
Bone & joints
Other tumors
Mazabraud syndrome
Editorial Board Member: Borislav A. Alexiev, M.D.
Editor-in-Chief: Debra L. Zynger, M.D.


Last author update: 24 September 2020
Last staff update: 5 May 2021
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed search: Mazabraud syndrome
Related topics: Myxoma

Table of Contents
Definition / general | Essential features | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Radiology description | Prognostic factors | Case reports | Treatment | Microscopic (histologic) description | Microscopic (histologic) images | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Johnson TH, Davis JL. Mazabraud syndrome. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/bonemazabraud.html. Accessed April 2nd, 2025.
Definition / general
- Mazabraud syndrome is a rare condition resulting from postzygotic activating somatic mutations in the GNAS gene
- Typically codon 201 and rarely codon 227 (Histopathology 2007;50:691)
- The exact presentation and severity depend on the extent of mosaicism and the involved tissues (Curr Osteoporos Rep 2015;13:146)
- Most patients are diagnosed in adulthood
Essential features
- Mazabraud syndrome is the dyad of:
- Fibrous dysplasia of bone, either polyostotic or monostotic
- One or more intramuscular myxomas
ICD coding
Epidemiology
- Mazabraud syndrome is a very rare disorder identified with an estimated prevalence of < 1 in 1,000,000 and most data is drawn from a single large European cohort (J Bone Joint Surg Am 2019;101:160)
- 2.2% of a multicenter European cohort of 1,446 patients with fibrous dysplasia eventually met criteria for Mazabraud syndrome (J Bone Joint Surg Am 2019;101:160)
- F:M = 2.2:1 (J Bone Joint Surg Am 2019;101:160)
- Women with right sided polyostotic fibrous dysplasia are statistically most likely to eventually be diagnosed
- 15% have a preexisting diagnosis of McCune-Albright syndrome
- Rare (< 1%) lifetime risk of sarcomatous transformation of fibrous dysplasia
Sites
- There is an unexplained slight (60%) right sided predominance (J Bone Joint Surg Am 2019;101:160)
- Fibrous dysplasia in Mazabraud syndrome is most commonly found in the proximal femur, pelvis and proximal tibia (J Bone Joint Surg Am 2019;101:160)
- In contrast, nonsyndromic fibrous dysplasia is most commonly found in the ribs
- Intramuscular myxomas are almost always adjacent to fibrous dysplasia lesions and are usually found in the quadriceps femoris or lower limb girdle muscles (J Bone Joint Surg Am 2019;101:160)
Pathophysiology
- Constitutively active mutant GNAS results in increased cAMP
- Increased cAMP:
- Promotes proliferation and inhibits differentiation of fibroblasts, which replace normal bone producing fibrous dysplasia lesions
- Promotes proliferation and inhibits differentiation of fibroblasts forming expansile, myxoid mass within muscle
- Fibrous dysplasia elaborates fibroblast growth factor 23 (FGF23):
- Inhibits renal resorption of phosphate
- Causes hypophosphatemia
- Causes hyperphosphaturia
Etiology
- Results from de novo mutations in GNAS (J Bone Joint Surg Am 2019;101:160)
- No inherited case has ever been reported
- Germline GNAS mutation is presumed embryonic lethal
- Has no risk factors
Clinical features
- The two most common presentations are:
- Fibrous dysplasia related pain / pathologic fracture
- Intramuscular myxomas related pain
- Fibrous dysplasia seen in Mazabraud syndrome:
- Commonly polyostotic but may be monostotic
- Is often unilateral, in keeping with postzygotic mutation and is more often right sided
- Intramuscular myxomas seen in Mazabraud syndrome:
- Are usually multiple
- Are more likely to recur than their sporadic counterparts, although this observation may instead represent additional primary lesions
- Often declare themselves up to 10 years after fibrous dysplasia
Diagnosis
- Mazabraud syndrome is essentially a clinical diagnosis
- Role of genetic testing:
- Not routinely performed but available
- False negatives are common due to mosaicism and sampling
- Positive results merely confirm a clinical diagnosis
- No genotype / phenotype correlation, therefore no prognostic value (Orphanet J Rare Dis 2008;3:12)
- Up to 10 years temporal separation between diagnosis of fibrous dysplasia and clinically / radiologically apparent intramuscular myxomas is a significant barrier to diagnosis
Laboratory
- Some patients with McCune-Albright syndrome have:
- Depressed serum phosphate
- Elevated urine phosphate
- However, these are also seen in sporadic fibrous dysplasia
Radiology description
- Fibrous dysplasia
- On plain radiography and CT, fibrous dysplasia is usually well defined and homogeneous with endosteal scalloping and cortical thinning
- Classic ground glass opacification is only sometimes present
- MRI is not a recommended modality for assessing fibrous dysplasia (Insights Imaging 2018;9:1035)
- Intramuscular myxoma
- On US, intramuscular myxoma is a hypoechoic ovoid mass frequently with a hyperechoic rim (a so called bright rim sign) or hyperechoic pole(s)
- Plain radiography is not recommended for assessing intramuscular myxoma
- On CT, intramuscular myxoma is a well demarcated, hypodense, ovoid mass
- On MRI, intramuscular myxoma has multiple patterns beyond the scope of this article (Radiographics 2014;34:964)
Prognostic factors
- Severity of hypophosphatemia and number or extent of fibrous dysplasia lesions correlates with the risk for bone pain and pathologic fracture (J Bone Miner Res 2016;31:2167)
- Sites of fibrous dysplasia are established early and burden of disease typically plateaus by age 15 (Expert Opin Investig Drugs 2007;16:761)
Case reports
- 25 year old woman with left thigh pain (Indian J Endocrinol Metab 2013;17:740)
- 28 year old woman with a preexisting diagnosis of McCune-Albright syndrome develops multiple intramuscular myxomas (Acta Biomed 2017;88:198)
- 51 year old woman develops chondrosarcoma arising in femoral fibrous dysplasia (Orthop Traumatol Surg Res 2015;101:875)
- 63 year old woman with maxillofacial Mazabraud syndrome (J Stomatol Oral Maxillofac Surg 2018;119:44)
- 69 year old woman with suspected metastatic colon cancer proven to be concomitant Mazabraud syndrome (Clin Nucl Med 2018;43:625)
Treatment
- There is no specific therapy
- Fibrous dysplasia and intramuscular myxoma are treated just as their sporadic counterparts (StatPearls: McCune Albright Syndrome [Accessed 21 April 2020])
Microscopic (histologic) description
- Fibrous dysplasia lesions seen in Mazabraud syndrome are histologically indistinguishable from nonsyndromic fibrous dysplasia, characterized by (Arch Pathol Lab Med 2013;137:134):
- Woven bone with trabeculae that are:
- Thin
- Irregular
- Curvilinear
- Fibrous stroma
- Absence of osteoblastic rimming
- Woven bone with trabeculae that are:
- Intramuscular myxoma lesions seen in Mazabraud syndrome are histologically indistinguishable from nonsyndromic intramuscular myxomas, characterized by (Am J Surg Pathol 1998;22:1222):
- Bland stellate and bipolar fibroblasts
- Abundant myxoid matrix
- Highly variable cellularity
Microscopic (histologic) images
Contributed by Jessica L. Davis, M.D.
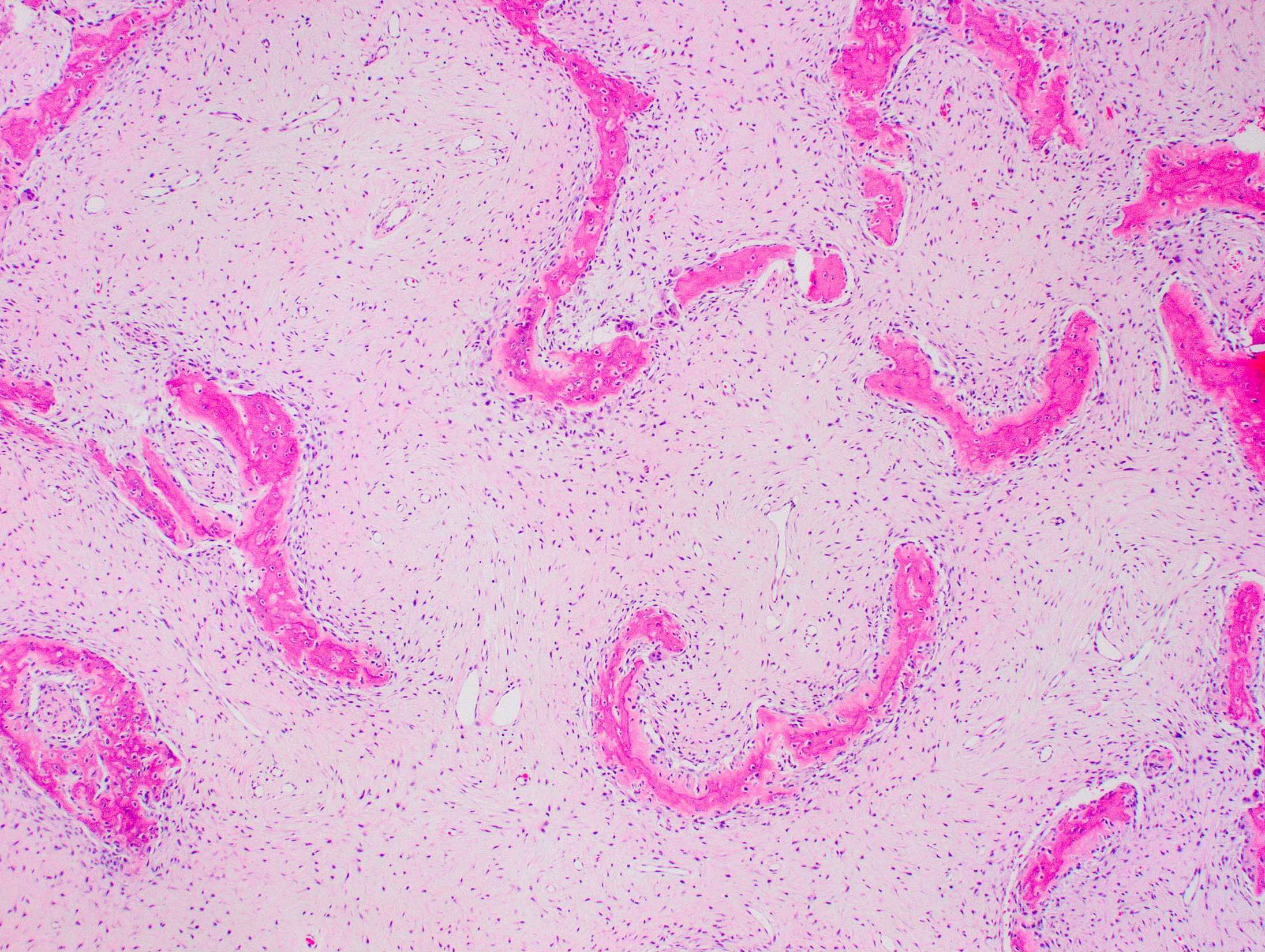
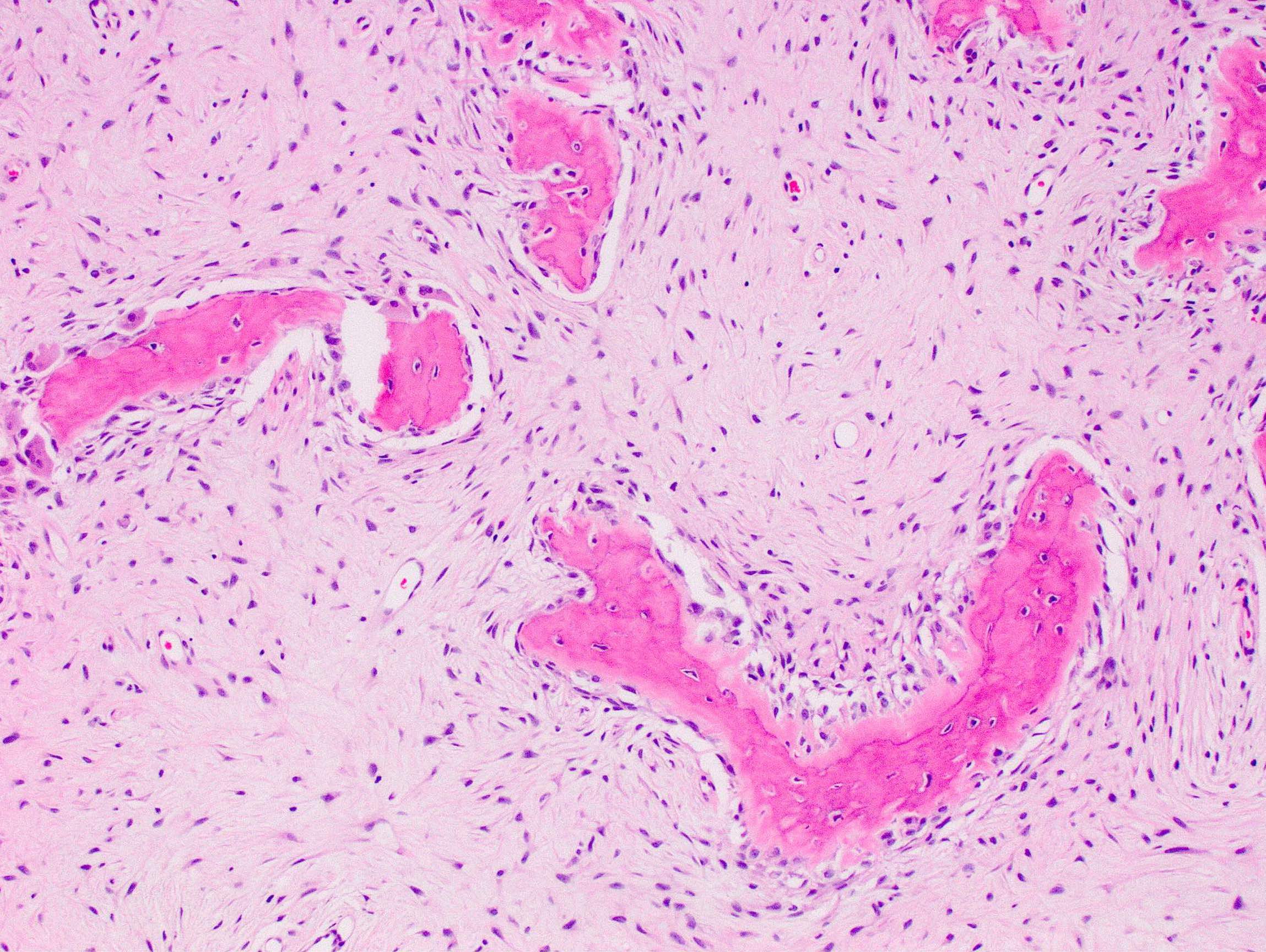
Fibrous dysplasia
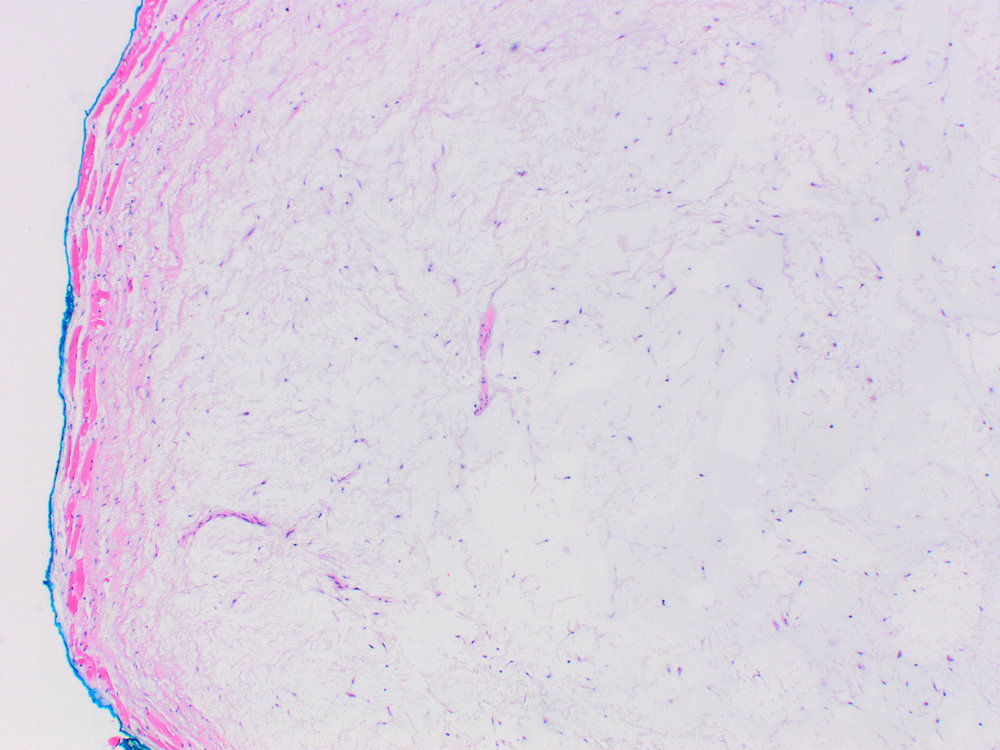
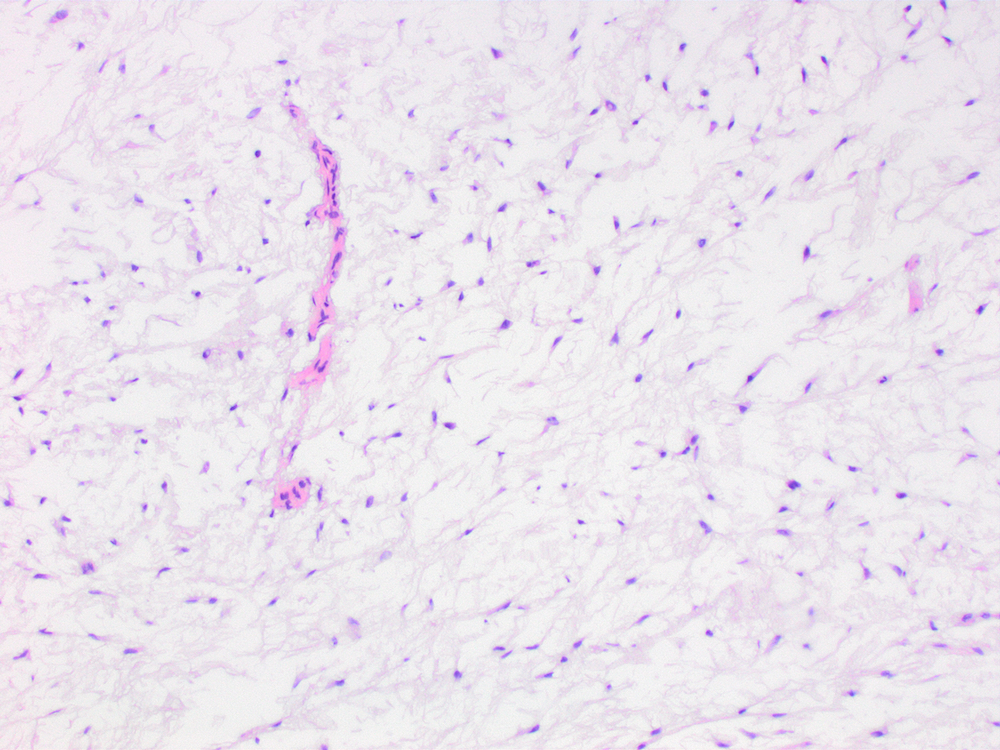
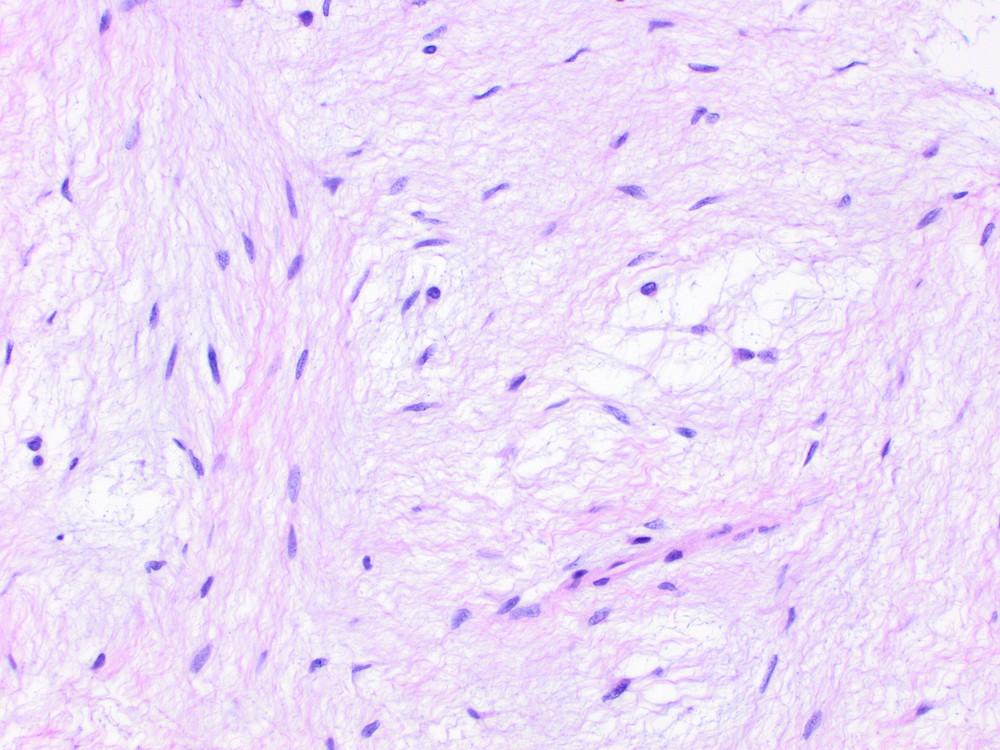
Intramuscular myxoma
Molecular / cytogenetics description
- Sequencing may identify mutations in codon 201 or codon 227 (Histopathology 2007;50:691)
Sample pathology report
- Bone, biopsy:
- Fibrous dysplasia of bone (see comment)
- Comment: Fibrous dysplasia is most commonly sporadic but is also a typical presenting feature of McCune-Albright syndrome and Mazabraud syndrome. Clinical correlation is advised.
- Soft tissue, biopsy:
- Intramuscular myxoma (see comment)
- Comment: Intramuscular myxomas are most commonly sporadic but are also a common presenting feature of Mazabraud syndrome. Clinical correlation is advised.
Differential diagnosis
- Myxofibrosarcoma, low grade fibromyxoid sarcoma and myxoid liposarcoma:
- Hypercellular areas of intramuscular myxoma can resemble these entities
- Lack GNAS mutations (Am J Surg Pathol 1998;22:1222)
- Juxta-articular myxoma:
- Primarily a pediatric lesion, whereas intramuscular myxoma is an adult lesion
- Lacks GNAS mutation (Virchows Arch 2002;440:12)
- Nonsyndromic fibrous dysplasia of bone:
- Results from postzygotic GNAS mutations
- Other features of McCune-Albright syndrome are absent or as yet undeclared
- Nonsyndromic intramuscular myxoma:
- Results from postzygotic GNAS mutations
- Other features of McCune-Albright syndrome are absent or as yet undeclared
- McCune-Albright syndrome:
- Results from postzygotic GNAS mutations
- Typically diagnosed in childhood or adolescence
- Lacks intramuscular myxomas
- Includes hyperfunctional endocrinopathy or café au lait macules
- 15% of patients diagnosed with Mazabraud syndrome carry a diagnosis of McCune-Albright syndrome
Board review style question #1
- A 54 year old woman is seen for 1 year of progressive radicular symptoms and on imaging is found to have a 2 cm lesion in her right piriformis muscle impinging upon her sciatic nerve. The resection specimen is signed out as intramuscular myxoma. She has no other significant medical history. Which of the following is true?
- The lesion is most likely sporadic
- The lesion most likely has an inactivating GNAS mutation
- The lesion most likely has wild type GNAS
- The patient most likely has Mazabraud syndrome
- The patient most likely has McCune-Albright syndrome
Board review style answer #1
A. Most intramuscular myxomas are sporadic. Although intramuscular myxomas are a feature of Mazabraud syndrome as in A, the patient does not meet diagnostic criteria which include polyostotic fibrous dysplasia and multiple intramuscular myxomas. McCune-Albright syndrome, as in C, does not include intramuscular myxomas. The genotype for sporadic intramuscular myxoma is an activating mutation in codon 201 of GNAS, not wild type as in B, and not an inactivating mutation as in E.
Comment Here
Reference: Mazabraud syndrome
Comment Here
Reference: Mazabraud syndrome
Board review style question #2
- A 49 year old man presents to the ER after sudden onset of severe left hip pain while watering his garden. A plain radiograph reveals a fracture of the left femur involving a well circumscribed lesion with central ground glass matrix and an incomplete sclerotic rim. Similar lesions are noted in the left pubic ramus and left iliac wing. He undergoes hip replacement, and while being seen for possible revision 4 years later, a CT demonstrates well demarcated, hypodense, ovoid lesions in the gluteus minor and vastus medialis muscles. What is the etiology of these lesions?
- Chronic abscess formation
- Dysplastic ossification of soft tissue
- Migration of prosthetic hardware
- Natural progression of Mazabraud syndrome
- Sporadic mutation of a tyrosine kinase
Board review style answer #2
D. The patient's lesions are most consistent with polyostotic fibrous dysplasia and intramuscular myxomas, which together constitute Mazabraud syndrome.
Comment Here
Reference: Mazabraud syndrome
Comment Here
Reference: Mazabraud syndrome
