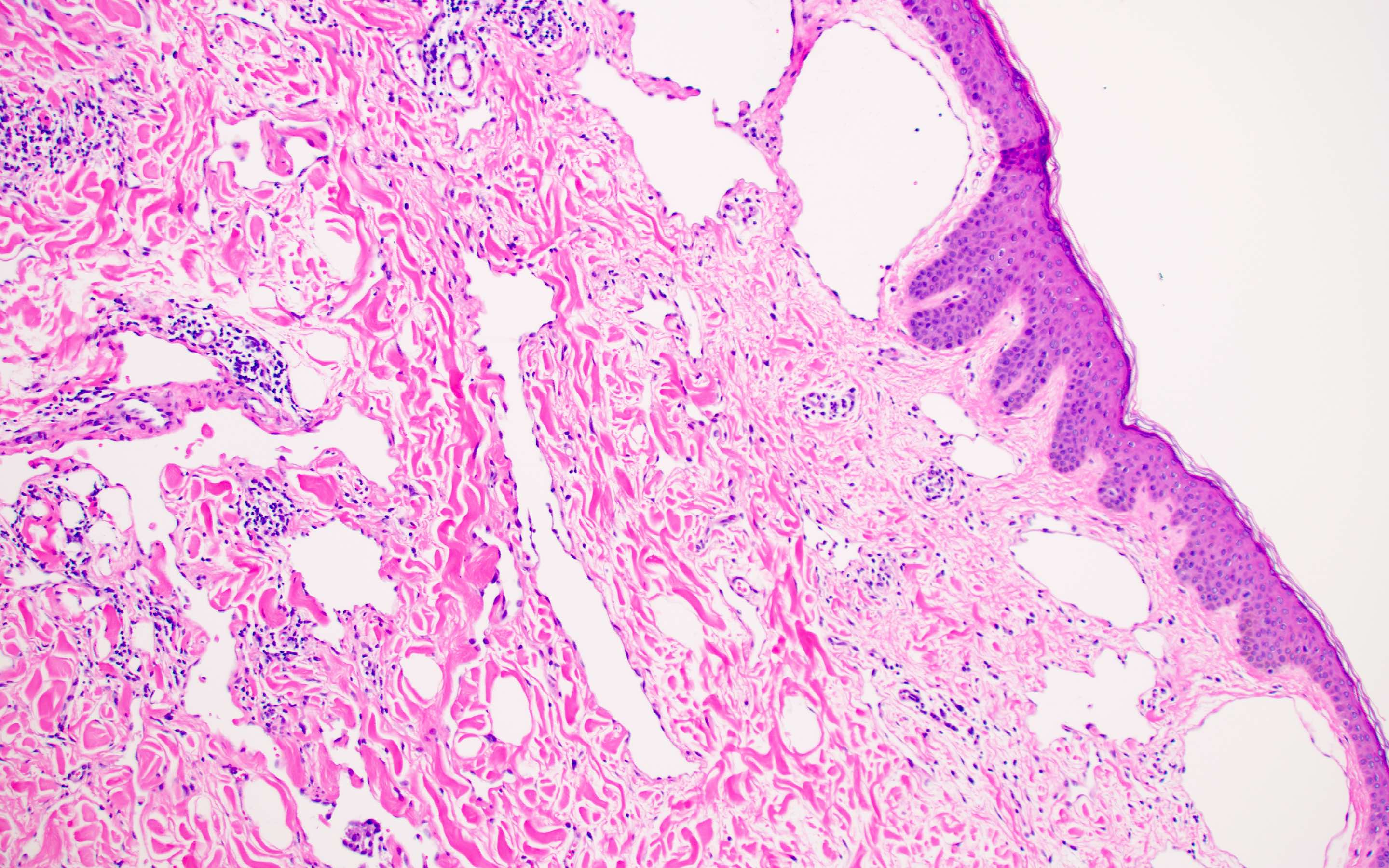
Flat to plump endothelial cells
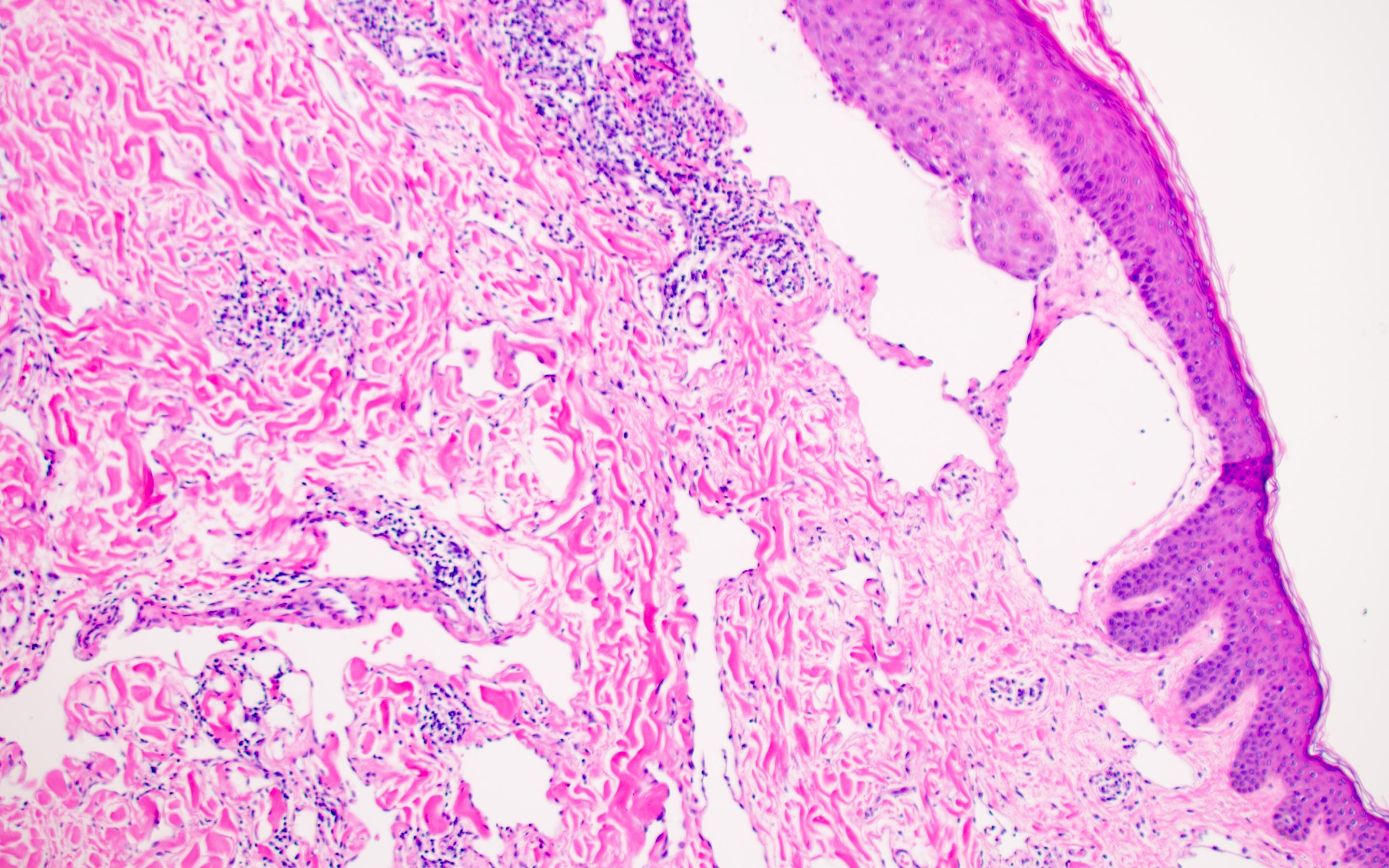
Vascular channels
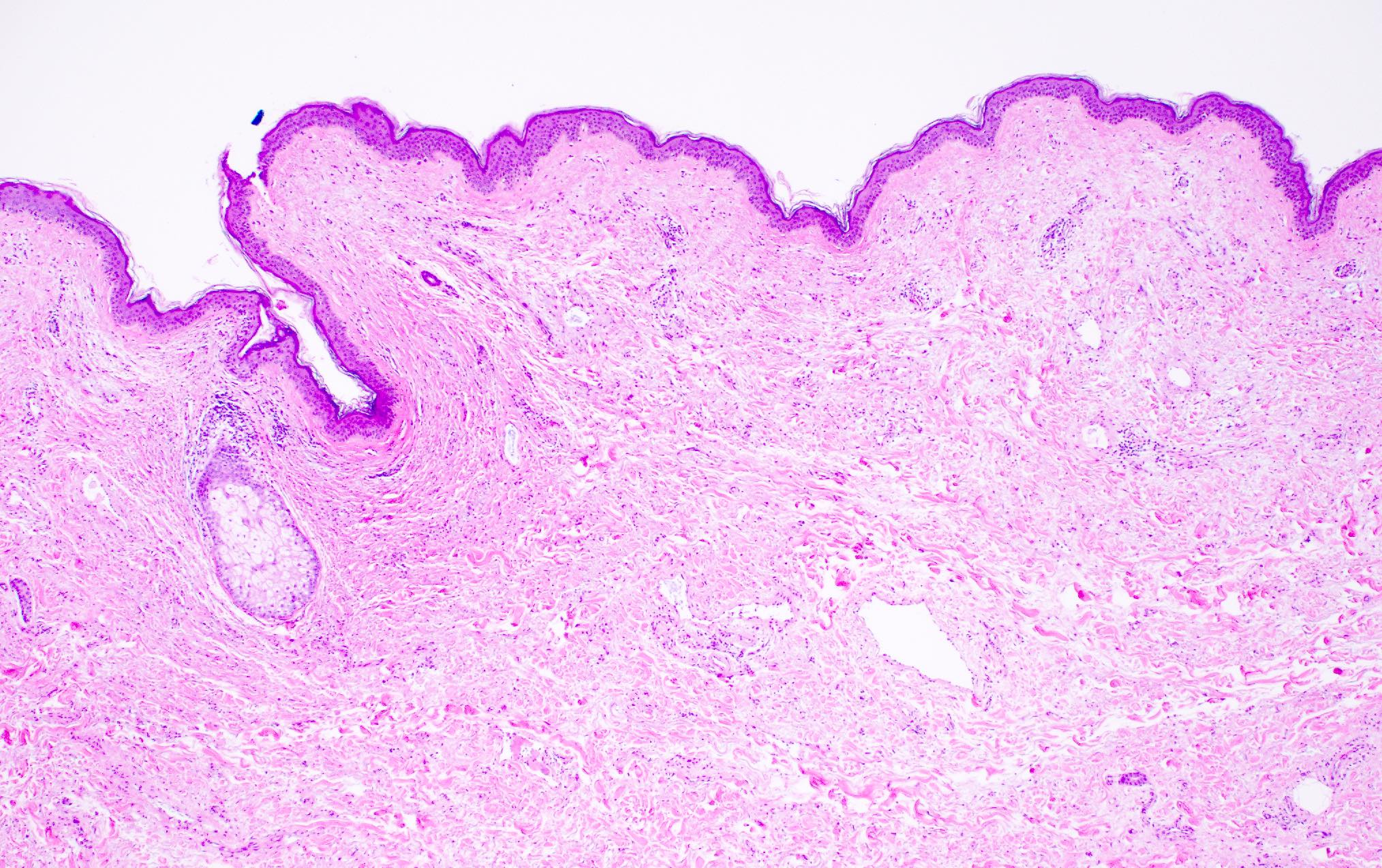
Excision specimen
Papule
Skin punch biopsy
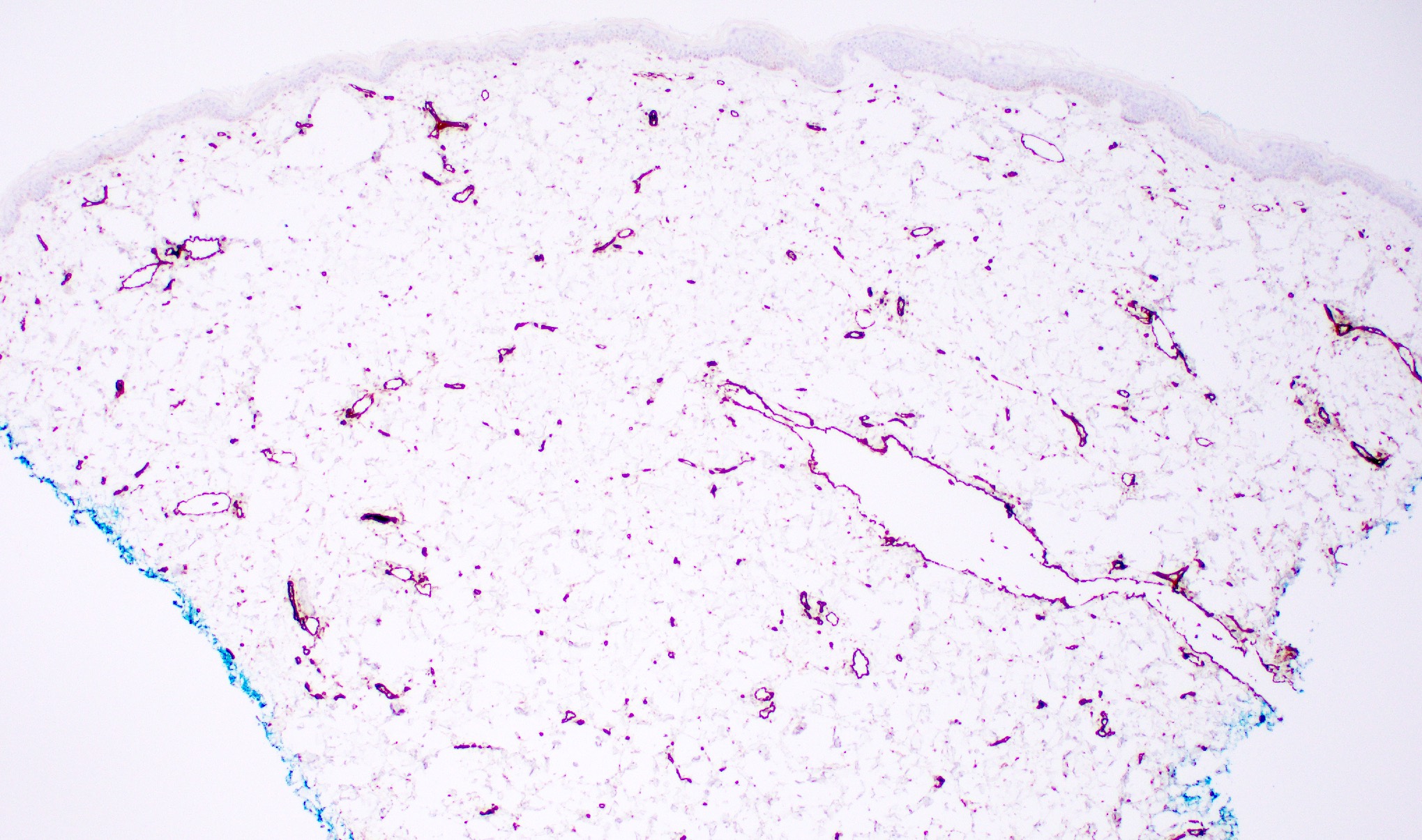
Skin punch biopsy (CD31)
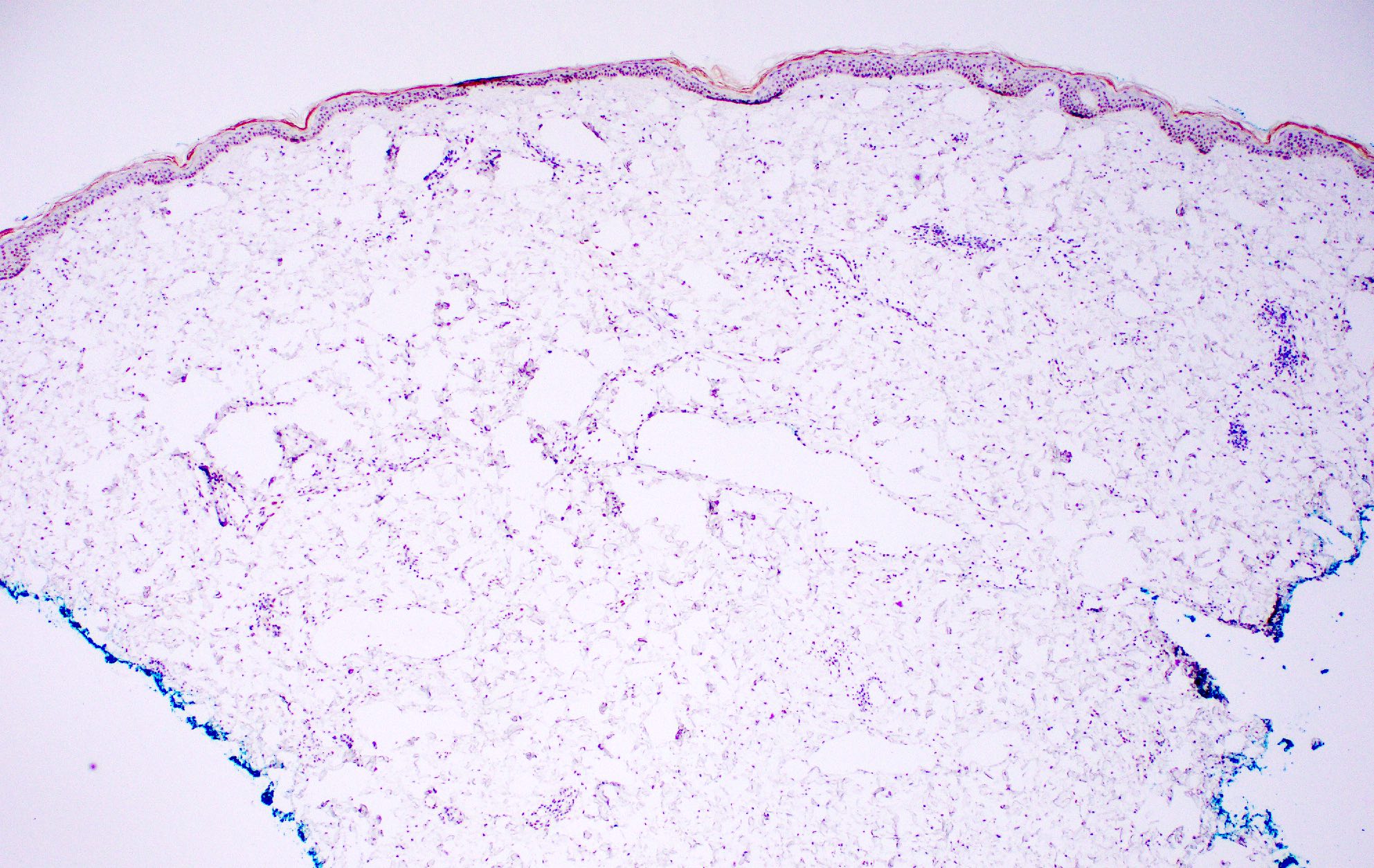
Skin punch biopsy (c-MYC)
Positive stains
- CD31, D2-40 (lymphatic type) (Breast Cancer Res Treat 2014;146:347)
- Variable CD34
Negative stains
Molecular / cytogenetics description
- Unknown
Sample pathology report
- Left breast skin, punch biopsy:
- Atypical vascular lesion (see comment)
- Comment: The lesion is comprised of a vascular proliferation dissecting the collagen in the superficial dermis. There is no significant nuclear pleomorphism or mitotic activity. An immunostain performed for c-MYC is negative in the lesion. Morphologic and immunohistochemical findings support the diagnosis.
Differential diagnosis
- Angiosarcoma, well differentiated:
- Features of angiosarcoma which are lacking in atypical vascular lesions:
- Large (median size is 7.5 cm) infiltrative lesion with destruction of adnexa and extension into subcutaneous tissues, multilayering of endothelial cells, prominent nucleoli, mitoses, blood lakes and solid areas
- Unlike secondary angiosarcomas, atypical vascular lesions lack MYC amplification (by FISH) and MYC overexpression by immunohistochemistry
- However, angiosarcoma may be part of morphologic continuum with atypical vascular lesions and may need additional biopsies to distinguish these entities (J Am Acad Dermatol 2007;57:126)
- Features of angiosarcoma which are lacking in atypical vascular lesions:
- Hemangioma of skin:
- No history of radiation
- Lesions consist of dilated blood vessels in skin, filled with blood
- Vessels have rounded contours and are nonanastomosing
- Benign lymphangioendothelioma (Am J Surg Pathol 2000;24:1047):
- Rare lesion with no history of radiation
- Head and neck are more common sites, followed by limbs and trunk
- Skin lesions may be macular or papular and pigmented
- Anastomosing dilated vessels lined by flattened endothelium are present in superficial dermis; spaces may be empty or contain blood
- Cytologic atypia and mitoses are absent
Additional references
Board review style question #1

A brownish papular lesion of skin on the breast is excised. Histopathologic examination shows that it is comprised of a wedge shaped, relatively well circumscribed vascular proliferation, dissecting the collagen in the superficial dermis. No significant nuclear pleomorphism or mitotic activity is noted. What is the most important information you need to make the diagnosis?
- Family history of cancer
- History of cancers of other sites
- History of chemotherapy
- History of radiation to the site
Board review style answer #1
D. History of radiation to the site. Atypical vascular lesions only occur in previously irradiated areas of the breast. The histologic description matches that of an atypical vascular lesion but to make a confident diagnosis, prior history of irradiation and histologic examination of the entire lesion is essential.
Comment Here
Reference: Atypical vascular proliferation
Comment Here
Reference: Atypical vascular proliferation
