
Bone & joints
Osteogenic tumors
Benign
Osteoma, NOS
Editorial Board Member: Nasir Ud Din, M.B.B.S.
Deputy Editor-in-Chief: Borislav A. Alexiev, M.D.


Last author update: 3 August 2021
Last staff update: 12 October 2023
Copyright: 2003-2025, PathologyOutlines.com, Inc.
PubMed Search: Osteoma pathology

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Videos | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Serinelli S, de la Roza G. Osteoma, NOS. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/boneosteoma.html. Accessed April 1st, 2025.
Definition / general
- Benign, bone forming tumor composed of mature cortical type or less frequently, trabecular bone, typically involving the craniofacial skeleton
Essential features
- Benign osteogenic tumor
- Usually involves the surface of craniofacial bones
- Admixture of mature lamellar and woven bone patterns, with Haversian-like canals
- Cortical type bone architecture is typical
- Lack of cellular atypia
Terminology
- Torus palatinus (if palate is involved)
- Torus mandibularis (if mandible is involved)
- Parosteal osteoma
- Button osteoma
- Ivory exostosis
ICD coding
Epidemiology
- Incidence:
- Accounts for 0.03% of biopsied primary bone tumors
- Paranasal sinus osteoma: 3 - 6.4% of CT scans performed for sinus conditions (Acta Otolaryngol 2015;135:602)
- Present in 80% with Gardner syndrome
- Age: fourth through sixth decades
- Sex: M = F
Sites
- Essentially restricted to the craniofacial skeleton (paranasal sinuses, orbit, nasal cavity, jaw bones, cranial vault)
- Common in frontal and ethmoid sinuses of mandible
- Rare locations: long tubular bones (Nielson: Diagnostic Pathology - Bone, 2nd Edition, 2017)
- Typically arises from the surface of the involved bone (Goldblum: Rosai and Ackerman's Surgical Pathology, 11th Edition, 2017)
Pathophysiology
- Controversy in the literature whether osteoma represents a true neoplasm or a developmental anomaly
Etiology
- Still unclear
- Theories: reactive bone hyperplasia triggered by trauma or infection; advanced ossification; end stage of fibrous dysplasia or subperiosteal hematomas (Imaging Sci Dent 2011;41:107)
- Presence of multiple osteomas is suggestive of Gardner syndrome, a variant of familial adenomatous polyposis (FAP) that is characterized by colorectal adenomas, osteomas and benign skin tumors; it is caused by mutations in the APC gene (Imaging Sci Dent 2016;46:267)
Clinical features
- Commonly an incidental finding (Nielson: Diagnostic Pathology - Bone, 2nd Edition, 2017)
- Usually slow growing and asymptomatic (Surg Pathol Clin 2012;5:101)
- Typically appears as a solitary mass; multiple tumors can be seen in Gardner syndrome (Imaging Sci Dent 2016;46:267)
- Depending on the size and location, it can cause headache, facial pain, obstruction of paranasal sinuses, vision disturbancies, interference with mastication
Diagnosis
- Radiology findings often helpful
Radiology description
- In general, the lesion involves the surface of the bone and appears well delineated, ovoid or mushroom shaped, with broad base of attachment to cortex (Nielson: Diagnostic Pathology - Bone, 2nd Edition, 2017)
- Xray: radiodense lesion with varying amounts of central lucency
- CT: cortical density on bone window; no contrast enhancement (Clin Radiol 2000;55:435)
- MRI: low signal intensity on T1 and T2 weighted images; no contrast enhancement
Radiology images
AFIP images

Dense lobular mass in frontal sinus
Images hosted on other servers:

CT bone window
Prognostic factors
- Excellent prognosis
- No recurrence if completely excised
Case reports
- 27 year old man with osteoma of the maxilla (J Oral Maxillofac Pathol 2020;24:179)
- 34 year old man with giant frontoethmoidal osteoma (Asian J Neurosurg 2020;15:737)
- 40 year old woman with retromastoid osteoma (J Surg Case Rep 2020;2020:rjz381)
- 45 year old woman with proximal femoral osteoma (Skeletal Radiol 2015;44:755)
- 47 year old man with thoracic spine osteoma (AME Case Rep 2019;3:10)
Treatment
- Observation for asymptomatic cases
- Surgical excision for symptomatic cases
Clinical images
Images hosted on other servers:

Osteoma of anterior maxilla

Forehead osteomas

Nasal cavity osteoma with actinomycosis
Gross description
- Typically a solitary lesion (Nielson: Diagnostic Pathology - Bone, 2nd Edition, 2017, Surg Pathol Clin 2012;5:101)
- Tan-white
- Oval, round or polypoid
- Firm
- Well circumscribed and attached to the underlying bone
- Cut surface with dense compact bone or trabecular bone
Gross images
Contributed by David R. Lucas, M.D. and Mark R. Wick, M.D.


Osteoblastoma-like osteoma
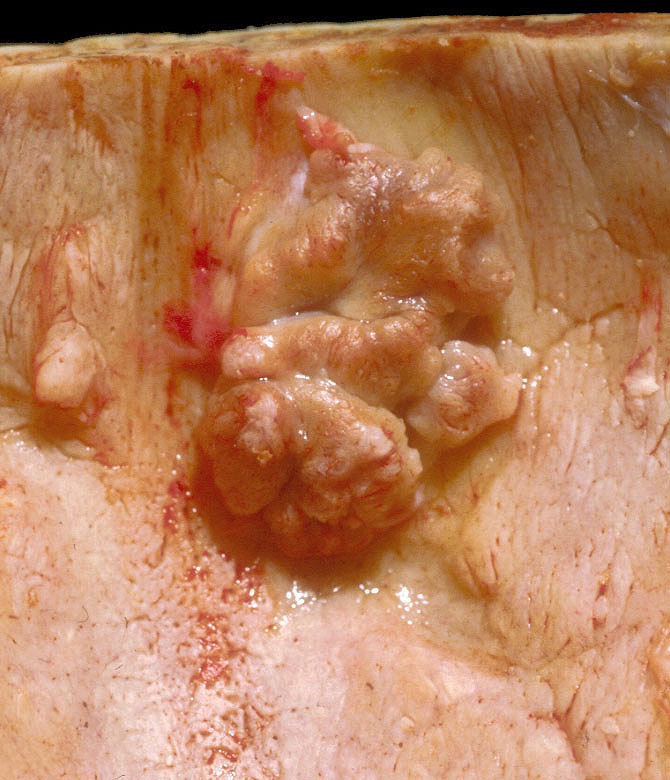
Skull osteoma
Images hosted on other servers:

Osteoma with smooth bosselated surface

Giant orbit osteoma

Fronto-ethmoidal osteoma
Microscopic (histologic) description
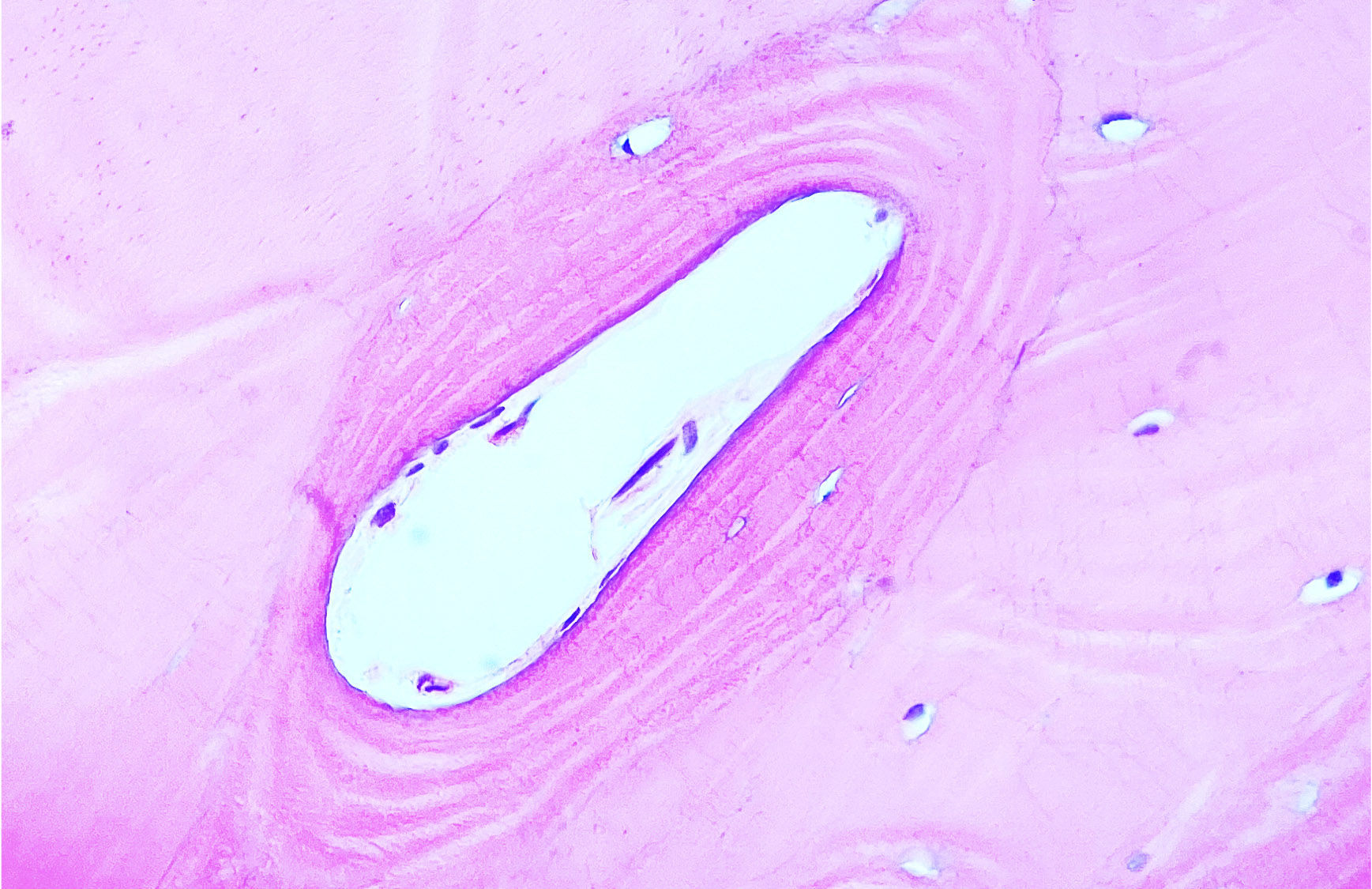
- Admixture of mature lamellar and woven bone patterns, with Haversian-like canals, which may have various sizes and shapes (Nielson: Diagnostic Pathology - Bone, 2nd Edition, 2017)
- More frequent: cortical type bone architecture
- Less frequent: trabecular bone architecture
- Osteoblasts rimming bone are inconspicuous and small but can be prominent in growing lesions
- Osteocytes in the matrix are small, not atypical and randomly distributed (Surg Pathol Clin 2012;5:101)
- Intertrabecular marrow spaces are filled with moderately cellular, loose fibrous stroma (BMJ Case Rep 2013;2013:bcr2013009857)
- Inflammatory infiltrates are typically absent
Microscopic (histologic) images
Contributed by Serenella Serinelli, M.D., Ph.D., Gustavo de la Roza, M.D. and Kelly Magliocca, D.D.S., M.P.H.
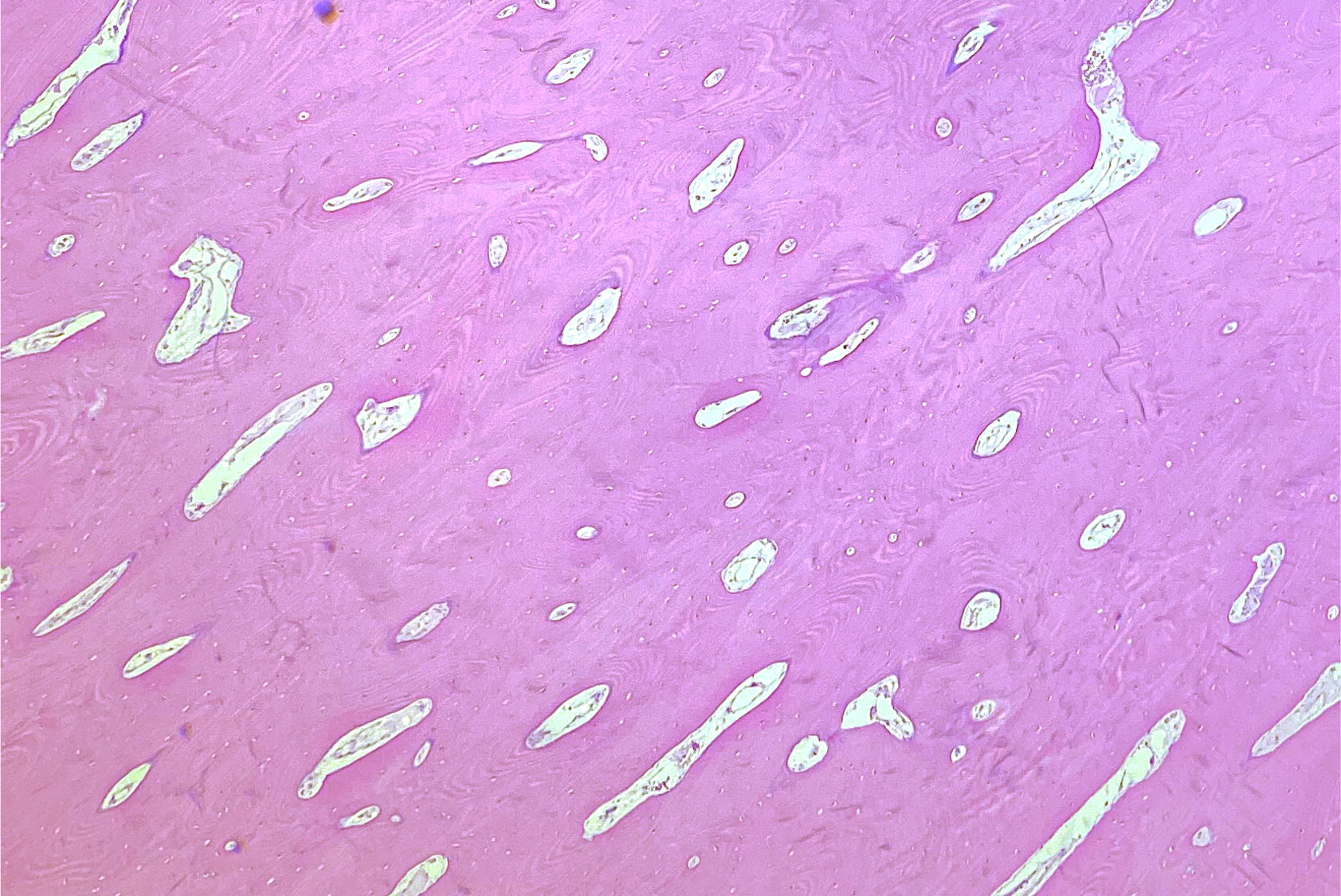
Cortical type bone architecture
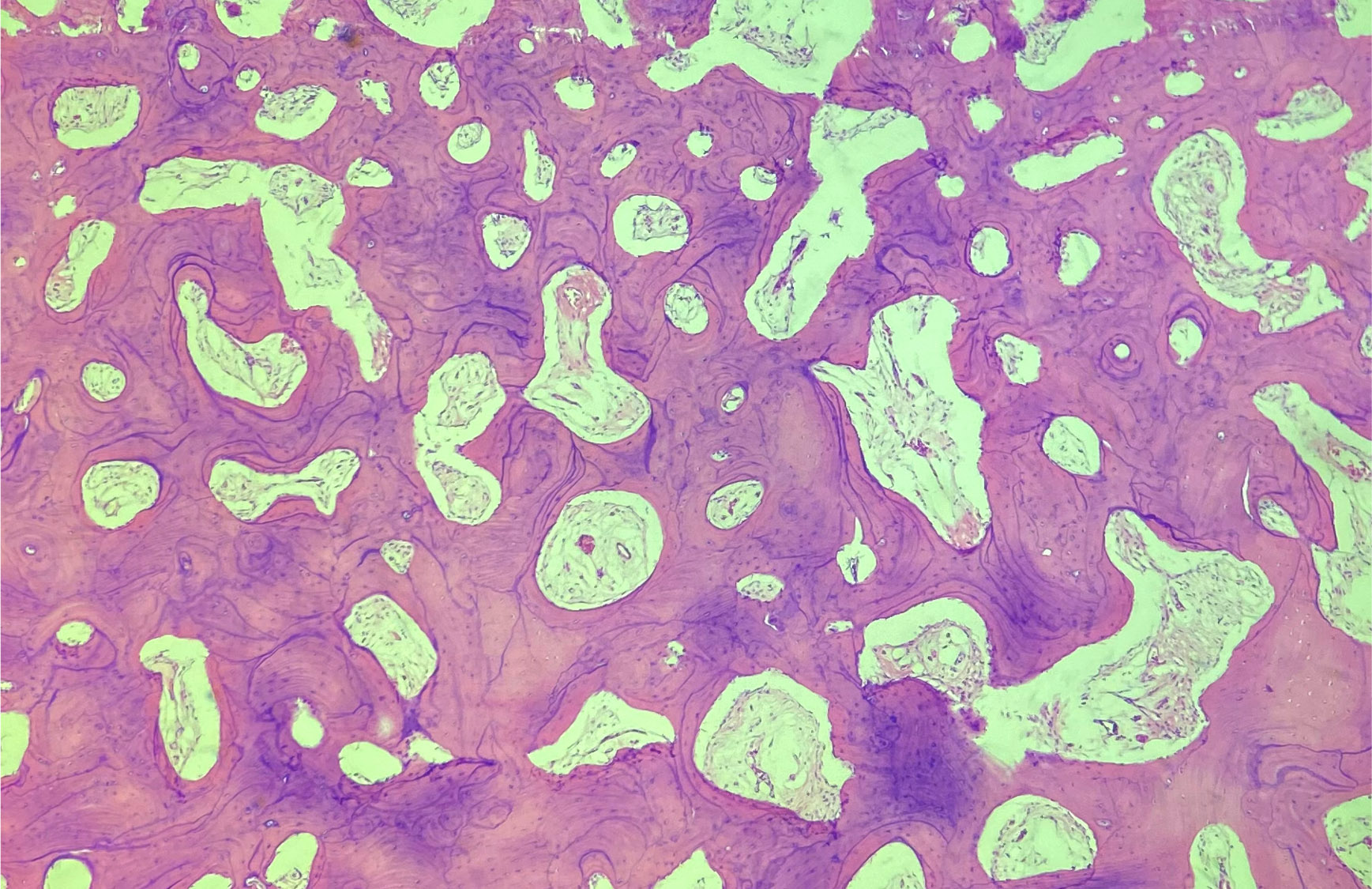
Trabecular bone architecture
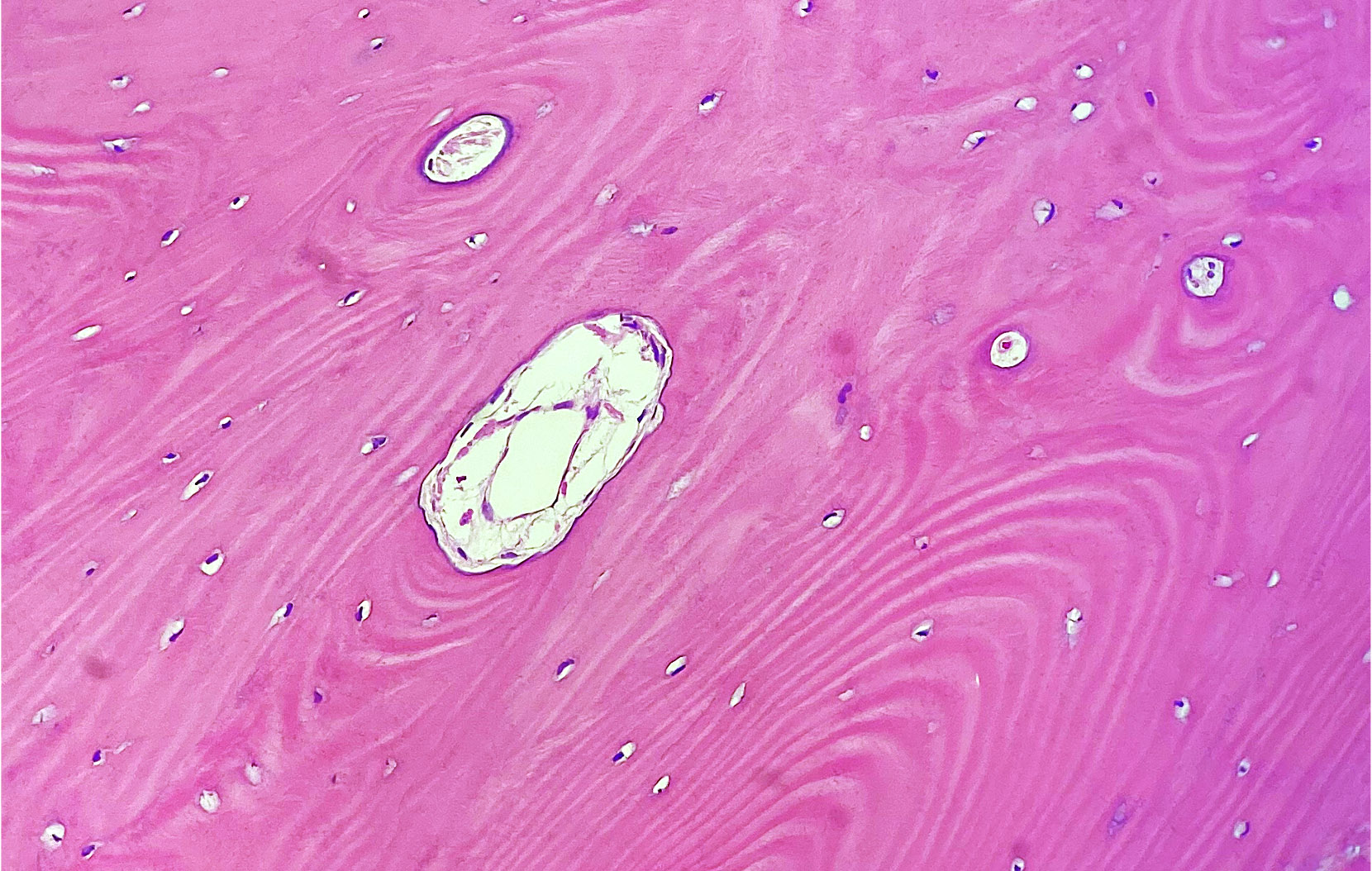
Lamellar bone
Osteoblasts and osteocytes
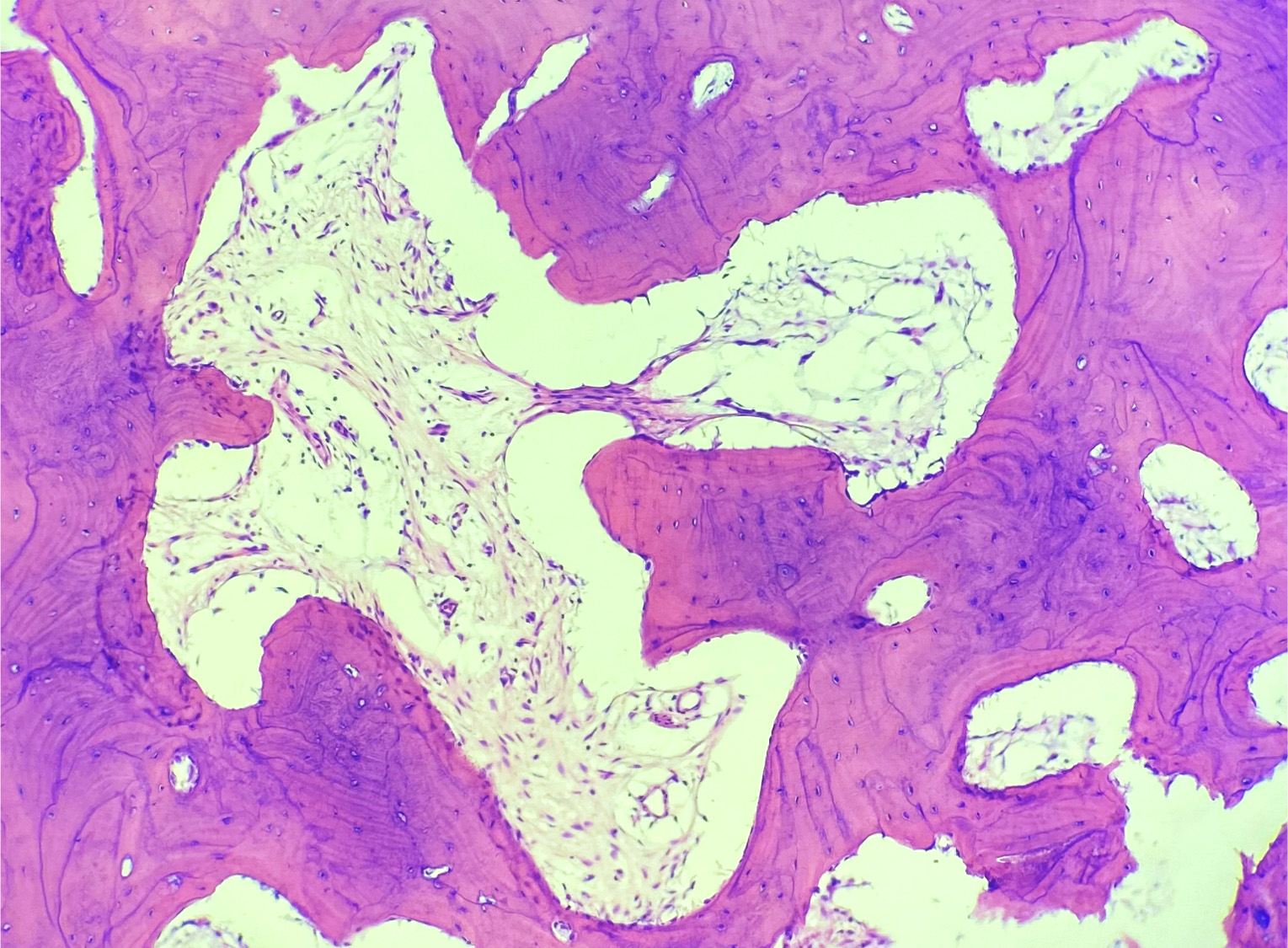
Fibrous stroma in marrow spaces

Osteoma
Videos
Osteoma of bone
Sample pathology report
- Bone, left forehead, excision:
- Osteoma
Differential diagnosis
- Parosteal osteosarcoma:
- Prominent spindle cell component with atypia
- Osteoid osteoma / osteoblastoma:
- Intracortical or intramedullary location
- Large osteoblasts rimming the surface of the bone
- Osteochondroma:
- Cartilagineous cap
- Continuity of the tumor with the medullary cavity
- Bone island:
- Intramedullary location
- Cortical type bone
- More common in males
Additional references
Board review style question #1
A 40 year old woman seeks treatment for a slowly enlarging lesion over the left forehead. The mass is found to involve the external surface of the left frontal skull and is excised. The histology is shown above. What is the diagnosis?
- Osteoblastoma
- Osteochondroma
- Osteoid osteoma
- Osteoma
- Parosteal osteosarcoma
Board review style answer #1
Board review style question #2
Which of the following is a feature of osteoma?
- Atypia has to be present to make the diagnosis
- Involves mainly the long bones
- Most frequent architecture is cortical type bone
- Most frequent architecture is trabecular bone
- Typically does not involve the craniofacial skeleton
Board review style answer #2
