

Bladder & urothelial tract
Urothelial neoplasms - noninvasive
Noninvasive papillary urothelial carcinoma low grade
Editorial Board Member: Maria Tretiakova, M.D., Ph.D.
Editor-in-Chief: Debra L. Zynger, M.D.


Last author update: 26 April 2021
Last staff update: 11 November 2021
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: Low grade papillary urothelial carcinoma [TIAB] pathology

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Prognostic factors | Case reports | Treatment | Gross description | Frozen section description | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Cytology images | Positive stains | Negative stains | Electron microscopy description | Molecular / cytogenetics description | Videos | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Yu YHS, Downes MR. Noninvasive papillary urothelial carcinoma low grade. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/bladderlgpap.html. Accessed December 25th, 2024.
Definition / general
- Neoplastic proliferation of the urothelium in a papillary configuration, with no invasion through the basement membrane
- Low grade architectural and cytologic abnormality, absence of high grade features, such as irregular nuclei with frequent, prominent nucleoli and mitoses, pleomorphism
Essential features
- Noninvasive papillary urothelial neoplasm with low grade cytoarchitectural abnormality
- Loss of polarity, rare mitoses, subtle variation in nuclear size but no significant pleomorphism
- Immunohistochemistry not helpful for diagnosis
- Hematuria common presentation
- Disease related death and progression is rare but recurrence common
Terminology
- Grade 1 and subset of grade 2 carcinomas from 1973 WHO classification
ICD coding
- ICD-O: 8130/2 - papillary transitional cell carcinoma, noninvasive
Epidemiology
- Incidence: 5 per 100,000 people per year (J Urol 1999;162:702)
- M:F = 3:1
- Median age: 70 years
- Lynch syndrome, especially MSH2 carriers, clinically earlier stage and low grade (Int J Urol 2018;25:151)
Sites
- Most commonly found in posterior and lateral walls of bladder
- 85% of urothelial neoplasms of renal pelvis are papillary but only 34% of them are low grade (Mod Pathol 2005;18:11)
- Anywhere with urothelium
Pathophysiology
- Normal urothelium, through loss of chromosome 9, becomes hyperplasia
- Followed by further genetic alterations, such as mutations in FGFR3, which activates mitogen activated protein (MAP) kinase pathway, leading to development of low grade noninvasive papillary urothelial carcinoma (Int J Clin Oncol 2008;13:287)
- Other genetic alterations: PIK3CA, loss of 11p or CCND1
Etiology
- Smoking (Int J Epidemiol 2016;45:857)
- Occupational exposure to chlorinated hydrocarbons, polycyclic aromatic hydrocarbons and aromatic amines (Eur Urol 2014;66:59)
- Arsenic exposure (Cancer Epidemiol Biomarkers Prev 2014;23:1529)
Clinical features
- Most common presentation: painless hematuria (gross or microscopic)
- Gross hematuria associated with more advanced pathologic stage (BJU Int 2016;117:783)
- Disease associated death and progression is rare (< 5%)
- Recurrence common (48 - 71%)
Diagnosis
- Cystoscopy: exophytic lesion, solitary or multiple, with varying size
- CT urography or ultrasound
- Urine cytology
Radiology description
- CT urography shows hydronephrosis and filling defects (Abdom Radiol (NY) 2018;43:663)
- Ultrasound can detect hydronephrosis and any intraluminal bladder masses
Prognostic factors
- WHO / ISUP histologic grade
- Concomitant urothelial carcinoma in situ: higher recurrence rate
- Multifocal disease: higher disease associated mortality and progression
- High Ki67: poor prognosis (Int J Mol Sci 2018;19:2548)
- Mutations in FGFR3 and PIK3CA lower recurrence rate (Cancer Res 2006;66:7401)
- PTEN deletions: increased recurrence rate (Virchows Arch 2018;472:969)
Case reports
- 31 year old man with low grade papillary noninvasive urothelial carcinoma mimicking xanothogranulomatous pyelonephritis (Int J Immunopathol Pharmacol 2020;34:2058738420925720)
- 49 year old woman with urachal low grade noninvasive papillary urothelial carcinoma (BMJ Case Rep 2013;2013:bcr2013200635)
- 75 year old woman with multicentric synchronous low grade noninvasive papillary carcinoma involving vagina, bladder and renal pelvis (Virchows Arch 2017;471:347)
Treatment
- Surgical: transurethral resection
- Adjuvant: usually not indicated for low grade
- Mitomycin C
Gross description
- Exophytic papillary lesions, single or multiple; can vary greatly in size
Frozen section description
- Papillary lesion with fibrovascular core, low grade nuclear features
- Infrequent mitoses, basal / suprabasal location
- Reference: Taxy: Biopsy Interpretation - The Frozen Section, 2nd Edition, 2013
Microscopic (histologic) description
- Neoplastic urothelium lining fibrovascular cores
- Long, slender papillae with minimal fusing or branching
- Orderly architecture at low magnification, some loss of polarity and mild pleomorphism at medium magnification
- Cells generally uniform in size, may have slight variation but no significant nuclear pleomorphism or nucleomegaly, occasional slight irregularities in nuclear contour
- Mitoses may be present but not atypical and usually confined to lower half of urothelium
- Inverted growth pattern (exophytic and endophytic components) may be present
Microscopic (histologic) images
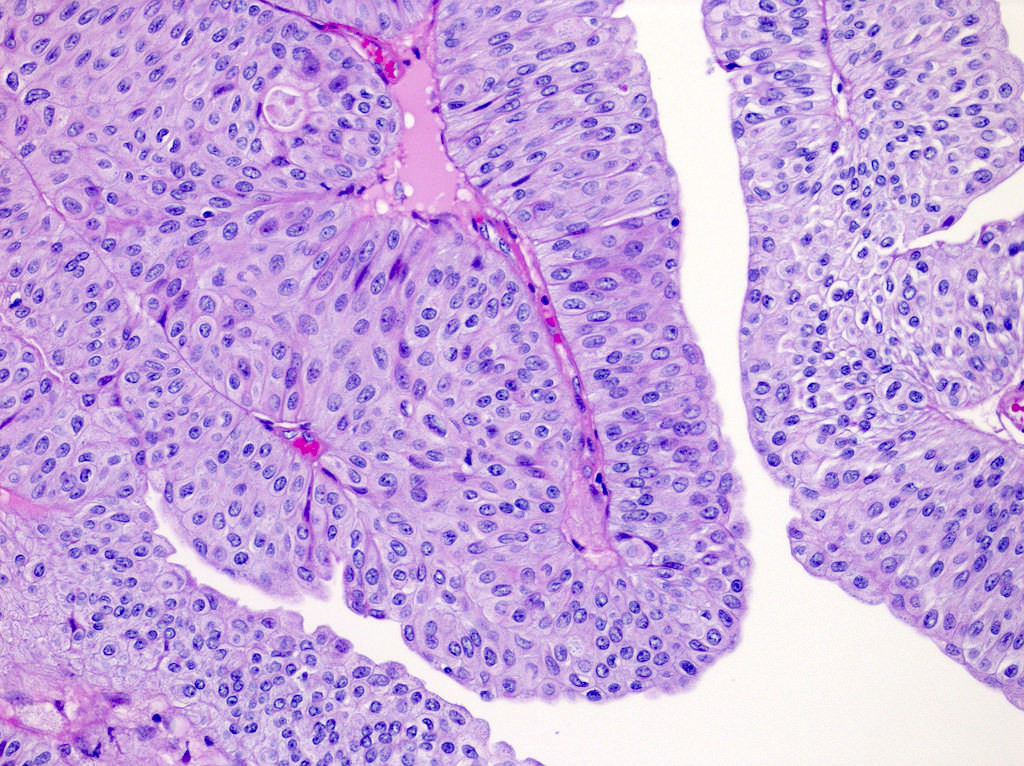
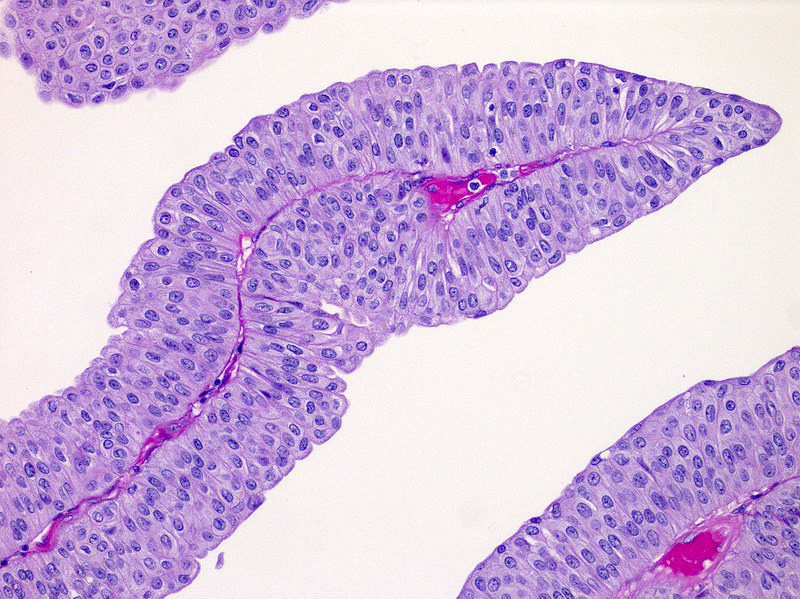
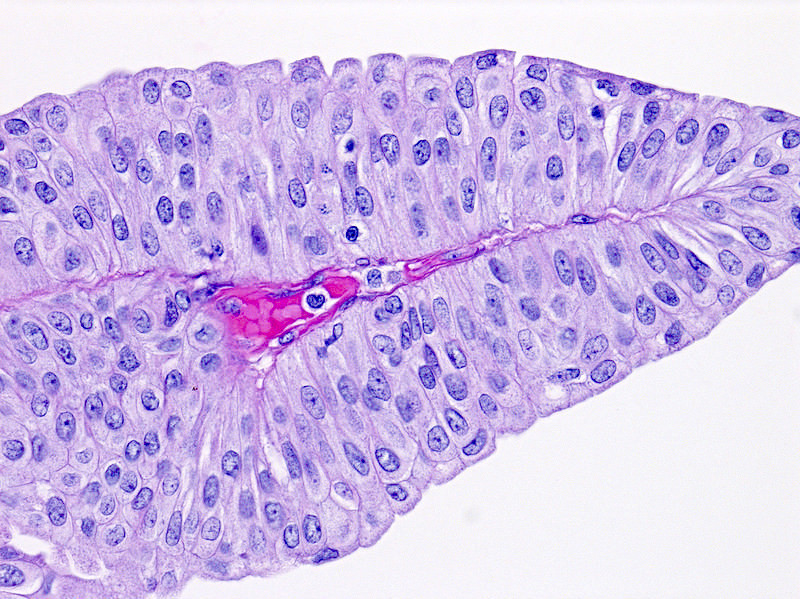
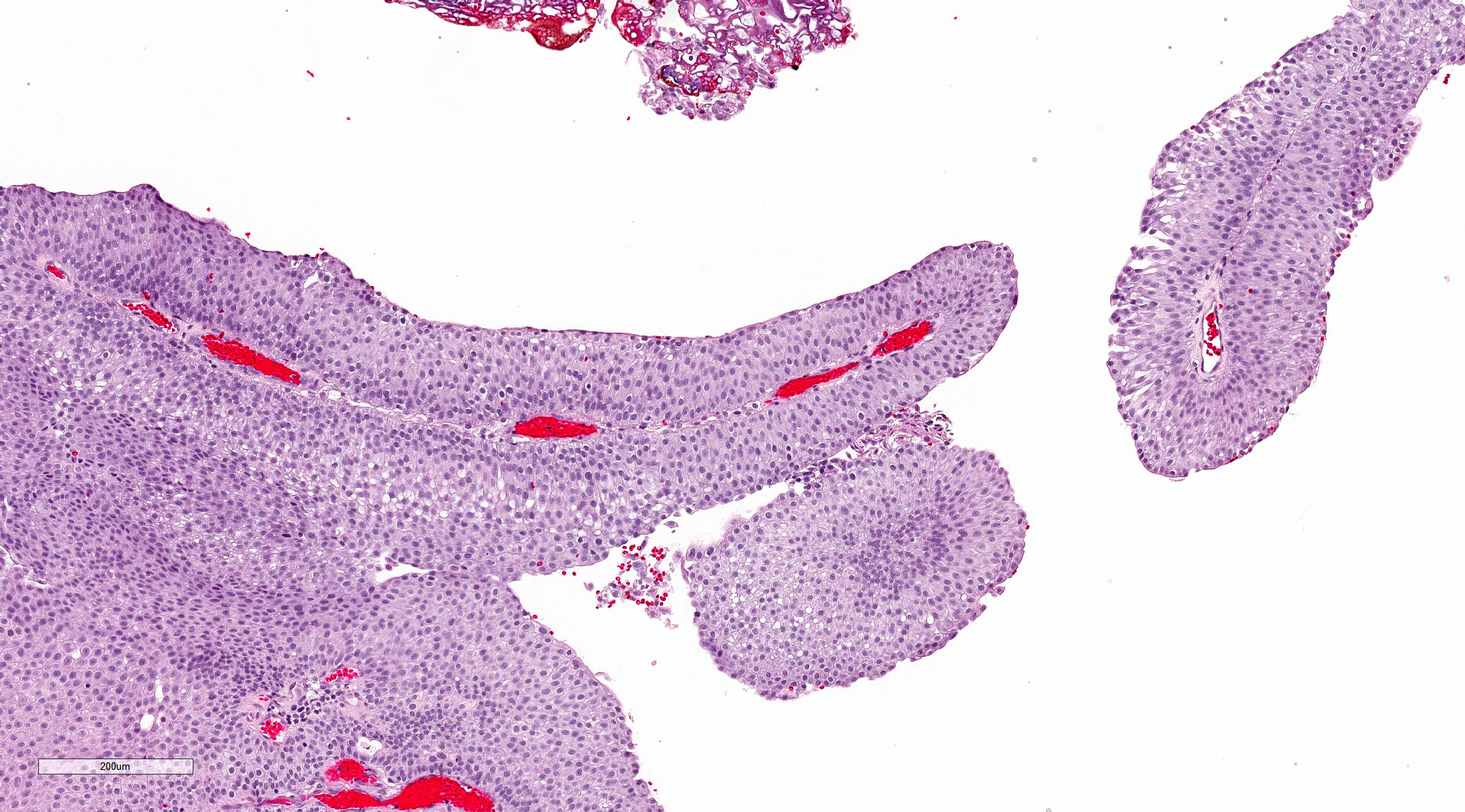
Contributed by Michelle R. Downes, M.D., Nicole K. Andeen, M.D. and Maria Tretiakova, M.D.
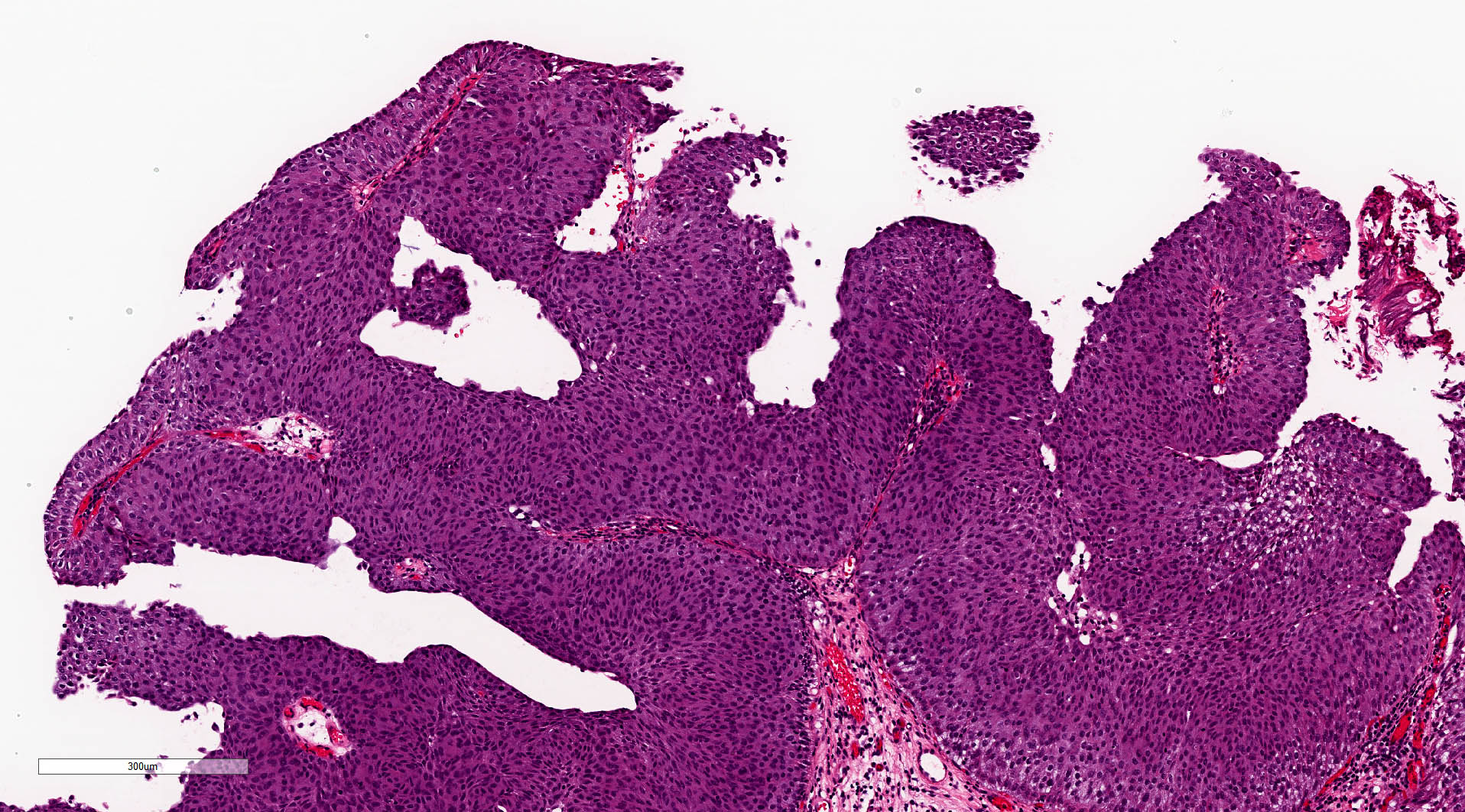
Fibrovascular cores lined by neoplastic urothelium
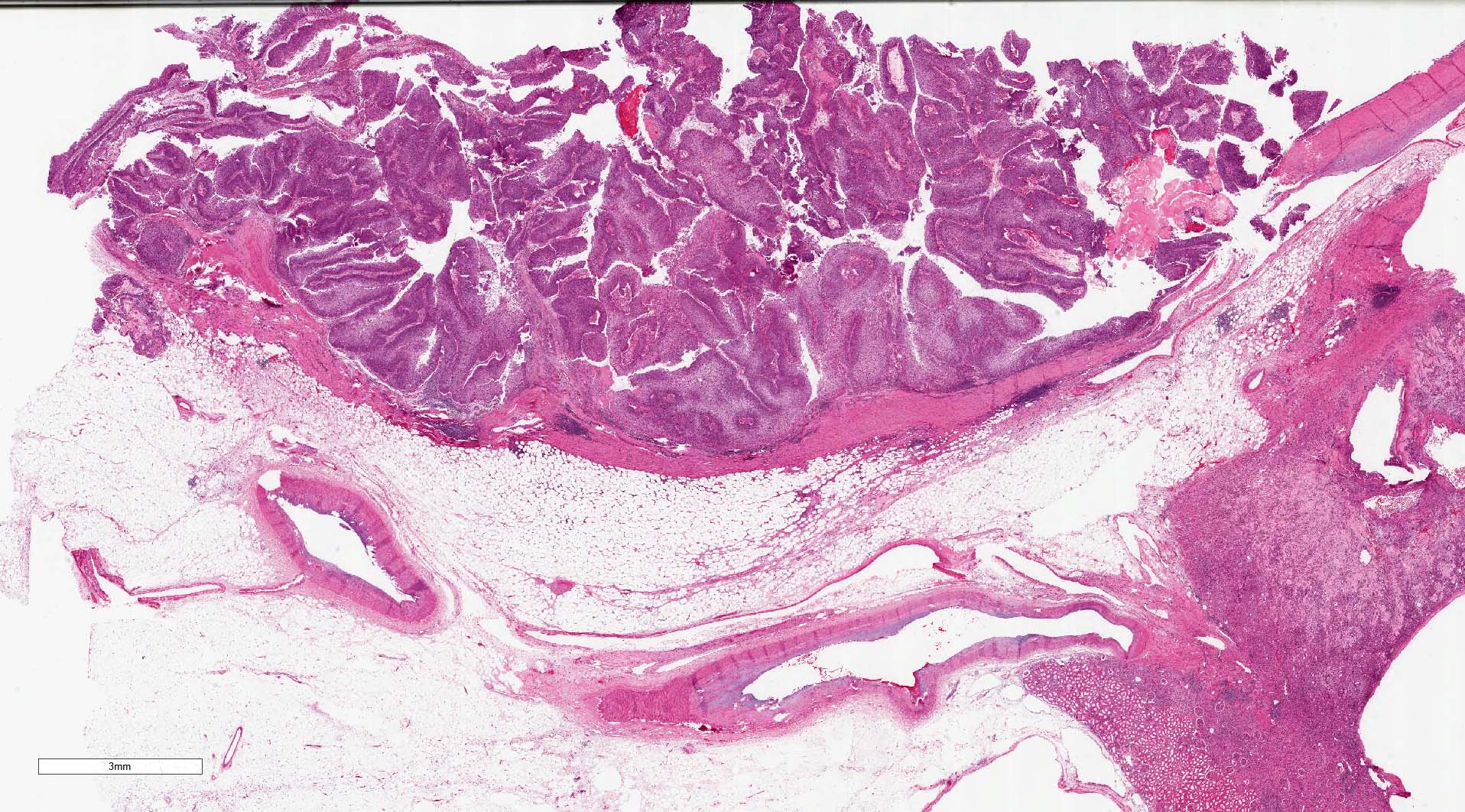
Noninvasive papillary, low grade urothelial carcinoma
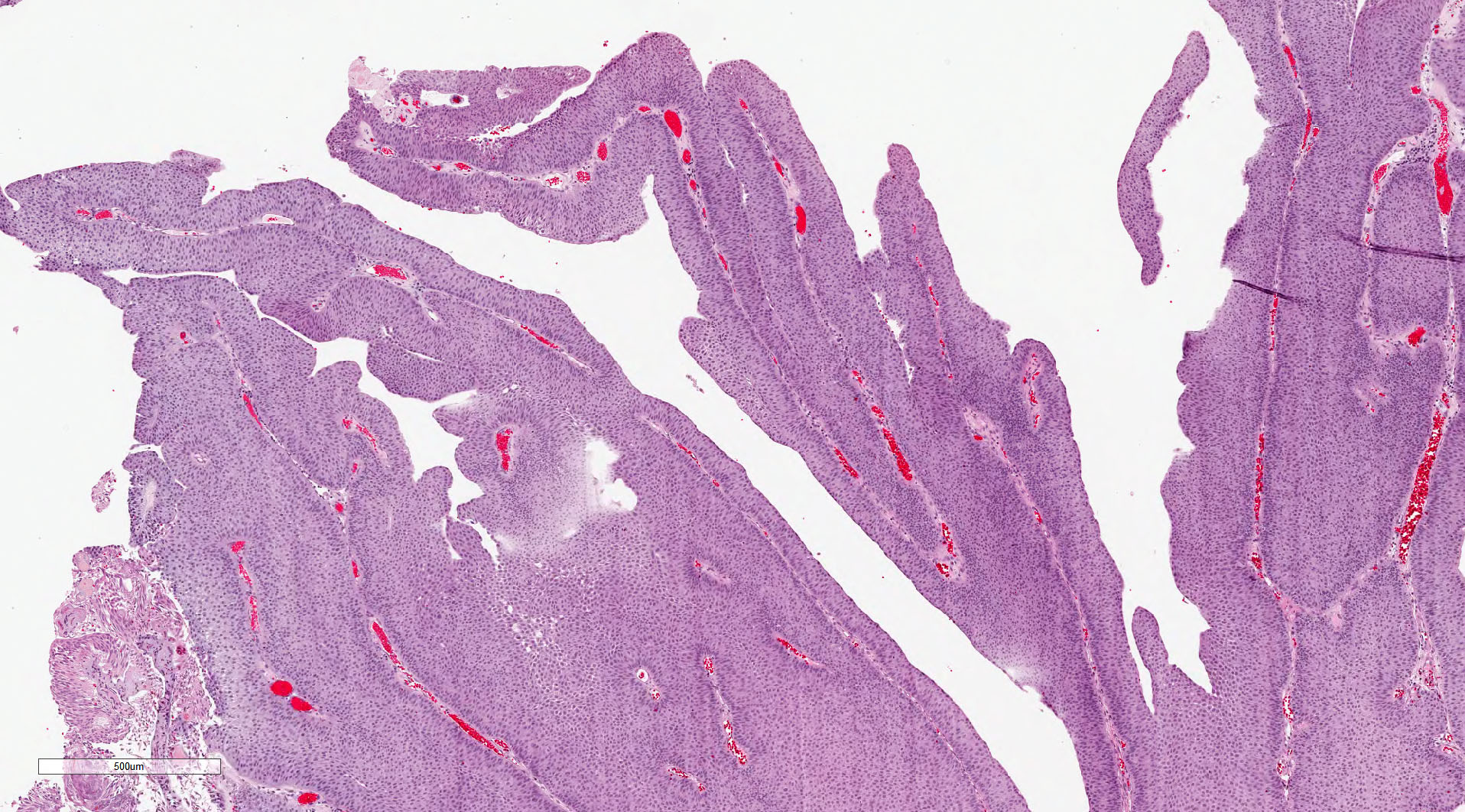
Papillary architecture

Architectural features
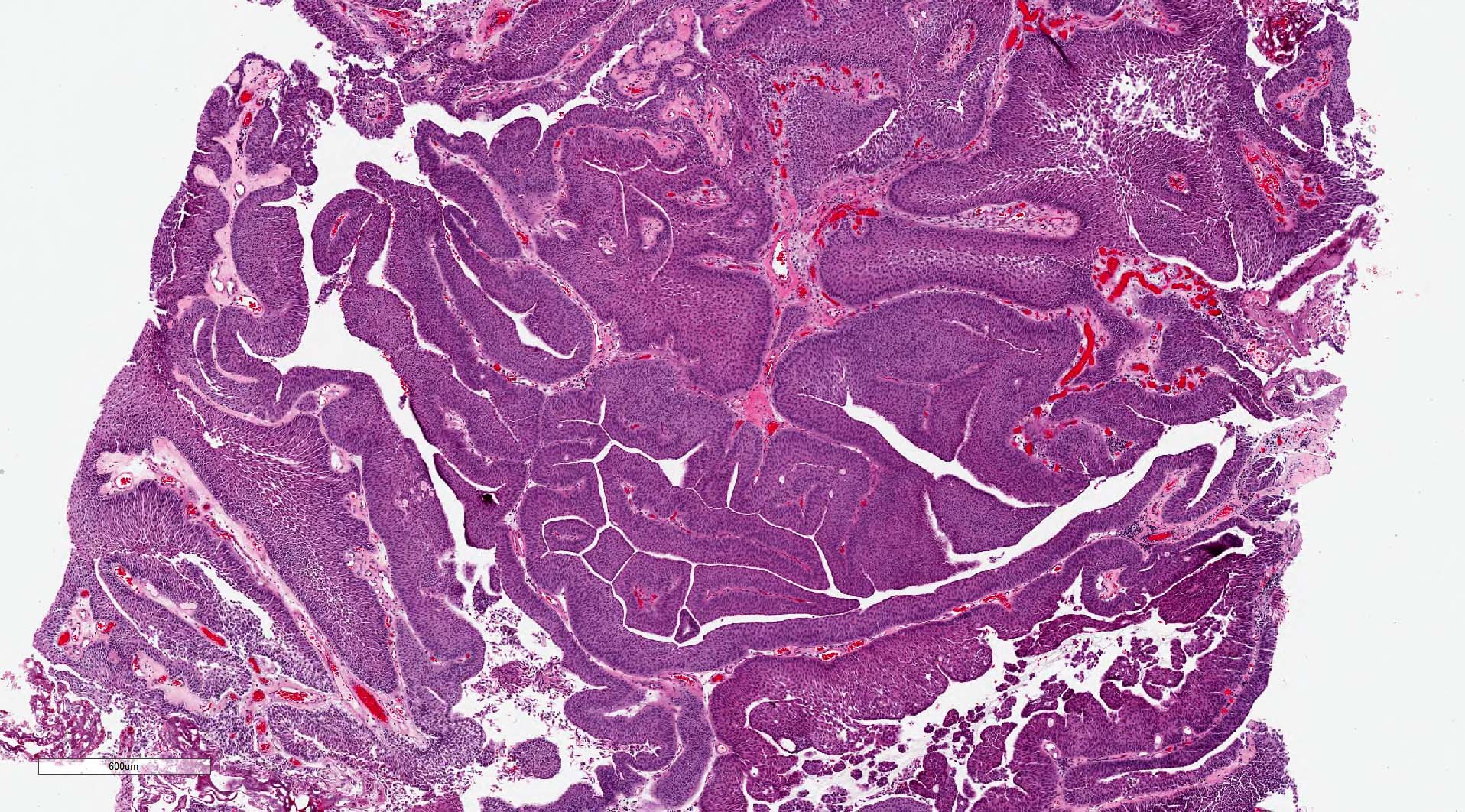
Endophytic growth pattern
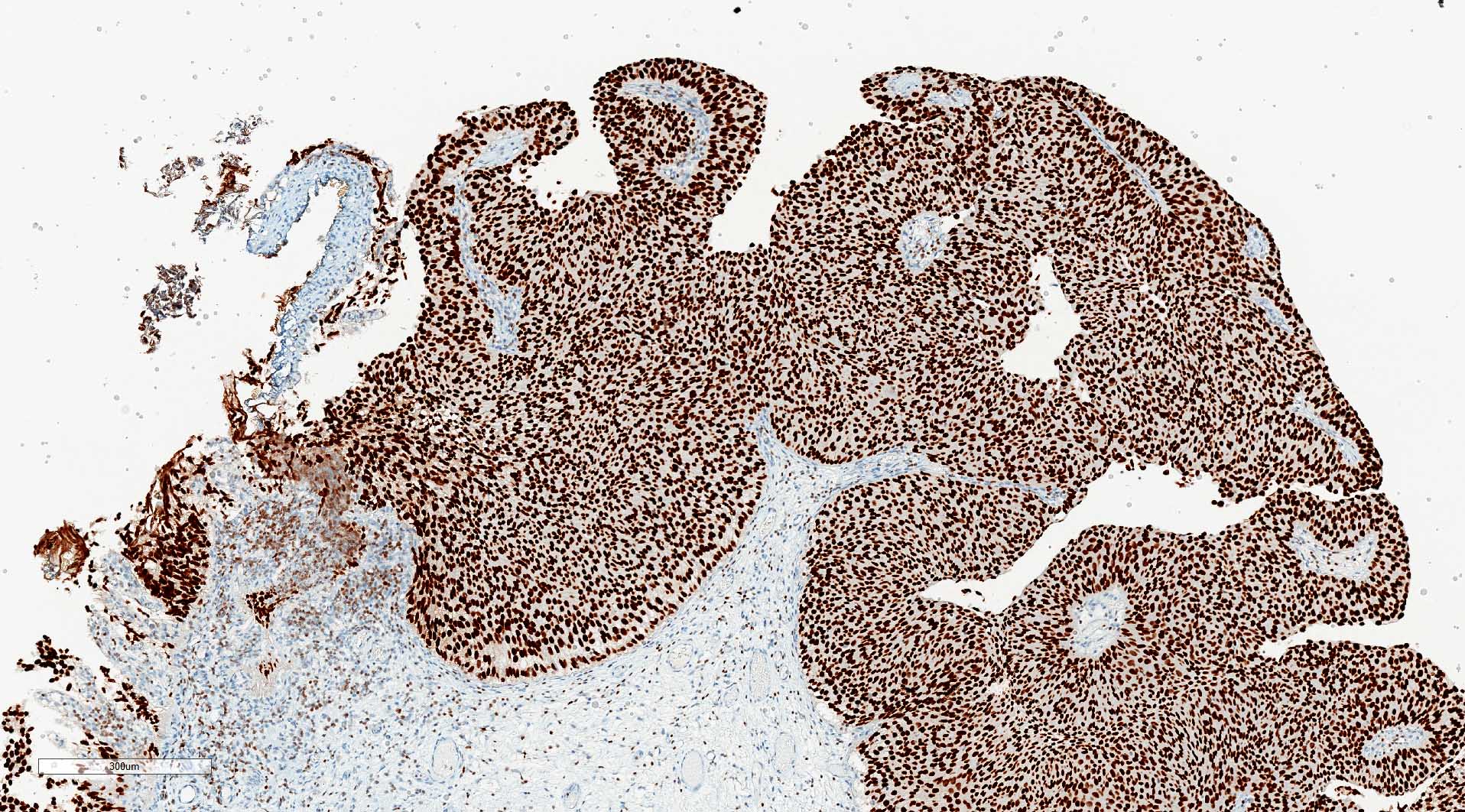
GATA3
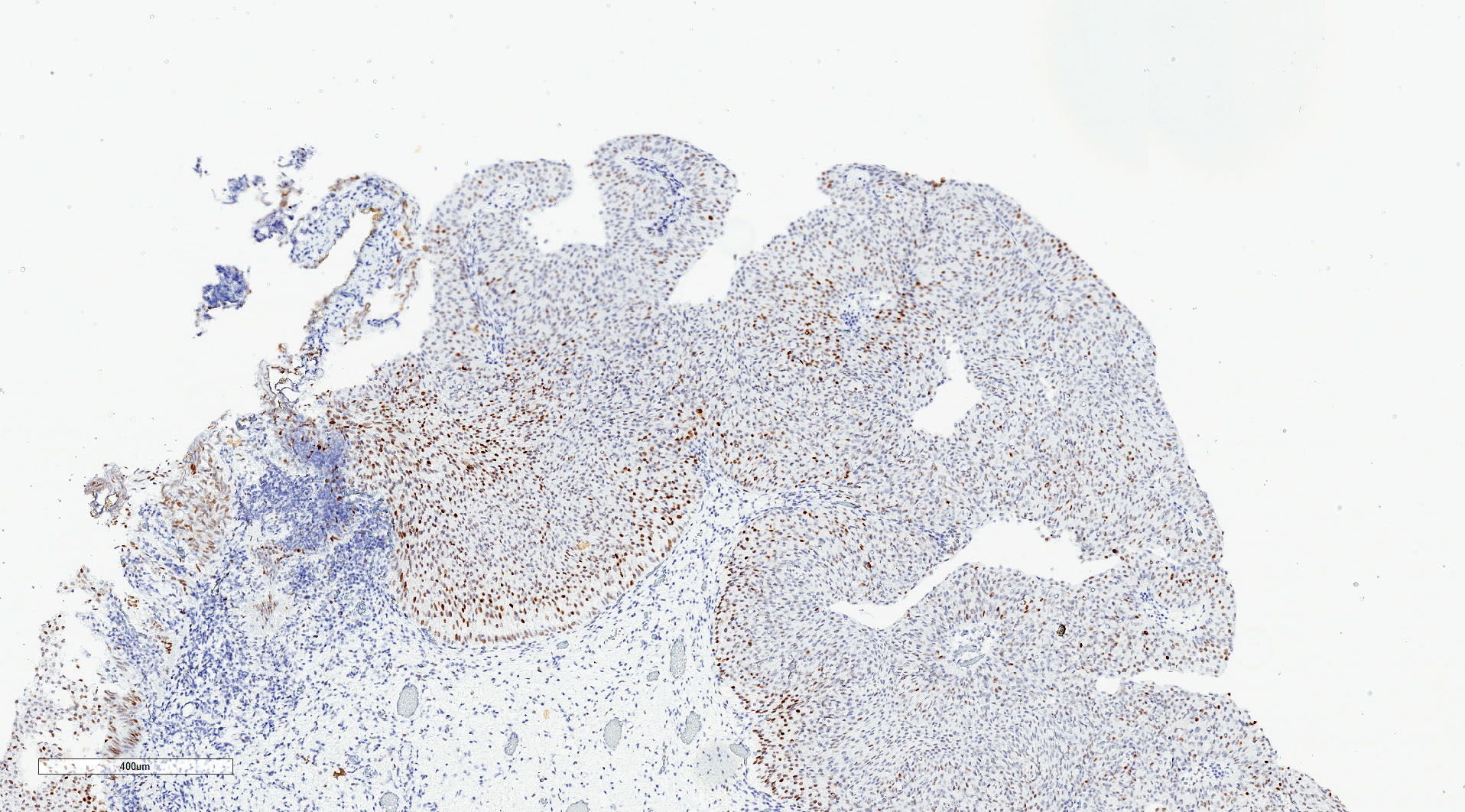
p53
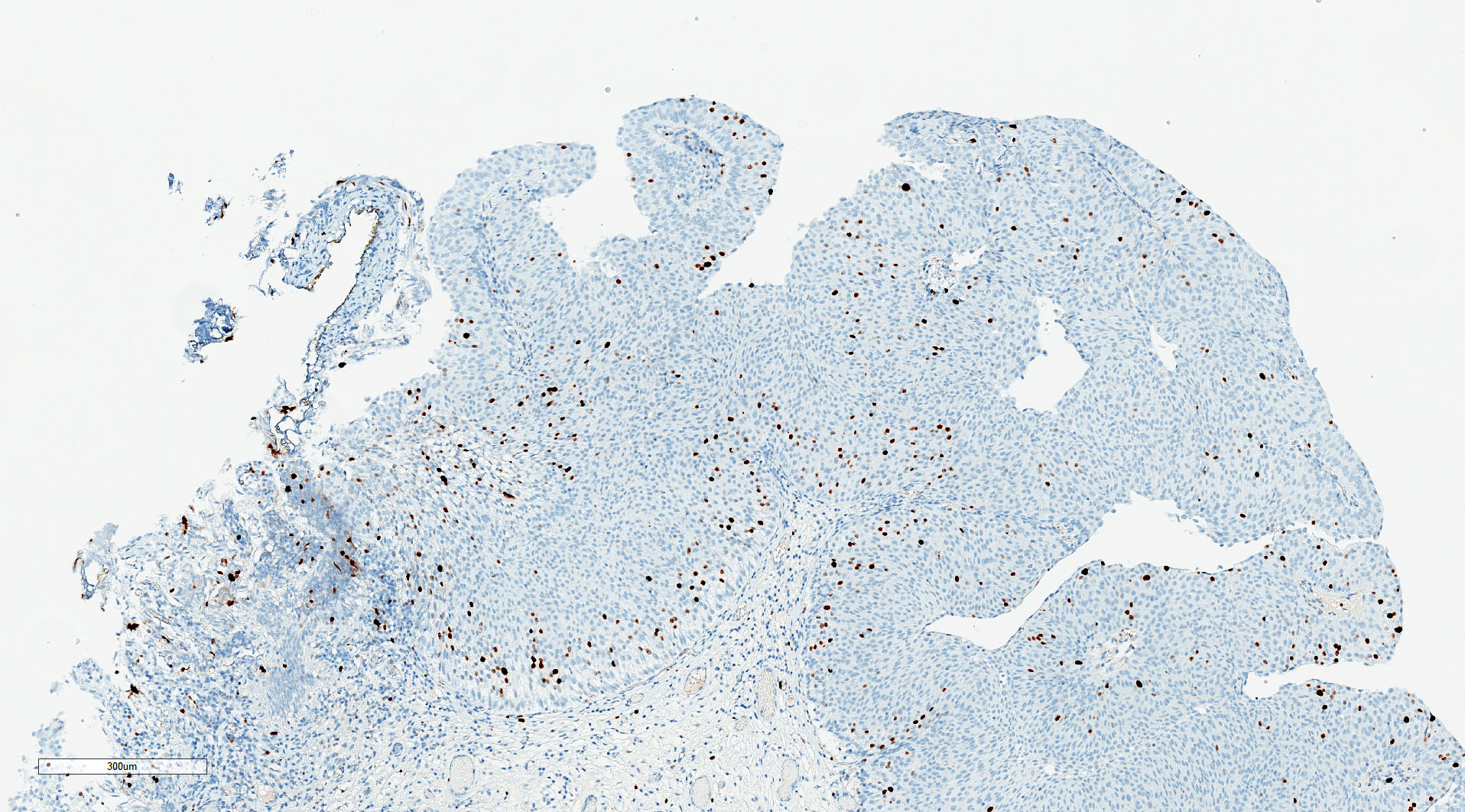
Ki67
Noninvasive papillary urothelial carcinoma, low grade (pTa)
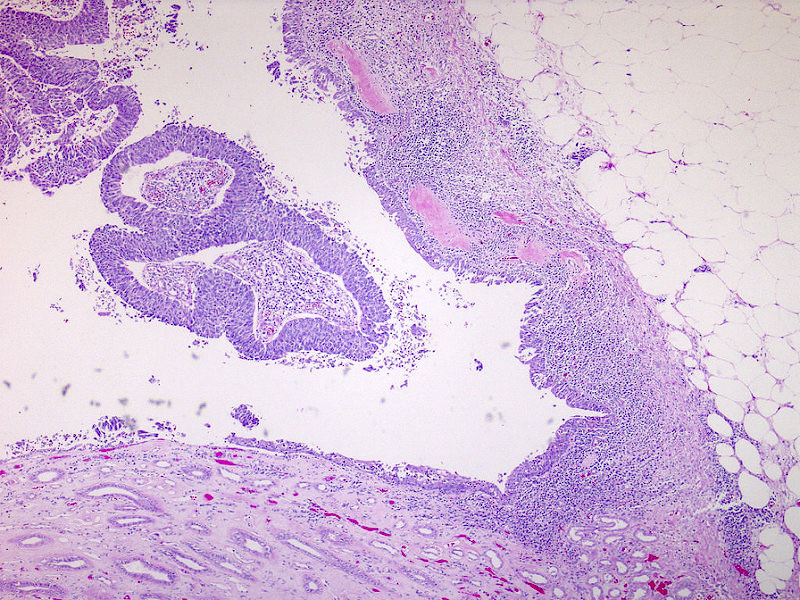
Papillary urothelial
carcinoma, absent
muscularis
Cytology description
- Lower sensitivity in low grade tumors compared with high grade (Urol Oncol 2015;33:66.e25)
- 2016 Paris Working Group reporting system recommended
- 3 dimensional cellular clusters or papillae with fibrovascular cores
- Increase in monotonous single cells with increased nuclear/cytoplasmic ratio and irregular nuclear contours
- For additional information, refer to the topic cytology-neoplastic
Cytology images
Contributed by Zeina Ghorab M.D. and Bonnie Choy, M.D.
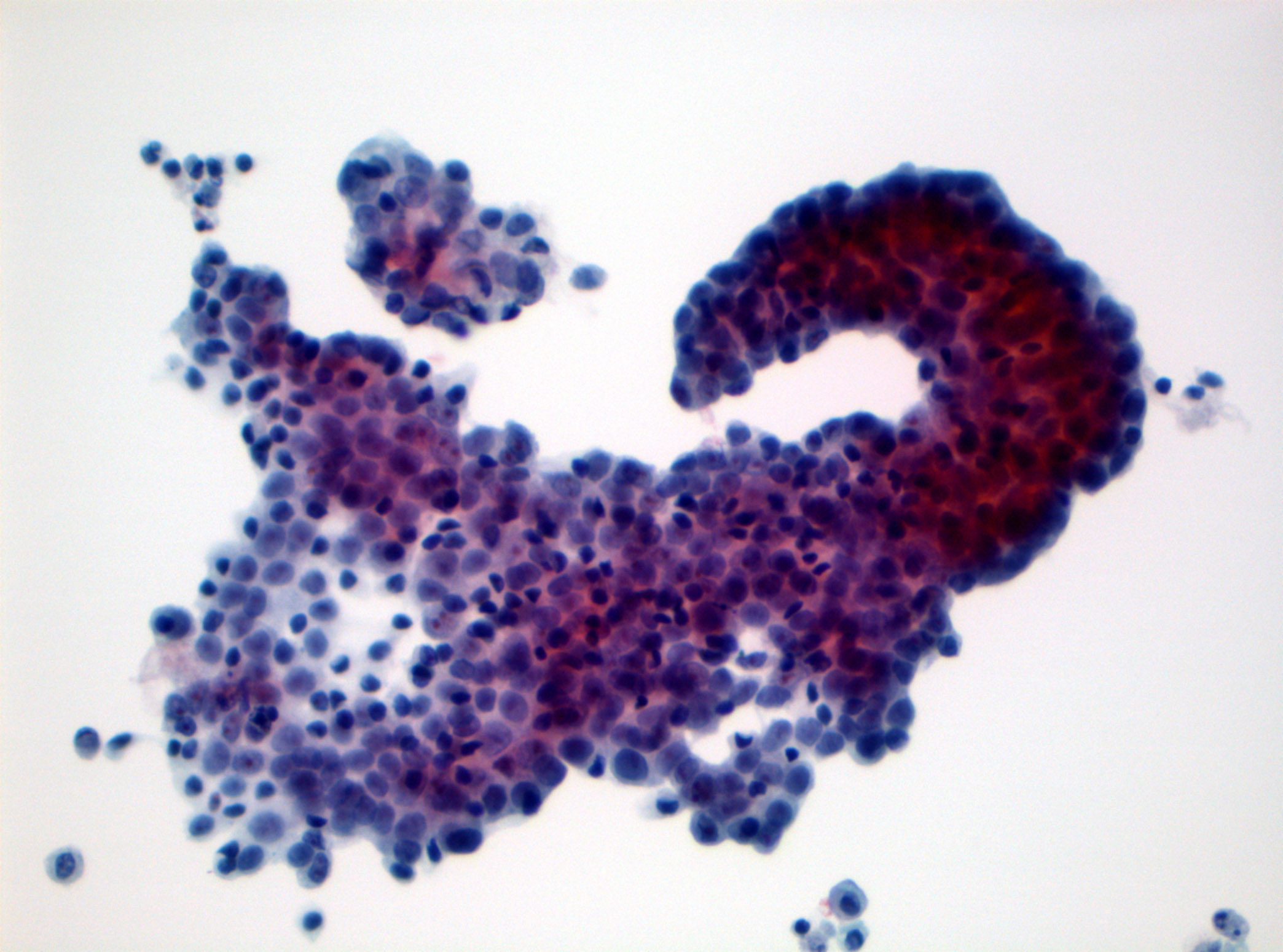
Cytology of
non high grade lesion
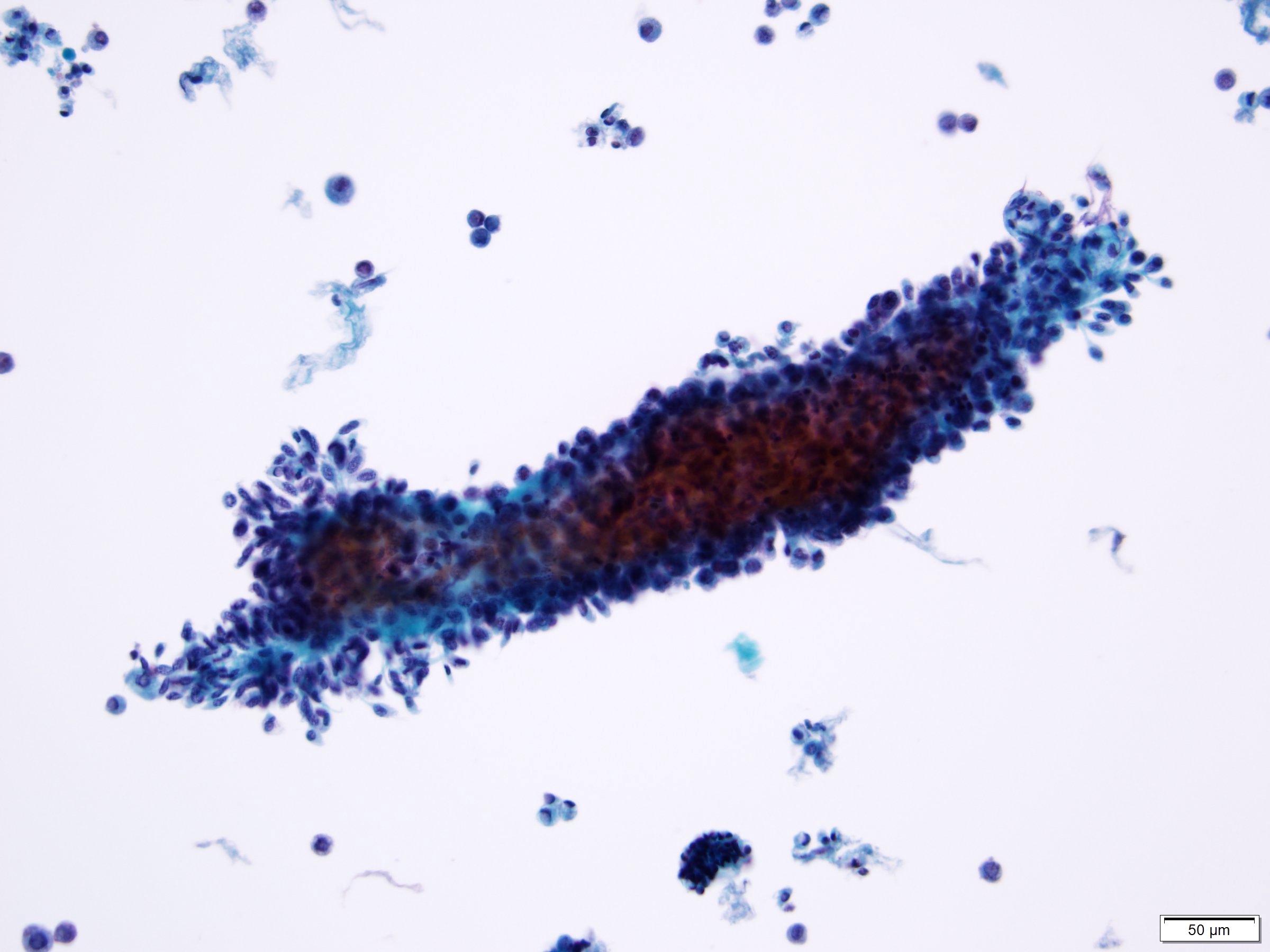
Low grade urothelial neoplasia
Positive stains
- GATA3: 97.5% in papillary lesions (SpringerLink: GATA-3 Expression in all Grades and Different Variants of Primary and Metastatic Urothelial Carcinoma [Accessed 5 April 2021])
- p63: 100% in noninvasive papillary carcinoma (Am J Surg Pathol 2014;38:e20)
- High molecular weight cytokeratin (Cancer 2003;97:1876)
- CK5/6: basal layer (Adv Urol 2020;2020:4920236)
- CK7 (Bratisl Lek Listy 2013;114:431)
Negative stains
- STAG2 in upper tract urothelial cancer (Ann Surg Oncol 2017;24:4059)
- Mismatch repair (MMR) protein (MLH1, MSH2, PMS2, MSH6) is lost in mismatch repair deficient tumors (Lynch syndrome)
Electron microscopy description
- Subset with urothelial eddies show microvillous projections and increased intercellular space (Int J Clin Exp Pathol 2013;6:1458)
- Low grade papillary urothelial carcinoma has zonula occludens (tight junctions) and well developed macula adherens (desmosomes), with fewer surface vesicles than normal epithelium
Molecular / cytogenetics description
- Activating mutations in FGFR3
- Somatic mutations in TERT promoter in 50% of low grade papillary noninvasive urothelial carcinomas; more commonly associated with FGFR3 mutated tumors (Histopathology 2018;72:795)
- Inactivating mutations in cohesion complex gene STAG2 in 32 - 36% noninvasive urothelial carcinomas; associated with low histologic grade and low tumor stage (Ann Surg Oncol 2017;24:4059)
- PIK3CA (25% cases) TSC1, HRAS, APC
- Epigenetic silencing of tumor suppressor genes through promoter hypermethylation: RUNX3, CDKN2A, MLH1, MGMT, VHL, DAPK, TBX2, TBX3, GATA2, ZIC4, GSTP1, CDH1 (Eur Urol 2012;61:1245, Nat Rev Urol 2013;10:327)
- MicroRNA alterations (J Pak Med Assoc 2018;68:759)
- Loss of chromosome 9 (9q and 9p in low grade)
Videos
Urothelial carcinoma, papillary and invasive
Sample pathology report
- Bladder, lesion, transurethral resection:
- Noninvasive papillary urothelial carcinoma, low grade
- Muscularis propria is present
Differential diagnosis
- Papillary urothelial neoplasm of low malignant potential (PUNLMP):
- Similar appearance at low and intermediate power
- No architectural or cytologic abnormalities (lacks variation in nuclear size / shape and polarity is maintained)
- Noninvasive papillary urothelial carcinoma, high grade:
- High grade features present, although may be focal
- Nucleomegaly, nuclear pleomorphism, irregular nuclear contours and clumped chromatin
- Mitoses readily identifiable
- Polypoid cystitis:
- Edematous or fibrotic papillary cores
- Broad base papillary excrescences
- Reactive epithelial changes may be present
- Urothelial papilloma:
- Papillary lesions with normal nondysplastic urothelium
- No cytologic atypia
- Inverted papilloma:
- Endophytic growth pattern of urothelium into lamina propria
- Degenerative atypia may be present
Additional references
Board review style question #1
A transurethral resection of bladder was performed on a 62 year old man. Histological examination showed a noninvasive papillary lesion. Which of the following is true about the lesion depicted above?
- Immunohistochemistry is helpful for diagnosis
- Mitoses are rare and usually confined to lower half of urothelium
- Nuclear pleomorphism is marked
- Progression to invasive disease is common
Board review style answer #1
B. Mitoses are rare and usually confined to lower half of urothelium. Diagnosis: low grade noninvasive papillary urothelial carcinoma.
Comment Here
Reference: Noninvasive papillary urothelial carcinoma low grade
Comment Here
Reference: Noninvasive papillary urothelial carcinoma low grade
Board review style question #2
Which of the following is the correct diagnosis?
- High grade noninvasive papillary urothelial carcinoma
- Invasive papillary urothelial carcinoma
- Inverted papilloma
- Low grade noninvasive papillary urothelial carcinoma
- Urothelial papilloma
Board review style answer #2
D. Low grade noninvasive papillary urothelial carcinoma
Comment Here
Reference: Noninvasive papillary urothelial carcinoma low grade
Comment Here
Reference: Noninvasive papillary urothelial carcinoma low grade

