

Bladder & urothelial tract
Urothelial carcinoma - invasive
Invasive urothelial carcinoma


Copyright: 2003-2025, PathologyOutlines.com, Inc.
PubMed Search: Invasive urothelial carcinoma

- Urothelial carcinoma that has penetrated the basement membrane and invaded into the lamina propria or deeper
- Histologic characterization and depth of invasion are the most important factors for determining prognosis (Adv Anat Pathol 2015;22:102)
- Urothelial carcinoma is morphologically heterogenous with many variants and subtypes (Surg Pathol Clin 2018;11:713)
- Invasive urothelial carcinoma involving the lamina propria (T1) is often treated with conservative intravesical therapy and mucosal resection (Ann Diagn Pathol 2007;11:395)
- Invasive urothelial carcinoma involving the muscularis propria (T2) is often treated with radical cystectomy (Ann Diagn Pathol 2007;11:395)
- Invasive transitional cell carcinoma (historical term)
- WHO classification 2016:
- Infiltrating urothelial carcinoma
- Urothelial carcinoma with divergent differentiation
- With squamous differentiation
- With glandular differentiation
- With trophoblastic differentiation
- Nested urothelial carcinoma
- Including large nested variant
- Microcystic urothelial carcinoma
- Micropapillary urothelial carcinoma
- Lymphoepithelioma-like urothelial carcinoma
- Plasmacytoid / signet ring / diffuse urothelial carcinoma
- Sarcomatoid urothelial carcinoma
- Giant cell urothelial carcinoma
- Poorly differentiated urothelial carcinoma
- Lipid rich urothelial carcinoma
- Clear cell (glycogen rich) urothelial carcinoma
- ICD-O:
- ICD-10: C67.9 - malignant neoplasm of bladder, unspecified
- Fourth most common malignancy in U.S. men
- Eight most common malignancy associated with death in U.S. men
- Median age: 69 years in men and 71 years in women (Adv Anat Pathol 2015;22:102)
- Incidence:
- 4x higher in men than women
- 2x higher in white men than in black men
- Lower tract urothelial carcinoma: bladder and urethra represent 90 - 95% (Eur Urol 2015;68:868)
- Upper tract urothelial carcinoma: ureter and renal pelvis represent 5 - 10% (Eur Urol 2015;68:868)
- Smoking or other chemical exposures start the process of carcinogenesis by altering the DNA of the bladder mucosa; these genetic alterations lead to unregulated cell growth (Adv Anat Pathol 2019;26:251)
- Tobacco smoking: population attributable risk for ever smoking is 50% for both men and women in U.S. (Eur Urol 2013;63:234)
- Occupational exposures: aromatic amines, chlorinated hydrocarbons and polycyclic aromatic hydrocarbons including benzidine (Eur Urol 2013;63:234)
- Genetic predisposition (Eur Urol 2013;63:234)
- Unlike squamous cell carcinoma, not due to indwelling catheters
- Hematuria, irritation / pain during urination, increased urinary frequency or urgency (Urology 2006;67:3)
- Urine cytology on voided samples (Eur Urol 2013;63:4)
- Cystoscopy with biopsy or transurethral resection (Eur Urol 2013;63:4)
- CT image findings include urothelial thickening / hyperenhancement, asymmetric collecting duct system, urothelial calcifications or the presence of a nodule / mass (Urol Clin North Am 2018;45:389)
- MRI T2 weighted images demonstrate hypointense thickening of bladder wall (Abdom Radiol (NY) 2019;44:3858)
Images hosted on other servers:

CT with bladder thickening

Bladder tumor and lung metastasis

Retrograde pyelogram

Pyeloureteral transitional cell
- 5 year relative survival: 69% with local disease, 37% with regional disease and 6% with distant disease (American Cancer Society: Survival Rates for Bladder Cancer [Accessed 6 April 2021])
- Stage, with histologic characterization and involvement of the muscularis propria (detrusor muscle) is an important factor for determining prognosis (Adv Anat Pathol 2015;22:102)
- Morphological variants associated with poor prognosis, possibly due to late stage diagnosis and aggressive behavior include:
- Urothelial carcinoma with divergent differentiation (squamous or glandular)
- Micropapillary urothelial carcinoma
- Plasmacytoid urothelial carcinoma
- Nested urothelial carcinoma (Adv Anat Pathol 2015;22:102)
- 53 year old woman with IgG4 related kidney disease from the renal pelvis that mimicked urothelial carcinoma (BMC Urol 2015;15:44)
- 56 year old man with testicular metastasis (Case Rep Urol 2014;2014:759858)
- 62 year old man with lymphadenopathies diagnosed with adenocarcinoma of unknown origin (Acta Med Okayama 2019;73:279)
- 65 year old man with recurrence of urothelial carcinoma in an orthotopic neobladder (BMJ Case Rep 2017;2017:bcr2017221052)
- 65 year old man with plasmacytoid urothelial carcinoma and unique clinicopathologic profile on rapid autopsy (Diagn Pathol 2019;14:113)
- 80 year old woman with invasive urothelial carcinoma with chordoid features (Int J Clin Exp Pathol 2015;8:15344)
- Conservative therapy is often offered for invasion into the lamina propria (T1) (Ann Diagn Pathol 2007;11:395)
- Conservative therapy includes Bacillus Calmette-Guérin (BCG) intravesical immunotherapy (American Cancer Society: Intravesical Therapy for Bladder Cancer [Accessed 8 April 2021])
- Radical cystectomy is usually required for invasion into the muscularis propria (T2) (Ann Diagn Pathol 2007;11:395)
- Locally advanced cancers are typically treated with chemotherapy, immunotherapy and occasionally radiation (J Urol 2018;199:1129)
Images hosted on other servers:

Cystoscopy: pedunculated tumor
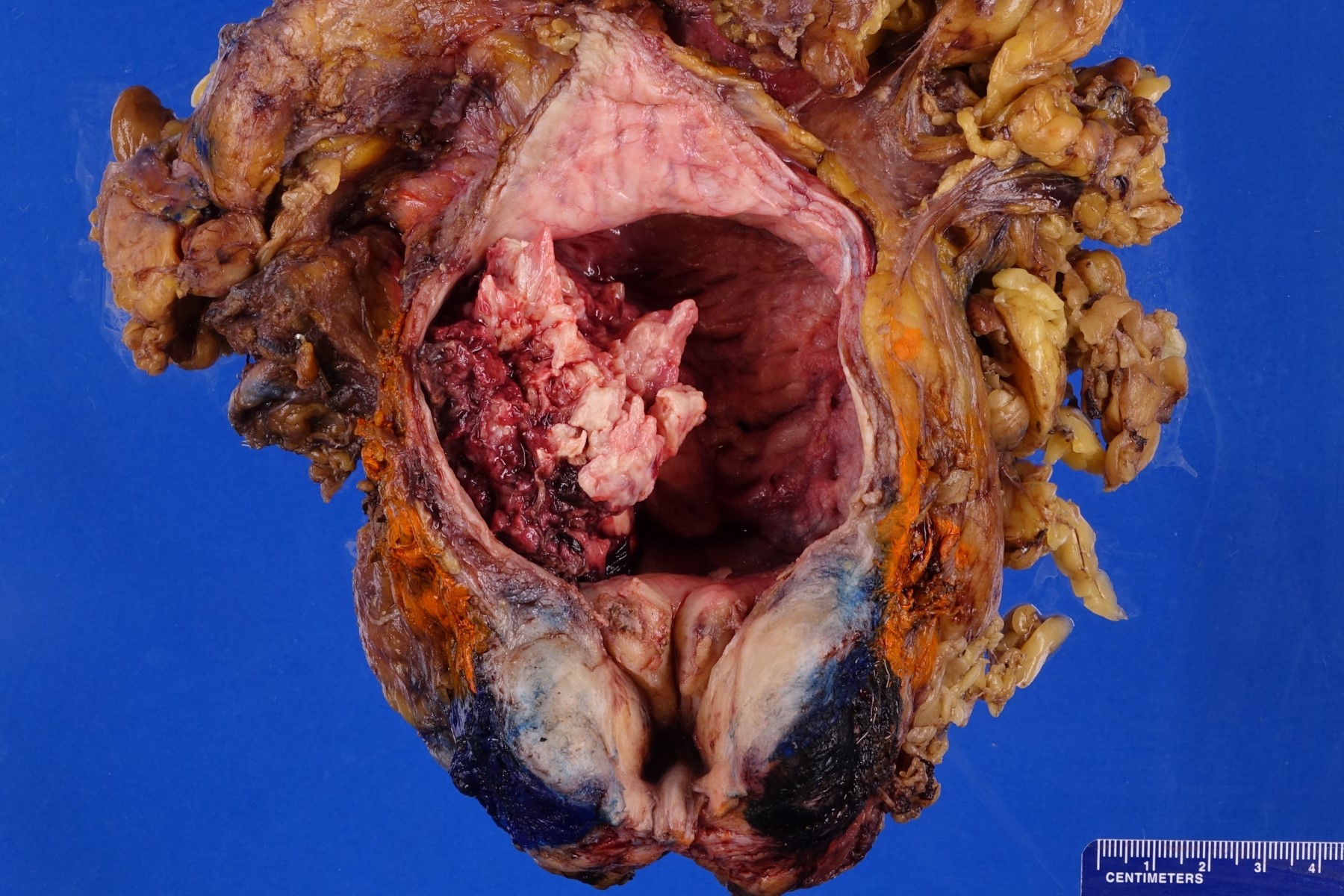
- Macroscopic findings range from subtle bladder wall thickening to obvious exophytic mass (Adv Urol 2014;2014:192720)
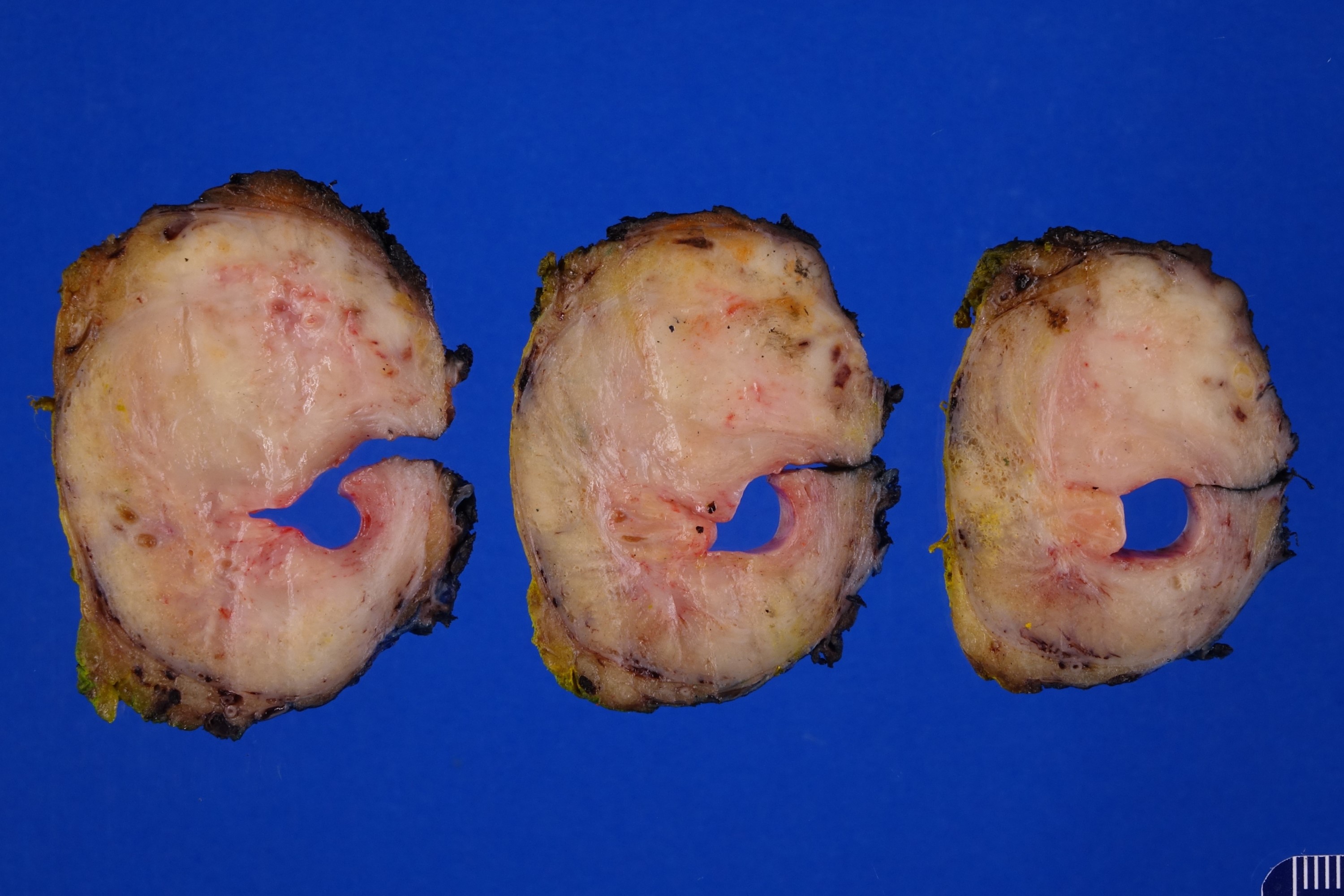
Contributed by Debra L. Zynger, M.D., Nicole K. Andeen, M.D. and Maria Tretiakova, M.D.
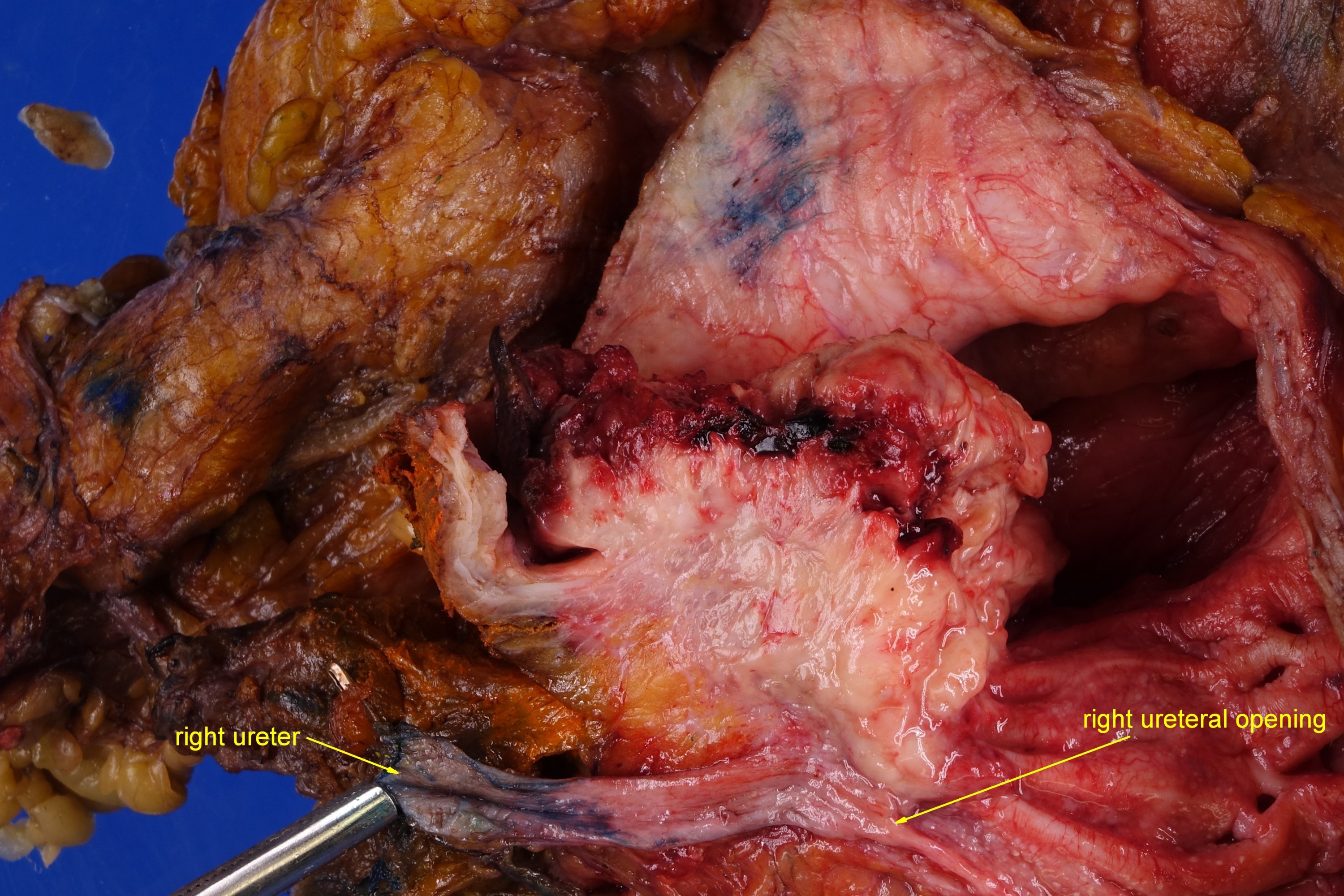
Muscularis propria invasion (pT2b)
Prostatic invasion (pT4a)

Renal pelvic and peripelvic fat invasion (pT3)
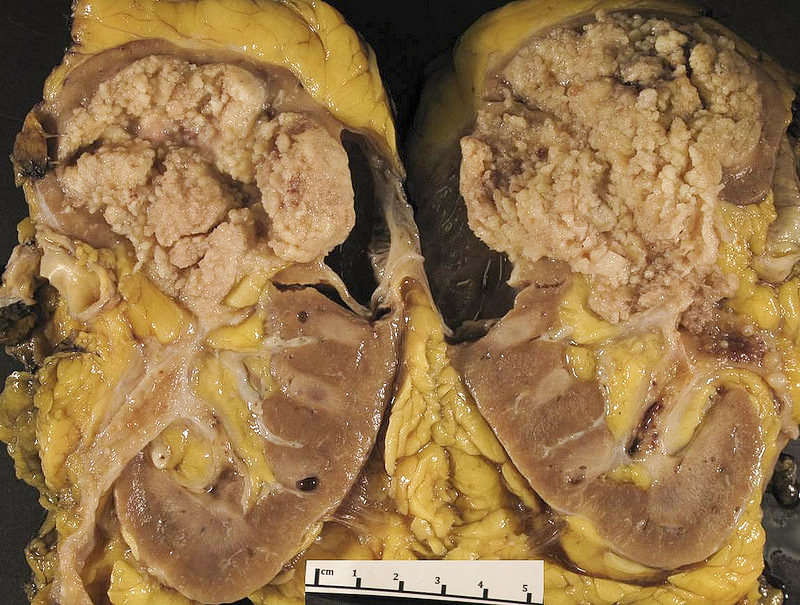
Friable, exophytic
papillary mass,
renal pelvis
- Positive margin is defined by the presence of in situ or invasive urothelial carcinoma on frozen section (Ann Diagn Pathol 2015;19:107)
- Ureteric intraoperative frozen sections have significant clinical limitations due to skip lesions, which often occur in multifocal urothelial carcinoma in situ (J Clin Pathol 2010;63:475)
Images hosted on other servers:

Urothelial carcinoma in situ in frozen section
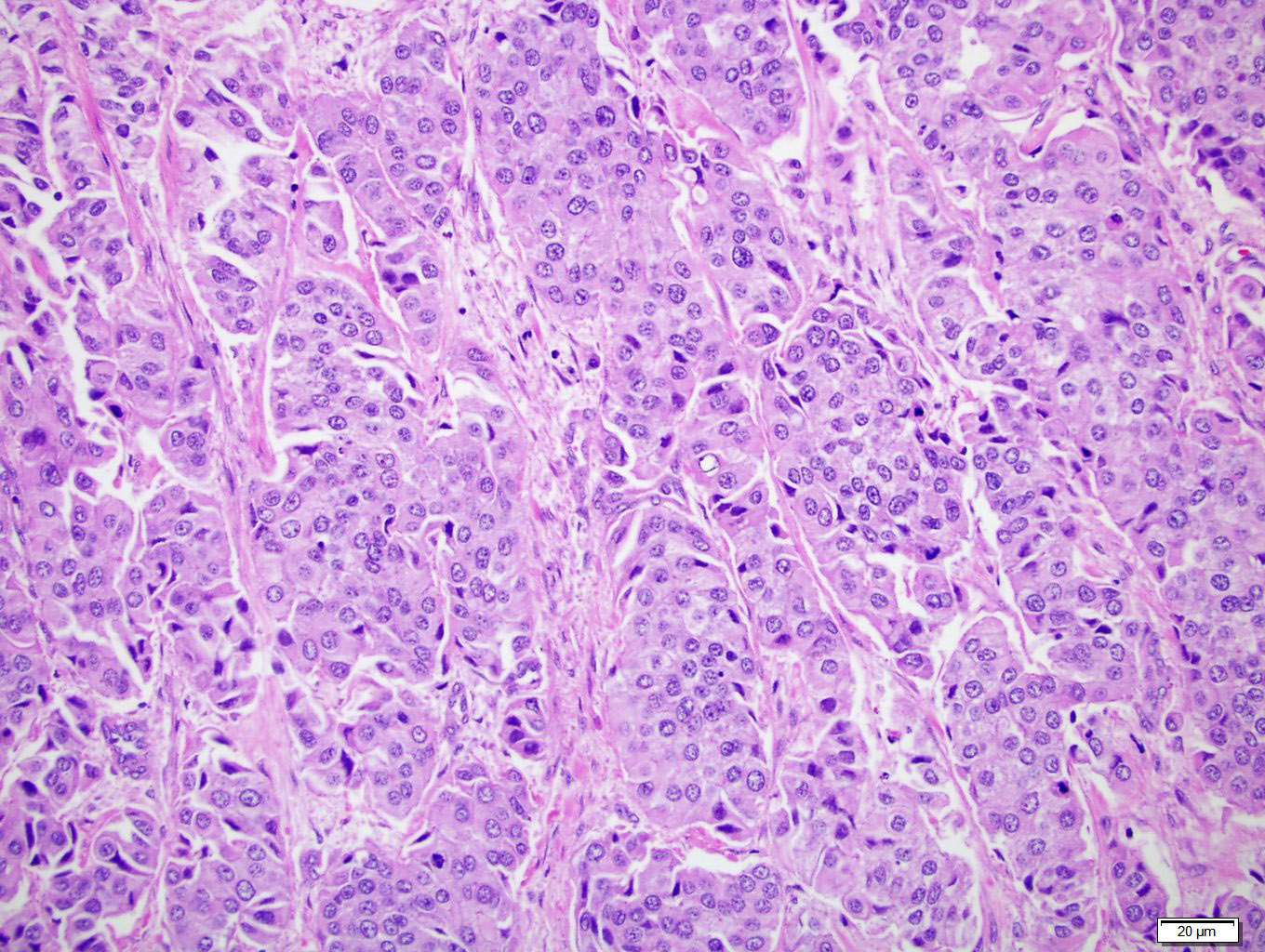
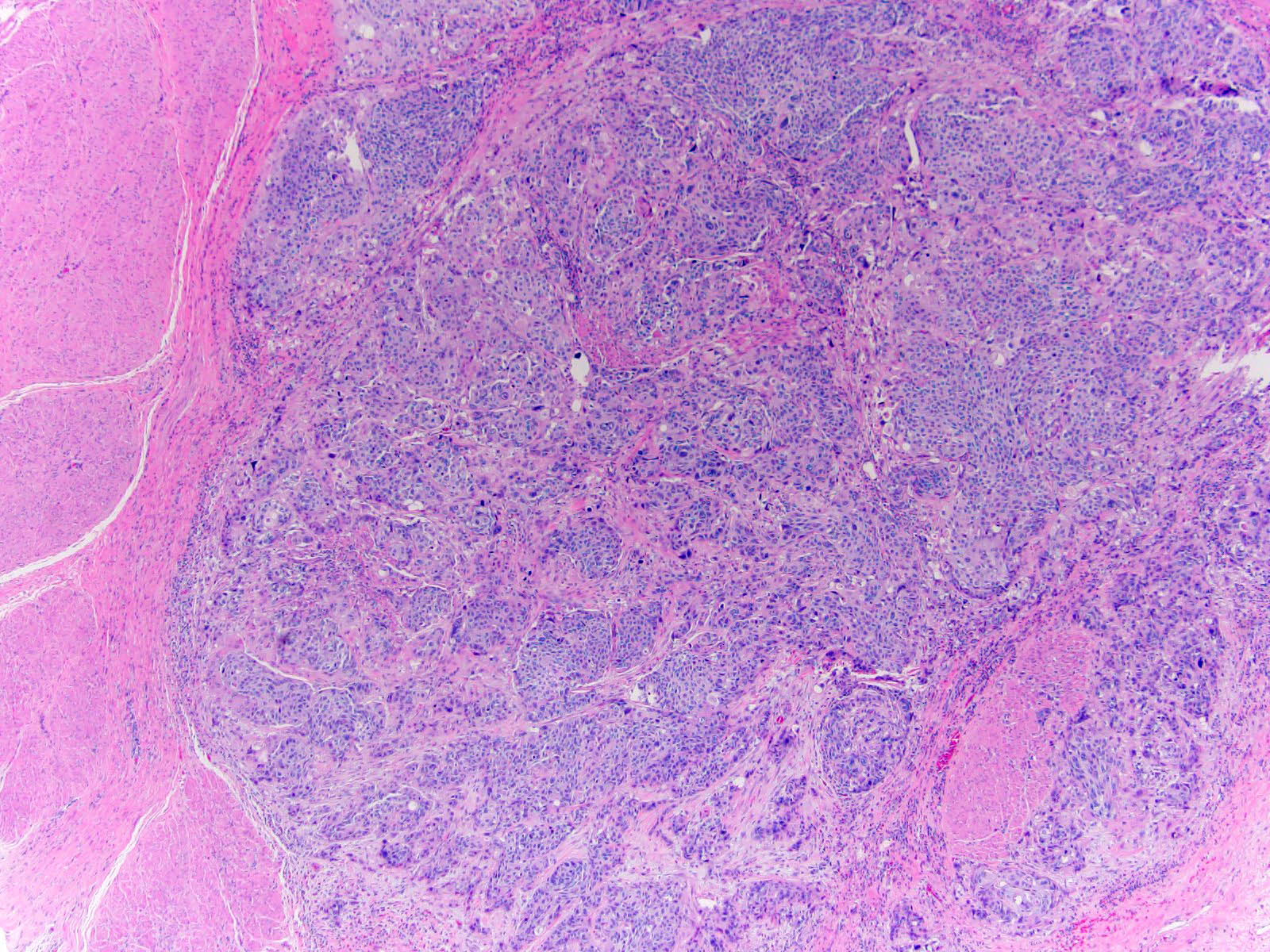
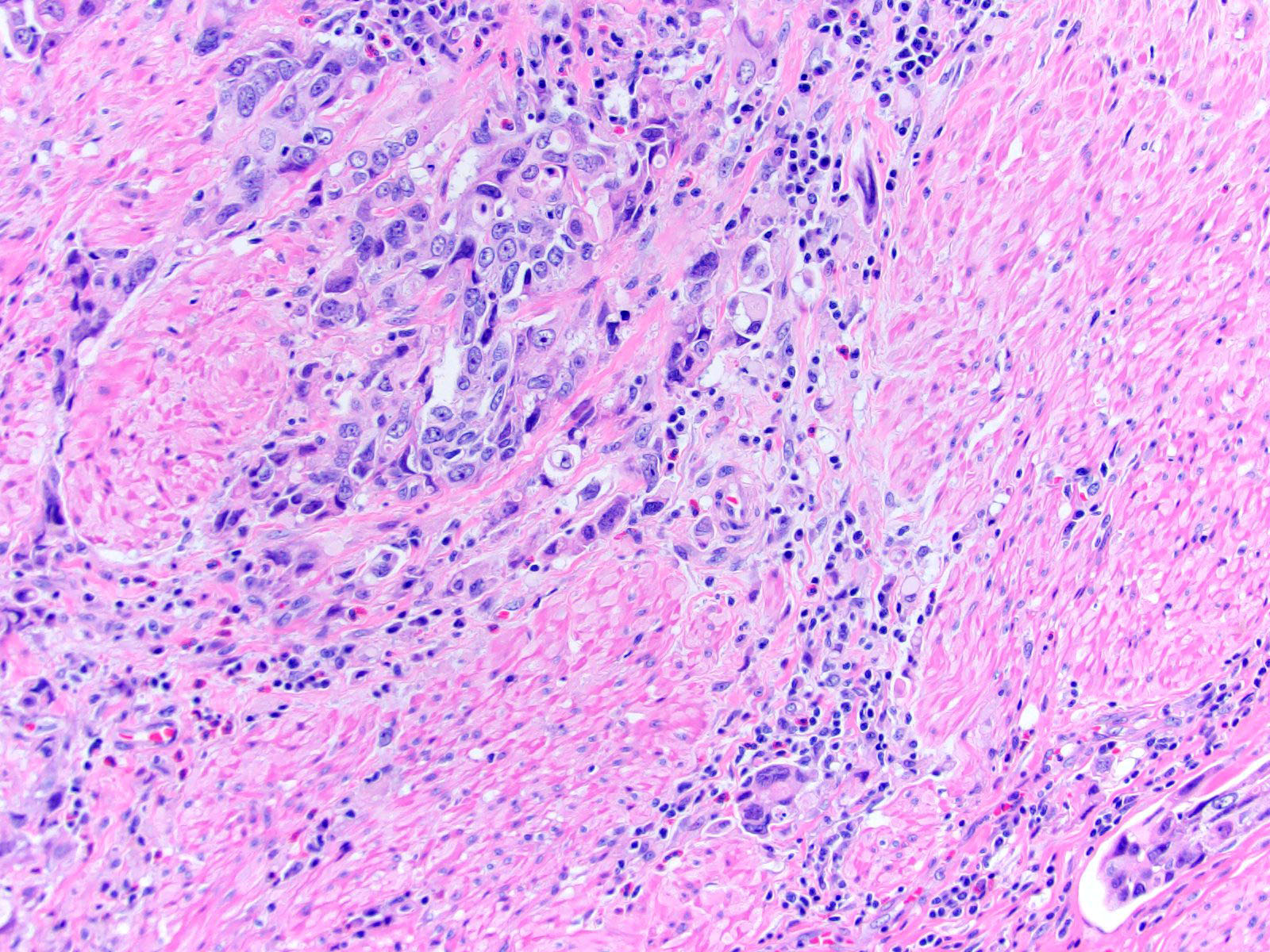
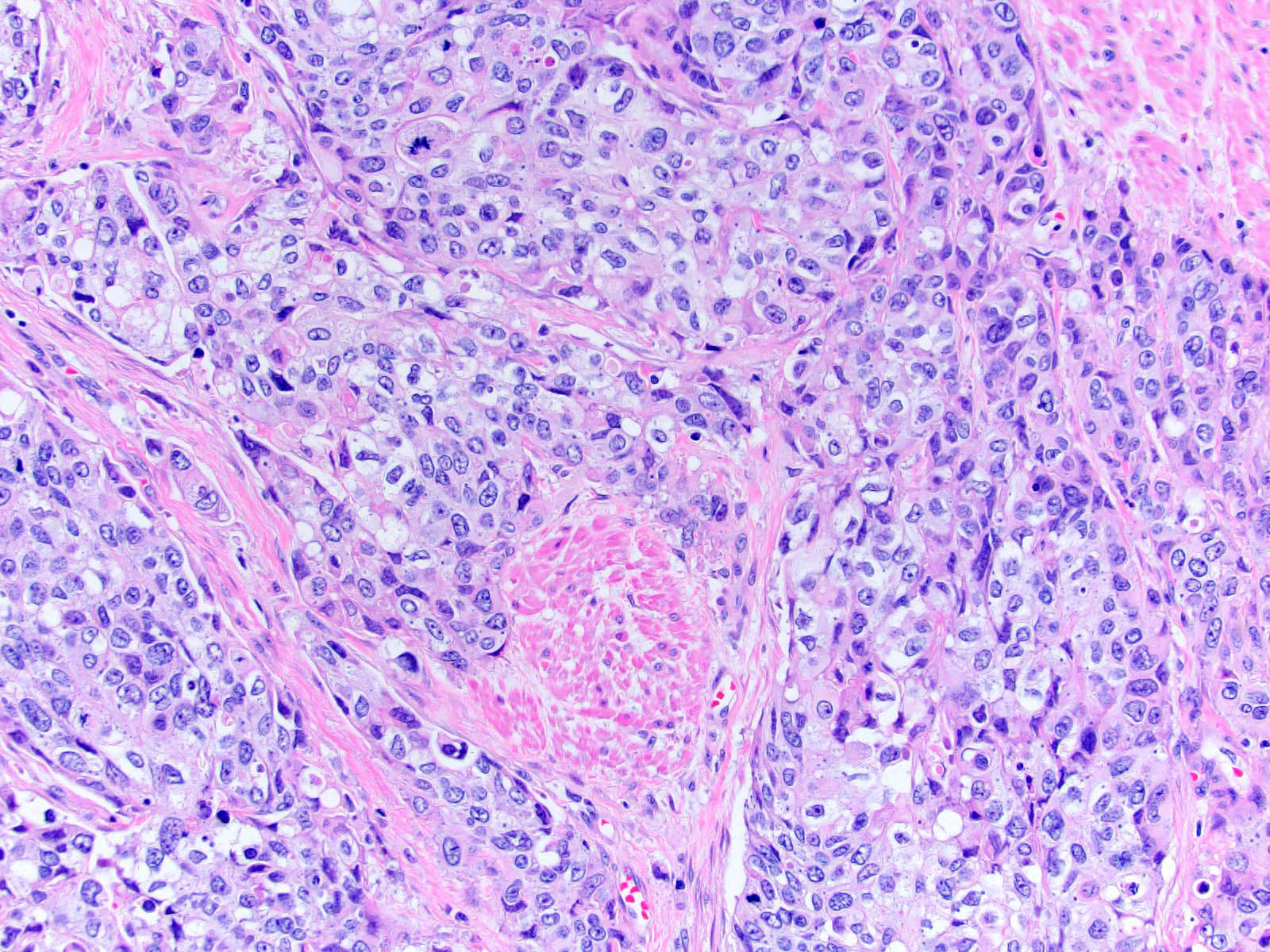
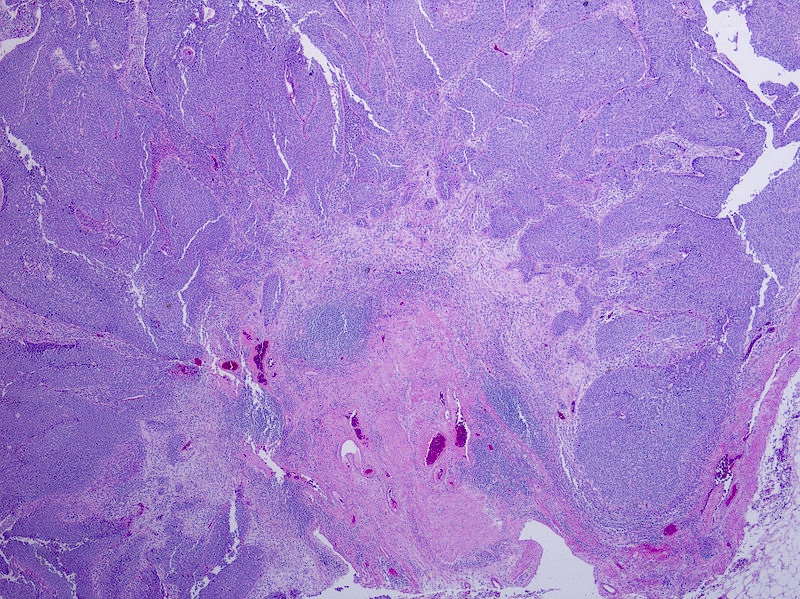
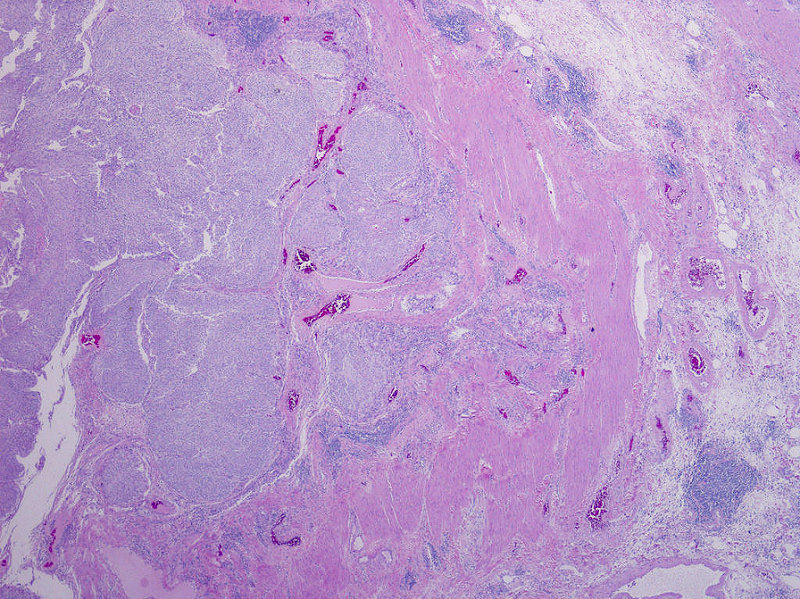
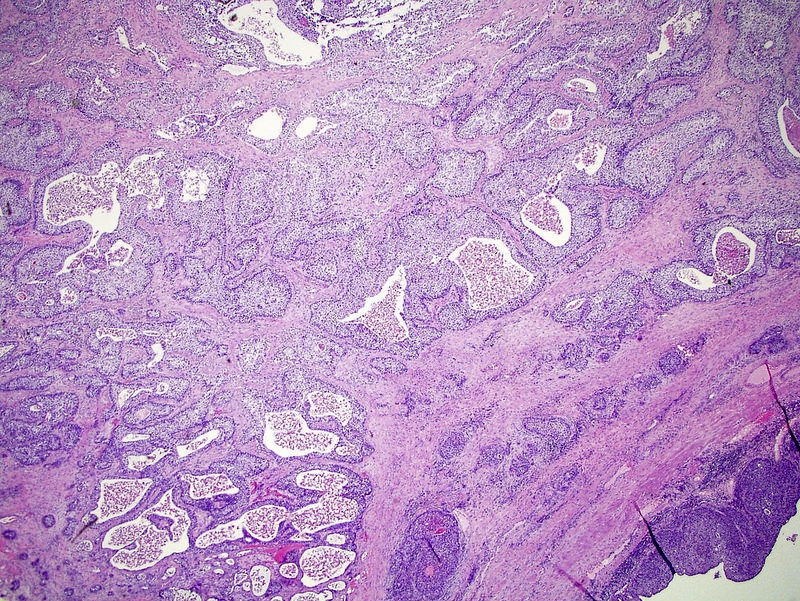
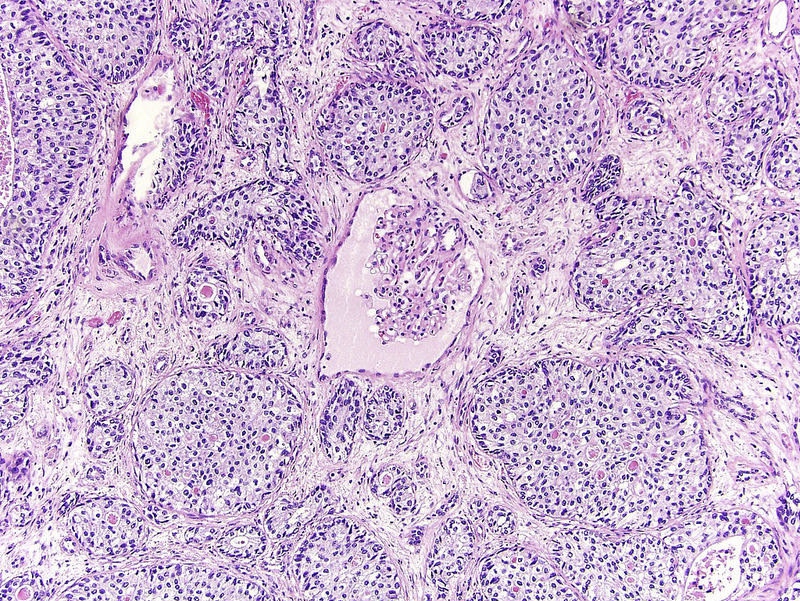
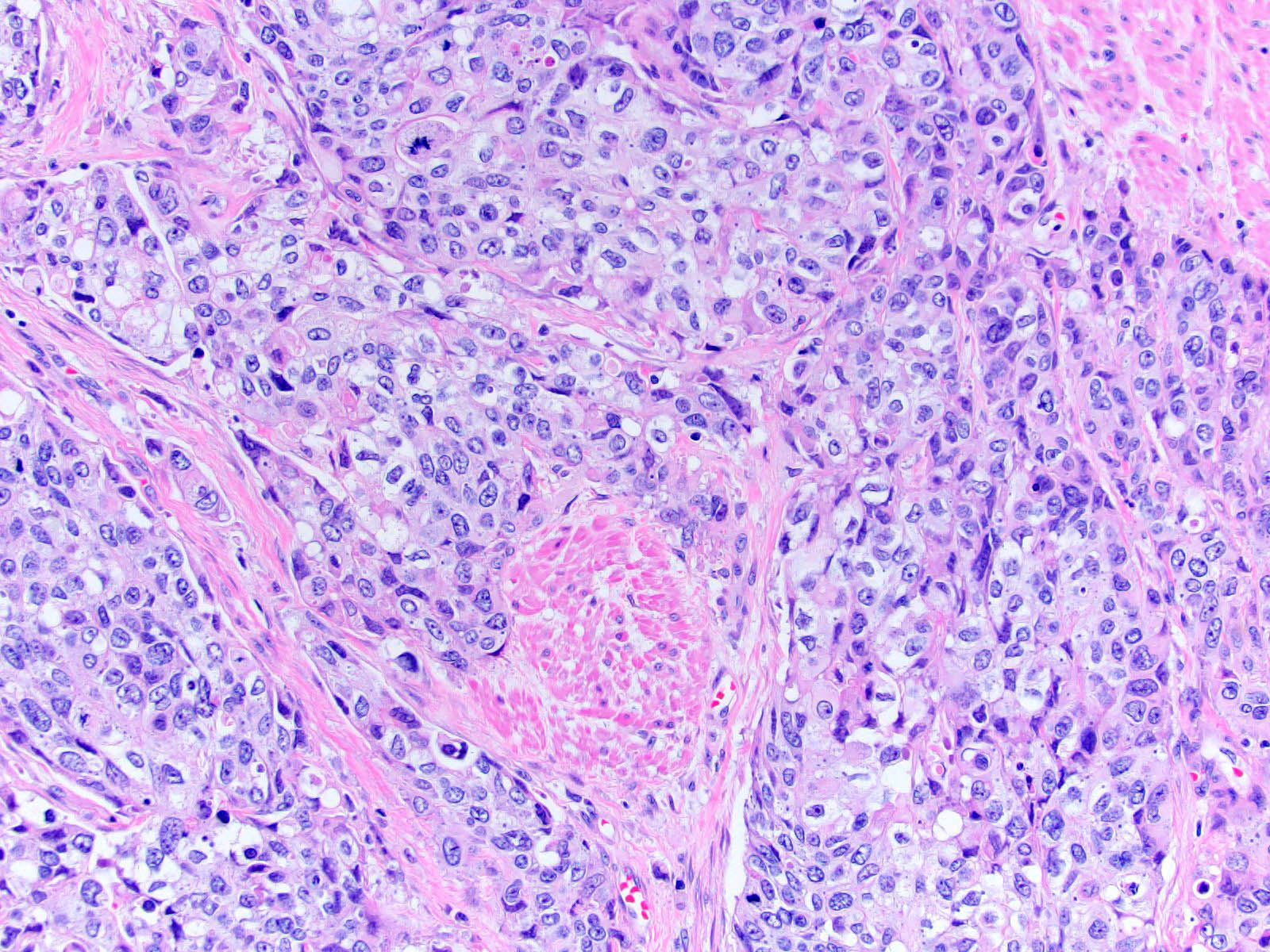
- Neoplastic cells arranged in irregular nests or single cells invading the lamina propria and muscularis propria
- Retraction artifact is often seen and can mimic vascular invasion (Am J Surg Pathol 2001;25:356)
- High grade nuclear features: nuclear pleomorphism, hyperchromasia, high N/C ratio with frequent mitotic figures (Am J Surg Pathol 2001;25:356)
- Note: nested urothelial carcinoma demonstrates bland, low grade cytology (Hum Pathol 2019;94:11)
Contributed by Maria Tretiakova, M.D., Ph.D., Andrey Bychkov, M.D., Ph.D., Nicole K. Andeen, M.D. and @katcollmd on Twitter
Invasive high grade urothelial carcinoma
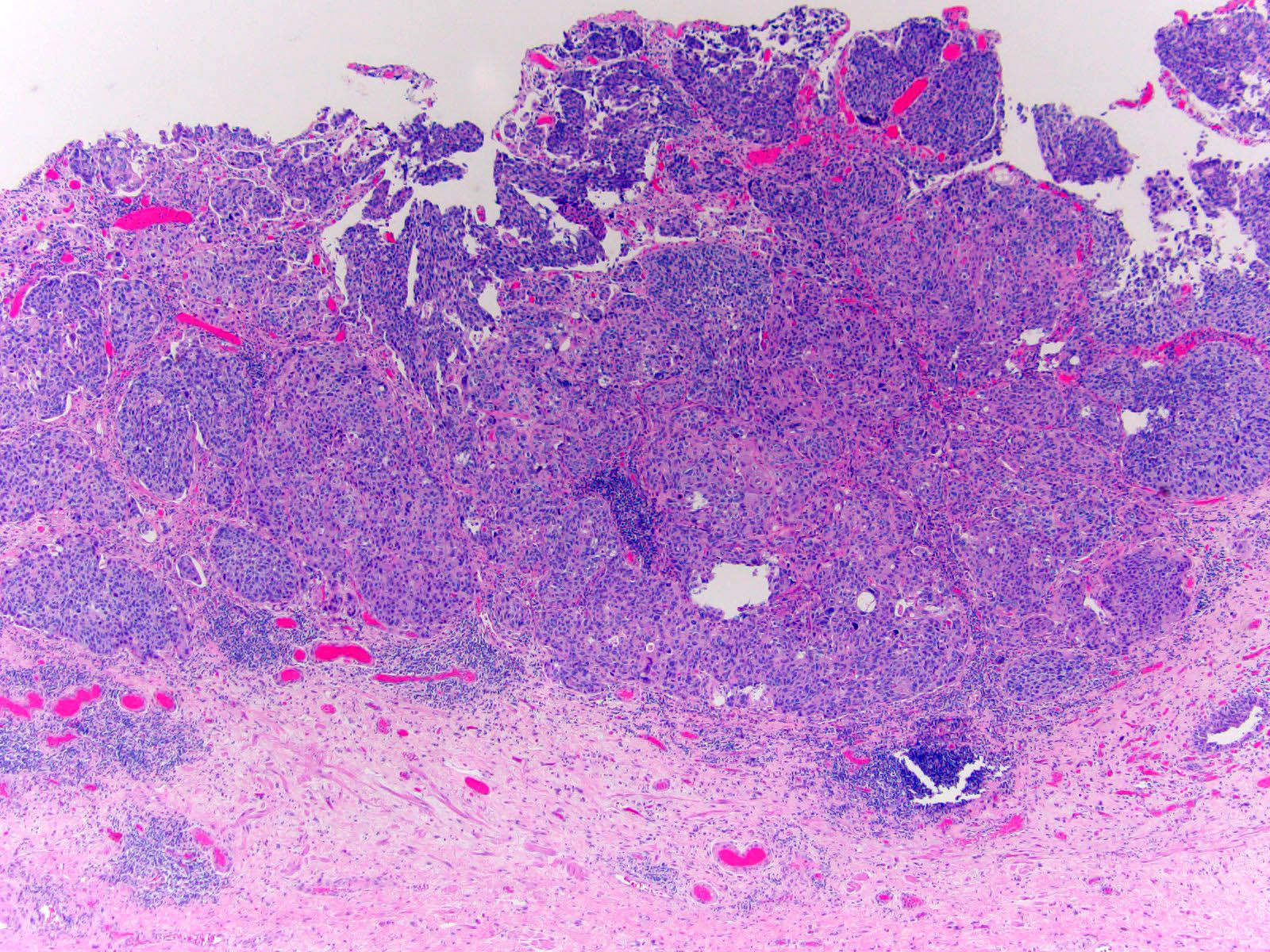
Extensive invasion into lamina propria
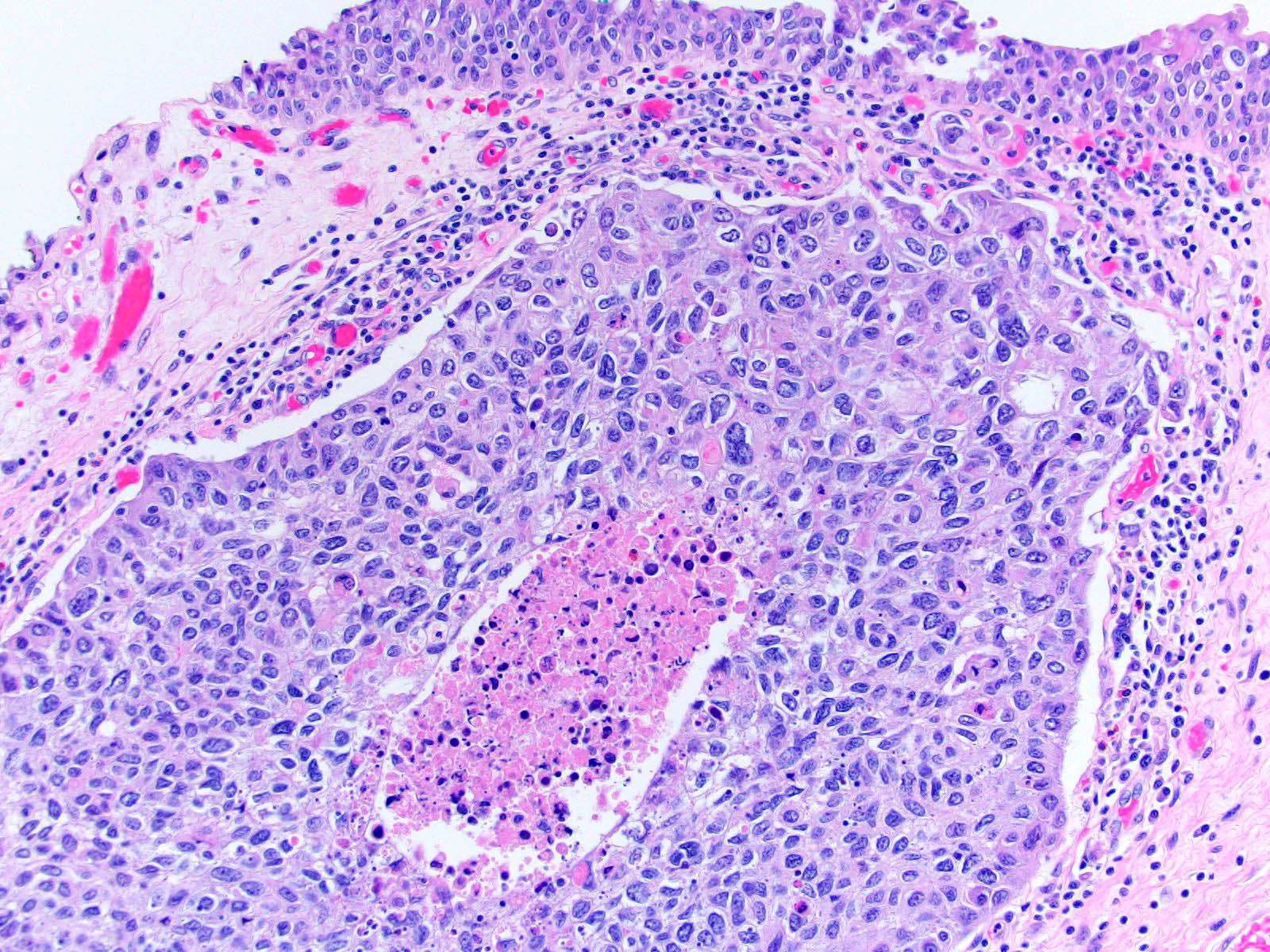
Invasive urothelial
carcinoma with
comedo necrosis
Lymphovascular invasion
Muscularis propria invasion
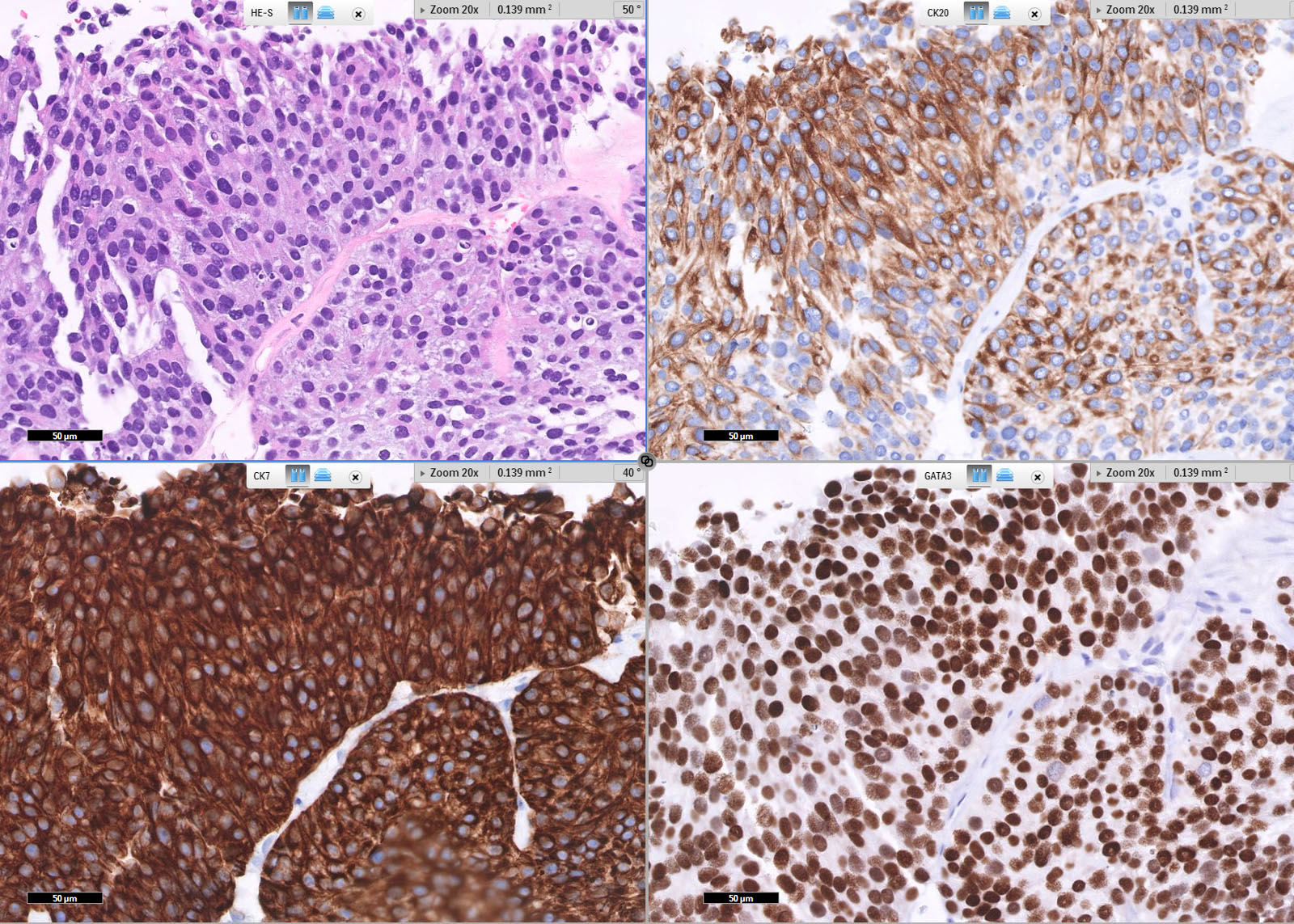
IHC profile
Subepithelial invasion (pT1)
Invasion into muscularis (pT2)
Invasion of renal parenchyma (pT3)


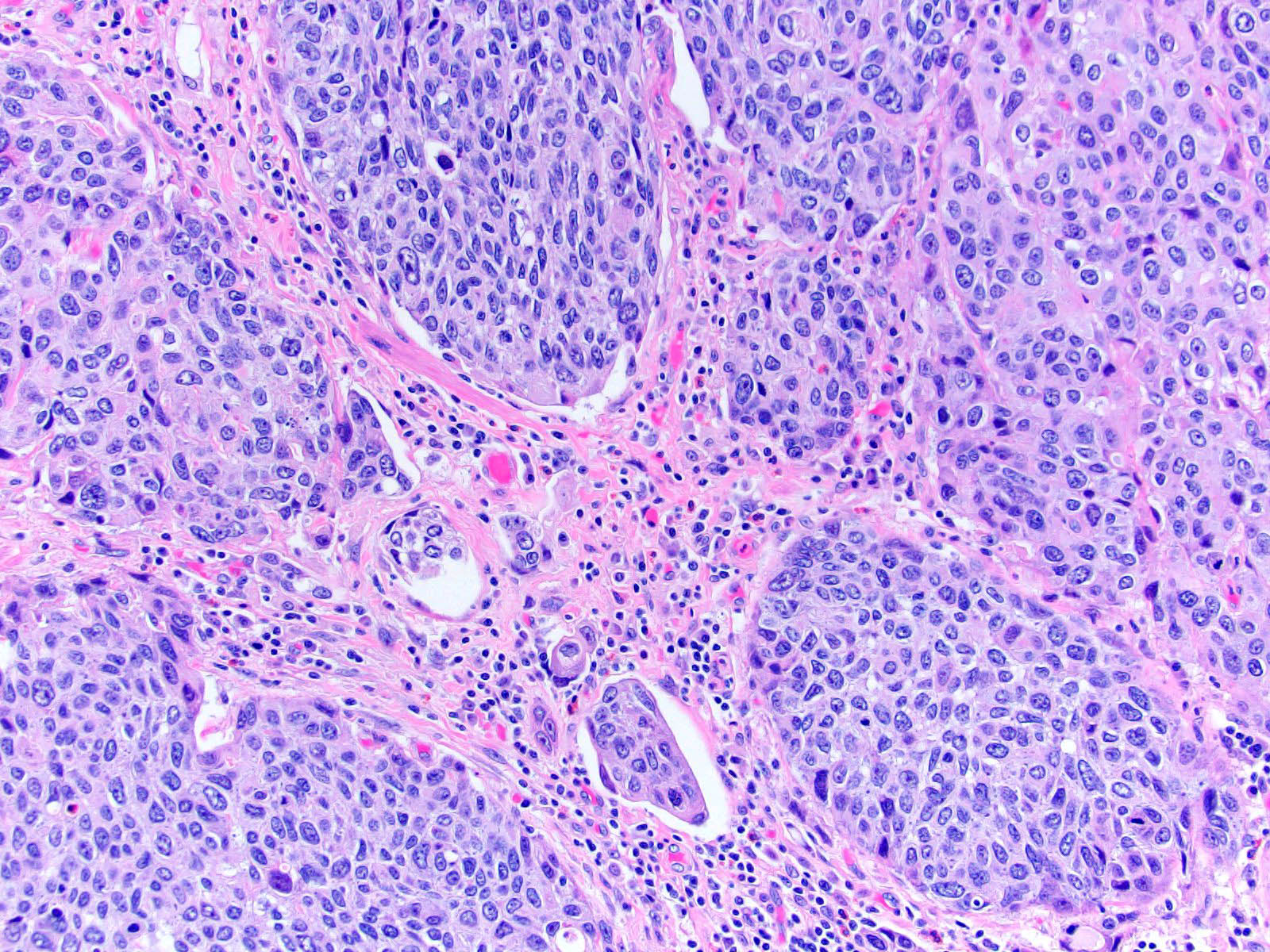
Invasive urothelial carcinoma


Invasive urothelial carcinoma
- Urine cytologic detection of urothelial carcinoma has sensitivity and specificity of 13 - 75% and 85 - 100%, respectively (PLoS One 2015;10:e0134940)
- Diagnostic categories are based on The Paris System for Reporting Urinary Cytology
- Cytologic diagnosis of high grade urothelial carcinoma requires > 10 cells with high N/C ratio, irregular chromatin pattern and hyperchromatic nuclei (Cancer Cytopathol 2018;126:207)
Contributed by Bonnie Choy, M.D.
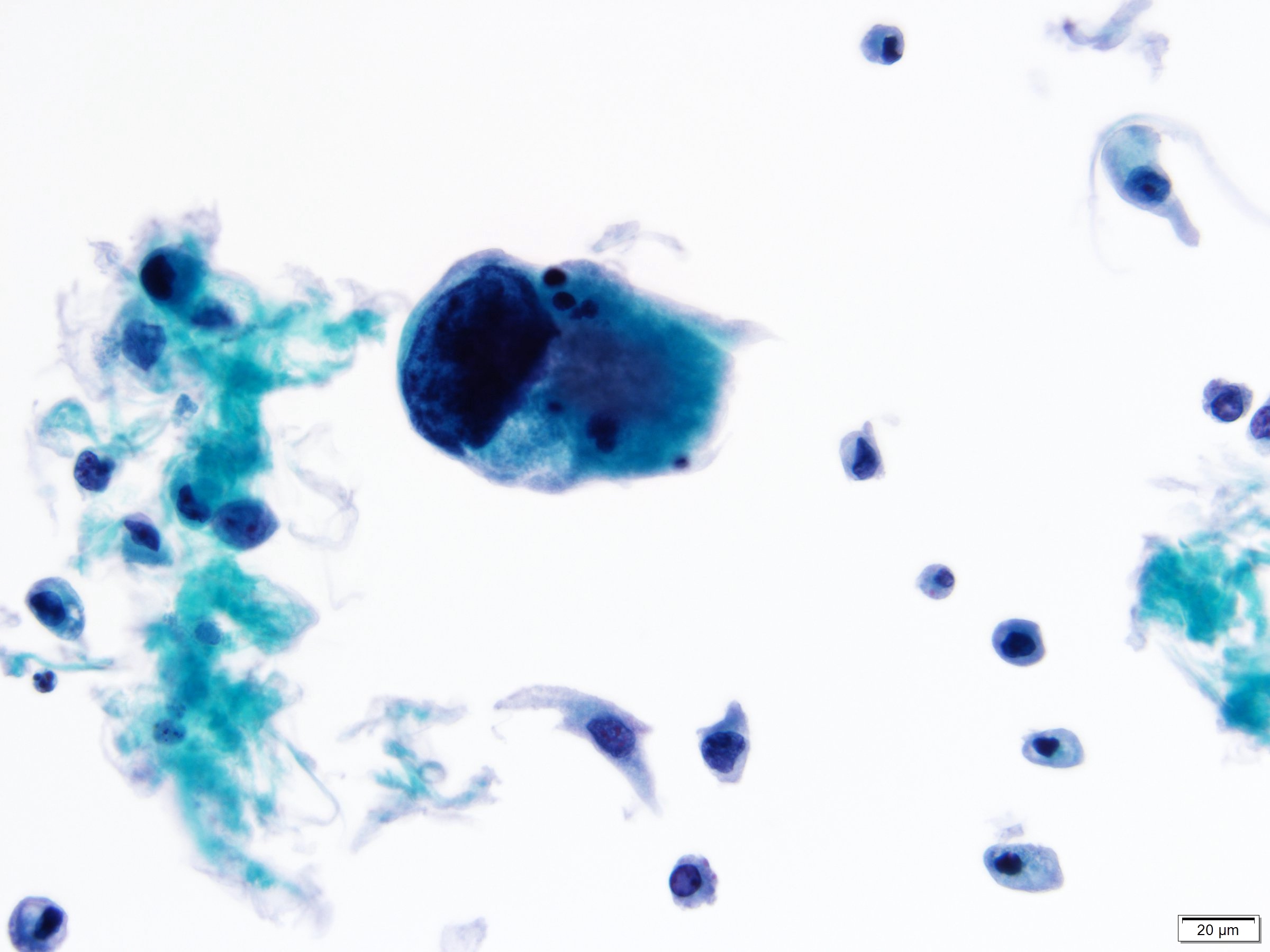
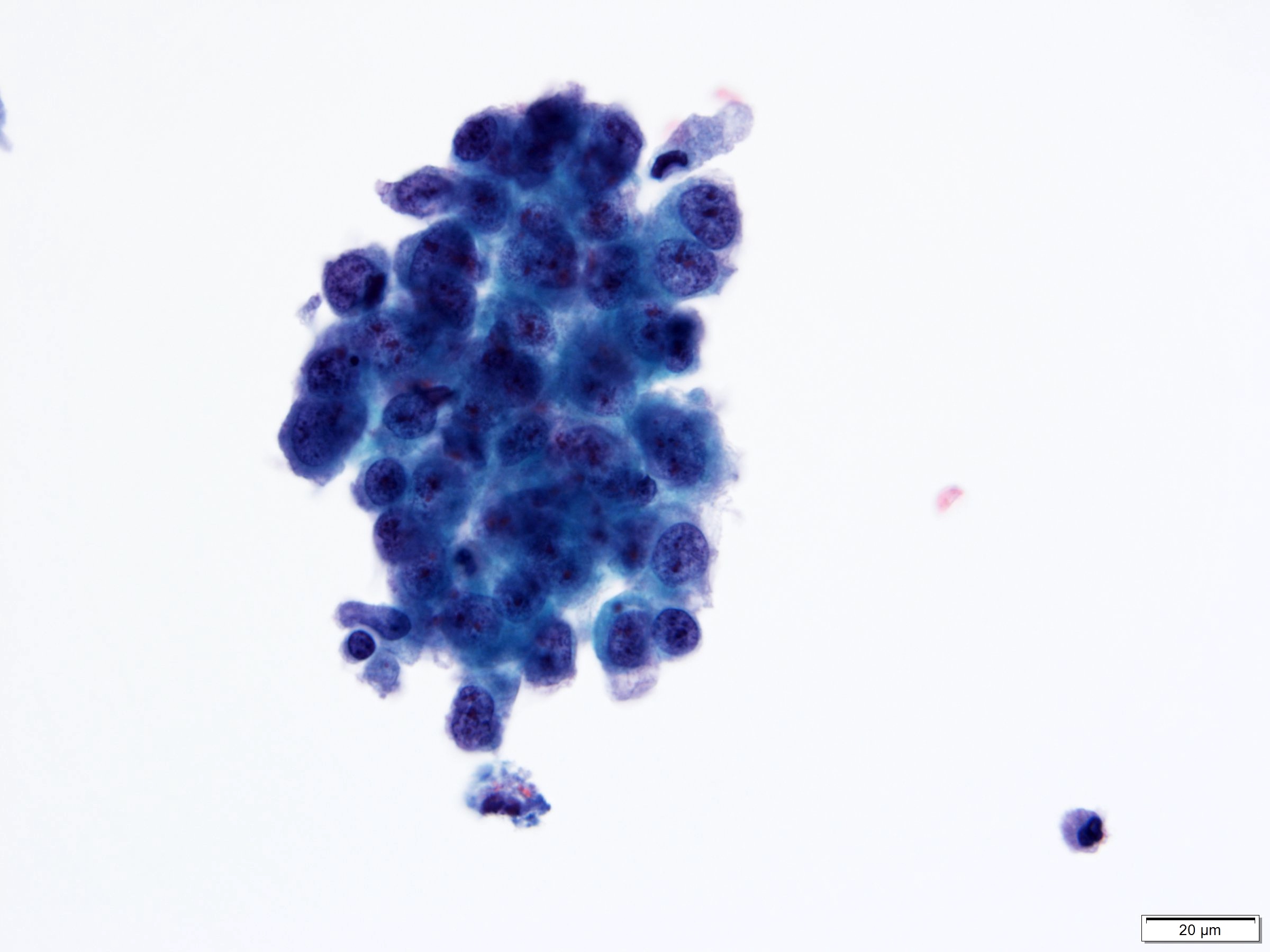

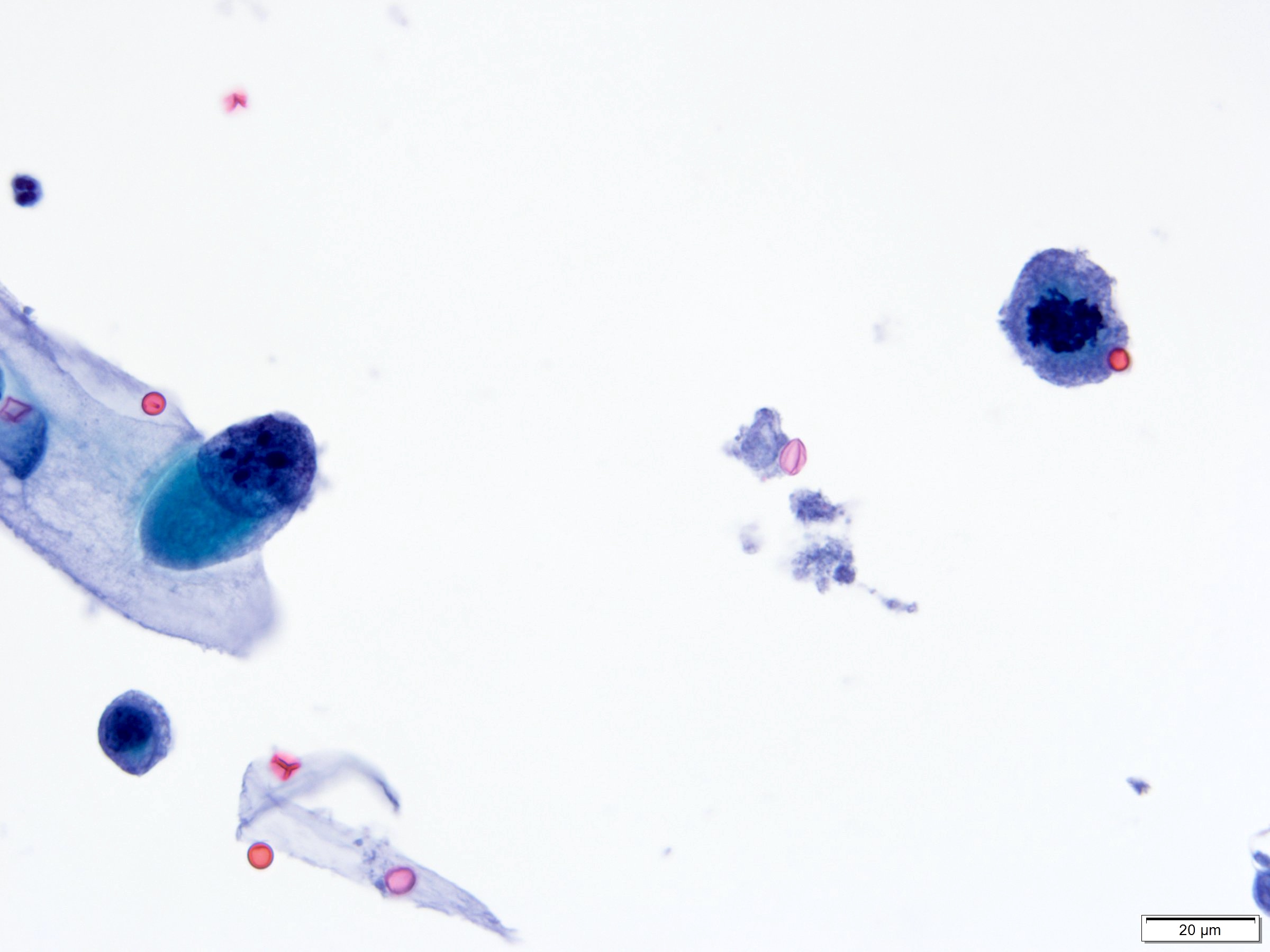
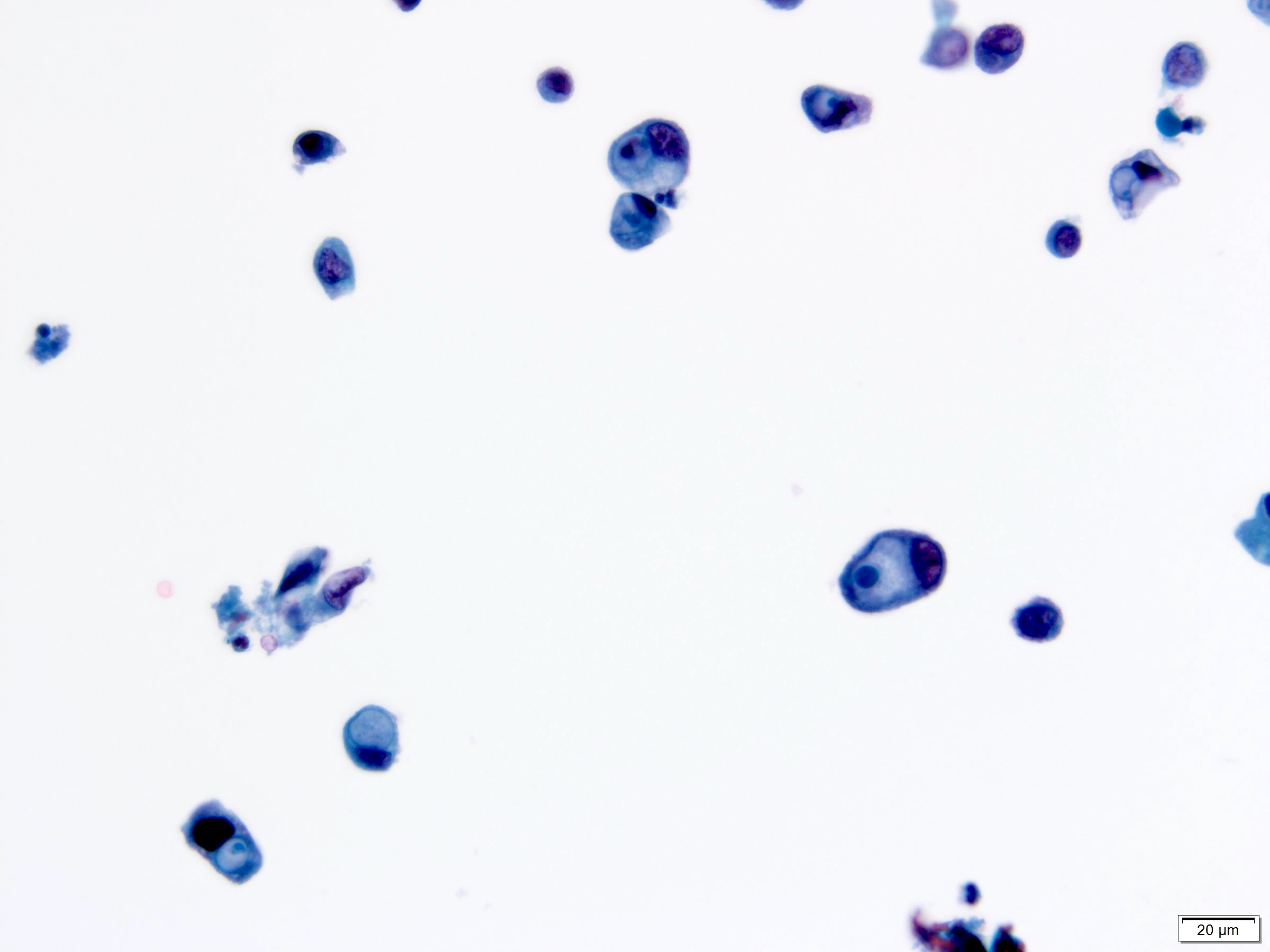
High grade urothelial carcinoma
Contributed by Nicole K. Andeen, M.D. and Maria Tretiakova, M.D.
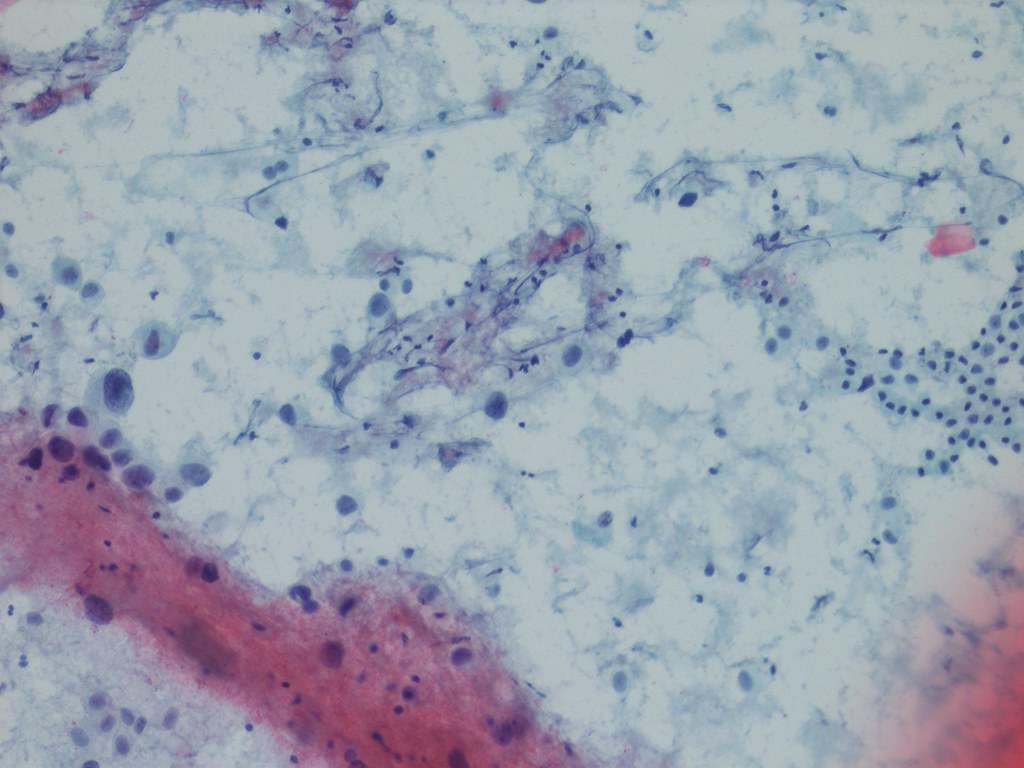
Highly atypical cells
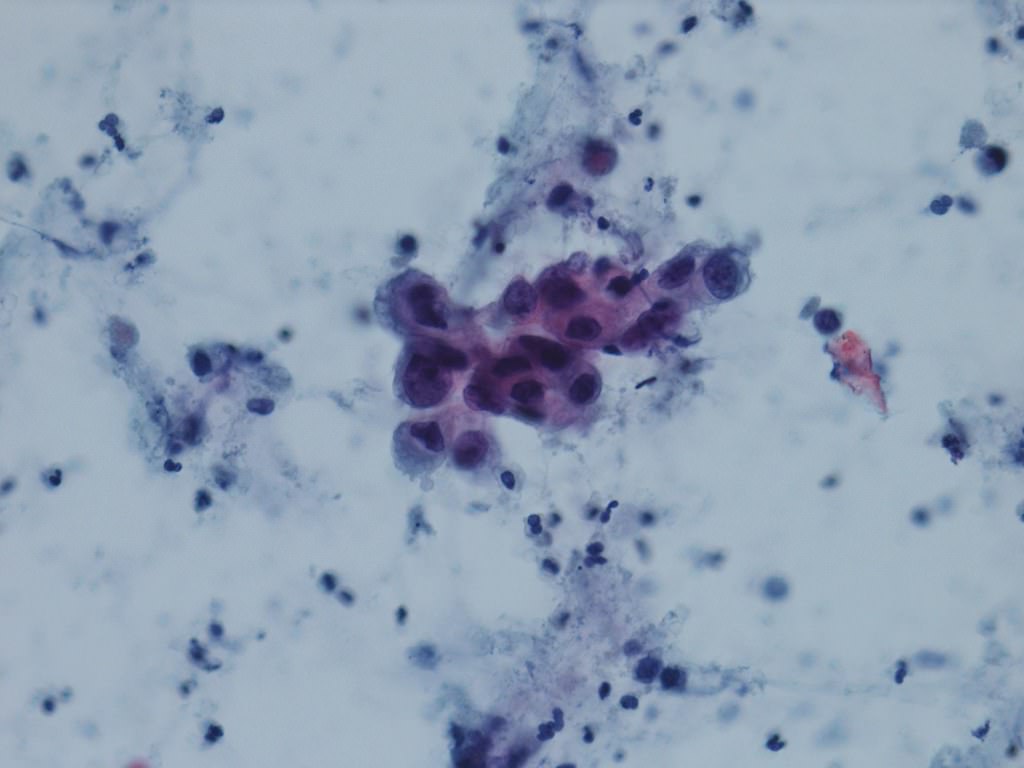
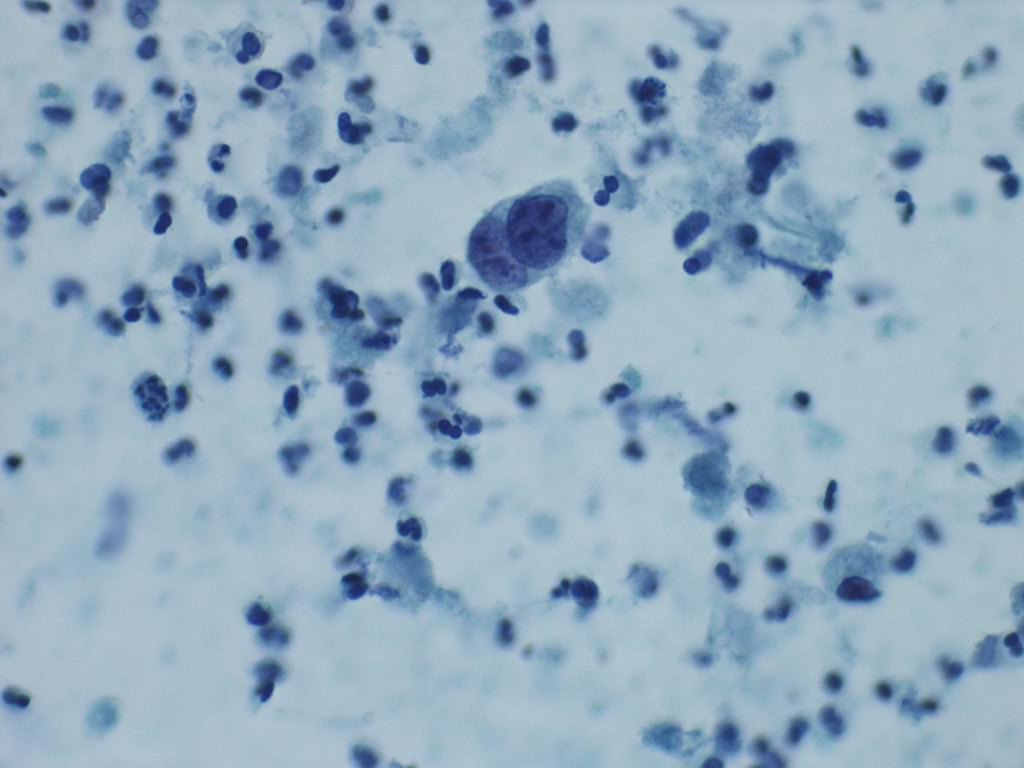
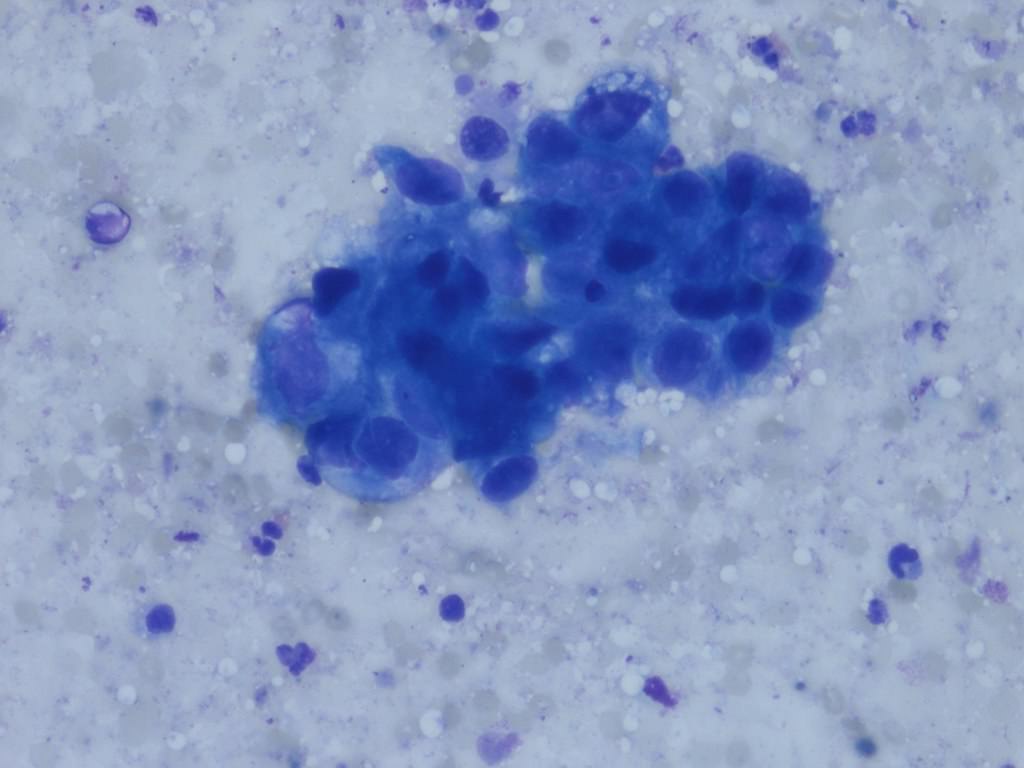
Large nuclei with high nuclear to cytoplasmic ratios, coarse chromatin and irregular nuclear contours (Papanicolaou and DiffQuik)
- GATA3, CK7, CK20, p63, p40, uroplakins II and III, HMWCK, thrombomodulin (Pathology 2016;48:543, Am J Surg Pathol 2012;36:1472)
- PDL1 in tumor cells characterized by ≥ 1% is expressed in 13.3 - 46.7% cases (Hum Pathol 2018;81:184, Mod Pathol 2018;3:623)
- Immunostaining can distinguish luminal and basal phenotypes (Sci Rep 2020;10:9743)
- Most commonly mutated genes are associated with cell cycle progression, including TP53, PIK3CA, RB1 and FGFR3 (Nature 2014;507:315)
- UroVysion is an FDA approved fluorescent in situ hybridization (FISH) that detects aneuploidy in chromosomes 3, 7 and 17 and loss of 9p21 locus (72% sensitivity and 83% specificity) (BJU Int 2013;112:E372, Curr Opin Urol 2019;29:203)
- Nuclear matrix proteins (NMP22): group of proteins produced by cancerous cells
- NMP22 BladderChek test is an FDA approved qualitative assay for surveillance and detection of bladder cancer (50% sensitivity and 87% specificity) (Curr Opin Urol 2019;29:203)
- Bladder tumor antigen (BTA): antigen produced by cancerous cells
- BTA Trak (quantitative) and BTA Stat (qualitative) are FDA approved assays for surveillance (68 - 77.5% sensitivity and 50 - 75% specificity) (Curr Opin Urol 2019;29:203)
Contributed by Nicole K. Andeen, M.D. and Maria Tretiakova, M.D.
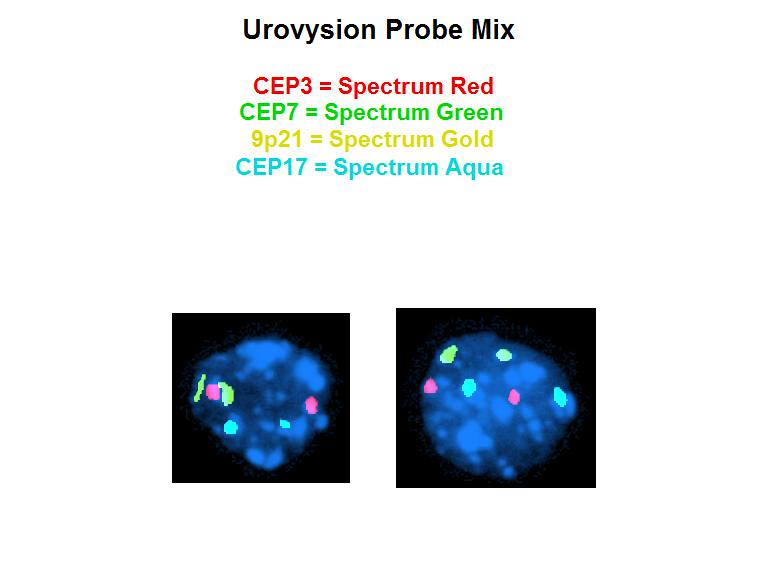
FISH, loss of 9p, normal disomy chromosomes 3, 7, 17

FISH, polyploidy chromosomes 3, 7, 17; 9p preserved
- Bladder, TURB:
- Urothelial carcinoma, high grade (see comment)
- Type / grade comment: micropapillary (20%)
- Associated lesions: carcinoma in situ
- Extent: lamina propria invasion, extensive (pT1)
- Angiolymphatic invasion: present
- Muscularis propria: present, uninvolved
- Inverted urothelial papilloma:
- Smooth or dome shaped surface with monotonous cells growing in an endophytic pattern without the presence of lamina propria invasion (Hum Pathol 2019;92:18)
- Prostatic adenocarcinoma:
- Paraganglioma:
- Similar nested architecture, prominent vascular network and distinguishable by immunohistochemistry
- Positive for S100 (sustentacular pattern), synaptophysin and chromogranin (Histopathology 2019;74:77)
- Negative for AE1 / AE3 and CK7
- Potential pitfall: also positive for GATA3 (J Mod Pathol 2013;26:1365)
- Nephrogenic adenoma:
- Rare nuclear atypia and distinguishable by immunohistochemistry: positive for PAX8, PAX2 and AMACR (Histopathology 2019;74:77)
- Cystitis cystica / glandularis:
- Lacks cytologic atypia, necrosis, stromal reaction and invasion into lamina propria and muscularis propria (Histopathology 2019;74:77, Ann Diagn Pathol 2019;38:11)
- Renal cell carcinoma (for renal pelvis):
- Lack of urothelial carcinoma in situ is the most helpful distinguishing factor
- Positive PAX8, negative p63 and negative GATA3 immunoprofile favors renal cell carcinoma; however, stain interpretation and immunohistochemical profile overlap can create diagnostic challenges (Adv Anat Pathol 2018;25:387)
- Tobacco smoke
- Polycyclic aromatic hydrocarbon exposure
- Benzidine exposure
- Indwelling catheter
- Clear cell urothelial carcinoma
- Microcystic urothelial carcinoma
- Conventional high grade urothelial carcinoma
- Plasmacytoid urothelial carcinoma
An 85 year old man has a mass involving the prostate and bladder shown above. Which of the following findings is most supportive of invasive urothelial carcinoma over prostatic adenocarcinoma?
- Sheets of monotonous cells with amphiphilic cytoplasm and prominent nucleoli
- Negative for PSA and CK7
- Positive for GATA3 and HMWCK
- Focus of squamous differentiation
Comment Here
Reference: Invasive urothelial carcinoma

