
Breast
Inflammatory / infectious
Amyloid
Author: Monika Roychowdhury, M.D.

Last author update: 1 October 2016
Last staff update: 21 March 2025 (update in progress)
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Amyloid tumor breast


Table of Contents
Definition / general | Essential features | Terminology | Epidemiology | Sites | Pathophysiology | Etiology | Diagrams / tables | Clinical features | Laboratory | Radiology description | Radiology images | Case reports | Treatment | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Cytology images | Positive stains | Negative stains | Electron microscopy description | Differential diagnosisCite this page: Roychowdhury M. Amyloid . PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/breastamyloidtumor.html. Accessed April 1st, 2025.
Definition / general
- Extracellular mass-like deposition of amorphous and insoluble proteins in an abnormal fibrillary configuration
Essential features
- Extracellular deposition of acellular eosinophilic material in fat, stoma or blood vessels creating a mass effect
- Stains positively for Congo red; metachromatic on Wright stain
- May be localized or part of systemic amyloidosis
- Treatment by complete excision
Terminology
- Amyloidosis in the breast first reported by Fernandez and Hernandez in 1973 (J Clin Pathol 2002;55:634)
- Also called amyloidoma
Epidemiology
- Very rare
- Usually women ages 45 - 79 years
Sites
- 80% occur in right breast
- Bilateral or unilateral but only rarely is confined to breast
Pathophysiology
- Abnormal deposition of insoluble protein in an abnormal fibrillary configuration
- Most common types are amyloid light chain (AL) and amyloid A (AA)
- AL is caused by immunoglobin light chains and is secondary to plasma cell dyscrasia
- AA is reactive amyloidosis and is secondary to chronic inflammatory disease
- In vast majority of patients, breast amyloidosis is part of a systemic AL type disease (usually kappa light chain proteins)
- It can be associated with malignancies of the breast
Etiology
- Depends on the type of amyloidosis:
- AL type amyloidosis - plasma cell dyscrasia (myeloma, Waldenström macroglobulinemia)
- AA type amyloidosis - chronic inflammatory disease (rheumatoid arthritis, reactive arthritis)
Diagrams / tables
Images hosted on other servers:

Figure 7: Flow chart for diagnosis of amyloidosis
Clinical features
- Painless mass
- May occur late in systemic disease
- Complete physical examination needed to differentiate primary and secondary amyloid tumors
Laboratory
- See diagram above
Radiology description
- Visualized as mass on ultrasound and MRI
Radiology images
Images hosted on other servers:


Figures 1 and 2
Case reports
- 58 year old woman with amyloid tumor mimicking breast carcinoma (South Med J 2008;101:199)
- 59 year old woman with sclerosing lymphocytic lobulitis and amyloid of the breast (Breast 2006;15:281)
- 60 year old woman with amyloid tumor in silicone implanted breast (Plast Aesthet Res 2016;3:240)
- 76 year old woman with amyloid deposition of breast (AJR Am J Roentgenol 2000;175:1590)
- 77 year old woman with bilateral breast masses (Arch Pathol Lab Med 2004;128:e67)
- Amyloid deposition of the breast in primary Sjögren syndrome (JBR-BTR 2006;89:313)
Treatment
- Excisional biopsy is successful if amyloid tumor is limited to the breast
Gross description
- 5 cm or less, firm, gray white, opalescent
Microscopic (histologic) description
- Amorphous eosinophilic extracellular deposits in fat, stroma or vessels
- May cause ductal atrophy, form rings around individual fat cells, have associated multinucleated giant cell reaction or osseous metaplasia (J Clin Path 2002;55:634)
Microscopic (histologic) images
Contributed by Dr. Mark R. Wick
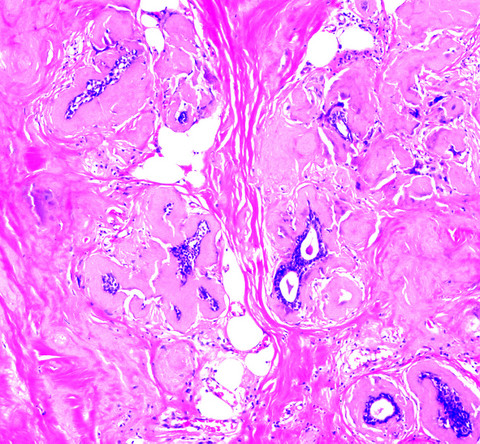
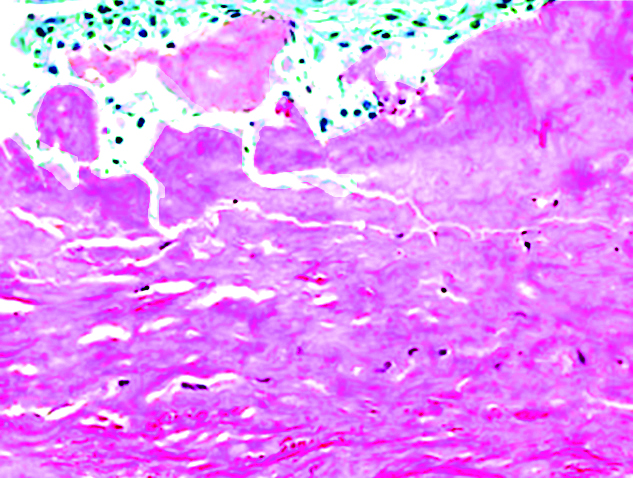
Amyloid tumor
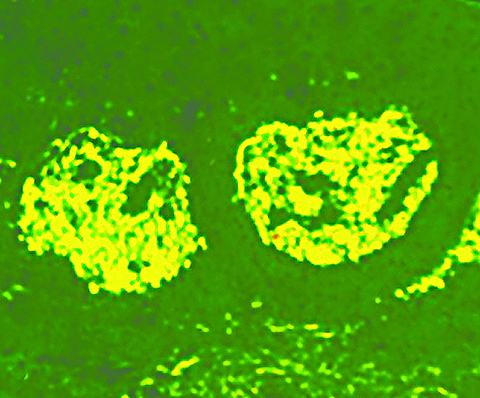
Thioflavin T stain
Parenchyma - Congo red
AFIP images

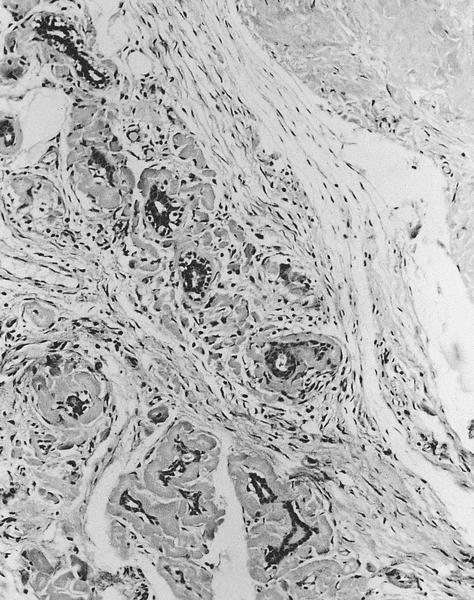
Thick wavy bands of
amyloid around lobular
glands and a nodular deposit
that is virtually acellular
Amyloid occurs in
lobule (lower left) and
as separate stromal
nodule (upper right)
Images hosted on other servers:

Various images

Amyloid with osseous metaplasia
Cytology description
- Amorphous acellular material with scattered plasma cells, lymphocytes, stromal cells and epithelial cells
- Rare multinucleated giant cells
- Metachromatic by modified Wright stain (Diagn Cytopathol 2003;28:325)
Cytology images
Images hosted on other servers:

Dense hyaline material and giant cells
Positive stains
- Congo red (red orange with apple green birefringence under polarized light)
- Metachromatic with crystal violet
Negative stains
Electron microscopy description
- Straight, nonbranching, haphazard amyloid fibrils, 5 - 10 nm, mixed with collagen fibers (Am J Surg Pathol 1986;10:539)
Differential diagnosis
- Plasmacytoma: immature plasma cells, no amyloid
- Stromal fibrosis: may have hyaline material but it has different histologic features from amyloid; also Congo red negative
