
Breast
Noninvasive lobular neoplasia
LCIS florid
Editorial Board Member: Julie M. Jorns, M.D.
Deputy Editor-in-Chief: Gary Tozbikian, M.D.


Last author update: 14 May 2024
Last staff update: 14 May 2024
Copyright: 2024, PathologyOutlines.com, Inc.
PubMed Search: LCIS florid


Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Diagnosis | Radiology description | Radiology images | Prognostic factors | Treatment | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Molecular / cytogenetics description | Videos | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Jones VM, Muller KE. LCIS florid. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/breastLCISflorid.html. Accessed April 3rd, 2025.
Definition / general
- Nonclassical or variant form of lobular carcinoma in situ (LCIS) where acini and ducts are markedly distended with little to no intervening stroma, sometimes imparting a mass-like architecture and comprising cells with cytologic features of classical LCIS (type A or type B cells) with or without comedonecrosis and calcifications
Essential features
- Nonclassical or variant form of lobular carcinoma in situ (LCIS) defined by markedly distended acini / ducts of involved terminal duct lobular units (TDLUs) with scanty to no intervening stroma or an expanded acinus / duct filling at least 1 high power field (~40 - 50 cells in diameter)
- Cells share cytologic features of classic LCIS (type A or type B cells) and lack significant cytologic atypia and pleomorphism
- Commonly unifocal and shows a continuous distribution compared to classic LCIS
- Shows features of a high risk precursor lesion of invasive carcinoma with a higher upgrade rate, increased association with invasive carcinoma and more genetic complexity compared to classic LCIS
Terminology
- Florid LCIS or LCIS, florid type (F-LCIS)
- LCIS with necrosis / comedonecrosis
- Lobular neoplasia (can include atypical lobular hyperplasia and LCIS)
- LCIS, variant type (not recommended)
- The term florid is not synonymous with extensive or diffuse
ICD coding
Epidemiology
- F > M
- Florid LCIS tends to significantly affect older, postmenopausal women (mean ages reported: 56 - 61 years) compared to classic LCIS (mean age: 50 years) (Hum Pathol 2013;44:1998, Am J Surg Pathol 2006;30:1445, Eur J Surg Oncol 2019;45:2279)
- Rare; comprises < 5% of LCIS
- Majority arise in association with classic LCIS or atypical lobular hyperplasia (ALH) (Ann Diagn Pathol 2020;45:151481)
- Strong association with invasive lobular carcinoma, potentially as a direct precursor (Am J Surg Pathol 2019;43:399, Arch Med Res 2010;41:436, Ann Diagn Pathol 2020;45:151481, Ann Surg Oncol 2011;18:1845)
Sites
- Florid and pleomorphic LCIS tend to be unifocal and shows a continuous distribution compared to classic LCIS, which has a tendency to be multicentric and bilateral (Virchows Arch 2000;436:421, Virchows Arch 2022;481:823, Am J Surg Pathol 2019;43:399)
Pathophysiology
- First described in 2006 as a form of LCIS with central necrosis (Am J Surg Pathol 2006;30:1445)
- Early tumorigenesis of LCIS is marked by loss of heterozygosity of the wild type allele and inactivating mutations of E-cadherin (Br J Cancer 1997;76:1131)
- E-cadherin, encoded by the CDH1 gene on chromosome 16q22.1, is a cell - cell adhesion molecule that helps maintains lobular architecture
- Clonal relationship to classic LCIS: harbors characteristic signature of LCIS showing 16q loss and 1q gain (Hum Pathol 2013;44:1998)
- Florid LCIS is proposed to progress from classic LCIS by acquiring additional genetic (i.e., frequent ERBB2 or ERBB3 alterations, CCND1 amplifications) and chromosomal alterations (Mod Pathol 2020;33:1287, Mod Pathol 2020;33:1078, Hum Pathol 2013;44:1998)
- Significantly more genome alterations and amplifications compared to classic LCIS (Hum Pathol 2013;44:1998)
- Similar genetic complexity as apocrine pleomorphic LCIS (Hum Pathol 2013;44:1998)
Etiology
- No specific risk factors reported for florid LCIS
- In patients with nonclassic LCIS variants, including florid LCIS, 10/24 patients (41.7%) are reported to have a first degree family history of breast cancer (Surg Oncol 2019;28:190)
- Overall, there is increased risk of LCIS with the following
- High mammographic breast density (Cancer 2015;121:1369)
- History of breast biopsy (J Natl Cancer Inst 2001;93:1811)
- Older age at menopause (J Natl Cancer Inst 2001;93:1811)
- Family history of breast cancer (Breast Cancer Res Treat 2003;78:7)
- Hormone replacement therapy in postmenopausal women (Am J Epidemiol 2017;186:1329)
Diagnosis
- Diagnostic core or excisional biopsy, surgical excision
Radiology description
- Florid and pleomorphic LCIS tend to have a radiographic (95%) or palpable target (5%) (Am J Surg Pathol 2019;43:399)
- Among nonclassic LCIS, including florid LCIS, calcifications were the most common biopsy indication (80%) and all categorized as BI-RADS 4 (Ann Surg Oncol 2019;26:55, Eur J Surg Oncol 2019;45:2279)
- Florid LCIS with necrosis typically presents with calcifications and rarely can present with a mass or density (Mod Pathol 2021;34:1495, Am J Surg Pathol 2019;43:399)
- Florid LCIS without necrosis typically presents as nonmass enhancement on magnetic resonance imaging (MRI) and architectural distortion (Mod Pathol 2021;34:1495, Am J Surg Pathol 2019;43:399)
Radiology images
Contributed by Kristen E. Muller, D.O. and Victoria M. Jones, M.D.

Mammographic calcifications
Prognostic factors
- Outcome data on pure florid LCIS is limited, many studies combine nonclassical LCIS (florid and pleomorphic LCIS) when reporting outcomes
- Florid LCIS shows features of a high risk precursor lesion of invasive carcinoma, which is frequently grade 2 or 3 invasive lobular carcinoma (Mod Pathol 2021;34:1495, Breast J 2020;26:2350, Am J Surg Pathol 2019;43:399, Eur J Surg Oncol 2019;45:2279)
- Pathologic excisional upgrade rate to invasive carcinoma or ductal carcinoma in situ (DCIS) on excision ranges from 17 to 39% (Mod Pathol 2021;34:1495, Am J Surg Pathol 2019;43:399, Eur J Surg Oncol 2019;45:2279)
- 57 - 87% of florid LCIS with necrosis and calcification shows an associated invasive carcinoma, frequently invasive lobular phenotype (Hum Pathol 2013;44:1998)
- Upgrade rate may be associated with the extent of radiographic microcalcifications, extensive florid LCIS (mean: 3.2 cm) and possibly the presence of necrosis (Eur J Surg Oncol 2019;45:2279, Mod Pathol 2021;34:1495)
- ER and HER2 biomarker expression, compared to classic LCIS, suggests a more unfavorable phenotype (Hum Pathol 2013;44:1998)
- Frequent ERBB2 / ERBB3 alterations are associated with more aggressive potential and invasive lobular carcinoma (Mod Pathol 2020;33:1078)
- There is significant variability in recurrence rates but one study found that 25 patients with nonclassic LCIS (including florid LCIS) treated solely with excision had a 4% incidence of future ipsilateral malignancy (Ann Surg Oncol 2019;26:55)
- Recurrences tend to be ipsilateral lobular tumors (Breast J 2020;26:2350)
- Natural history is unknown; out of 3 cases of florid LCIS without necrosis on core biopsy not excised due to patient preference or clinical recommendation, none recurred within a follow up range of 56 - 73 months (Am J Surg Pathol 2019;43:399)
Treatment
- Complete surgical excision of florid LCIS is recommended (WHO) (Virchows Arch 2022;481:823, Hum Pathol 2013;44:1998, Eur J Surg Oncol 2019;45:2279, Mod Pathol 2021;34:1495, Arch Pathol Lab Med 2017;141:1668)
- In one study, 58% of pure LCIS variants (including 5 florid LCIS) were excised to negative margins and treated with endocrine but not radiation therapy (Am J Surg Pathol 2019;43:399)
- No recurrences in a mean follow up interval of 50 months
- Consensus and optimal treatment regimens remain unclear, including the benefits of hormone chemoprevention in women without associated invasive carcinoma (WHO) (Virchows Arch 2022;481:823)
- There are no data supporting the use of adjuvant radiation therapy (Ann Diagn Pathol 2020;45:151481, Virchows Arch 2022;481:823)
Microscopic (histologic) description
- Diagnosis requires the presence of at least 1 of 2 architectural features (Mod Pathol 2020;33:1287, Am J Surg Pathol 2019;43:399, Ann Diagn Pathol 2020;45:151481)
- Markedly distended acini / ducts of involved TDLUs with little to no intervening stroma or
- Expanded acinus / duct filling at least 1 high power field (~40 - 50 cells in diameter)
- Marked distention of acini and ducts with little intervening stroma may impart a confluent, mass-like architecture
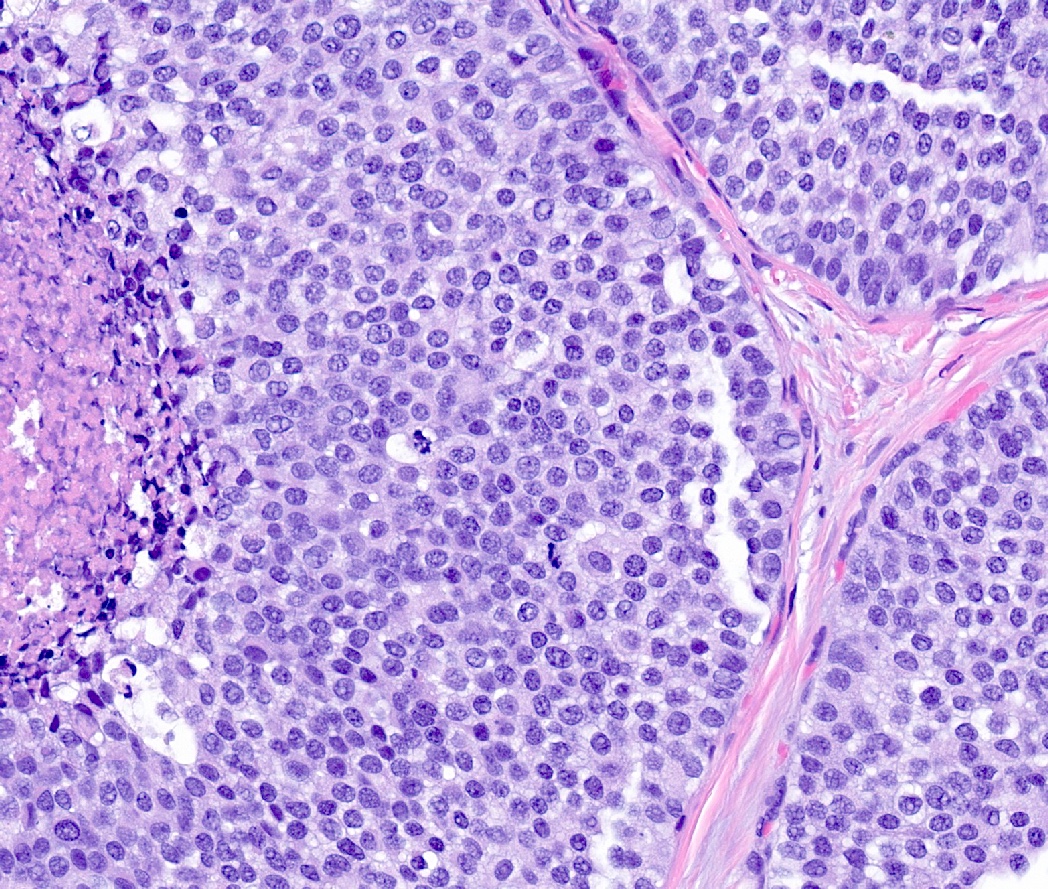
- Solid, dyshesive, monomorphic proliferation of classic LCIS type A cells (scant cytoplasm, small uniform nuclei, inconspicuous nucleoli) or type B cells (increased cytoplasm, larger nuclei, more prominent nucleoli) (Am J Surg Pathol 2019;43:399, Ann Diagn Pathol 2020;45:151481)
- Absence of marked nuclear pleomorphism and atypia, distinguishes from pleomorphic LCIS
- Comedo or single cell necrosis is common, up to 71% of cases (Mod Pathol 2020;33:1287, Mod Pathol 2021;34:1495)
- Comedo type necrosis, mitosis and apoptosis are more frequent in florid LCIS than in pleomorphic LCIS (Hum Pathol 2018;78:163)
- May observe apocrine features (rounded, enlarged nuclei with prominent nucleoli and abundant eosinophilic and granular cytoplasm), more commonly in ER negative cases (Mod Pathol 2021;34:1495)
- Rarely composed entirely of signet ring cells, which has a high frequency of associated invasive lobular carcinoma (80% of 10 cases in small series) (Arch Med Res 2010;41:436)
- Often coexists with classic or pleomorphic LCIS
Microscopic (histologic) images
Contributed by Kristen E. Muller, D.O. and Victoria M. Jones, M.D.

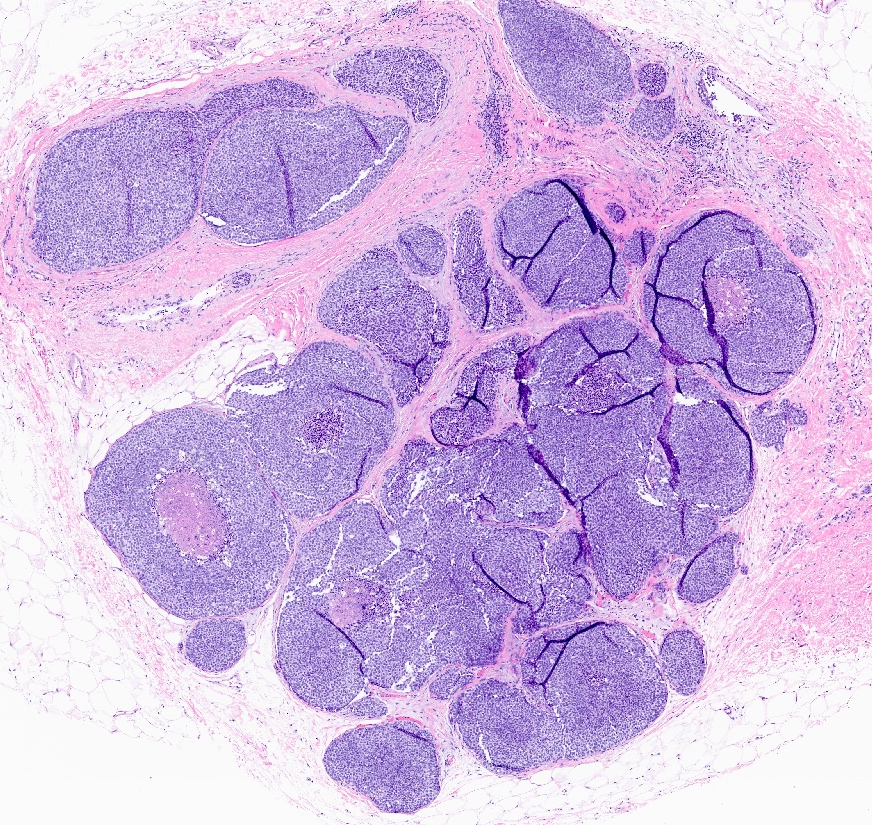
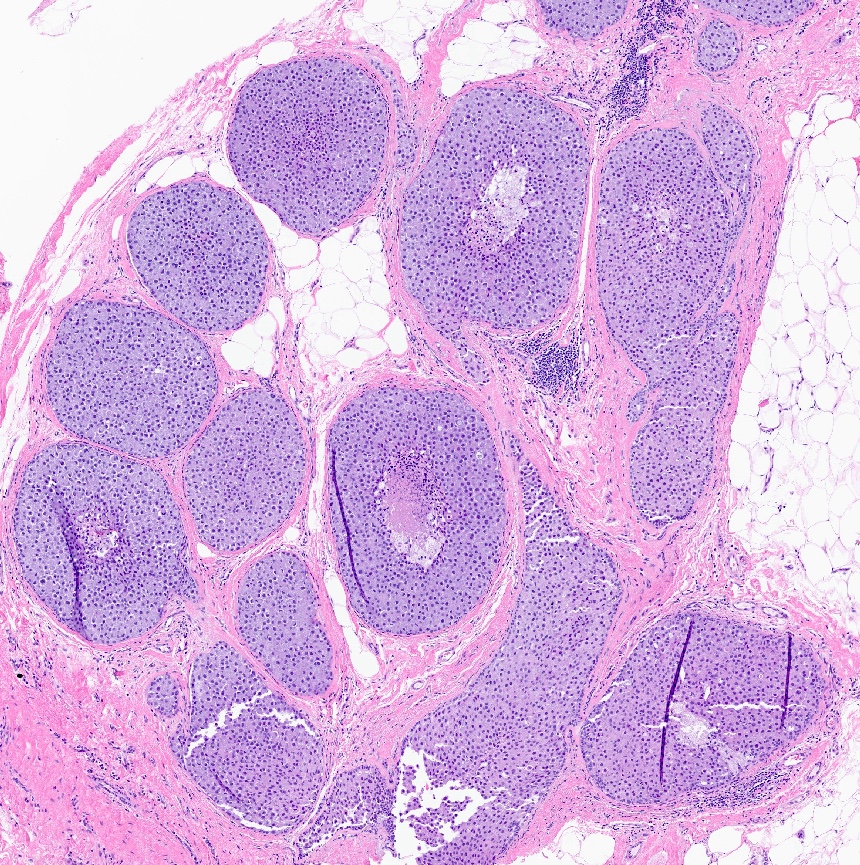
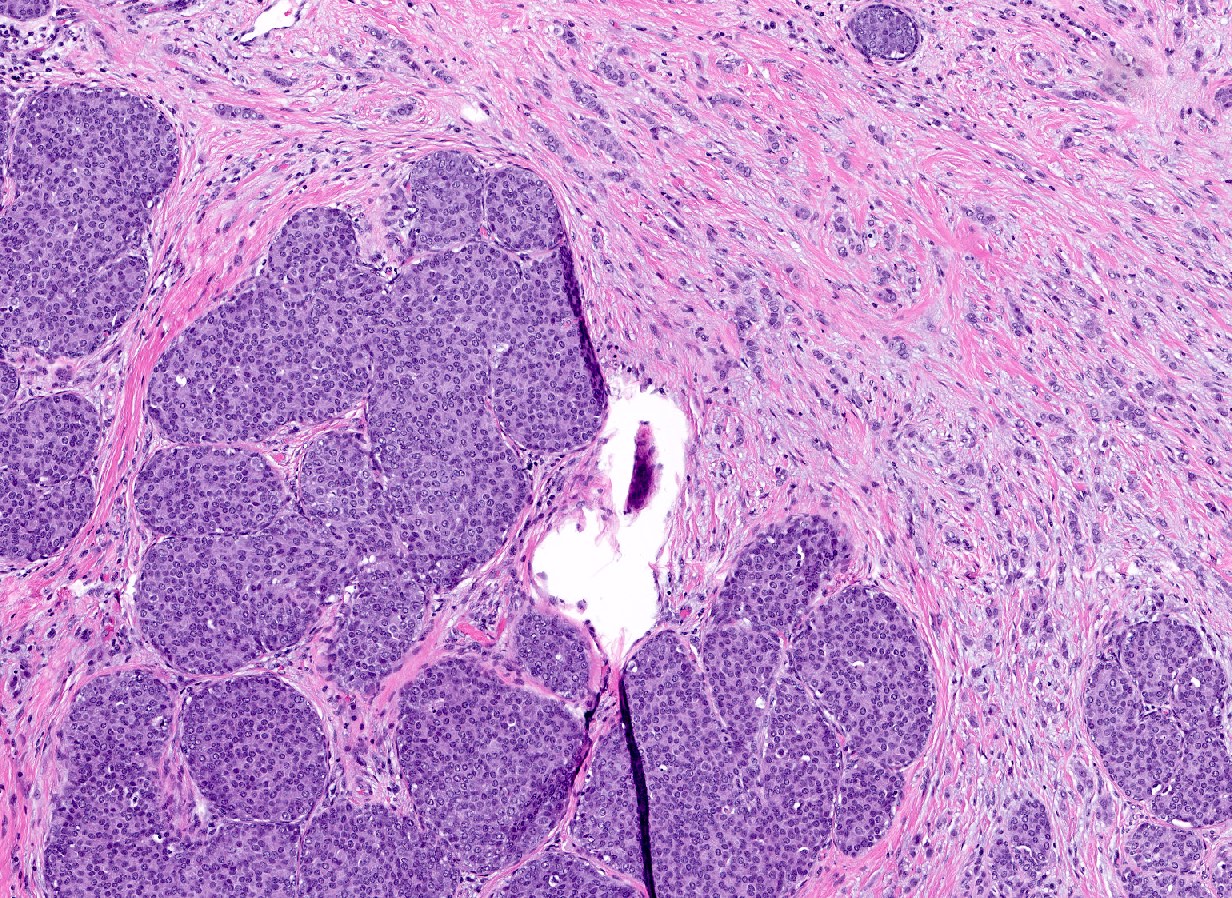
Florid LCIS with mass-like architecture

Single acinus
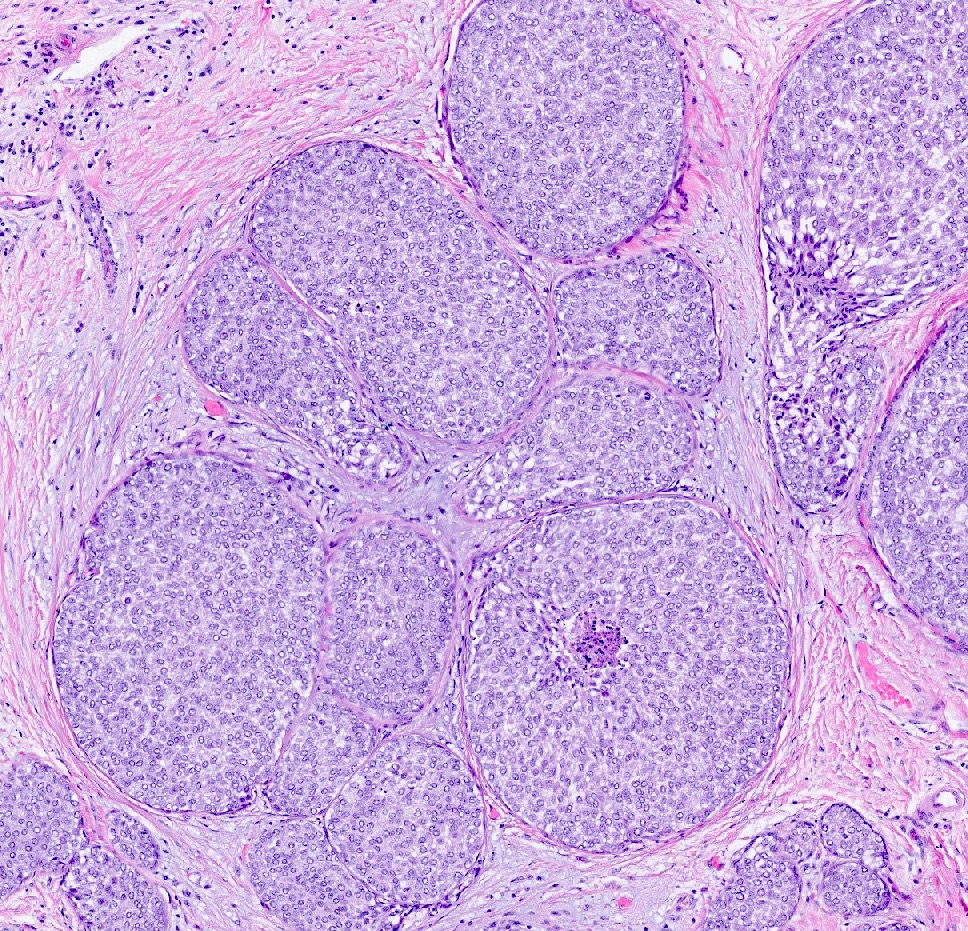
Little intervening stroma

Necrosis

Calcifications


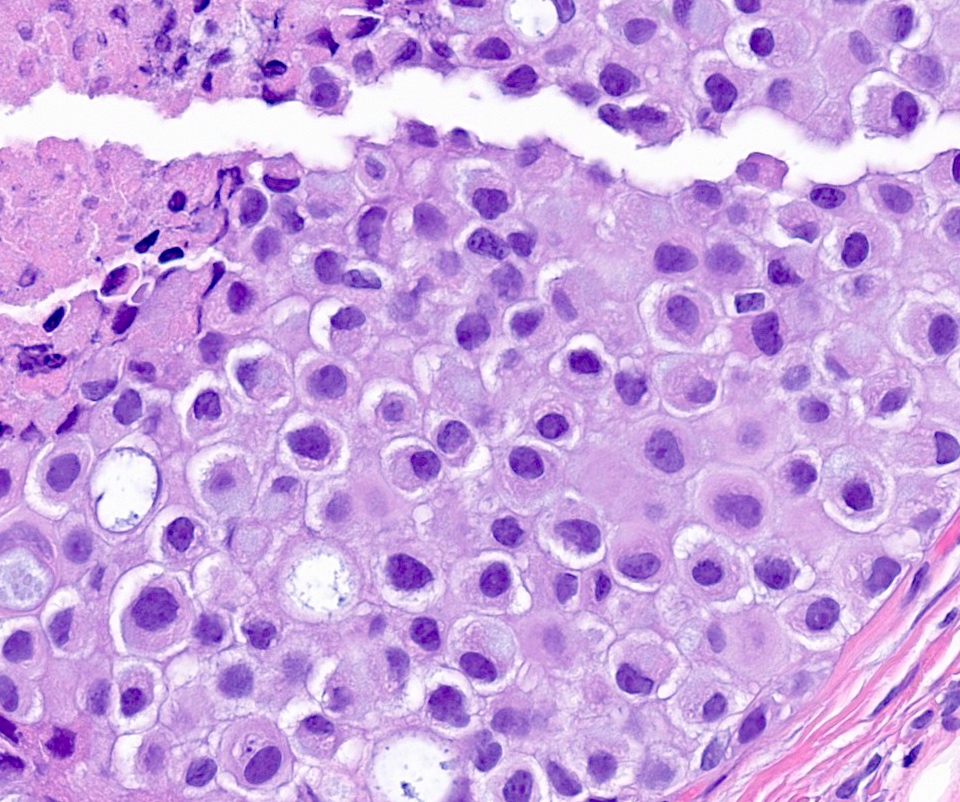
Type B cells
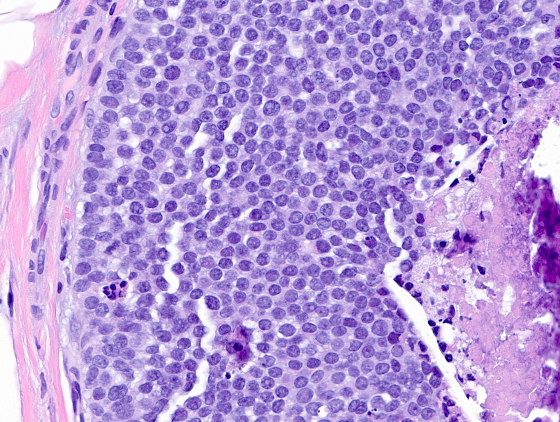
Type A cells
Mitoses
Apocrine features
Invasive lobular carcinoma
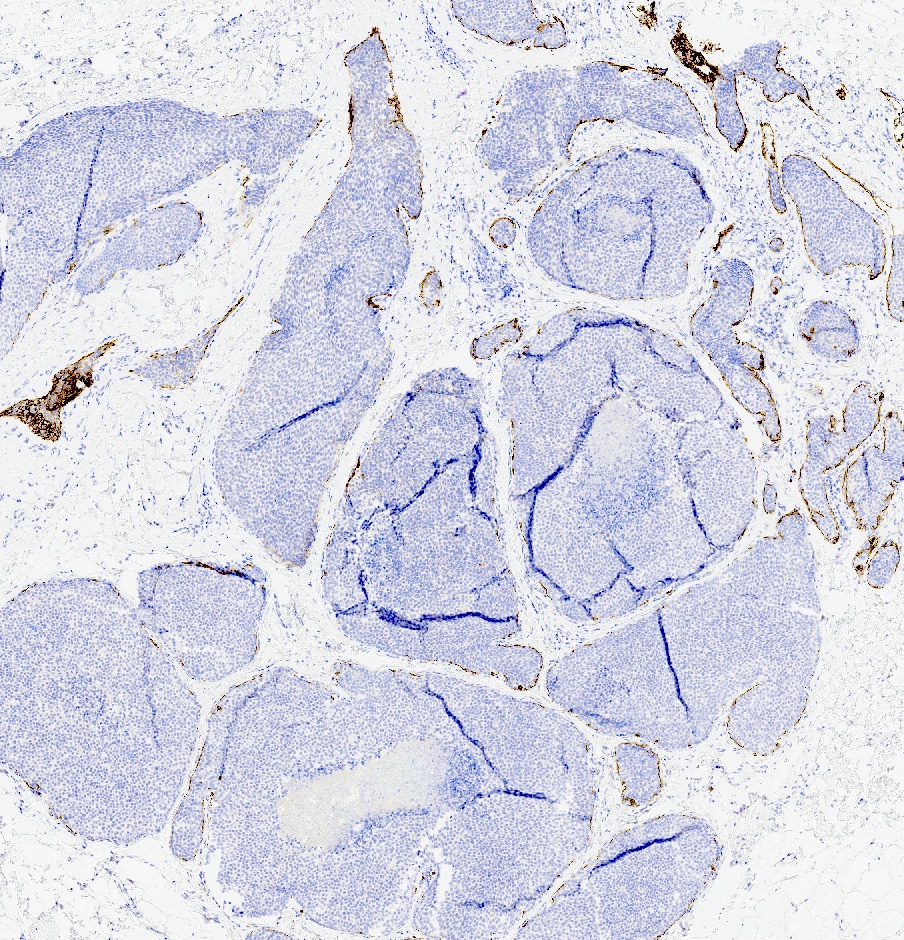
E-cadherin
Positive stains
- ER, strong and diffuse (77 - 100%) (Hum Pathol 2013;44:1998, Am J Surg Pathol 2019;43:399, Mod Pathol 2021;34:1495)
- ER positive in 33% in florid LCIS with apocrine features, 94% in florid LCIS without apocrine features (Mod Pathol 2021;34:1495)
- Ki67 (median of 7.5% and range of 1 - 23% in LCIS variants of no significant difference between florid and pleomorphic LCIS) (Am J Surg Pathol 2019;43:399)
- p120, abnormal cytoplasmic accumulation (Surg Pathol Clin 2018;11:123)
- Androgen receptor expression, positive in all LCIS variants, independent of apocrine features (Virchows Arch 2022;481:823, Mod Pathol 2021;34:1495)
Negative stains
- PR (35% in LCIS variants including florid LCIS) (Am J Surg Pathol 2019;43:399)
- HER2 (13 - 18%, florid LCIS) (Hum Pathol 2013;44:1998), Mod Pathol 2021;34:1495)
- Classic LCIS is typically ER positive, PR positive, HER2 negative (Breast Cancer Res Treat 2005;90:249, Surg Pathol Clin 2018;11:123)
- ER and HER2 are consistently concordant between florid LCIS variants and upgraded invasive lobular carcinoma (Am J Surg Pathol 2019;43:399)
- Cyclin D1 protein expression (40%, florid LCIS) (Hum Pathol 2013;44:1998)
- E-cadherin, negative or aberrant membranous expression in florid LCIS (Mod Pathol 2021;34:1495)
- Loss of beta catenin membranous expression in LCIS variants, including florid LCIS (Mod Pathol 2020;33:1287)
Molecular / cytogenetics description
- Florid LCIS shares the LCIS molecular hallmarks of 16q loss and 1q gain (Mod Pathol 2020;33:1287, Mod Pathol 2020;33:1078)
- CDH1 gene encoding for E-cadherin on chromosome 16
- Pathogenic alterations in CDH1, ERRB2, PIK3CA, ERRB3, RUNX1, FOXA1, CCND1 and CBFB (Mod Pathol 2020;33:1287, Mod Pathol 2020;33:1078)
- Frequent ERBB2 / ERBB3 alterations (HER2 / HER3) are associated with more aggressive potential and invasive lobular carcinoma (Mod Pathol 2020;33:1078)
- Additional, complex genomic alterations including (Mod Pathol 2020;33:1078)
- Gain of interstitial or whole arm 17q, loss of distal or whole arm 8p, 11q and 17p, loss of distal or whole arm 18q or whole chromosome 18, loss of 13q or whole chromosome 13, gain of distal or whole arm 16p, gain of 8q or whole chromosome 8
- Significantly more fraction genome alteration and loss, number of breakpoints and chromosomes with breakpoints and amplifications than classic LCIS (Hum Pathol 2013;44:1998)
- Similar genetic complexity to apocrine pleomorphic LCIS (Hum Pathol 2013;44:1998)
Videos
Lobular carcinoma in situ and high risk breast lesions
Sample pathology report
- Breast, right, core needle biopsy:
- Lobular carcinoma in situ (LCIS), florid type (see comment)
- Comment: The biopsy shows ducts and lobules that are markedly distended by a proliferation of classic LCIS cells (small, round, discohesive, uniform cells) with comedo type necrosis and calcifications. An E-cadherin immunostain is negative in lesional cells supporting interpretation as florid LCIS.
Differential diagnosis
- Classic LCIS:
- Similar cytologic features as florid LCIS (type A or type B cells)
- Lacks marked distention of acini and ducts
- If borderline distension is between florid and classic, it should be categorized as classic (Ann Diagn Pathol 2020;45:151481)
- Florid is not synonymous with extensive or diffuse LCIS (implies extensive involvement of multiple terminal duct lobular units [TDLUs] but without marked distension) (Mod Pathol 2021;34:8)
- Pleomorphic LCIS:
- Similar expanded architecture, large ducts, comedonecrosis and calcifications as florid LCIS
- Distinguishing high grade, pleomorphic nuclei
- Large (> 4x lymphocyte nuclei), occasional multinucleation (Ann Diagn Pathol 2020;45:151481)
- Solid pattern DCIS, low and intermediate grade:
- May have necrosis, degeneration and a discohesive appearance
- Sharply defined cell membranes
- Retained E-cadherin (Ann Diagn Pathol 2020;45:151481)
- Usual ductal hyperplasia, florid type:
- Heterogeneous cohesive cells that may be spindled and overlapping
- May also have central necrosis
- E-cadherin positive
- Atypical lobular hyperplasia:
- Similar cytologic features as florid LCIS (type A or type B cells)
- Lacks uniform, marked distention of acini and ducts
- Criteria of Page et al. (Schnitt: Biopsy Interpretation of the Breast, 3rd Edition, 2017)
- Distends 50% or more acini within a lobule (so resembles lobular carcinoma in situ) but not uniformly present throughout entire lobule or
- Involves all acini in a TDLU and so resembles lobular carcinoma in situ but does not distend the acini (i.e., caliber of the involved acini is similar to that of uninvolved acini)
Additional references
Board review style question #1
The photomicrographs above are from a 63 year old woman who underwent core needle biopsy for screen detected calcifications. An E-cadherin immunostain is negative in lesional cells. What is the most appropriate diagnosis?
- Atypical lobular hyperplasia
- Ductal carcinoma in situ
- Lobular carcinoma in situ, classic type
- Lobular carcinoma in situ, florid type
- Lobular carcinoma in situ, pleomorphic type
Board review style answer #1
D. Lobular carcinoma in situ, florid type. The images show markedly expanded acini with central necrosis and calcification and little intervening stroma. The cells are uniform, small and round without marked pleomorphism. The differential usually includes ductal carcinoma in situ (DCIS) and lobular carcinoma in situ (LCIS). A negative E-cadherin immunostain supports interpretation as LCIS and given the marked distention with scanty stroma, florid LCIS is the best diagnosis. Answer B is incorrect because this lesion is negative for E-cadherin and DCIS would have it retained. Answer C is incorrect because this meets diagnostic criteria for florid LCIS given the marked acinar distention. Answer E is incorrect because the lesional cells lack cytologic features of pleomorphic LCIS. Answer A is incorrect because atypical lobular hyperplasia (ALH) shows similar cytologic features to florid LCIS; however, criteria for ALH include either type A or type B cells that distend 50% or more acini within a lobule but not uniformly present throughout the entire terminal duct lobular unit (TDLU) or involves all acini in a TDLU but does not distend the acini. In contrast, florid LCIS shows markedly distended acini in a TDLU.
Comment Here
Reference: LCIS florid
Comment Here
Reference: LCIS florid
Board review style question #2
Which of the following is a true statement regarding florid lobular carcinoma in situ (LCIS)?
- Florid LCIS is always HER2 negative
- Florid LCIS is not typically detected by mammography
- Florid LCIS is rarely upgraded to invasive carcinoma; thus, surgical excision is not recommended
- Florid LCIS shares the classic LCIS molecular hallmarks of 16q loss and 1q gain
Board review style answer #2
D. Florid LCIS shares the classic LCIS molecular hallmarks of 16q loss and 1q gain. In addition, florid LCIS has significantly more genomic alterations and amplifications compared to classic LCIS and in some studies, shows a similar genetic complexity to apocrine pleomorphic LCIS. Answer B is incorrect because florid LCIS is frequently detected by imaging and presents with calcifications (most commonly) or a mass / density. Answer C is incorrect because the upgrade rate to invasive carcinoma or DCIS is between 17 and 39%. Although consensus guidelines are not yet available, most experts agree that surgical excision should be recommended. Answer A is incorrect because florid LCIS is reported to be HER2 positive 13 - 18% of the time and shows frequent ERBB2 / ERBB3 alterations in molecular studies.
Comment Here
Reference: LCIS florid
Comment Here
Reference: LCIS florid
