

Bone & joints
Other chondrogenic tumors
Periosteal chondroma
Editorial Board Member: Nasir Ud Din, M.B.B.S.
Deputy Editor-in-Chief: Borislav A. Alexiev, M.D.

Last author update: 3 March 2022
Last staff update: 3 March 2022
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: Periosteal chondroma [TI]

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Frozen section description | Microscopic (histologic) description | Microscopic (histologic) images | Virtual slides | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Shaker N, Qasem S. Periosteal chondroma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/bonechondroma.html. Accessed December 25th, 2024.
Definition / general
- Rare benign cartilaginous neoplasm that arises on the surface of cortical bone beneath periosteum
Essential features
- Children and young adults
- Well defined dome shaped lesion on the surface of the bone
- Composed of benign hyaline cartilage
- No connection with medullary cavity (radiologically)
Terminology
- Juxtacortical chondroma, subperiosteal chondroma
ICD coding
- ICD-O: 9221/0 - periosteal chondroma
- ICD-11: 2E82 & XH3BC3 - benign chondrogenic tumors & periosteal chondroma
Epidemiology
- < 2% of all chondromas
- Affects children and young adults, predominantly < 30 years of age (Oncol Lett 2015;9:1637)
- M:F = 1.5:1
Sites
- Small bones of the hands and long bones of the skeleton, particularly proximal metaphyseal or diaphyseal regions of humerus and femur (Oncol Lett 2015;9:1637)
Pathophysiology
- A subset of periosteal chondromas harbor mutations in one of the IDH genes (J Pathol 2011;224:334)
- Other cytogenetic abnormalities have been reported
Etiology
- Unknown
Clinical features
- Usually small; < 3 cm in diameter (Case Rep Orthop 2014;2014:763480)
- Typically painless, may cause swelling / palpable mass
Diagnosis
- Depends greatly on radiologic features
Radiology description
- Sharply defined juxtacortical mass
- Contains popcorn or ring-like calcifications, characteristic of cartilaginous tumors
- Plain radiographs may show a discernible soft tissue mass with underlying cortical saucerization or scalloping, subjacent cortical sclerosis and overhanging margins
- CT may be helpful in identifying the presence of scattered calcification and the lack of intramedullary extension (Case Rep Orthop 2014;2014:763480)
- On MRI, periosteal chondroma typically appears as a well circumscribed juxtacortical mass with intermediate signal intensity on T1 weighted images and high signal intensity on T2 weighted images (Case Rep Orthop 2014;2014:763480)
Radiology images
Contributed by Shadi Qasem, M.D., M.B.A.

Xray of distal femur lesion

CT scan of distal femur lesion

Proximal tibia lesion
Prognostic factors
- Benign tumor with a reported recurrence rate of 3.6% (Oncol Lett 2015;9:1637)
Case reports
- 12 year old girl with a swelling in the chest wall (Indian J Thorac Cardiovasc Surg 2019;35:101)
- 39 year old man with a pelvic mass (Int J Burns Trauma 2020;10:174)
- 54 year old woman presented with difficulty ambulating and worsening cognition (Cureus 2018;10:e2099)
- 55 year old woman with neck pain (Cureus 2019;11:e4523)
- 56 year old man with a painless swelling above the left clavicle (Int J Surg 2009;7:140)
Treatment
- Surgical management in the form of intralesional, marginal or en bloc resection, is the mainstay of therapy
- Marginal excision and curettage are preferable options if the diagnosis is certain prior to surgery (Oncol Lett 2015;9:1637)
Gross description
- Well defined, waxy blue-gray
- Size: < 5 cm
- Focal calcification and lobulation (Am J Surg Pathol 1982;6:631)
- Bone buttressing at the lateral edge but no medullary invasion
Gross images
Contributed by Shadi Qasem, M.D., M.B.A. and Mark R. Wick, M.D.

Marginal resection specimen
%20type%20gross.jpg)
Wide resection specimen
Frozen section description
- These lesions are typically sent for frozen section; frozen section would show mature hyaline cartilage
Microscopic (histologic) description
- Well demarcated from the underlying sclerotic bone, which may be focally eroded but never permeated
- Lobular architecture
- Covered by a continuous layer of attenuated periosteum
- Cellularity is variable but generally low
- Chondrocytes do not show cytologic atypia
- Occasionally, some tumors are more cellular and exhibit a greater degree of nuclear pleomorphism, including spindling and binucleation
- Invasion of surrounding soft tissue or medullary canal is not seen
Microscopic (histologic) images
Contributed by Shadi Qasem, M.D., M.B.A.
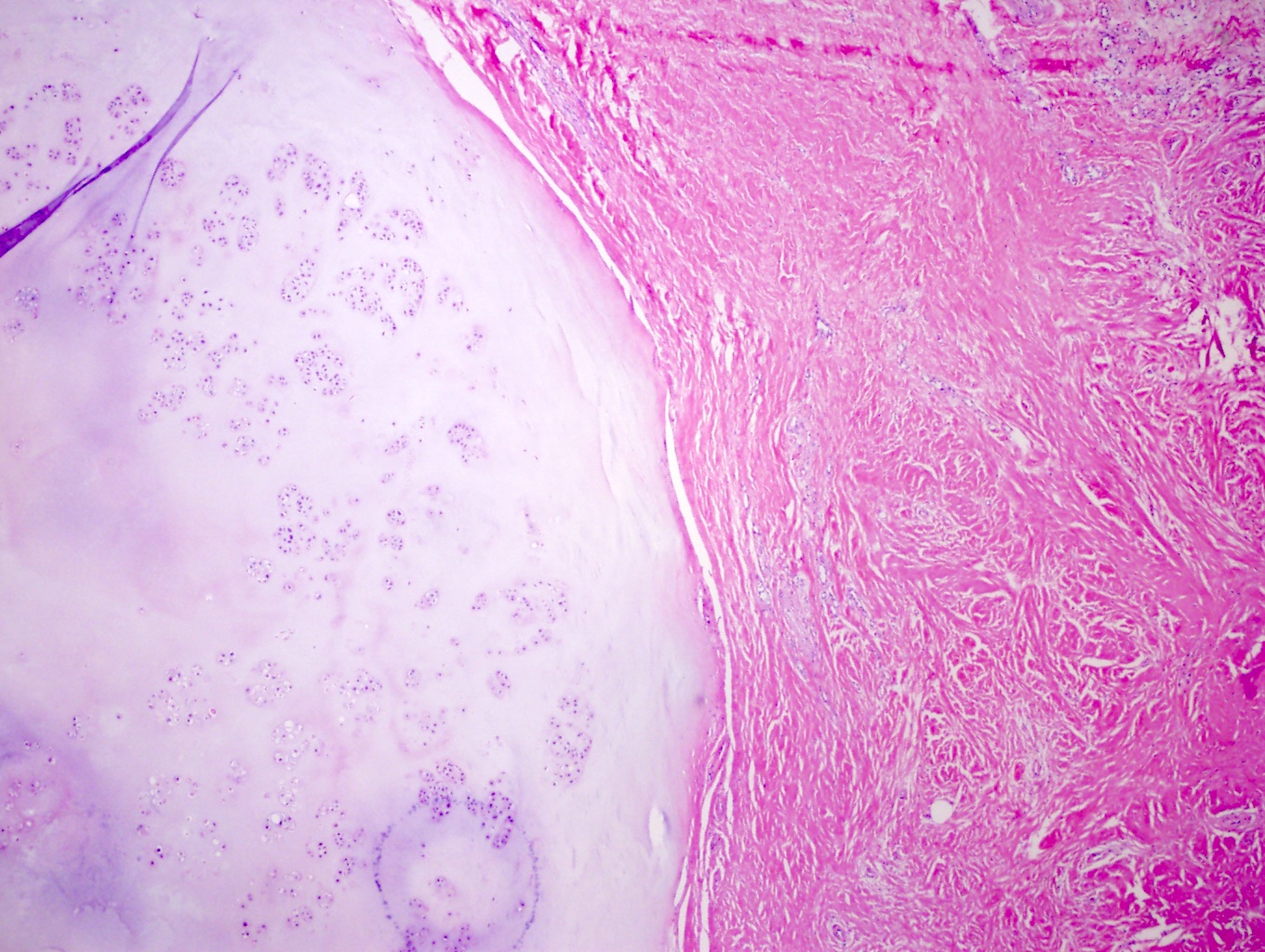
Well defined margin
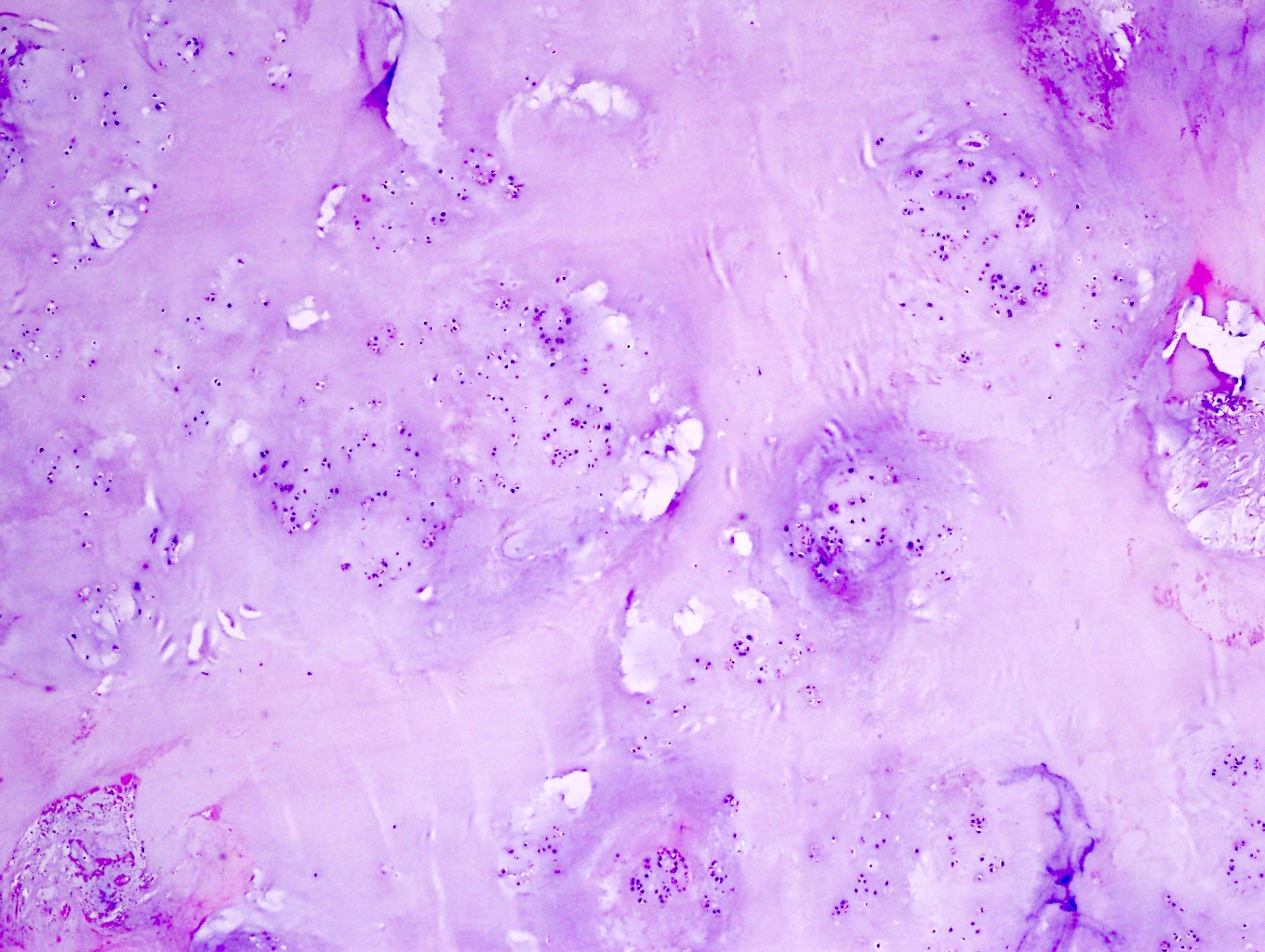
Low cellularity
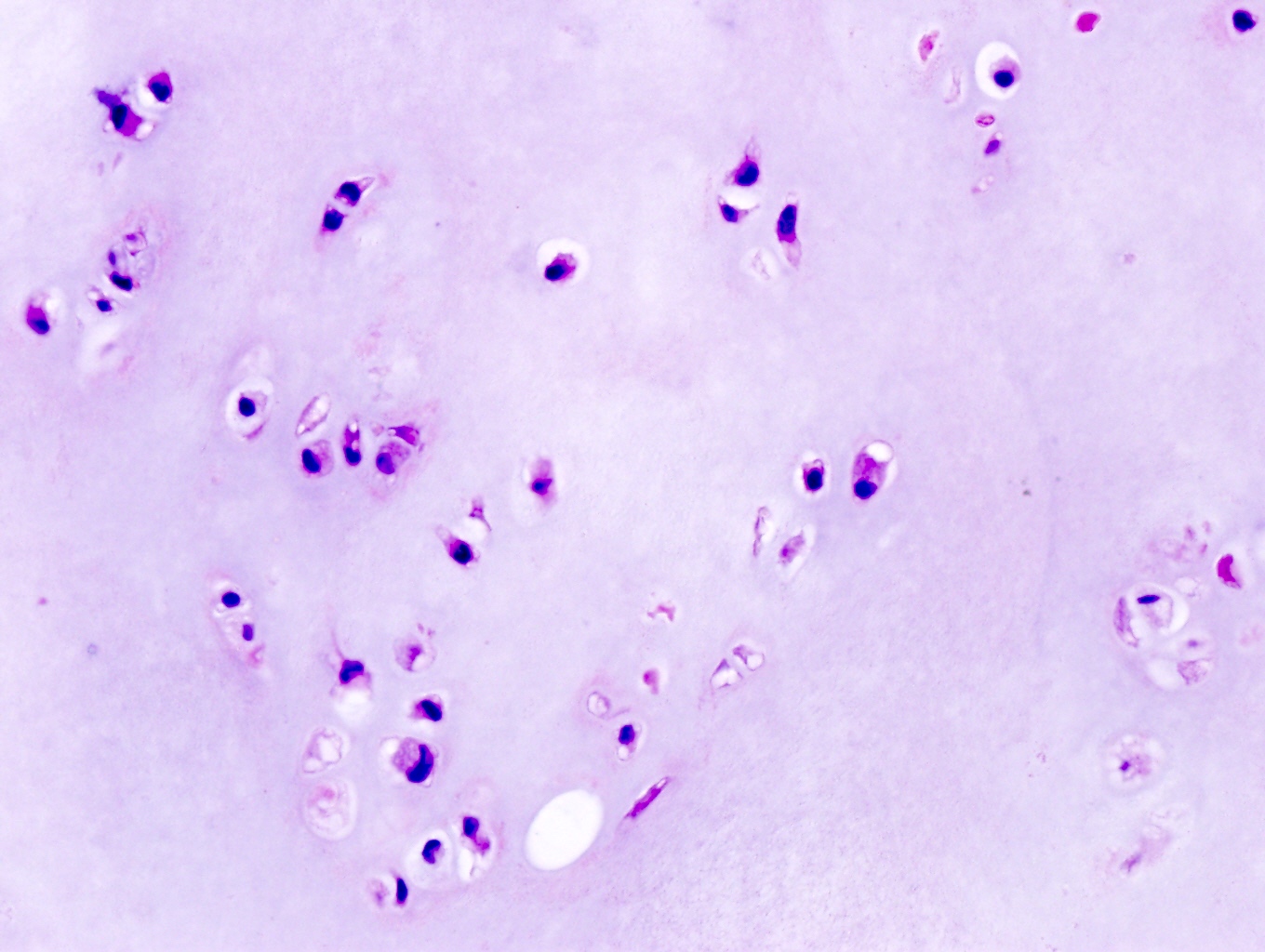
No significant atypia
Virtual slides
Images hosted on other servers:

Juxtacortical chondroma in Ollier disease
Molecular / cytogenetics description
- IDH1 and IDH2 mutations have been identified in periosteal chondromas (Am J Surg Pathol 1982;6:631)
- No consistent cytogenetic abnormality has been reported
Sample pathology report
- Humerus, excision:
- Periosteal chondroma (see comment)
- Comment: The diagnosis is made in concert with radiologic findings.
Differential diagnosis
- Periosteal chondrosarcoma:
- Favored: if tumor size > 5 cm
- Definitive diagnosis: presence of invasion into haversian system in addition to radiologic findings of a destructive bone lesion
- Periosteal osteosarcoma:
- Radiology: lucent, fusiform mass on the surface of bone, with variable mineralization; the cortex is thickened with periosteal reaction
- Histology: poorly delineated lobules of atypical cartilage with intervening bands of primitive sarcomatous cells and neoplastic bone formation
- Parosteal osteosarcoma:
- Radiology: mineralized, lobular mass at the bone surface; the underlying cortex may be normal, thickened or destroyed
- Histology: well formed bone trabeculae with intervening fascicles of spindle cells with minimal atypia and low mitotic activity
- MDM2 amplification
- Bizarre parosteal osteochondromatous proliferation:
- Radiology: well circumscribed calcified mass on the cortical surface
- Histology: disorganized cellular lesion composed of spindle cells, atypical chondrocytes and bone; the presence of blue bone is characteristic
- Periosteal chondromyxoid fibroma:
- Radiology: often multilobated with prominent calcifications
- Histology: myxoid stroma with stellate cells
- Soft tissue chondroma:
- Radiology: well demarcated, separated from the bone and has calcifications
- Histology: nodules of well delineated cartilage, matrix is hyaline or myxoid and may calcify; chondrocytes show limited atypia and little mitotic activity
Additional references
Board review style question #1
A 17 year old boy had a distal femur lesion (see images above). Which of the following is true regarding this lesion?
- Connection with bone marrow is a key feature
- IDH mutation is diagnostic
- Often presents with intense localized pain, relieved by aspirin
- Radiology review is essential for diagnosis
Board review style answer #1
Board review style question #2
Which of the following is true for periosteal chondroma?
- Bone buttressing is characteristic on gross examination
- En bloc resection is the preferred therapy
- Molecular testing is helpful for differentiating this lesion from chondrosarcoma
- Tumor size > 5 cm is not unusual
Board review style answer #2
A. Bone buttressing is characteristic on gross examination
Comment Here
Reference: Periosteal chondroma
Comment Here
Reference: Periosteal chondroma

