

Bladder & urothelial tract
Urethral carcinoma
Urethral carcinoma
Authors: Michelle Garrison, B.S., Debra L. Zynger, M.D.
Editorial Board Member: Michelle R. Downes, M.D.
Deputy Editor-in-Chief: Maria Tretiakova, M.D., Ph.D.

Last author update: 30 December 2024
Last staff update: 30 December 2024
Copyright: 2024, PathologyOutlines.com, Inc.
PubMed Search: Urethral carcinoma


Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Virtual slides | Cytology description | Cytology images | Positive stains | Negative stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Garrison M, Zynger DL. Urethral carcinoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/bladderurethralcarcinoma.html. Accessed January 18th, 2025.
Definition / general
- Primary urethral carcinoma is a rare but aggressive genitourinary malignancy that leads to urethral obstruction (Res Rep Urol 2021;13:325)
Essential features
- Primary urethral carcinoma is rare with diverse tumor histology
- Nonspecific clinical findings and lack of screening techniques often lead to late detection and poor prognosis
Terminology
- Urothelial carcinoma
- Squamous cell carcinoma
- Adenocarcinoma of the urethra
ICD coding
- ICD-O: 8140/3 - carcinoma of Littré glands
- ICD-10: C68.0 - malignant neoplasm of urethra
- ICD-11
- 2C93 - malignant neoplasms of urethra or paraurethral gland
- 2C93.0 & XH22Z8 - adenocarcinoma of urethra or paraurethral gland & carcinoma of Skene, Cowper and Littré glands
Epidemiology
- From 2004 to 2016, 436 - 622 new cases of primary urethral carcinoma were diagnosed each year (Cancer Causes Control 2021;32:627)
- Men (68 - 71%) > women (29 - 32%) (Hum Pathol 2018;72:35, World J Urol 2016;34:97, Cancer Causes Control 2021;32:627)
- Median age of diagnosis among men and women is 61 - 71 years old (Hum Pathol 2018;72:35, World J Urol 2016;34:97, Clin Genitourin Cancer 2018;16:e1003, Int J Surg Pathol 2022;30:15, J Surg Oncol 2022;125:907)
- 46% of all patients (male and female) were age 75 or older, 42% were 55 - 74 and 12% were 54 or younger (Cancer Causes Control 2021;32:627)
- Incidence rate highest in Black populations (3.33), followed by White populations (1.72), other race groups (1.57) and Hispanic populations (1.57) (Cancer Causes Control 2021;32:627)
- Race reported as 71% for White population, 16% Black population, 7% Hispanic population and 5% other (Cancer Causes Control 2021;32:627)
- Higher proportion in Black women (12% male, 26% female) (Cancer Causes Control 2021;32:627)
- Overall, urothelial carcinoma is the most common histological subtype (53%), followed by squamous cell carcinoma (24%), adenocarcinoma (15%) and other (9%) (Cancer Causes Control 2021;32:627)
- Men: urothelial (39 - 64%), squamous cell carcinoma (24 - 54%), adenocarcinoma (9%) and other (4%) (Actas Urol Esp (Engl Ed) 2022;46:70, Cancer Causes Control 2021;32:627)
- Women: urothelial (29 - 45%), squamous cell carcinoma (19 - 25%), adenocarcinoma (27 - 40%) and other (7 - 19%) (Cancer Causes Control 2021;32:627, World J Urol 2013;31:147, J Surg Oncol 2022;125:907)
- One study proposed classification of a new hybrid tumor with both urothelial and squamous features, a basaloid appearance and expression and frequent identification of p16 or HPV18 as the overwhelming histology (82%) in the urethra for both men and women (Hum Pathol 2018;72:35)
Sites
- Men (among all histologic subtypes) (World J Urol 2016;34:97)
- Proximal (prostatic + membranous) urethra only: 54%
- Distal (penile) urethra only: 36%
- Proximal + distal urethra: 10%
- Women (among all histologic subtypes) (Clin Genitourin Cancer 2018;16:e1003, World J Urol 2016;34:97)
- Proximal urethra only: 29 - 44%
- Distal urethra only: 21 - 69%
- Proximal + distal urethra: 2 - 33%
Etiology
- Chronic inflammation and irritation of the urinary tract are risk factors for the development of primary urethral carcinoma
- Men: history of sexually transmitted infections (HPV16), urethral stricture, intermittent catheterization and history of radiation therapy (Hum Pathol 2022;129:71)
- Women: recurrent urinary tract infections and urethral diverticula (Clin Genitourin Cancer 2018;16:e1003)
- 77% of patients with urothelial carcinoma of the urethra had a prior history of urothelial carcinoma of the bladder (Int J Surg Pathol 2022;30:15)
Clinical features
- Common presenting features include mass lesion (75 - 79%), urethral narrowing (20%) obstructive urinary tract symptoms (82%) and hematuria (67%) (Hum Pathol 2018;72:35, Clin Genitourin Cancer 2018;16:e1003)
- Among men with bulbar and penile urethral carcinoma, 46% presented with urethral abscess (Actas Urol Esp (Engl Ed) 2022;46:70)
- Inguinal lymph nodes are the most common regional metastatic site (Hum Pathol 2018;72:35)
- Liver and lung are the most frequent distant metastatic sites (Hum Pathol 2018;72:35)
Diagnosis
- Physical examination for suspicious masses or indurations through palpation of external genitalia (Eur Urol 2013;64:823)
- Bilateral inguinal lymph node palpation to assess for the presence of enlarged lymph nodes (Eur Urol 2013;64:823)
- Role of urinary cytology limited due to varying sensitivity (Eur Urol 2013;64:823)
- Urethrocytoscopy with biopsy is diagnostic (Eur Urol 2013;64:823)
Radiology description
- Magnetic resonance imaging (MRI) visualized all tumors in one study with appearance as intermediate signal intensity on T2 imaging (Hum Pathol 2018;72:35)
Radiology images
Images hosted on other servers:

Urothelial carcinoma stricture (male patient)

Urothelial carcinoma with extension (female urethra)

Urothelial carcinoma with metastases (female urethra)
Prognostic factors
- Staging is based on TNM, refer to links for the current system for women and men
- Recurrence rate of 53% for urethral carcinoma (World J Urol 2016;34:97)
- Pathologically advanced (pT3 or greater), pathologically or clinically node positive disease and proximal tumor location associated with recurrence (World J Urol 2016;34:97)
- Most common sites of recurrence were lymph nodes (12%) and urethra (18%) (World J Urol 2016;34:97)
- Clinical nodal assessment 93% accurate in predicting pathological lymph node involvement (World J Urol 2016;34:97)
- Median survival of 21 months (mean of 39 months) and 10 year survival of 25% for surgical patients (Hum Pathol 2018;72:35)
- Among patients without metastatic disease that underwent radical urethrectomy, 5 year cancer specific mortality free survival was 62% (87% for those with 36 month disease free interval) (J Surg Oncol 2024;129:1348)
- 5 year survival for T3 - 4 N0 - 2 patients was 54% (84% for those with 36 month disease free interval)
- Urothelial carcinoma
- 1 year overall survival rate of 73%; 3 year overall survival rate of 33% (Int J Surg Pathol 2022;30:15)
- Previous history of urothelial carcinoma of the bladder confers no effect on overall survival (Int J Surg Pathol 2022;30:15)
- Men
- Bulbar or penile urethral carcinoma (all histologic subtypes) yielded a mean 5 year overall survival of 50%, cancer specific survival 66% and relapse free survival of 58%; 62% with recurrence after surgery after a median of 6.3 months (Actas Urol Esp (Engl Ed) 2022;46:70)
- Proximal squamous cell carcinoma confers poor survival outcomes with a mean survival of 14 months and 90% develop distant metastatic disease (Eur Urol Focus 2021;7:163)
- Women
- Median overall survival (all histologic subtypes): 70 months (J Surg Oncol 2022;125:907)
- 5 year survival: 67% for stage 0 - II, 53% for stage III and 17% for stage IV (World J Urol 2013;31:147)
- Node positive and tumor size of ≥ 3 cm confer worse overall survival (J Surg Oncol 2022;125:907)
- 5 year survival: adenocarcinoma (31%), urothelial carcinoma (61%) and squamous cell carcinoma (64%) (World J Urol 2013;31:147)
- Advanced disease present: adenocarcinoma (65%), urothelial carcinoma (32%) and squamous cell carcinoma (53%) (World J Urol 2013;31:147)
Case reports
- 54 year old man with low grade papillary tumor of the anterior urethra (Ann Med Surg (Lond) 2022;76:103561)
- 67 year old woman with primary clear cell adenocarcinoma of the urethra (BMC Womens Health 2022;22:251)
- 68 year old man with urethral bulbar carcinoma with mixed urothelial and squamous differentiation (Mol Clin Oncol 2022;17:142)
- 76 year old woman with urothelial carcinoma with squamous metaplasia (Int J Surg Case Rep 2023;109:108505)
Treatment
- Among all patients with primary urethral carcinoma, rates of treatment with adjuvant radiotherapy and chemotherapy have increased over time (World J Urol 2013;31:147)
- Adjuvant radiotherapy: 28% of patients from 1989 to 1998; 43% from 1999 to 2008
- Adjuvant chemotherapy: 4% from 1989 to 1998; 12% from 1999 to 2008
- Men
- Locally advanced disease or metastasis: neoadjuvant therapy often recommended before surgical resection (Eur Urol Focus 2021;7:163)
- Distal (penile and bulbar carcinoma): partial penectomy (8 - 75%), total penectomy (17 - 54%) and transurethral resection (8 - 38%) (Int J Urol 2006;13:716, Actas Urol Esp (Engl Ed) 2022;46:70)
- Proximal: total penectomy (41%) and radical cystectomy / total penectomy with ileal conduit (59%) (Int J Urol 2006;13:716)
- Proximal squamous cell carcinoma: panurethrectomy (80%) and radical prostatectomy (20%) (Eur Urol Focus 2021;7:163)
- Women
- Among all histologic subtypes: 43% surgery alone, 16% radiotherapy alone and 22% surgery and radiotherapy (World J Urol 2013;31:147)
- T1 or Tis: 30% were treated with cystourethrectomy, 40% underwent local excision and 30% received chemotherapy and radiation (Clin Genitourin Cancer 2018;16:e1003)
- Locally advanced, nonmetastatic disease: 52% received multimodal therapy (radical cystourethrectomy, lymph node dissection and chemotherapy or radiation) and 48% received nonmultimodal therapy (radical cystourethrectomy alone, local excision with or without additional therapy or chemotherapy with or without radiation therapy), with no difference in survival (Clin Genitourin Cancer 2018;16:e1003)
Clinical images
Images hosted on other servers:


Penile urothelial carcinoma

Penile squamous carcinoma with fistula

Urothelial carcinoma at urethral orifice (female patient)
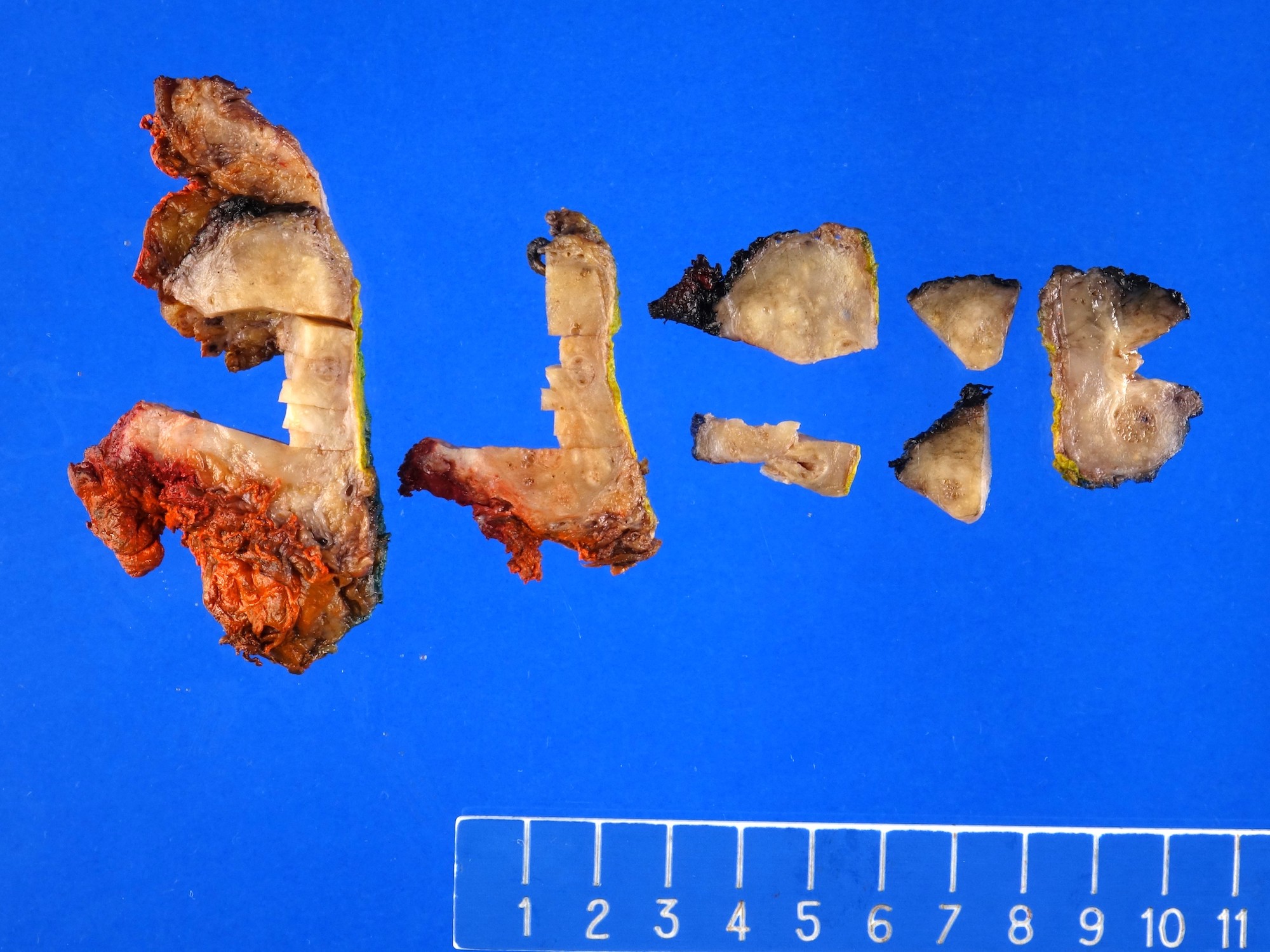
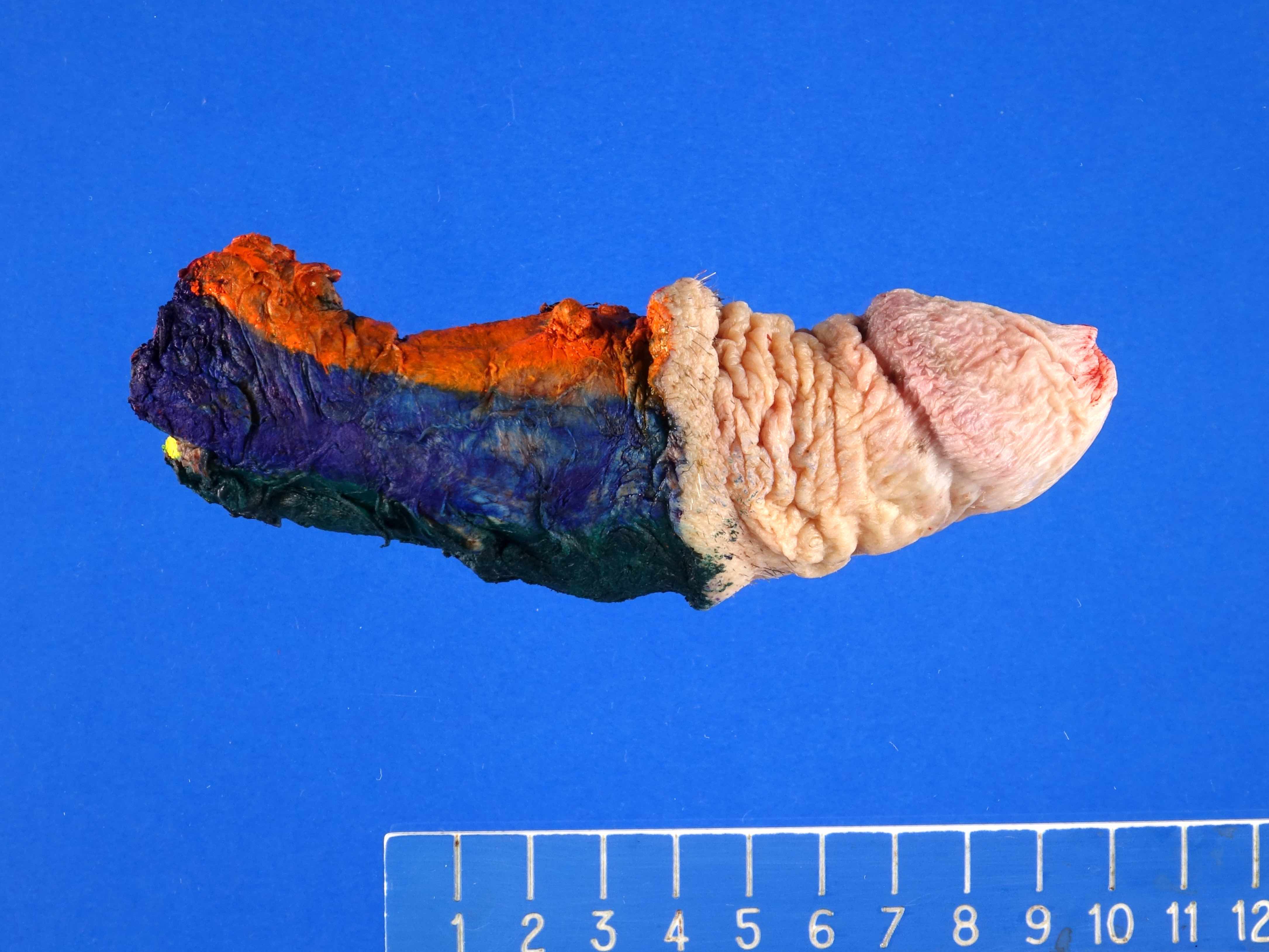
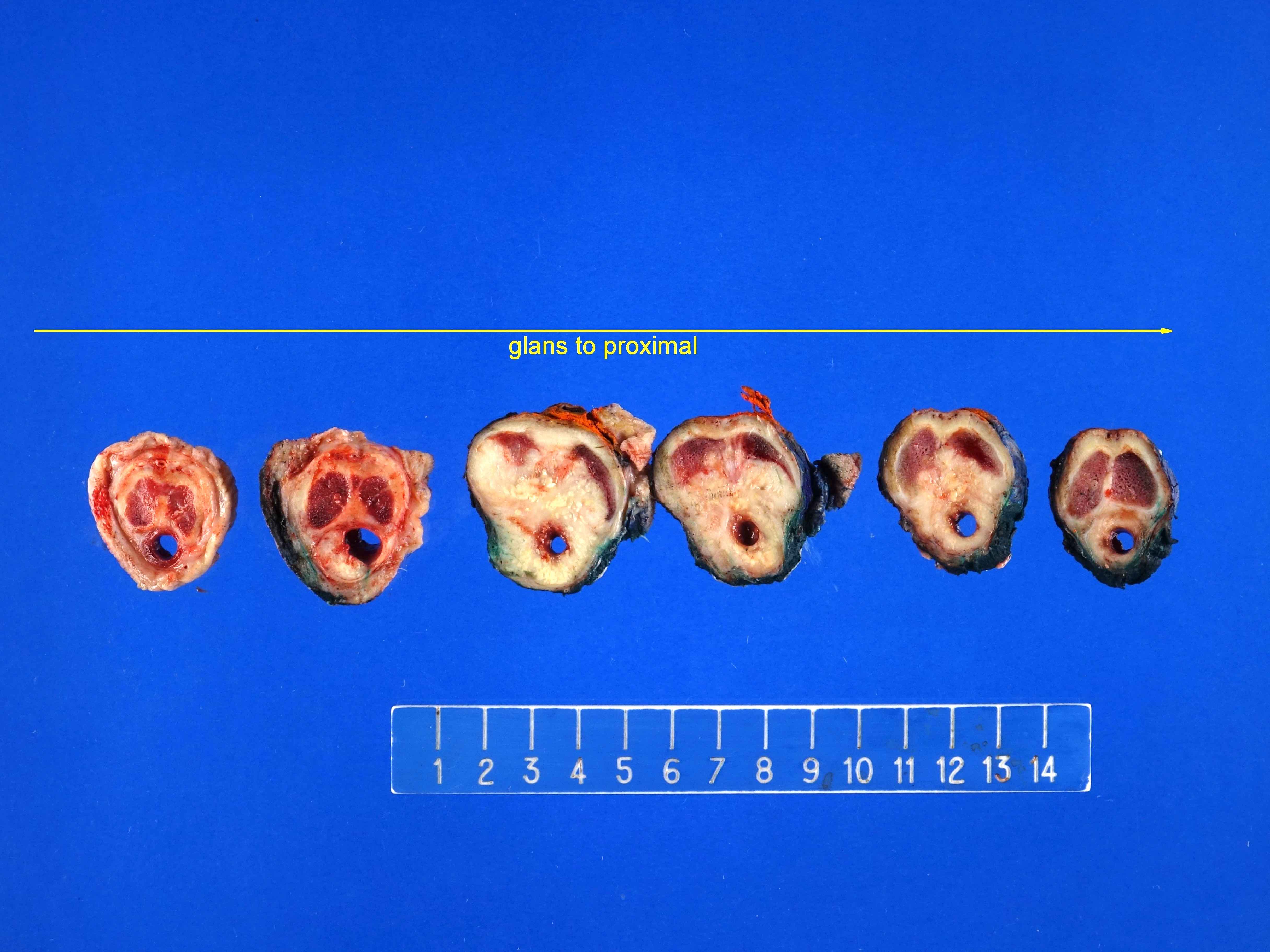
Gross description
- Poorly circumscribed mass with white to yellow-tan appearance (Hum Pathol 2018;72:35)
- Mean size: 3.7 cm (range: 0.5 - 6 cm) (Hum Pathol 2018;72:35)
- Range of appearances
- Fungated mass with protrusion to urethral lumen
- Flat lesions with invasion of surrounding tissue (Hum Pathol 2018;72:35)
Gross images
Contributed by Debra L. Zynger, M.D.
Urothelial carcinoma (prostate)
Urothelial carcinoma (penis)

Urothelial carcinoma (penile urethra)
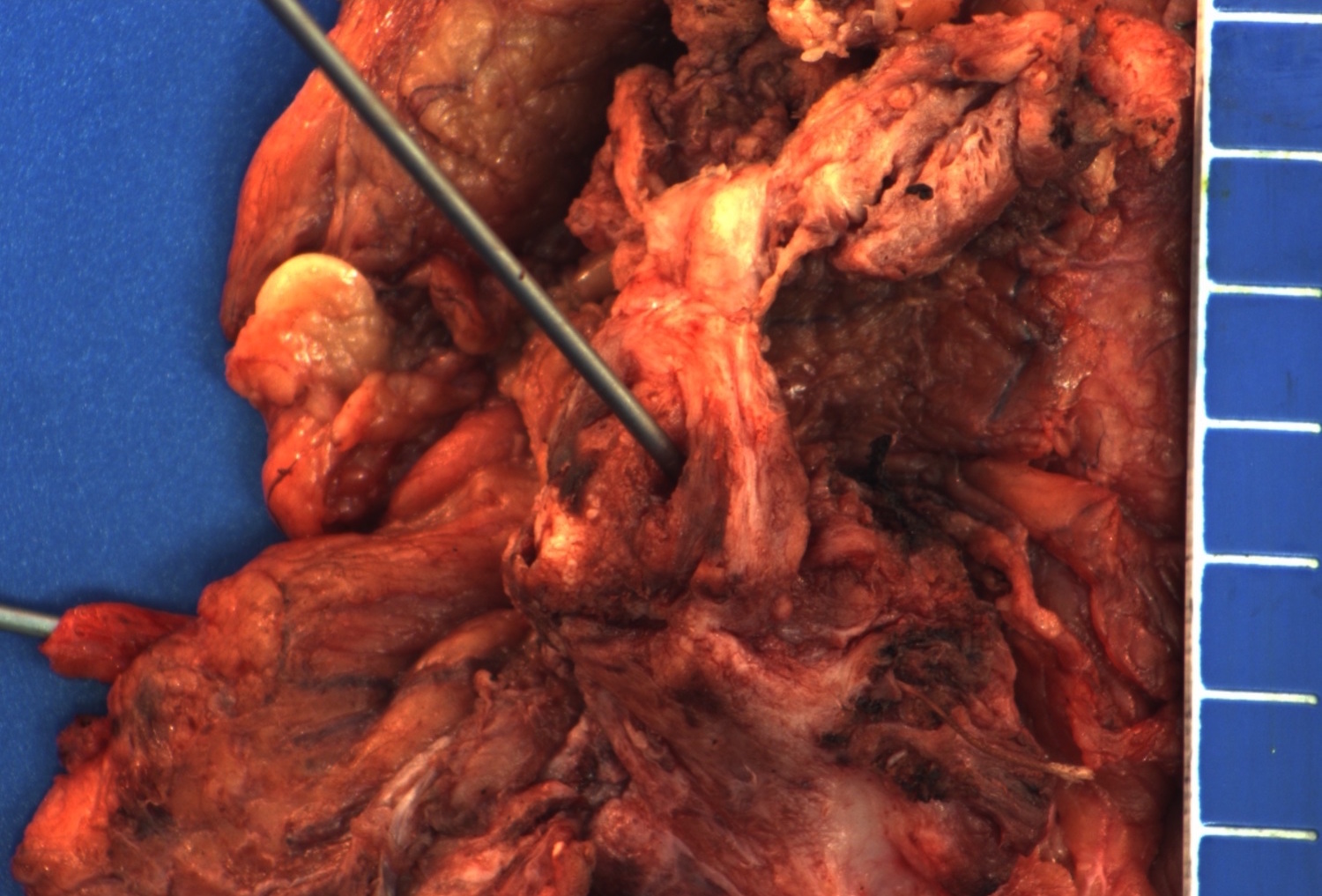
Squamous cell carcinoma (female urethra)
Microscopic (histologic) description
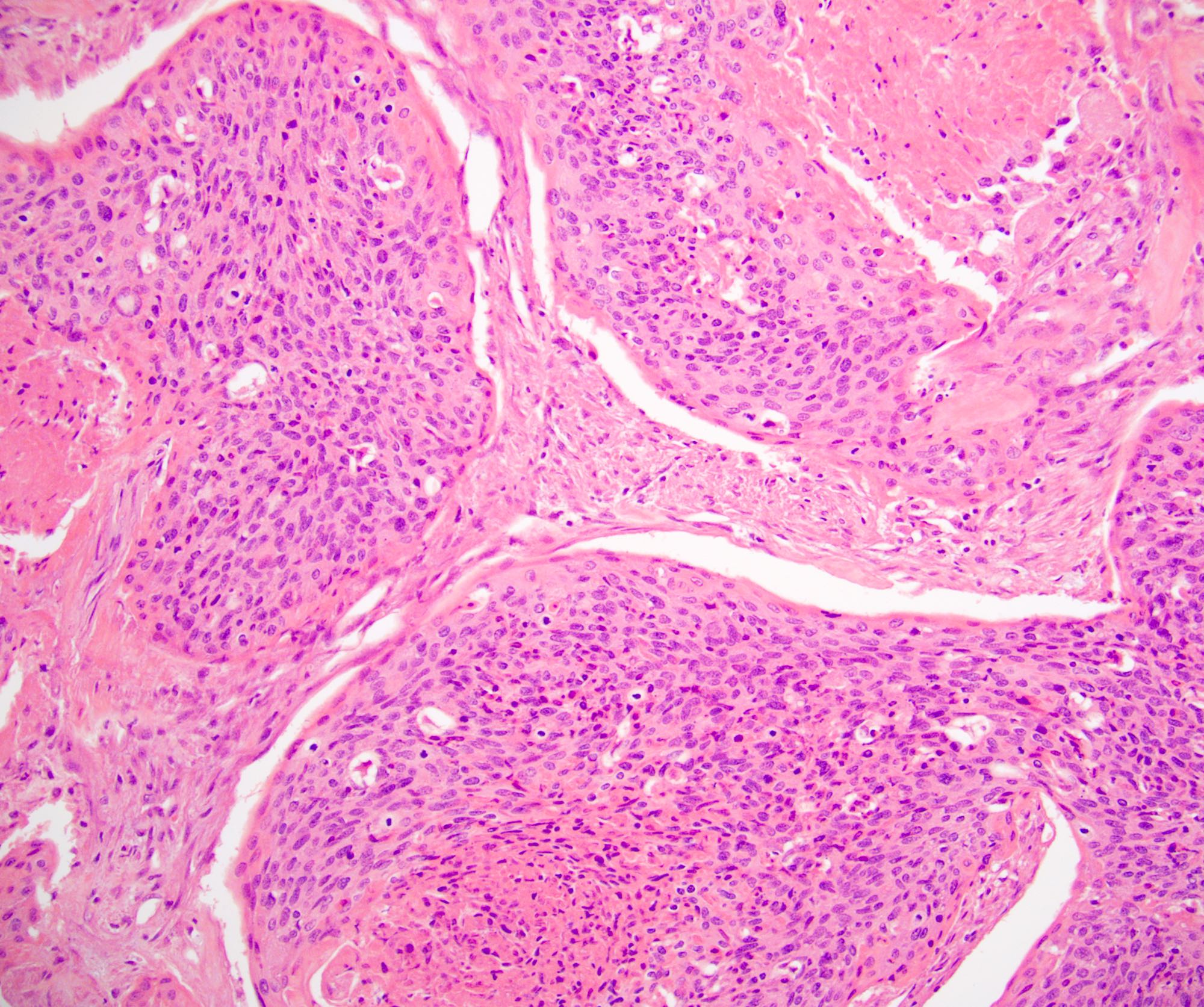
- Urothelial carcinoma
- Cytologically malignant urothelial cells with visible cell membranes, marked nucleomegaly, irregular nuclei, prominent nucleoli, dark chromatin and identifiable mitoses
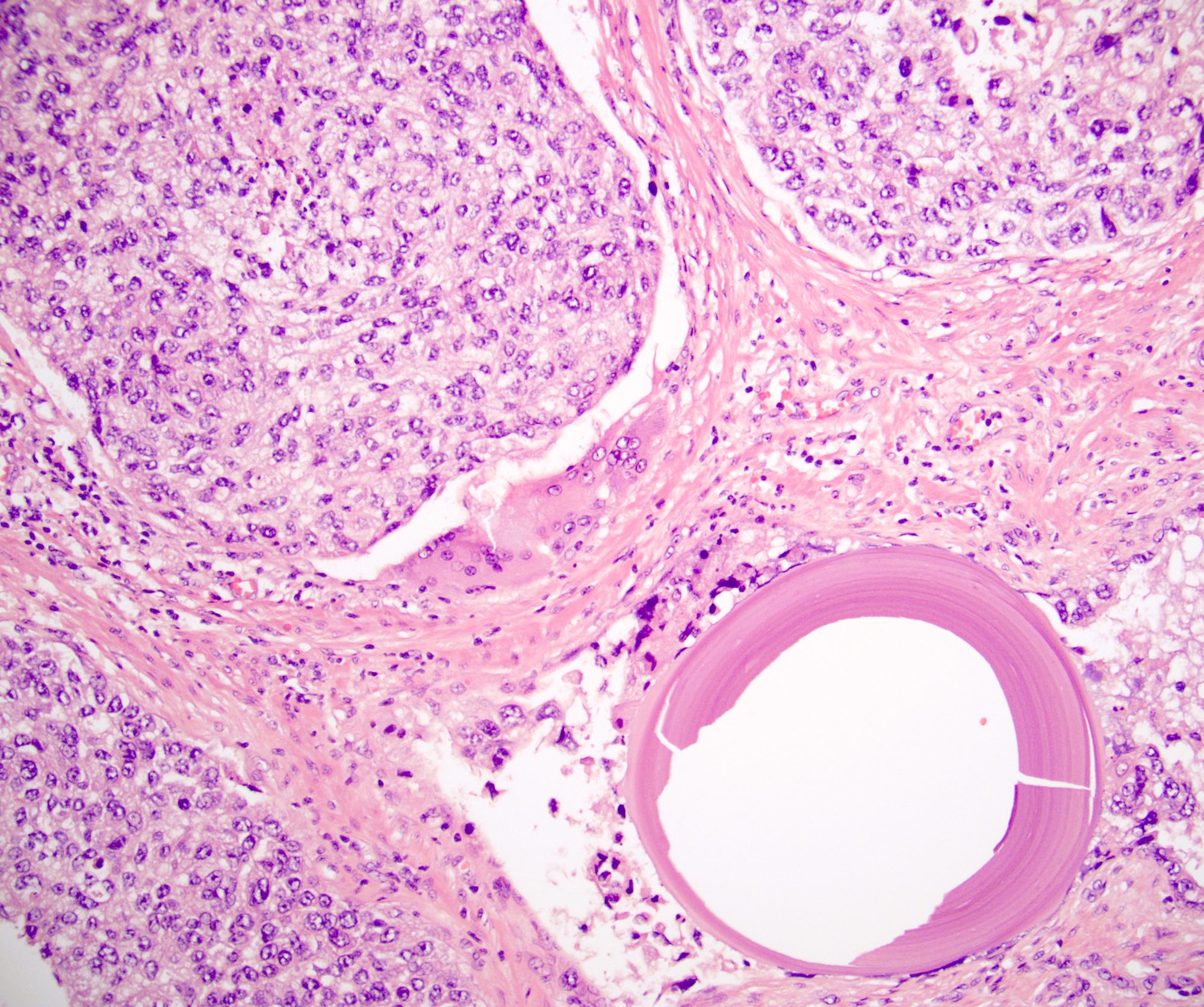
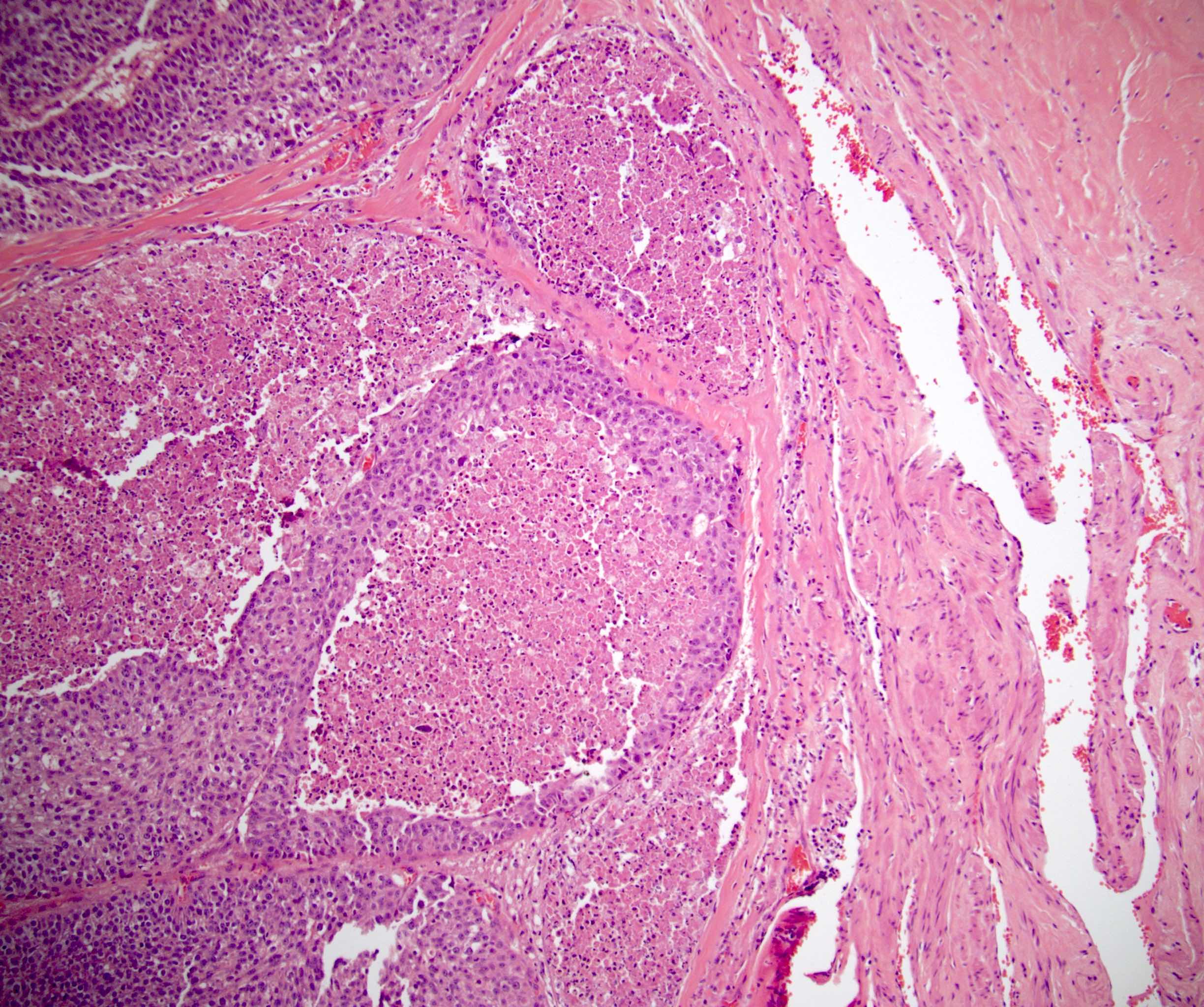
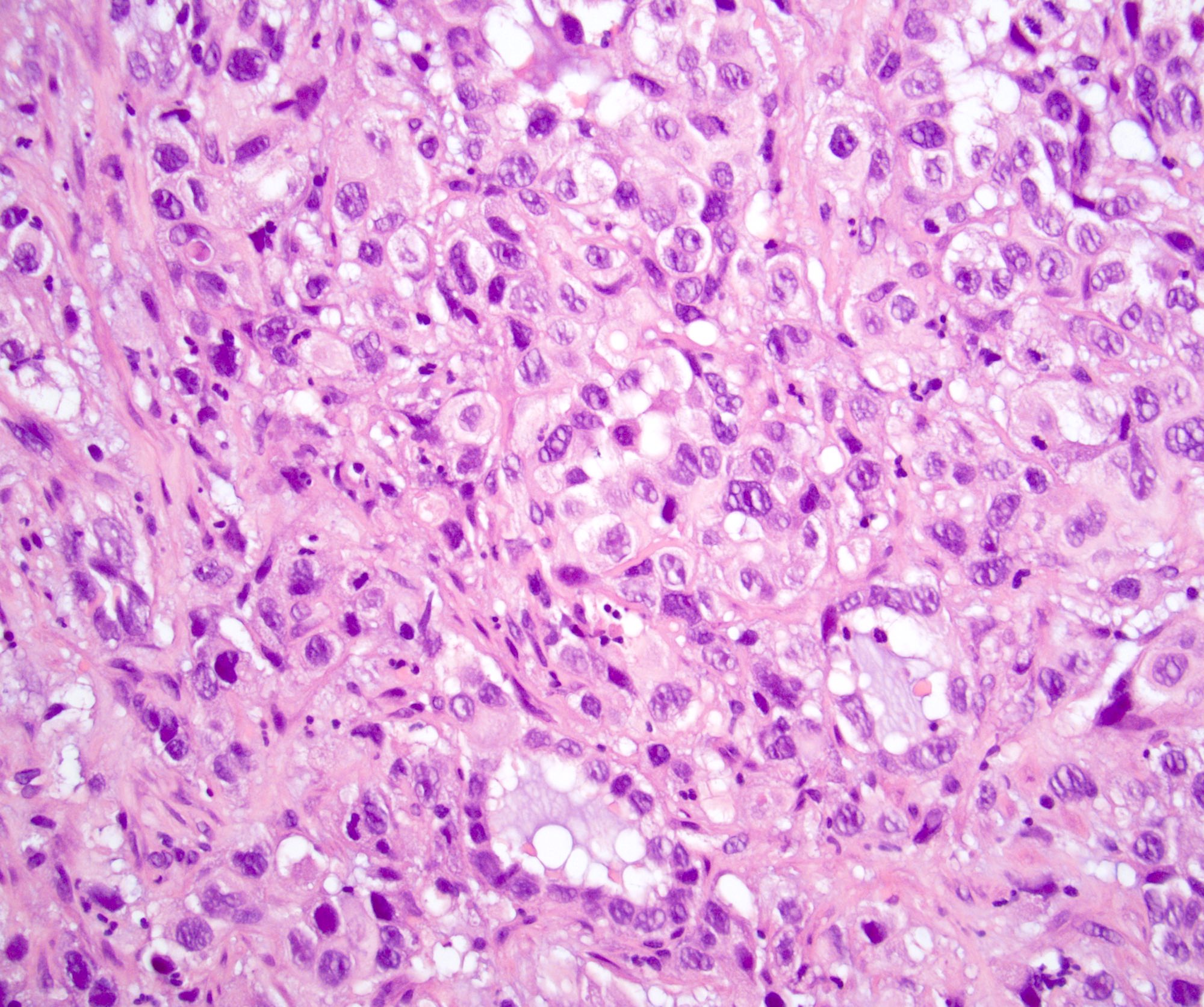
- Squamous cell carcinoma
- Sheets of large, pleomorphic tumor cells with focal or abundant keratinization (depending on the degree of differentiation), ample cytoplasm, intercellular bridges, prominent nuclear atypia and high mitotic activity
- Adenocarcinoma
- Composed of simple or pseudostratified columnar epithelium, apical cytoplasm and basally located hyperchromatic nuclei
- Occasional vacuolated cytoplasm with mucin or can be a true mucinous tumor with mucin pools
- Clear cell adenocarcinoma
- May have glandular, tubulocystic, solid / diffuse, papillary or micropapillary growth patterns
- Cuboidal, variably sized cells with abundant clear or eosinophilic cytoplasm and cytoplasmic vacuoles
- Nuclei that are hyperchromatic, pleomorphic and have prominent nucleoli
- Hobnail changes and extracellular mucoid material may be present
- Mitoses and necrosis are often seen
- One study proposed a hybrid tumor with urothelial and squamous features, similar to basaloid squamous cell carcinoma, as the histology for most urethral tumors (Hum Pathol 2018;72:35)
Microscopic (histologic) images
Contributed by Debra L. Zynger, M.D.
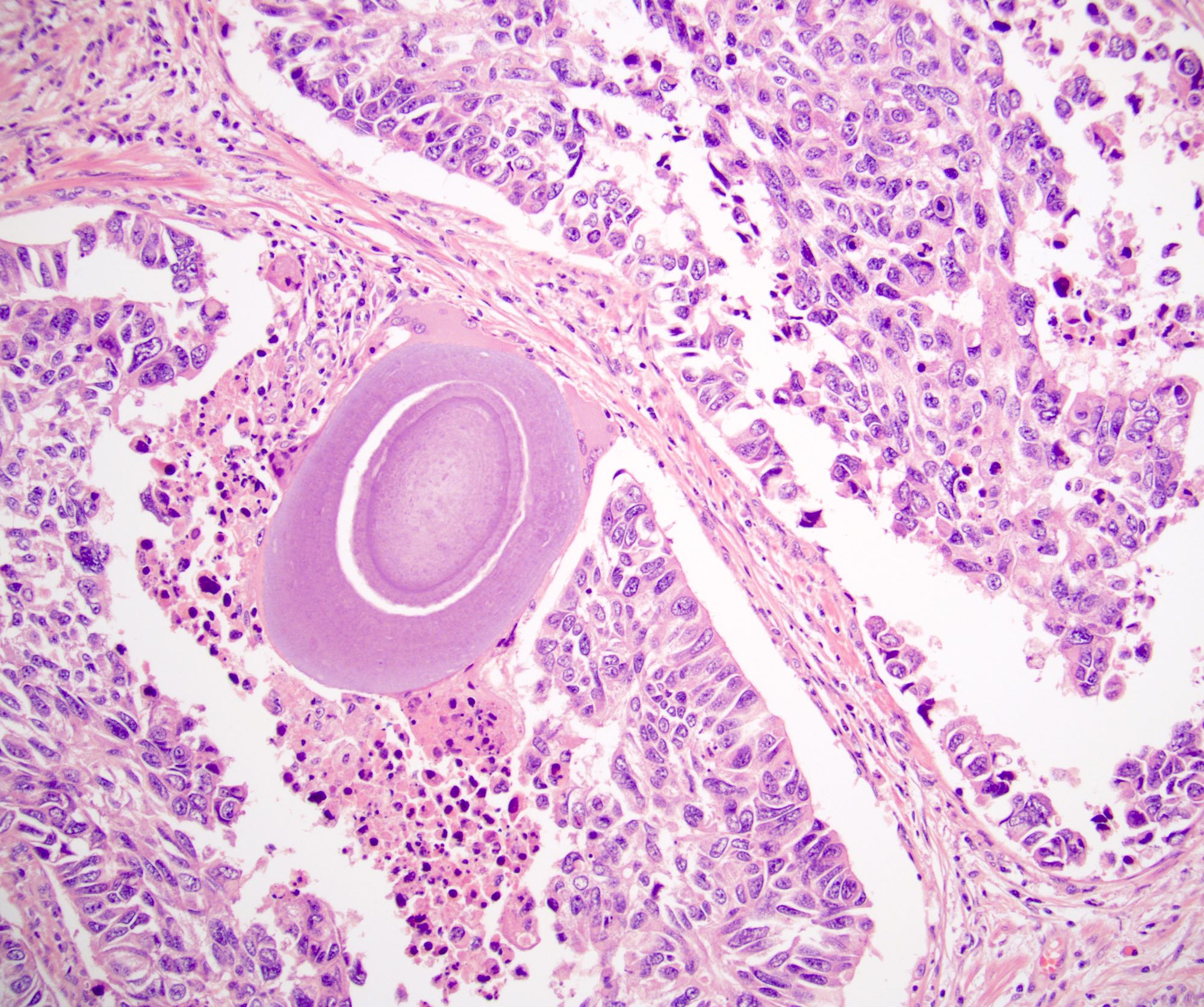
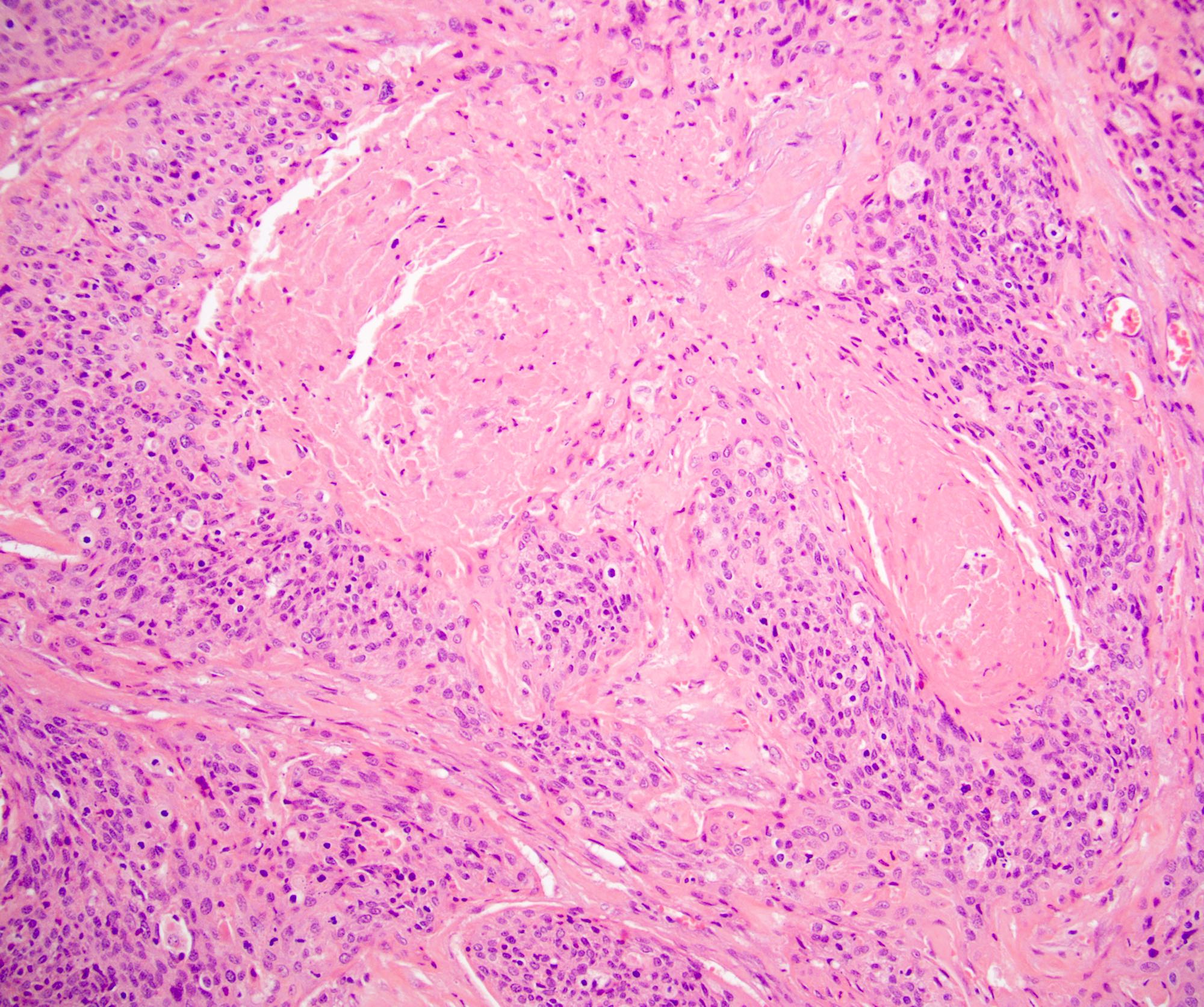
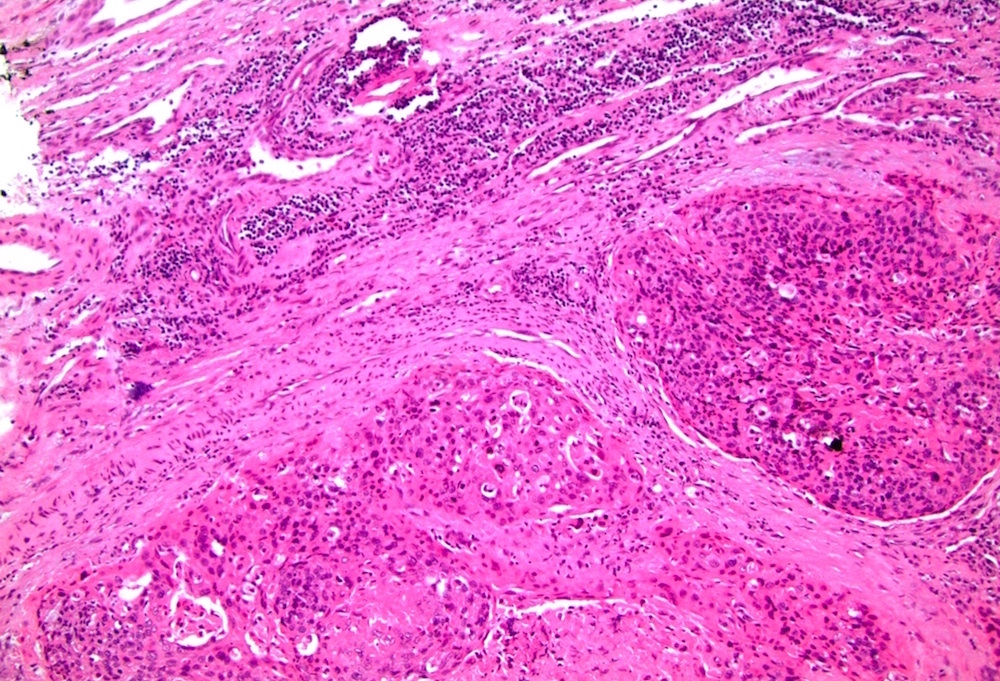
Urothelial carcinoma (prostate)

Urothelial carcinoma (penis)
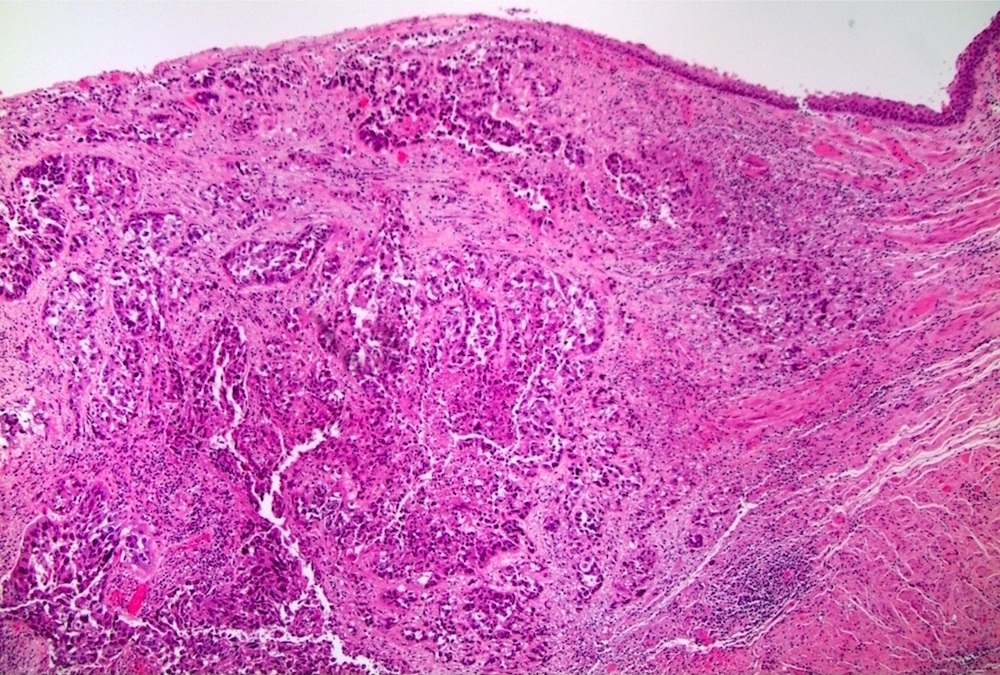
Squamous cell carcinoma (female urethra)
Metastatic squamous cell carcinoma (female urethra)
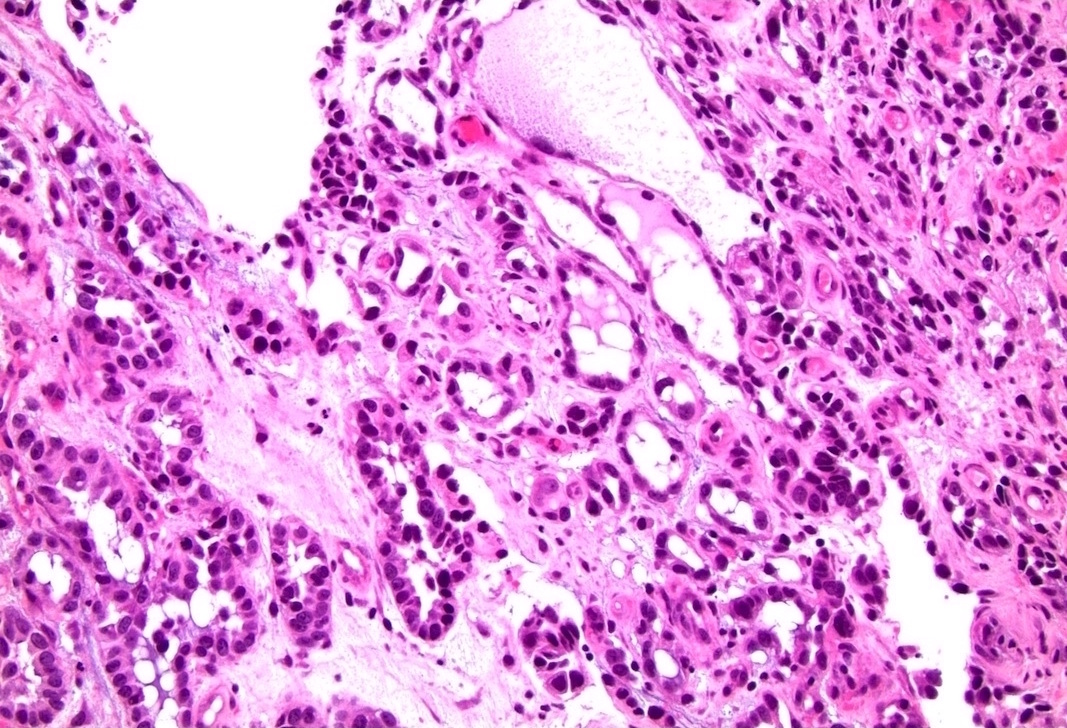
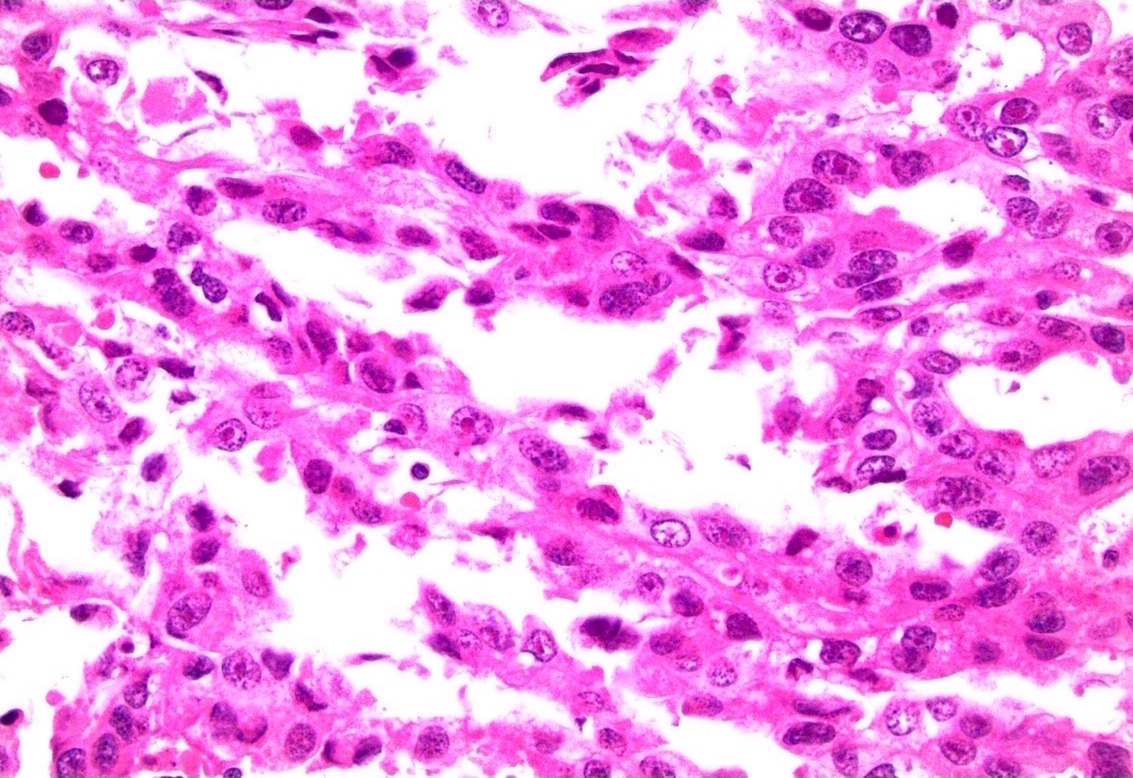
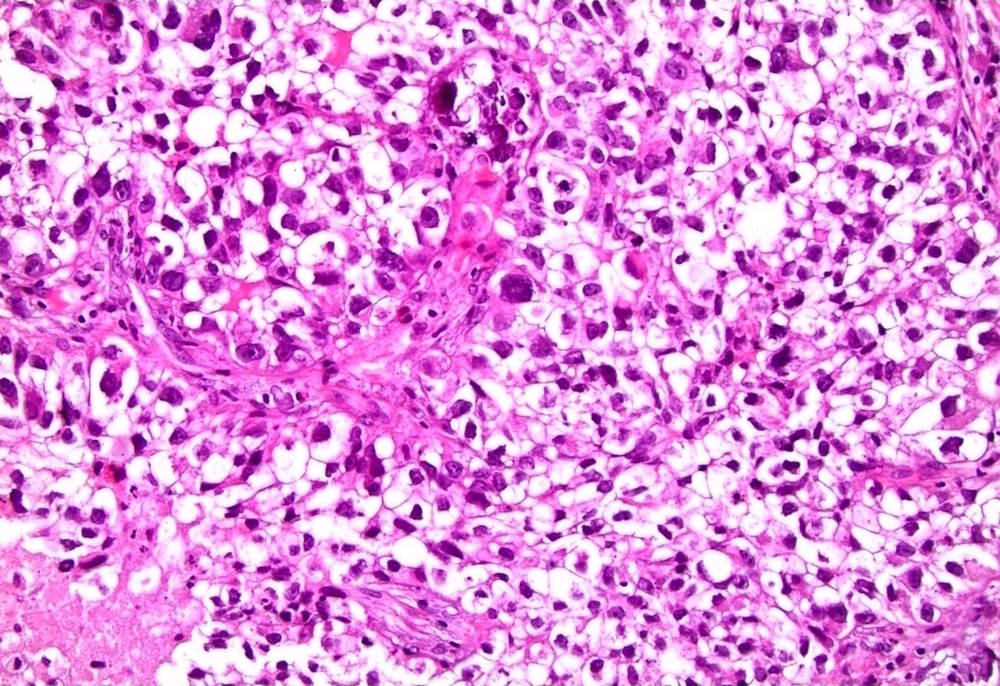
Clear cell adenocarcinoma (female urethra)
Virtual slides
Images hosted on other servers:

Urothelial carcinoma cytology (male urethra)
Cytology description
- Positive cytology seen in 59% with primary urethral carcinoma (Urology 2004;63:33)
- Sensitivity greatest for urothelial cell carcinoma (80%) and lowest for squamous cell carcinoma (50%) (Urology 2004;63:33)
Cytology images
Images hosted on other servers:

Clear cell adenocarcinoma (female urethra)
Positive stains
- Urothelial carcinoma (Hum Pathol 2013;44:2760)
- Squamous cell carcinoma
- Adenocarcinoma
- CK20 (variable), CDX2 (variable), cytoplasmic beta catenin
- Clear cell adenocarcinoma (Virchows Arch 2013;462:193, Arch Pathol Lab Med 2008;132:1417, Diagn Pathol 2022;17:87)
Negative stains
- Urothelial carcinoma (Hum Pathol 2013;44:2760)
- E-cadherin, CD44s, PAX8, PSA, PSAP
- Squamous cell carcinoma
- Adenocarcinoma
- Clear cell adenocarcinoma
Molecular / cytogenetics description
- PIK3CA found to be the most frequently targeted genomic alterations of advanced urethral carcinoma (Urol Oncol 2021;39:731.e1)
- Adenocarcinoma: PTEN was the top potentially targetable genomic alteration (Urol Oncol 2021;39:731.e1, Int J Surg Pathol 2021;29:447)
- Clear cell adenocarcinoma: focal copy number loss at SMAD4 and ARID2 loci, truncating mutation in ATM, ALK mutation (Am J Pathol 2014;184:584)
Sample pathology report
- Prostate, radical prostatectomy:
- Invasive urothelial carcinoma, high grade (see synoptic report)
- Surgical margins, negative for carcinoma
- Comment: The tumor expresses GATA3, CK7, CK20 and p63 and has focal, patchy expression of CK5/6.
- Penile urethra, biopsy:
- Carcinoma consistent with invasive urothelial carcinoma, high grade (see comment)
- Carcinoma invades corpus spongiosum
- Comment: The tumor expresses GATA3, CK7, CK20 and p63 and has focal, patchy expression of CK5/6.
- Female urethra, biopsy:
- Clear cell adenocarcinoma of the urothelial tract
- Comment: The tumor expresses PAX8, CK7 and AMACR and is negative for p16, CK20 and p63.
Differential diagnosis
- Mimickers of primary urethral urothelial carcinoma
- Urothelial carcinoma arising from the bladder:
- Clinical history, imaging and gross description are critical for differentiation
- Inverted urothelial papilloma:
- Typically develops at trigone of bladder but can develop anywhere that urothelium is present (Ann Diagn Pathol 2019;38:11)
- Absent mitotic activity without cellular atypia (Ann Diagn Pathol 2019;38:11)
- Urothelial carcinoma arising from the bladder:
- Mimickers of primary urethral squamous cell carcinoma
- Mimickers of primary urethral adenocarcinoma
- Prostatic adenocarcinoma:
- Colonic adenocarcinoma:
- Colonic adenocarcinoma expresses nuclear beta catenin but not CK7, p63 and GATA3
- Mimickers of clear cell adenocarcinoma
- Nephrogenic metaplasia:
- Minimal atypia or mitotic activity
- Overlapping immunoprofile
- Nephrogenic metaplasia:
Board review style question #1
A female urethra is resected with the primary tumor shown in the above image. The tumor strongly and diffusely expresses CK5/6 and p63 but is negative for PAX8 and only has weak expression of GATA3. What is the best diagnosis?
- Adenocarcinoma, intestinal type
- Clear cell adenocarcinoma
- Squamous cell carcinoma
- Urothelial carcinoma
Board review style answer #1
C. Squamous cell carcinoma. The most common 2 tumors primary to the female urethra are urothelial carcinoma and squamous cell carcinoma. Squamous cell carcinoma characteristically expresses CK5/6 and p63 and does not express PAX8. GATA3 can be positive but is often weaker in intensity compared to urothelial carcinoma. Answer A is incorrect because adenocarcinoma, intestinal type would show gland formation and be negative for CK5/6 and p63. Answer B is incorrect because clear cell adenocarcinoma would show tubules, hobnailed cells and clear cells and would express PAX8 but not CK5/6 and p63. Answer D is incorrect because urothelial carcinoma usually has a strong expression of GATA3 and does not have a diffuse and strong expression of CK5/6. Both urothelial carcinoma and squamous cell carcinoma express p63.
Comment Here
Reference: Urethral carcinoma
Comment Here
Reference: Urethral carcinoma
Board review style question #2
A female urethral tumor shown above contains tubules, hobnailed cells and patches of clear cells. PAX8 is positive. What is the best diagnosis?
- Adenocarcinoma, intestinal type
- Clear cell adenocarcinoma
- Squamous cell carcinoma
- Urothelial carcinoma
Board review style answer #2
B. Clear cell adenocarcinoma. Clear cell adenocarcinoma can have many growth patterns including glandular, tubulocystic, solid / diffuse, papillary or micropapillary. The cells can be cuboidal or hobnailed and have clear or eosinophilic cytoplasm. The tumor typically expresses PAX8. Answers A, C and D are incorrect because adenocarcinoma, intestinal type, squamous cell carcinoma and urothelial carcinoma do not have the described morphology and they do not express PAX8.
Comment Here
Reference: Urethral carcinoma
Comment Here
Reference: Urethral carcinoma

