

Bone & joints
Other chondrogenic tumors
Enchondroma
Author: Borislav A. Alexiev, M.D.
Editorial Board Members: Farres Obeidin, M.D., Josephine K. Dermawan, M.D., Ph.D.

Last author update: 10 July 2023
Last staff update: 10 July 2023
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: Enchondroma

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Alexiev B. Enchondroma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/bonechondromaenchondroma.html. Accessed December 28th, 2024.
Definition / general
- Enchondroma is a benign hyaline, cartilaginous tumor that arises within the medullary cavity of bone (Clin Orthop Relat Res 1985;201:214, Semin Diagn Pathol 2014;31:10)
Essential features
- Abundance of cartilaginous matrix (Skeletal Radiol 1997;26:325)
- Histology with typical encasement pattern (deposition of bone surrounding the tumor lobules, a sign of indolent growth) (Clin Orthop Relat Res 1985;201:214)
- Absence of cytological atypia, mitoses, cortical invasion and soft tissue extension
- Tumors arising in the small bones or in patients with enchondromatosis may show more cellularity and atypia
Terminology
- Not recommended: chondroma
ICD coding
- ICD-O: 9220/0 - enchondroma
- ICD-11: 2E83.Y & XH9SY5 - benign osteogenic tumor of other specified site & enchondroma
Epidemiology
- 20% of all cartilaginous tumors, second only to osteochondroma (30%) (Skeletal Radiol 1997;26:325)
- Most common in 20 - 50 year olds
- M:F = 1:1
- Enchondromatosis presents with multiple enchondromas; most common subtypes are Ollier disease and Maffucci syndrome (StatPearls: Enchondroma [Accessed 20 April 2023], Am J Med Genet A 2020;182:1093)
- Ollier disease: multiple enchondromas in the appendicular skeleton in an asymmetric manner
- Typically in short and long bones of the limbs; epiphyseal tumors can prevent normal bone growth in young patients
- Maffucci syndrome
- Multiple enchondromas in association with soft tissue and visceral hemangiomas and lymphangiomas
- Ollier disease: multiple enchondromas in the appendicular skeleton in an asymmetric manner
Sites
- Enchondromas are usually solitary, central and metaphyseal lesions of tubular bones, favoring the small bones of the hand and feet followed by the femur and humerus (StatPearls: Enchondroma [Accessed 20 April 2023], Skeletal Radiol 1997;26:325)
- Location in the flat bones is very uncommon
- Most common primary bone tumors of the hand
- In the hands, they most commonly involve the proximal phalanges
Pathophysiology
- Increased levels of D-2-hydroxyglutarate (D-2-HG) can be detected in cartilage tumors with an IDH1 or IDH2 mutation (Nat Genet 2011;43:1262)
- D-2-HG has been shown to promote chondrogenic and inhibit osteogenic differentiation of mesenchymal stem cells during skeletogenesis (Oncotarget 2015;6:14832, PLoS One 2015;10:e0131998)
Etiology
- Heterozygous somatic mutations in the IDH1 and IDH2 genes
- Found in 40% of sporadic enchondromas and in ~80% of enchondromas in patients with Ollier disease and Maffucci syndrome (Nat Genet 2011;43:1256)
- Mutant PTH / PTHrP type I receptor account for rare cases of enchondromatosis (Nat Genet 2002;30:306)
Clinical features
- Most common presenting symptoms are pain, swelling and deformity
- Pathologic fractures can be seen in 40 - 60% of patients at presentation (J Hand Surg Am 2012;37:1229, Hand (N Y) 2015;10:461)
- Many are ultimately found incidentally on radiographic imaging
Diagnosis
- Coordination between radiologists, oncologists, pathologists, surgeons and the primary medical team is needed to arrive at the diagnosis of an enchondroma (StatPearls: Enchondroma [Accessed 20 April 2023])
- Decisive point of an enchondroma diagnosis is differentiating enchondroma from atypical cartilaginous tumor / chondrosarcoma grade 1 (ACT / CS1)
- Combination of nonaggressive radiology and histology with indolent growth and no bone permeation
Radiology description
- Enchondromas typically appear as well defined, solitary defects in the metaphyseal region of bones, especially in the long bones (StatPearls: Enchondroma [Accessed 20 April 2023])
- Their appearance depends heavily on the location and extent of the calcification of the tumor
- Radiographically visible calcifications appear as fine, punctate stippling
- Larger lesions can cause endosteal scalloping along with expansion and thinning of the cortex
- Heavily calcified lesions may resemble bone infarct or bone islands, while an uncalcified lesion may appear lytic
- Computed tomography (CT) is useful for detecting matrix mineralization and cortex integrity, while magnetic resonance imaging (MRI) adds insight into the aggressive and destructive features of the tumor (Indian J Radiol Imaging 2021;31:582)
- Progressive destruction of the chondrite matrix by an expanding, non mineralized component, an enlarging lesion associated with pain or an expansile soft tissue mass is strongly associated with the malignant transformation of an enchondroma (Indian J Radiol Imaging 2021;31:582)
Radiology images
Contributed by Borislav A. Alexiev, M.D. and Terrance D. Peabody, M.D.

Left thumb Xray

Right index finger Xray
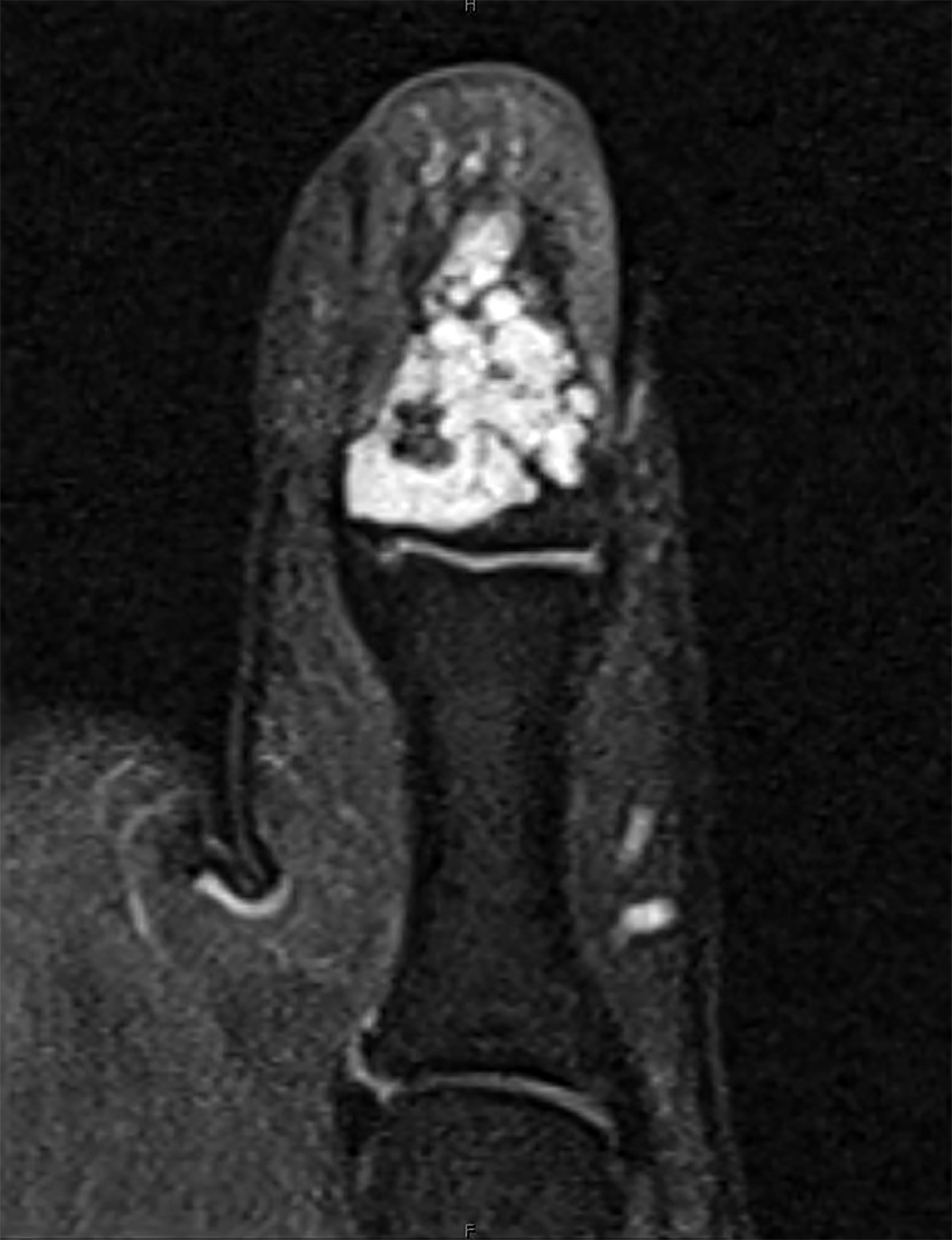
Left thumb MRI
Images hosted on other servers:

Ollier disease
Prognostic factors
- Asymptomatic enchondromas can be followed clinically and do not need to be treated (StatPearls: Enchondroma [Accessed 20 April 2023])
- Longstanding enchondromas identified radiologically have been shown to progress
- Malignant transformation is rare in a nonsyndromic setting (< 1%)
- Malignant transformation to chondrosarcoma is a major complication of enchondromatosis (Ollier disease and Maffucci syndrome) (J Clin Diagn Res 2016;10:TD01)
- Risk of malignant transformation is up to 45.8% in patients with Ollier disease and 57% in patients with Maffucci syndrome, respectively (Neoplasma 2014;61:365)
Case reports
- 17 year old boy presented with enchondroma of the left great toe (Cureus 2022;14:e21772)
- 18 year old woman with Mafucci syndrome and a cranial base chondrosarcoma (Neurosurgery 1997;41:269)
- 52 year old woman with enchondroma of anterior maxilla (Cureus 2022;14:e32834)
- 54 year old woman with Ollier disease and nasal enchondroma (Head Neck 2015;37:E30)
- 66 year old man with enchondroma of the left hand (Case Reports Plast Surg Hand Surg 2022;9:179)
Treatment
- Management of symptomatic enchondroma lesions typically involves surgical management in the form of simple curettage with bone grafting (StatPearls: Enchondroma [Accessed 20 April 2023])
- Asymptomatic enchondromas can be observed (J Am Acad Orthop Surg 2016;24:625)
Gross description
- If treated with curettage, the specimen is usually received in fragments
- Tissue fragments contain bluish white glistening cartilage tissue admixed with medullary bone
- Resection specimens are uncommon and demonstrate a well marginated, often multinodular, whitish blue or whitish yellow tumor in the medullary cavity of the bone, with intact cortex (see Additional references section)
Gross images
Contributed by Borislav A. Alexiev, M.D. and Mark R. Wick, M.D.

First rib lesion
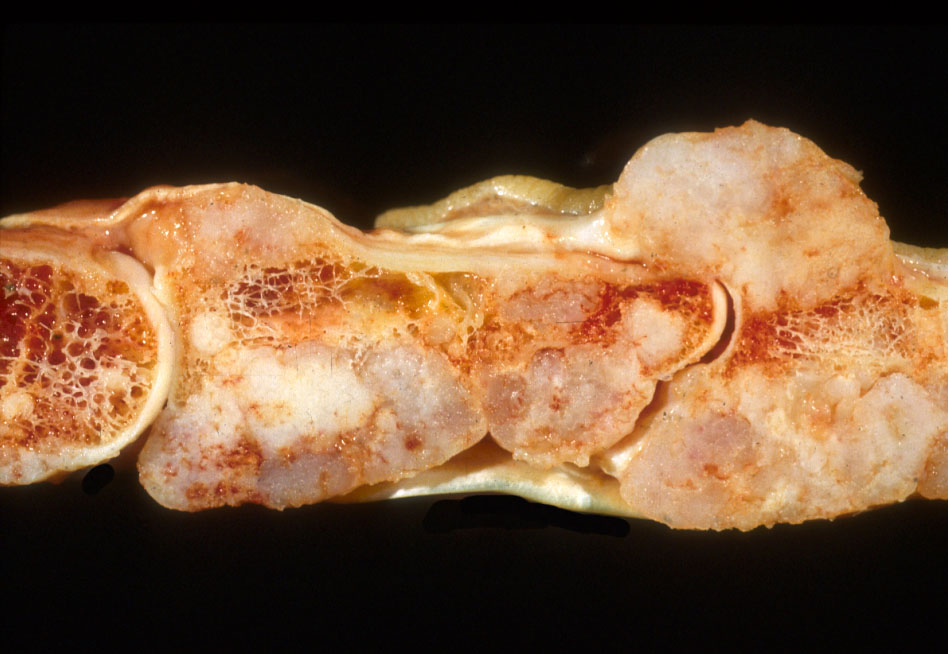
Multifocal in Ollier disease
Microscopic (histologic) description
- Enchondromas are hypocellular, with an abundance of hyaline cartilage matrix (Clin Orthop Relat Res 1985;201:214, Semin Diagn Pathol 2014;31:10)
- Tumor cells are embedded within lacunar spaces and evenly dispersed
- Nuclei are small and round, with condensed chromatin (lymphocyte-like)
- Cytoplasm is eosinophilic
- Architecture can be multinodular or confluent
- Separate cartilaginous nodules can be surrounded by bone, which is referred to as encasement (a sign of slow growth)
- Normal bone marrow can be present between the cartilaginous nodules
- Cytologic atypia and mitoses are absent
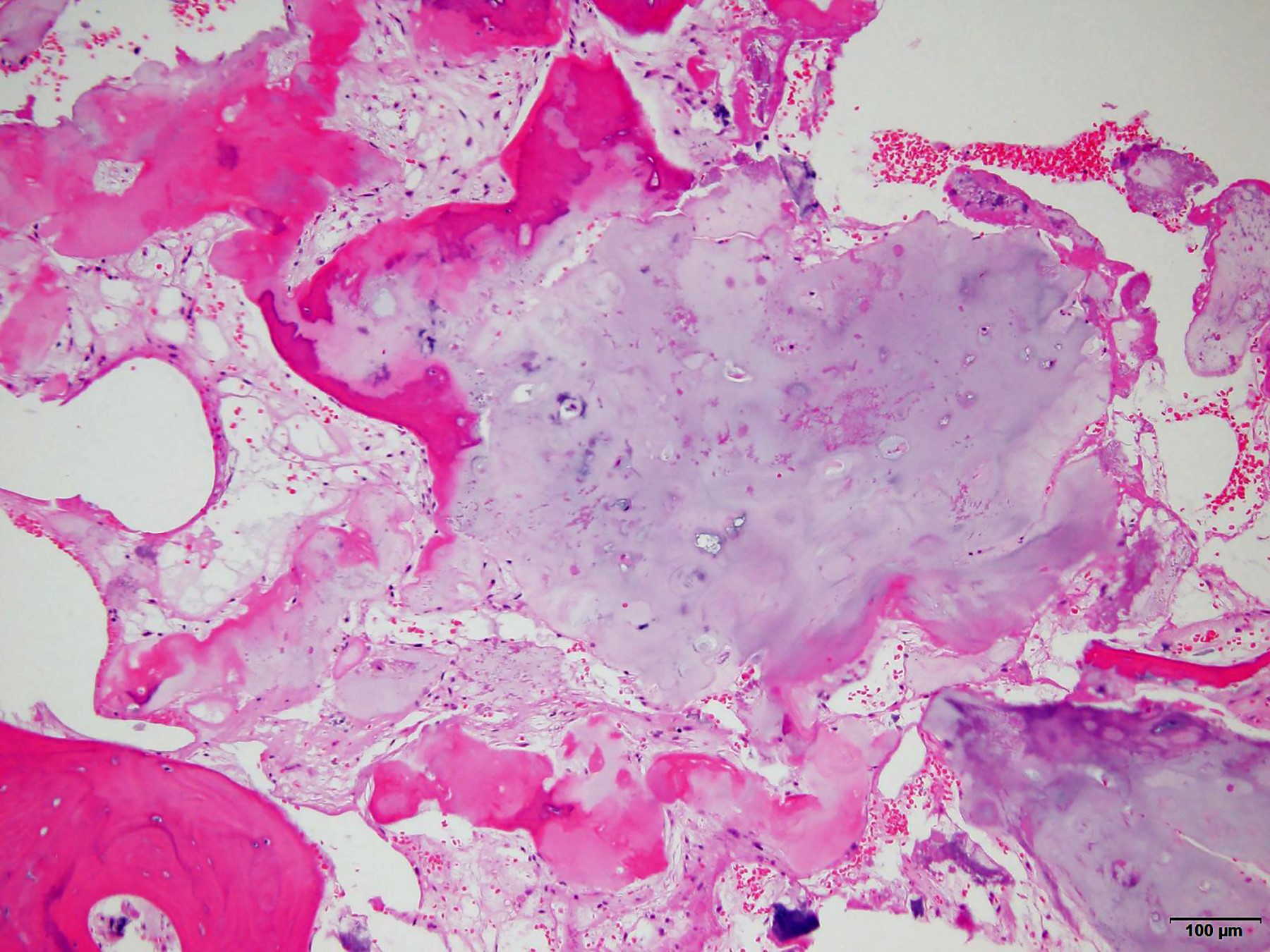
- Degenerative changes, such as ischemic necrosis or calcification, can be prominent
- In the small phalangeal bones and in patients with enchondromatosis, enchondromas can be much more cellular and the tumor cells occasionally have more open chromatin and small nucleoli; binucleated cells can seen
- Enchondromas do not invade and destroy the cortex, entrap pre-existing lamellar bone or extend into soft tissue (see Additional references section)
Microscopic (histologic) images
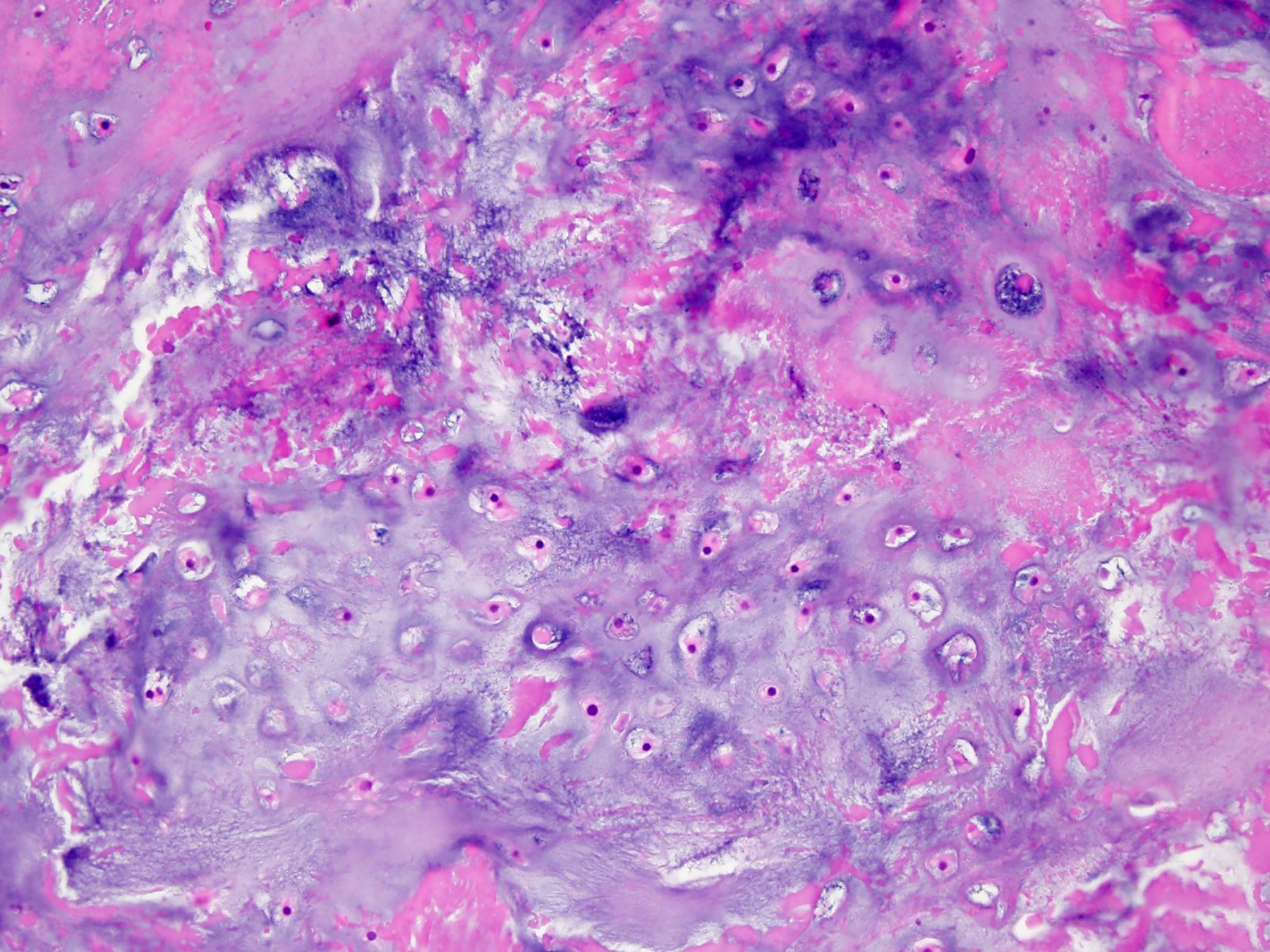
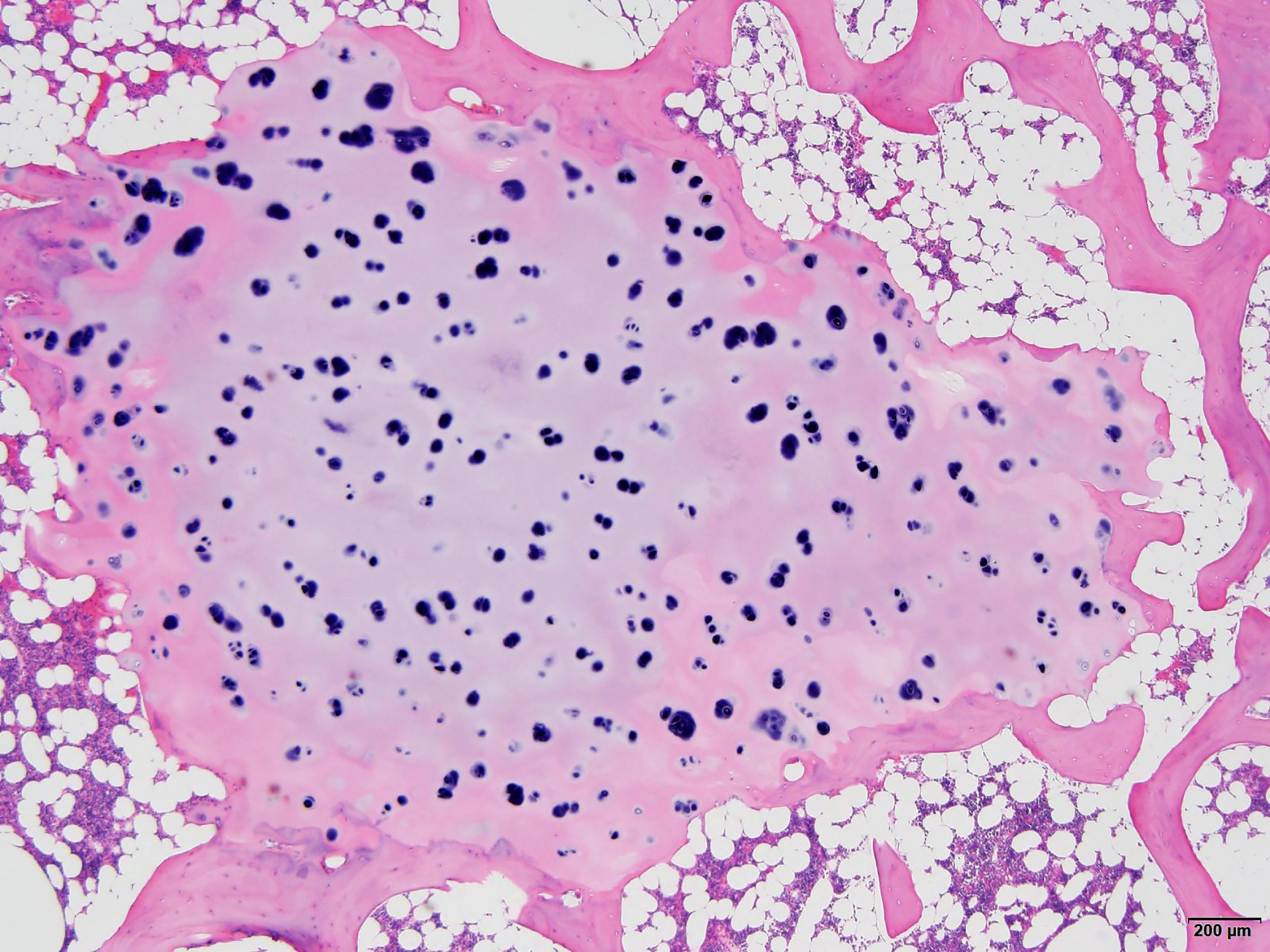
Contributed by Borislav A. Alexiev, M.D.
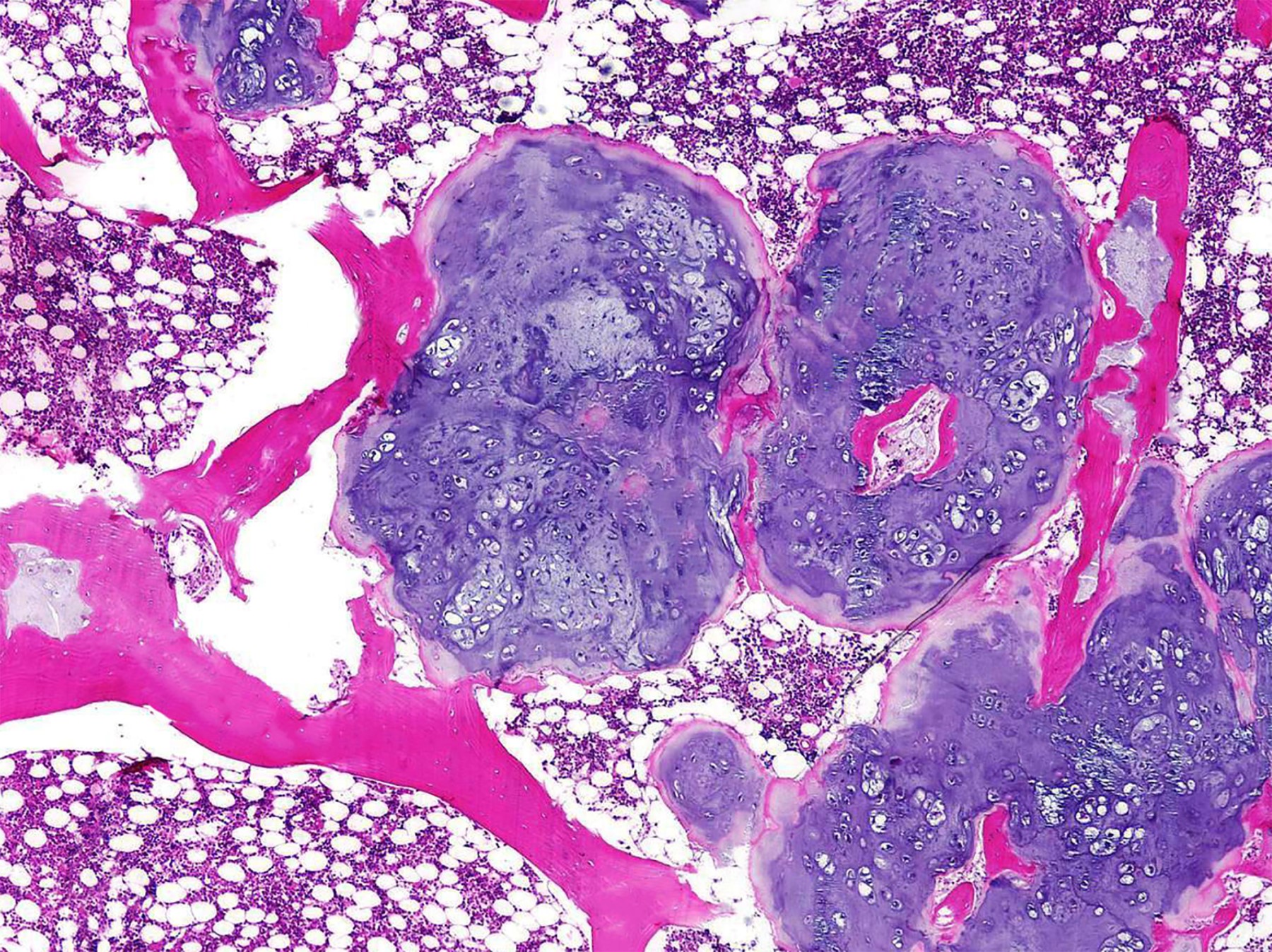
Intramedullary lesion
Hypocellular lesion
Chondrocytes in lacunar spaces

Short tubular bone lesion
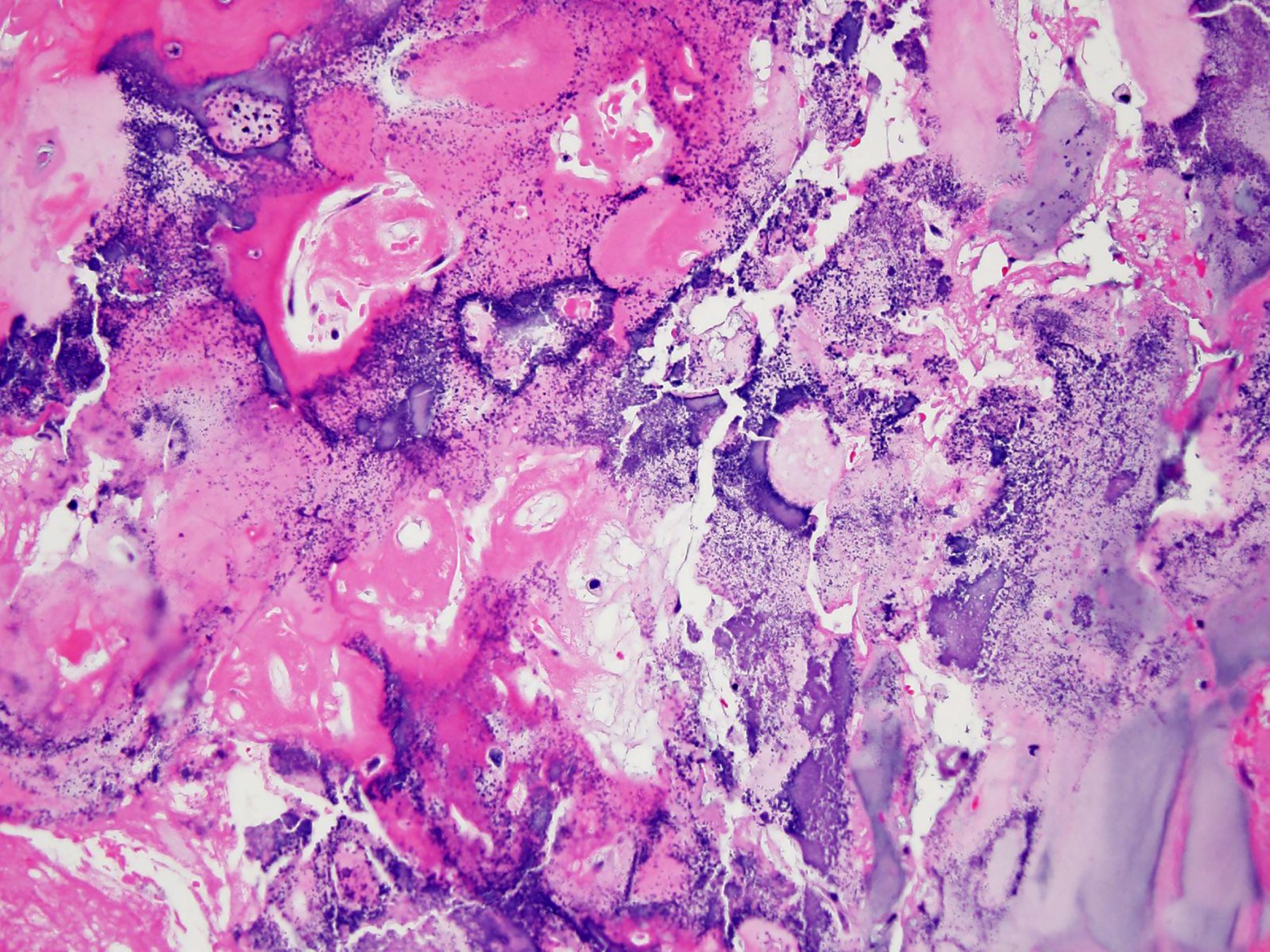
Degenerative changes
Positive stains
Negative stains
Molecular / cytogenetics description
- Molecular pathology is rarely used for diagnosis
- Hotspot mutations are exclusively found at the IDH1 p.Arg132 and the IDH2 p.Arg172 positions (Nat Genet 2011;43:1256)
- Mutation analysis cannot be used to distinguish enchondroma from ACT / CS1
Sample pathology report
- Left fourth distal phalanx lesion, curettage:
- Fragments of benign cartilaginous tissue consistent with enchondroma (see comment)
- Comment: The patient is a 27 year old woman with left ring finger distal phalanx lesion with imaging characteristics suggestive of a chondroid lesion measuring 0.3 x 0.5 x 0.9 cm. The lesion is confined to the medullary space. Histologically, the lesion is hypocellular, with an abundance of hyaline cartilage matrix and is composed of separate cartilaginous nodules encased by thin mantles of bone. Normal bone marrow is seen between the nodules. The tumor cells are situated within sharped edged lacunar spaces and evenly distributed. The nuclei are small and round, with condensed chromatin (lymphocyte-like). The cytoplasm is clear or eosinophilic. Cytological atypia and mitoses are absent. There is no cortical destruction, entrapment of host lamellar bone and soft tissue extension. Overall, these findings are most consistent with enchondroma. Enchondroma is a benign cartilaginous neoplasm. Malignant transformation is rare (< 1%) in a nonsyndromic setting.
Differential diagnosis
- Central atypical cartilaginous tumor / chondrosarcoma, grade 1 (ACT / CS1):
- Distinction between enchondroma and ACT / CS1 can be difficult and is subject to interobserver variability (AJR Am J Roentgenol 1997;169:1097, Clin Orthop Relat Res 1985;201:214)
- Multidisciplinary approach with clinicoradiological correlation is often indispensable
- Combination of 5 parameters (high cellularity, host bone entrapment, open chromatin, mucoid matrix degeneration > 20% and patient age > 45 years) is helpful in differentiating between enchondromas and central ACT / CS1 (Am J Surg Pathol 2009;33:50)
- In the phalanges, the main discriminatory factors in distinguishing chondrosarcoma from enchondroma are the presence of mitoses, cortical breakthrough, soft tissue involvement and host lamellar bone entrapment (Cancer 1999;86:1724)
Additional references
Board review style question #1
A 40 year old man presented with a bubbly appearing lytic lesion involving most of the distal phalanx of the left thumb. The lesion is mildly expansile without evidence of frank cortical breakthrough or extraosseous soft tissue extension. Hematoxylin eosin stains demonstrate a lesion with multinodular architectural pattern characterized by islands of hyaline cartilage encased by thin mantles of bone that are separated by marrow. The tumor cells are situated within sharped edged lacunar spaces and are evenly distributed. The nuclei are small and round, with condensed chromatin (lymphocyte-like). The cytoplasm is eosinophilic. Cytological atypia and mitoses are absent. There is no cortical destruction, entrapment of host lamellar bone and soft tissue extension. Which of the following is most likely the correct diagnosis?
- Central atypical cartilaginous tumor / chondrosarcoma, grade 1
- Chondromyxoid fibroma
- Clear cell chondrosarcoma
- Enchondroma
- Osteochondroma
Board review style answer #1
D. Enchondroma. Enchondroma is located in the medullary cavity and is composed of separate nodules encased by thin mantels of bone, which is a sign of slow growth. Answer A is incorrect because there is no cortical destruction, soft tissue extension and entrapment of pre-existing lamellar bone (i.e., features of more aggressive behavior indicative of central atypical cartilaginous tumor / chondrosarcoma, grade 1). Answer B is incorrect because chondromyxoid fibroma demonstrates a zonal architecture and is composed of chondroid, myxoid and myofibroblastic areas. Answer C is incorrect because clear cell chondrosarcoma involves the epiphysis of a long bone and consists of tumor cells with abundant clear cytoplasm. Infiltrative growth can be seen. Answer E is incorrect because osteochondroma consists of a bony projection covered by a cartilaginous cap, arising at the external surface of bone and containing a marrow cavity that is continuous with that of the underlying bone.
Comment Here
Reference: Enchondroma
Comment Here
Reference: Enchondroma
Board review style question #2
Which of the following is true about enchondroma?
- Deposition of bone surrounding the tumor nodules is a sign of indolent growth
- Enchondromas most commonly affect flat bones
- Immunohistochemistry is usually helpful in the diagnosis
- Malignant transformation is frequent in a nonsyndromic setting
- Mutation analysis can be used to distinguish enchondroma from ACT / CS1
Board review style answer #2
A. Deposition of bone surrounding the tumor nodules is a sign of indolent growth. Answer B is incorrect because location in the flat bones is very uncommon. Answer C is incorrect because Immunohistochemistry is not helpful in the diagnosis. Answer D is incorrect because malignant transformation is rare (< 1%) in nonsyndromic setting. Answer E is incorrect because mutation analysis cannot be used to distinguish enchondroma from ACT / CS1.
Comment Here
Reference: Enchondroma
Comment Here
Reference: Enchondroma

