

Bone & joints
Other nonneoplastic
Epidermoid inclusion cyst
Authors: Alnoor Akber, M.D., Nasir Ud Din, M.B.B.S.
Resident / Fellow Advisory Board: Josephine K. Dermawan, M.D., Ph.D.
Deputy Editor-in-Chief: Borislav A. Alexiev, M.D.


Last author update: 3 May 2022
Last staff update: 3 May 2022
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed search: Epidermoid inclusion cyst

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Frozen section description | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Akber A, Ud Din N. Epidermoid inclusion cyst. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/boneepidermoidcyst.html. Accessed December 25th, 2024.
Definition / general
- Benign epithelial inclusion cyst in the bone lined with stratified squamous epithelium, identical to cutaneous counterpart
Essential features
- Benign cystic lesion
- Post traumatic squamous epithelium embedded in bone
- Cyst wall lined by squamous epithelium, including granular layer
- Cyst contents contain laminated keratin
Terminology
- Epidermoid inclusion cyst, epidermal inclusion cyst, intraosseous epidermoid cyst
ICD coding
- ICD-10: L72.0 - epidermal cyst
Epidemiology
- Rare incidence
- Young to middle aged
Sites
- Common in the acral skeleton (fingers and toes) and skull (J Bone Joint Surg Br 1966;48:577, Cancer 1958;11:643, J Bone Joint Surg Am 1964;46:1442)
- Skull lesions arise during the first decade
Pathophysiology
- Traumatic embedding of squamous epithelium in the bone that forms a mass (Clin Orthop Relat Res 1970;68:84, J Bone Joint Surg Br 1982;64:456)
Clinical features
- Asymptomatic / painless lump
- Can become tender due to inflammation
Diagnosis
- Clinical, radiological and pathological correlation is adequate for diagnosis
Radiology description
- Xray
- Round osteolytic lesion with sharply demarcated sclerotic borders and thin cortex
- Expansion of bone
- Pathologic fracture is uncommon
- MRI (Clin Neurol Neurosurg 2021;200:106381):
- Hypointense on T1
- Hyperintense on T2
Radiology images
Contributed by Nasir Ud Din, M.B.B.S
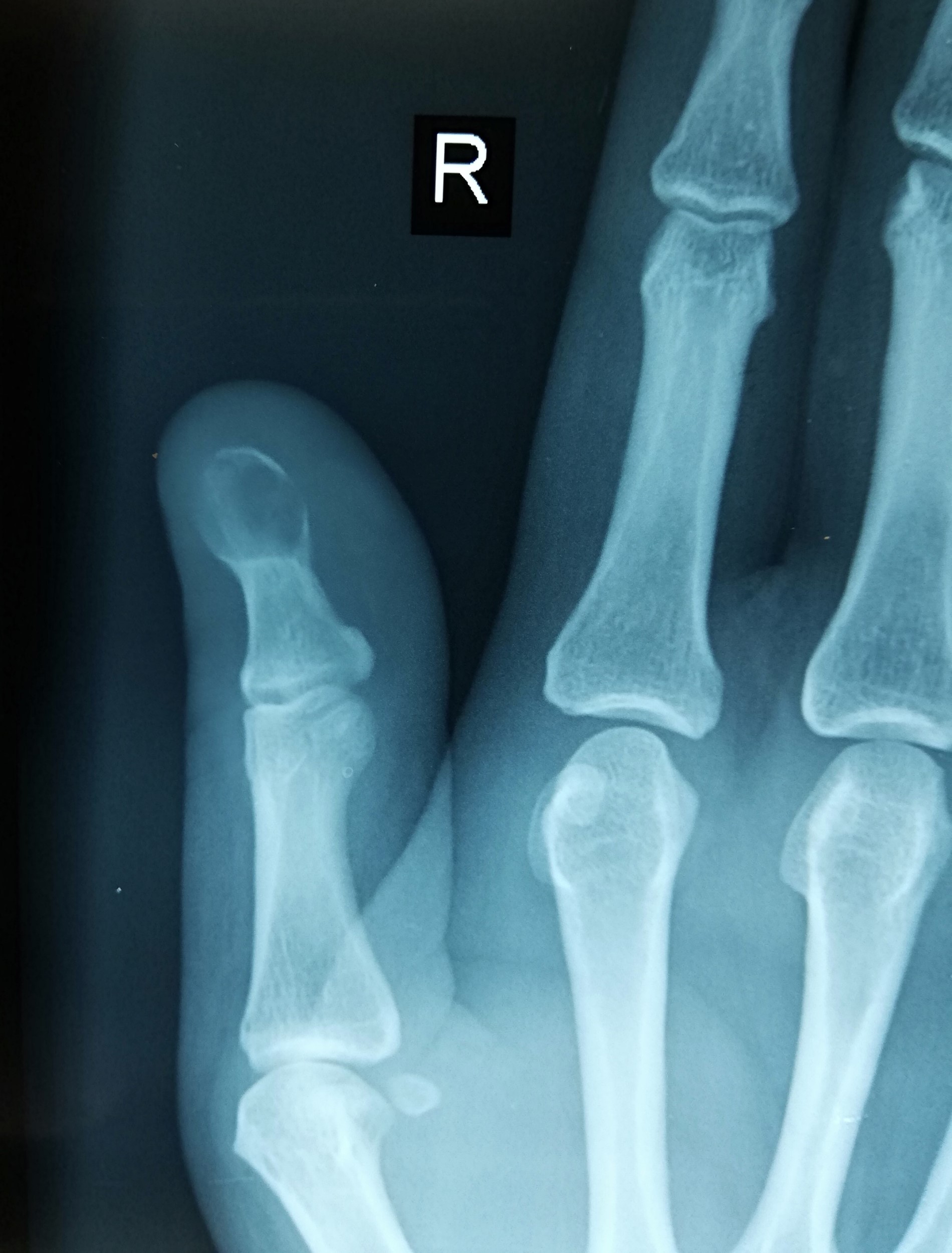

Distal phalanx of thumb

Distal phalanx of fourth finger
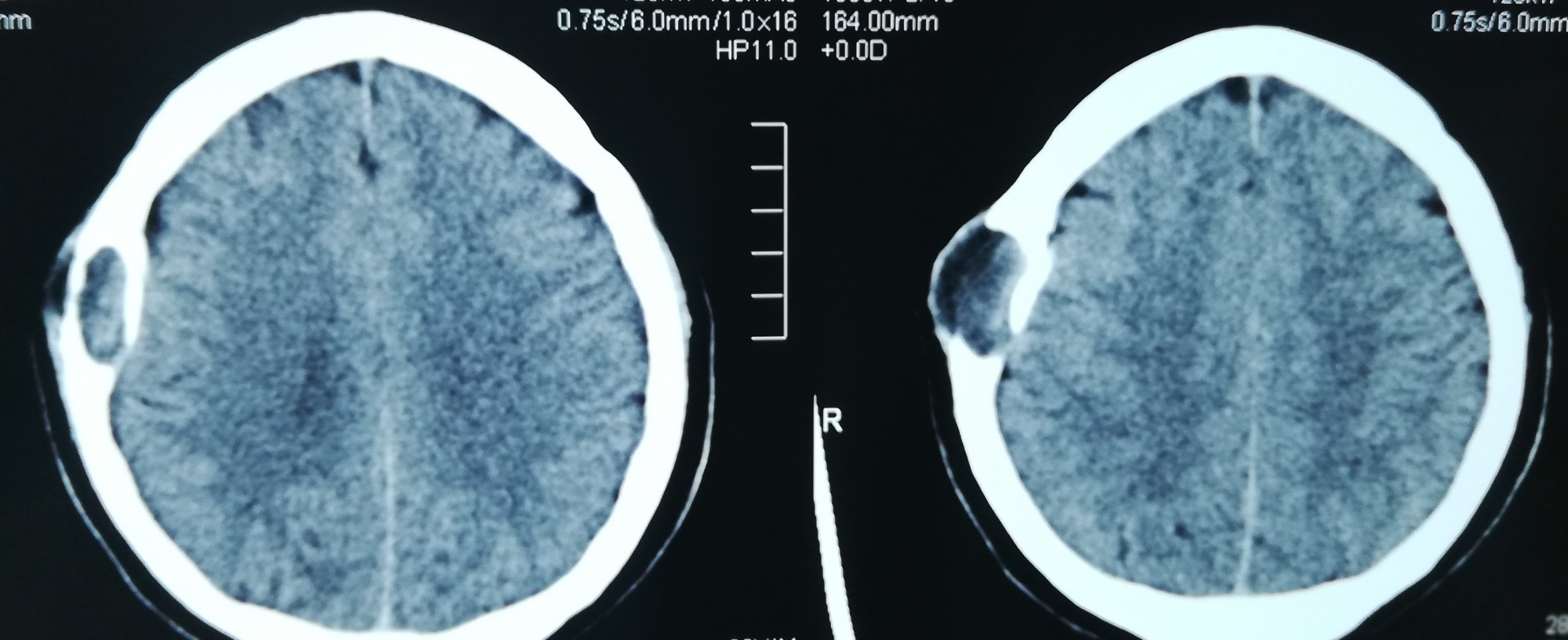
Skull bone
Prognostic factors
- Excellent prognosis
- Squamous cell carcinoma may very rarely arise in an epidermoid inclusion cyst; has been reported in the skull and finger (Neuroradiology 1999;41:570, Int J Surg Case Rep 2015;11:37)
Case reports
- 24 year old woman with an intraosseous epidermoid cyst of the skull (Dermatol Online J 2018;24:13030)
- 49 year old man with an epidermoid cyst of the anterior clinoid process (Clin Neurol Neurosurg 2021;200:106381)
- 63 year old woman with epidermal inclusion cyst of the fifth toe (Foot Ankle Spec 2017;10:470)
- 66 year old man with epidermal inclusion cyst of the knee (Eur J Orthop Surg Traumatol 2019;29:1355)
- 8 patients with intraosseous epidermoid cysts (J Hand Surg Eur Vol 2011;36:376)
Treatment
- Simple curettage or excision
Gross description
- Unilocular cyst filled with white to pale yellow, malodorous, cheesy material
Frozen section description
- Seldom required
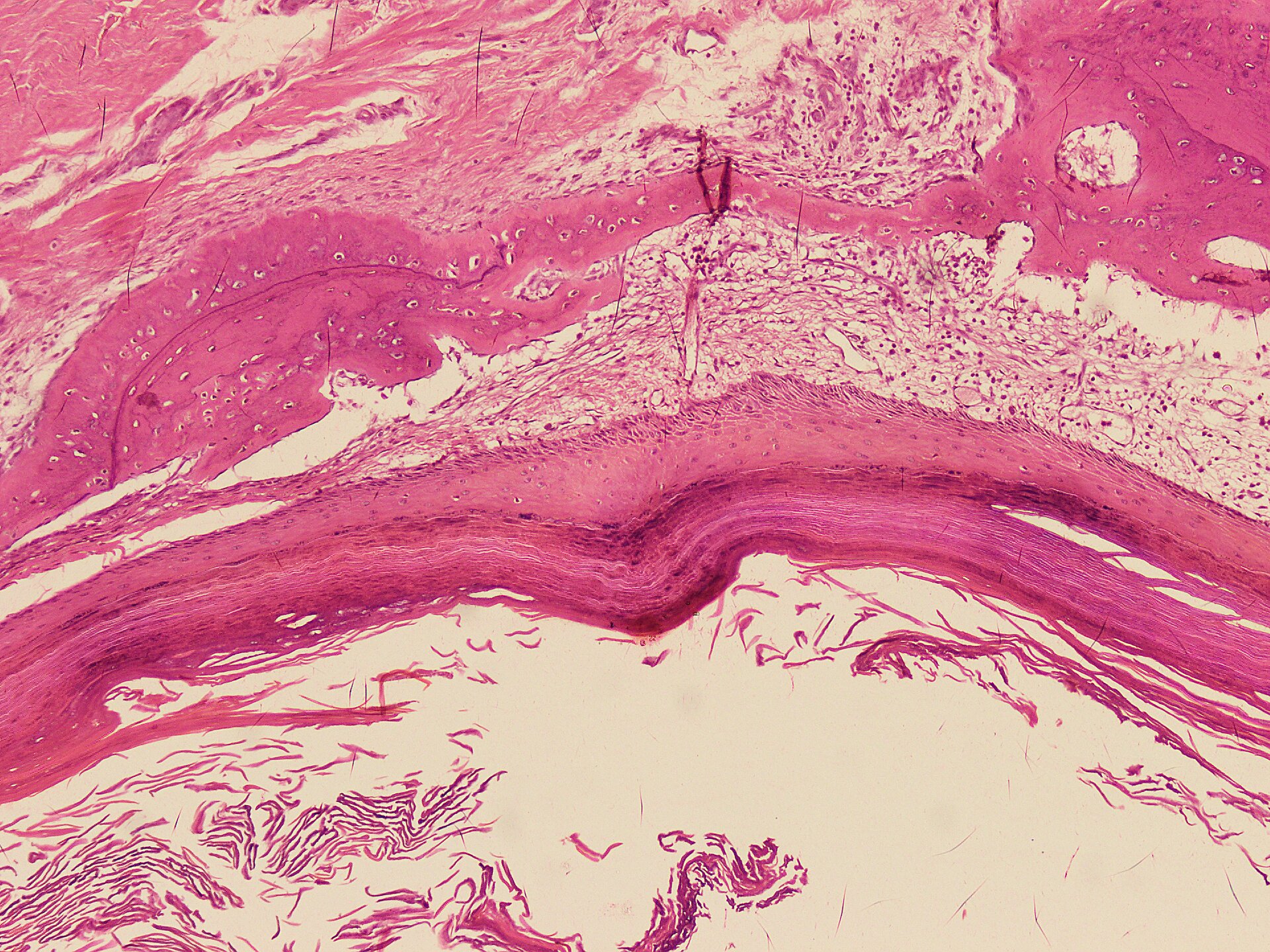
Microscopic (histologic) description
- Cyst is lined by squamous epithelium, including a granular layer
- Cyst wall is devoid of skin adnexal structures
- Cyst contents contain laminated keratin flakes
- Acute inflammation and foreign body type giant cell reaction may be present in the ruptured cyst
- Reference: Eur J Orthop Surg Traumatol 2019;29:1355
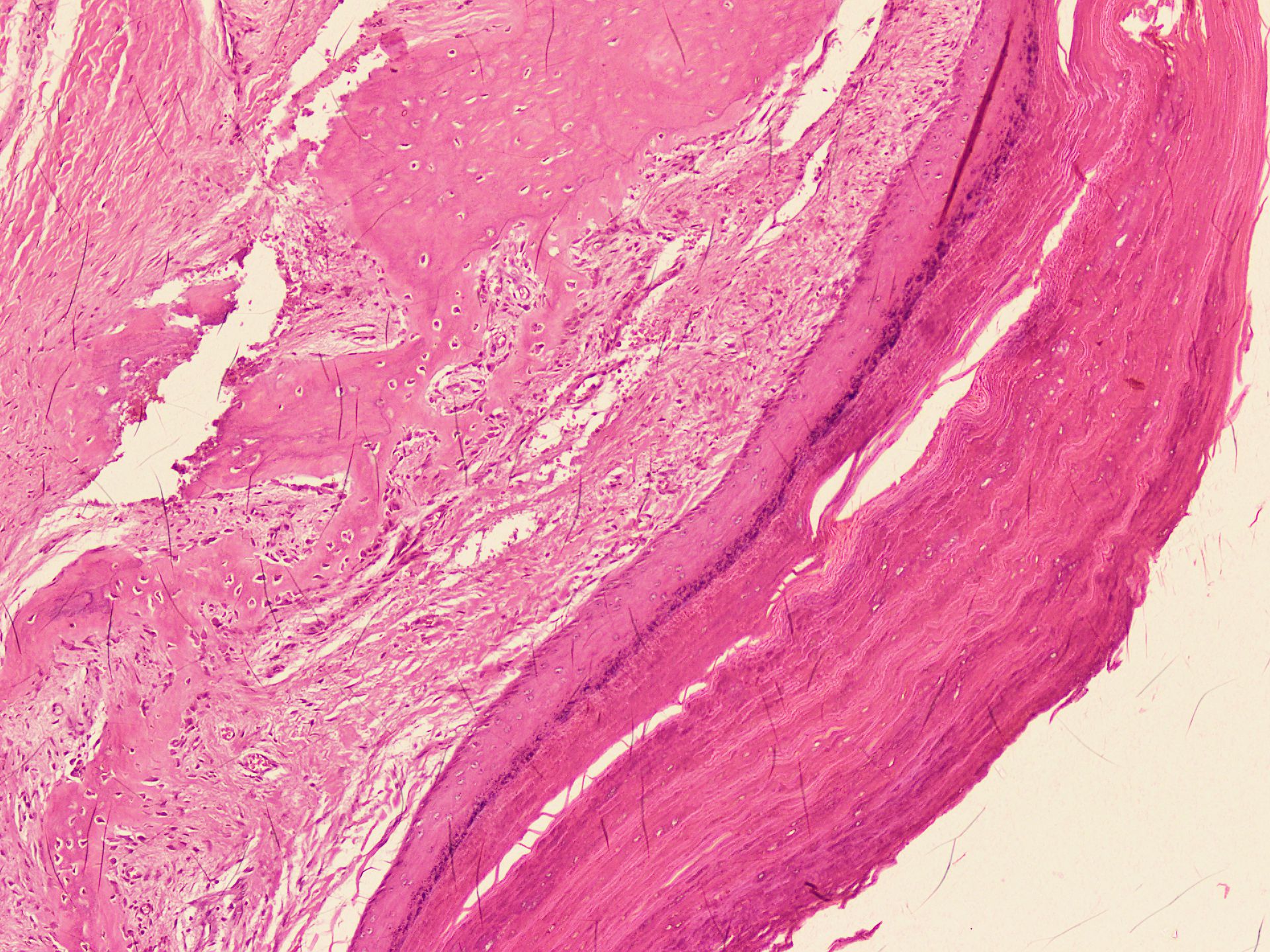
Microscopic (histologic) images
Contributed by Nasir Ud Din, M.B.B.S.
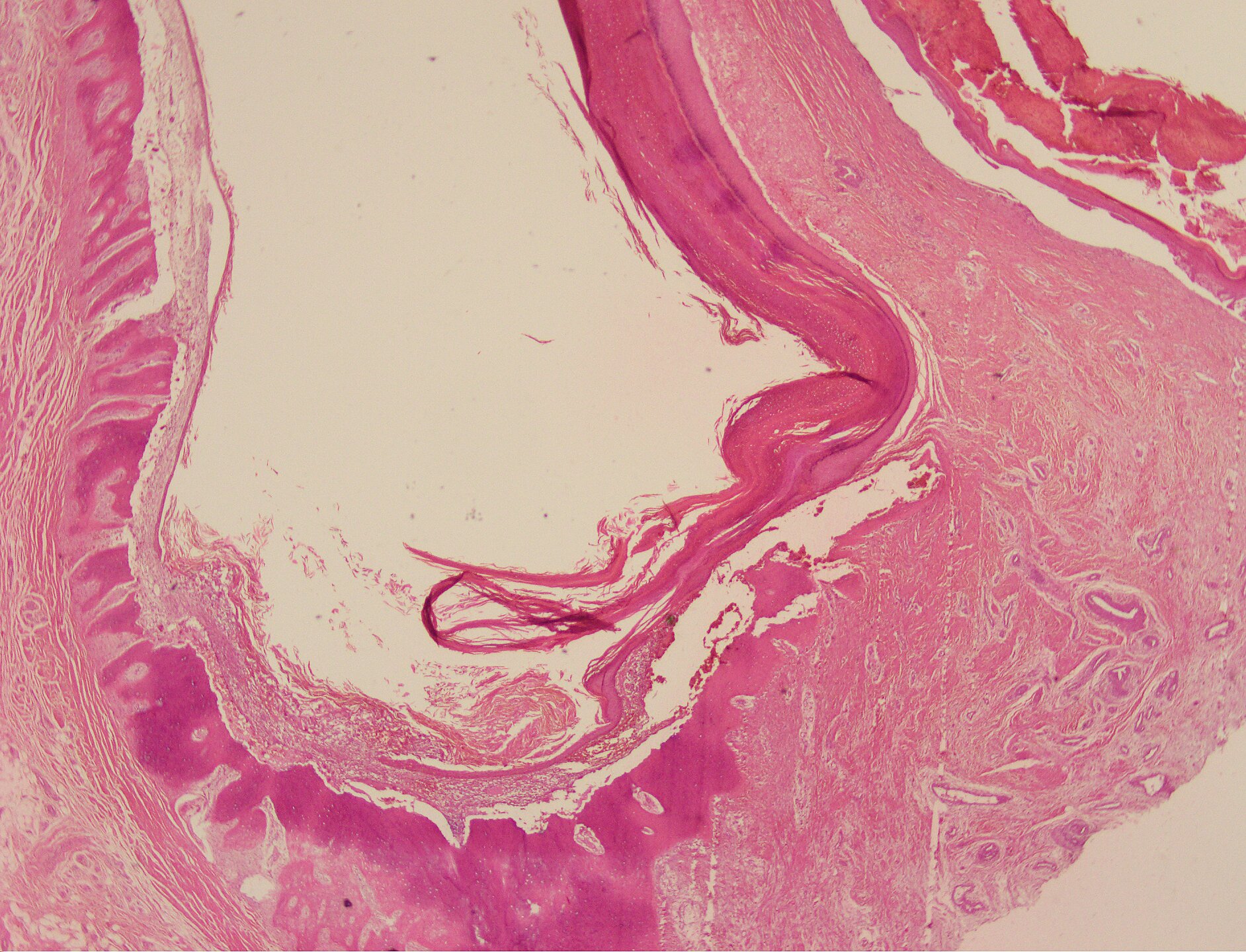
Absence of adnexal structures
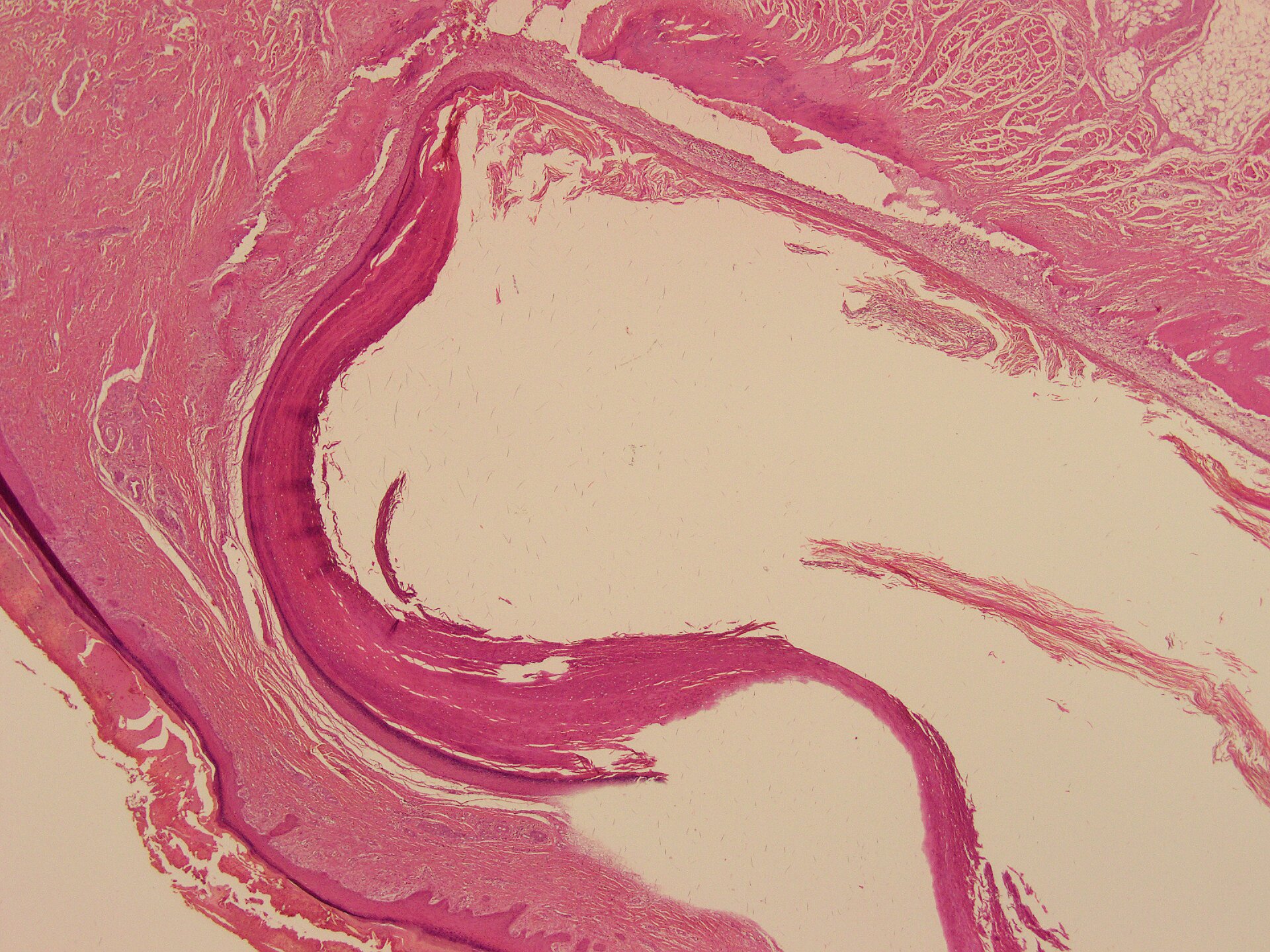
Keratin flakes in cystic cavity
Lamellated keratin
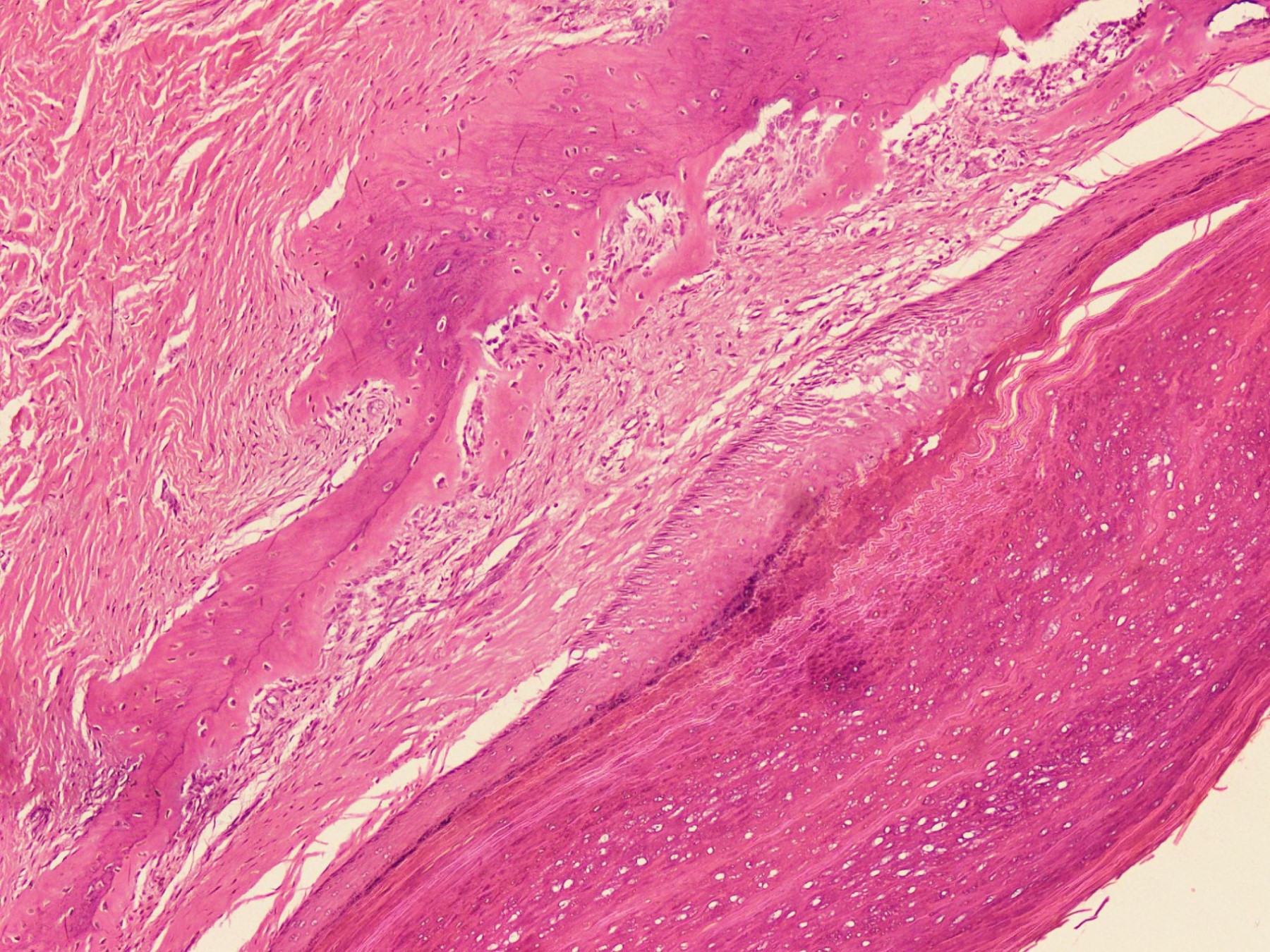
Squamous epithelium with granular layer
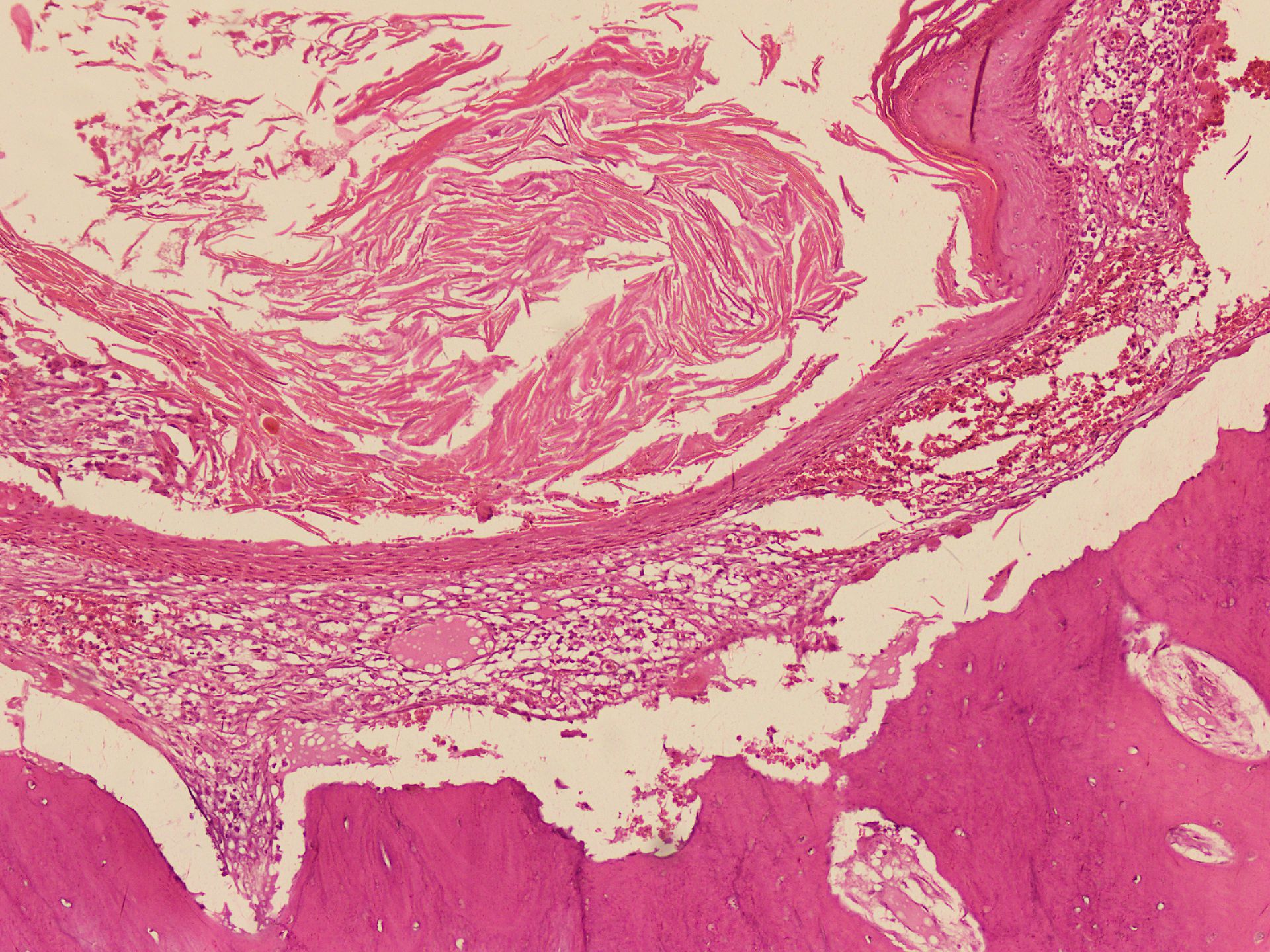
Reactive bone around the cyst
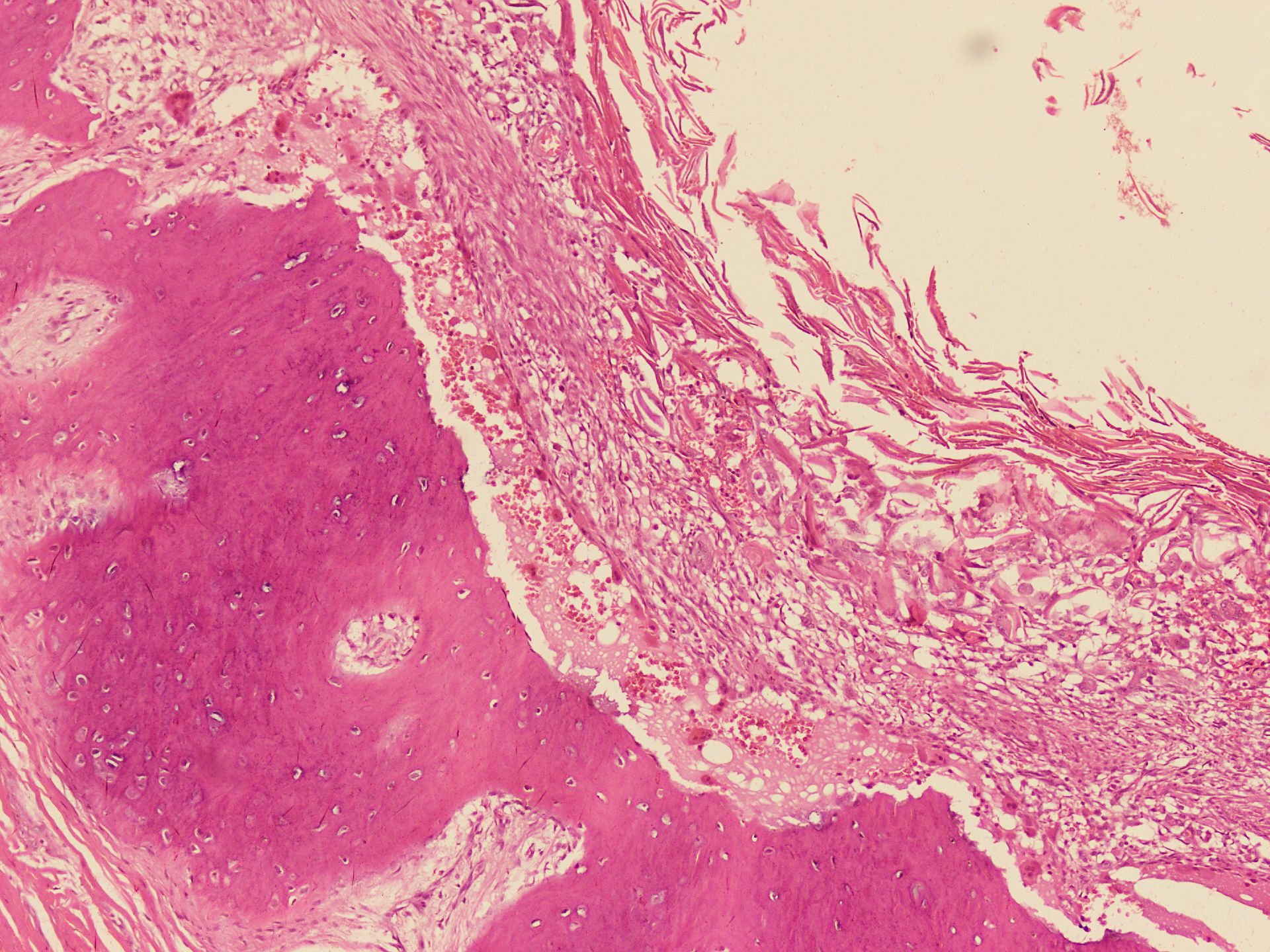
Chronic inflammation
Positive stains
- H&E diagnosis
Sample pathology report
- Bone, right fifth distal phalanx, excision:
- Epidermoid inclusion cyst
Differential diagnosis
- Dermoid cyst:
- Presence of skin appendages in the cyst wall
- Compact keratin
- Enchondroma:
- Included in the radiological differential diagnosis
- Histologically composed of hypocellular cartilaginous nodules
- Glomus tumor:
- Rare in bone
- Included in the radiological differential diagnosis
- Histologically uniform small round cells with eosinophilic cytoplasm, distinct cell borders
- Osteomyelitis:
- Clinically mimics epidermal inclusion cyst
- Infiltration of bone by inflammatory cells including neutrophils, lymphocytes, and plasma cells
- Bone erosion and necrosis
- Reactive bone formation
- Squamous cell carcinoma:
- Associated precursor lesions, such as actinic keratosis or squamous cell carcinoma in situ are often present
- Invasion of dermis by tumor
- Tumor is composed of dysplastic squamous cells and may show lack of normal maturation
- Moderate and poorly differentiated carcinoma show focal or no keratinization
Additional references
Board review style question #1

Which of the following is one of the morphological features of intraosseous epidermoid inclusion cyst?
- Cyst contents contain compact keratin
- Cyst wall lined by benign squamous epithelium including a granular layer
- It is a malignant neoplasm
- Presence of skin adnexal structures in the cyst wall
Board review style answer #1
B. Cyst wall lined by benign squamous epithelium including a granular layer. The presence of a granular layer in the squamous epithelium and lamellated keratin are the key features that differentiate the epidermoid inclusion cyst from the trichilemmal (pilar) cyst.
Comment Here
Reference: Epidermoid inclusion cyst
Comment Here
Reference: Epidermoid inclusion cyst
Board review style question #2
Which of the following morphological features differentiates dermoid cyst from epidermoid inclusion cyst?
- Benign squamous epithelium
- Chronic inflammation and fibrosis
- Overlying skin with dysplasia
- Presence of skin adnexal structures in the cyst wall
Board review style answer #2
D. Presence of skin adnexal structures in the cyst wall. Dermoid cyst differs from epidermoid inclusion cyst by the presence of skin appendages.
Comment Here
Reference: Epidermoid inclusion cyst
Comment Here
Reference: Epidermoid inclusion cyst

