
Appendix
Benign tumors
Tubular adenoma
Editorial Board Member: Maryam Kherad Pezhouh, M.D., M.Sc.
Deputy Editor-in-Chief: Aaron R. Huber, D.O.


Last author update: 10 May 2023
Last staff update: 10 May 2023
Copyright: 2022-2025, PathologyOutlines.com, Inc.
PubMed Search: Tubular adenoma


Table of Contents
Definition / general | Essential features | ICD coding | Epidemiology | Sites | Pathophysiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1Cite this page: Mallikarjunappa SS, Gonzalez RS. Tubular adenoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/appendixtubularadenoma.html. Accessed April 3rd, 2025.
Definition / general
- Polypoid dysplastic lesion in the appendix, analogous to conventional adenomas in the colorectum
Essential features
- Uncommon (not included in WHO classification of tumors of the appendix)
- Tubulovillous adenomas are often resected as mass lesions, while small tubular adenomas may be encountered incidentally in colectomy specimens from patients with polyposis syndromes
- Many adenocarcinomas of the appendix arise from adenomas
ICD coding
- ICD-10: D12.1 - benign neoplasm of appendix
Epidemiology
- Uncommon; identified in 0.02 - 0.06% of appendectomy specimens (Jpn J Clin Oncol 2003;33:413, Int J Surg Case Rep 2019;61:60)
Sites
- Appendix
Pathophysiology
- Understudied but likely to have the same pathophysiology as colorectal tubular adenoma
Clinical features
- Often asymptomatic but may cause appendicitis (Gastroenterol Clin Biol 2010;34:633, Hong Kong Med J 2010;16:12)
- Other clinical manifestations include intussusception and bowel obstruction (Jpn J Clin Oncol 2003;33:413, BMC Gastroenterol 2011;11:35)
- Appendiceal adenocarcinoma can arise in appendiceal adenomas (Jpn J Clin Oncol 2003;33:413)
- May be sporadic or arise in the setting of syndromes such as familial adenomatous polyposis (J Med Genet 2000;37:71)
Diagnosis
- Can be encountered on colonoscopy, abdominal CT or barium enema (Int J Surg Case Rep 2021;83:105949)
- May be found incidentally in appendectomy specimens (Hong Kong Med J 2010;16:12)
Radiology description
- Abdominal CT scan: appendix invaginating into the cecal cavity or thickening of the wall of the appendix (Jpn J Clin Oncol 2003;33:413, Int J Surg Case Rep 2021;83:105949)
Radiology images
Images hosted on other servers:

Double contrast barium enema

Abdominal CT scan
Prognostic factors
- Appendiceal adenocarcinoma can arise from adenomas
- Risk of progression likely increases with size and high grade dysplasia (as in the colon) but data are limited
Case reports
- 19 year old woman with tubulovillous adenoma of the appendix (Gastroenterol Clin Biol 2010;34:633)
- 49 year old man with complete appendiceal intussusception induced by primary appendiceal adenocarcinoma in tubular adenoma (Jpn J Clin Oncol 2003;33:413)
- 55 year old man with tubular adenoma of the appendix (J Clin Gastroenterol 1997;25:486)
- 69 year old man with tubulovillous adenoma of the appendix (Int J Surg Case Rep 2019;61:60)
- 78 year old woman with perforated acute appendicitis resulting from appendiceal villous adenoma presenting with small bowel obstruction (BMC Gastroenterol 2011;11:35)
Treatment
- Established guidelines do not exist, only recommendations
- Appendectomy alone is generally considered adequate for most benign appendiceal lesions, including adenoma (Rev Esp Enferm Dig 2002;94:537)
- Right hemicolectomy may be necessary for adenomas > 2 cm or with known malignant progression (Int J Surg Case Rep 2019;61:60)
- Endoscopic mucosal resection is not recommended (Gastroenterol Clin Biol 2010;34:633)
Gross description
- Similar to colorectal tubular adenomas, which can appear pedunculated, sessile, flat or depressed
- May be seen arising from the appendix
- Features of acute appendicitis and perforation can be seen if the adenoma presents accordingly (BMC Gastroenterol 2011;11:35)
Gross images
Images hosted on other servers:

Grossly visible appendiceal adenoma
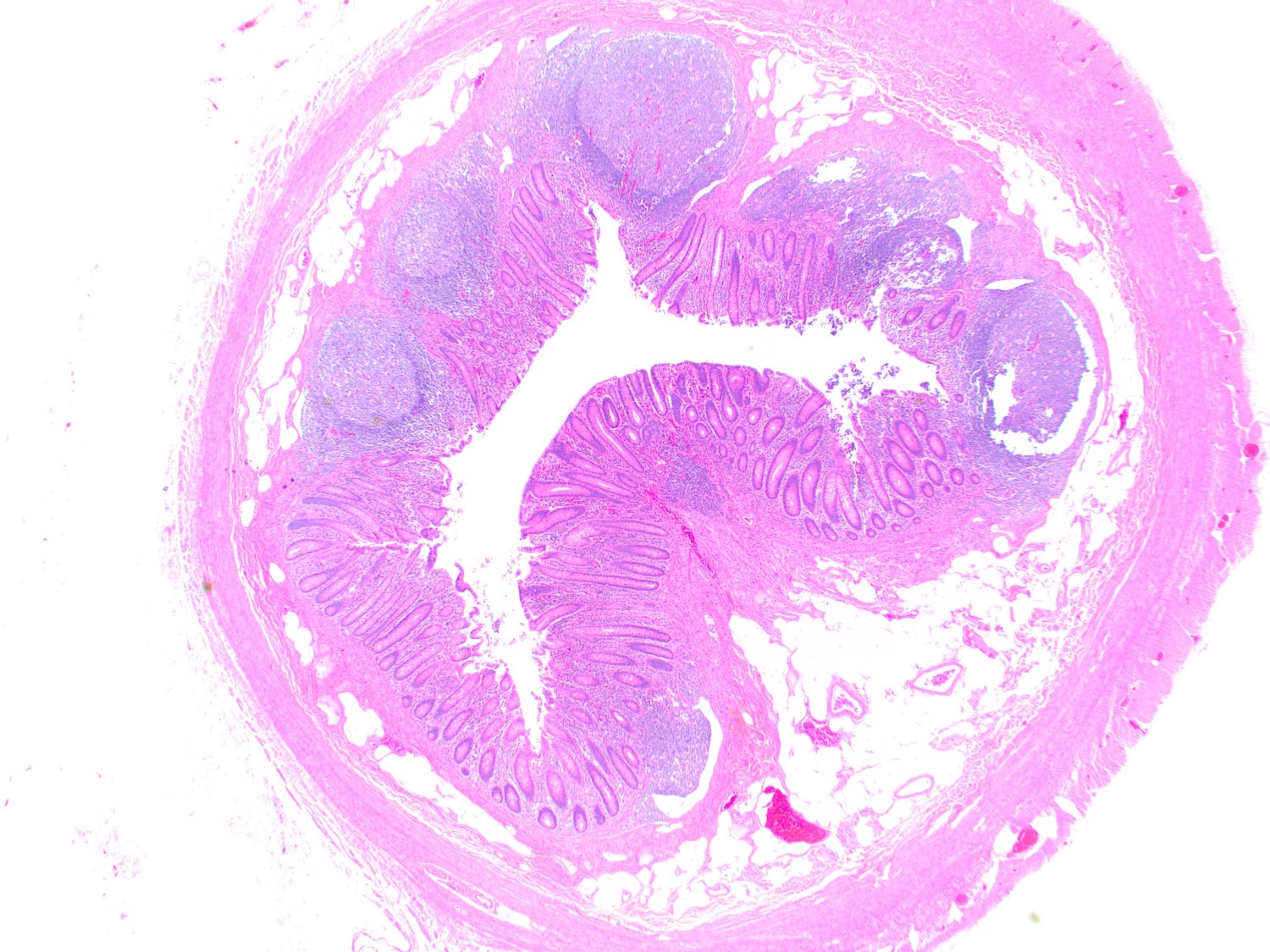
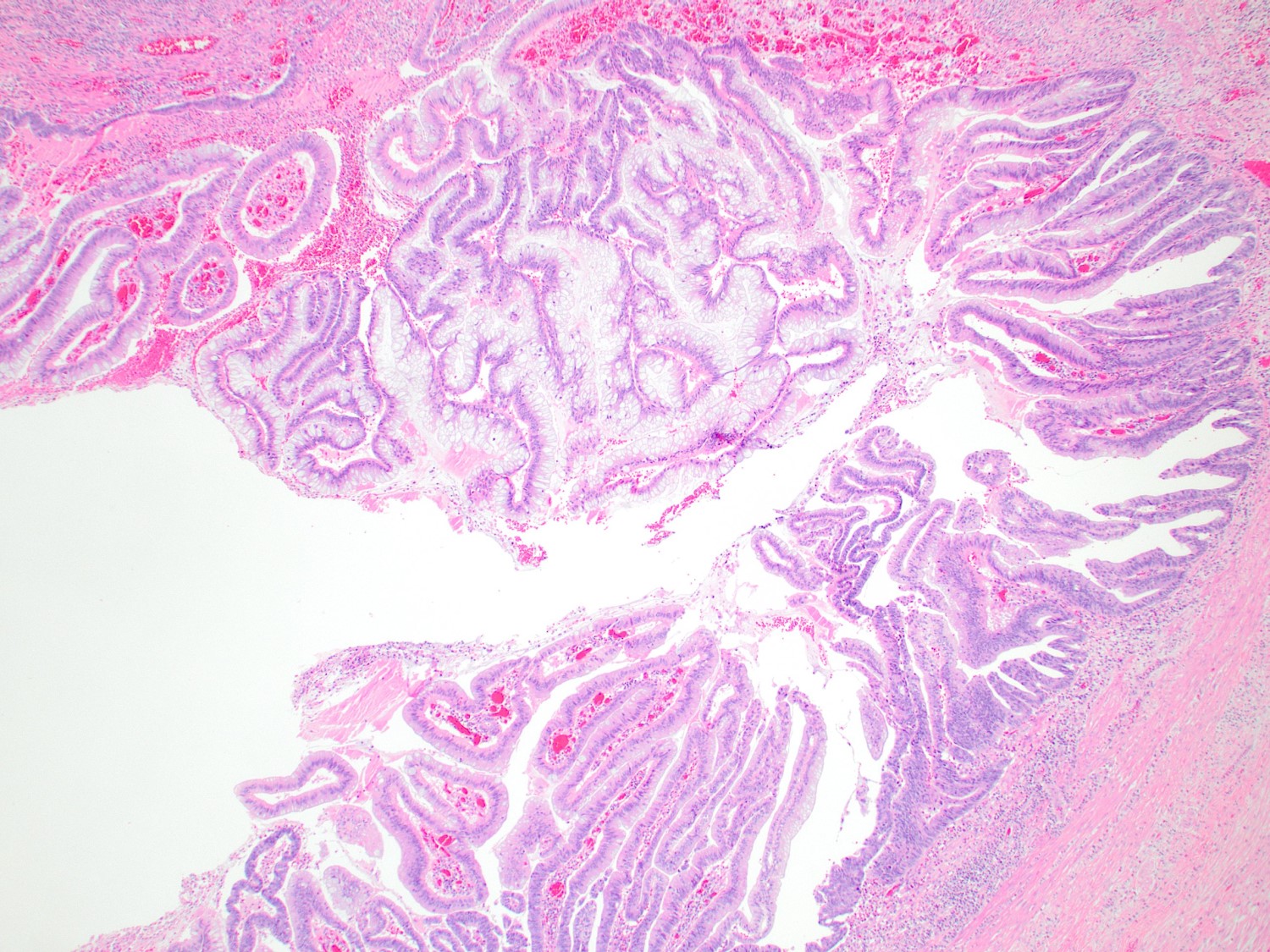
Microscopic (histologic) description
- Largely similar to colorectal tubular adenomas
- Architecture is most often villous but may also be tubular
- Predominantly composed of low grade dysplasia, with elongated, hyperchromatic nuclei and crowded glands
- Foci of high grade dysplasia may show rounded cells with nucleoli, low polarity and cribriform architecture
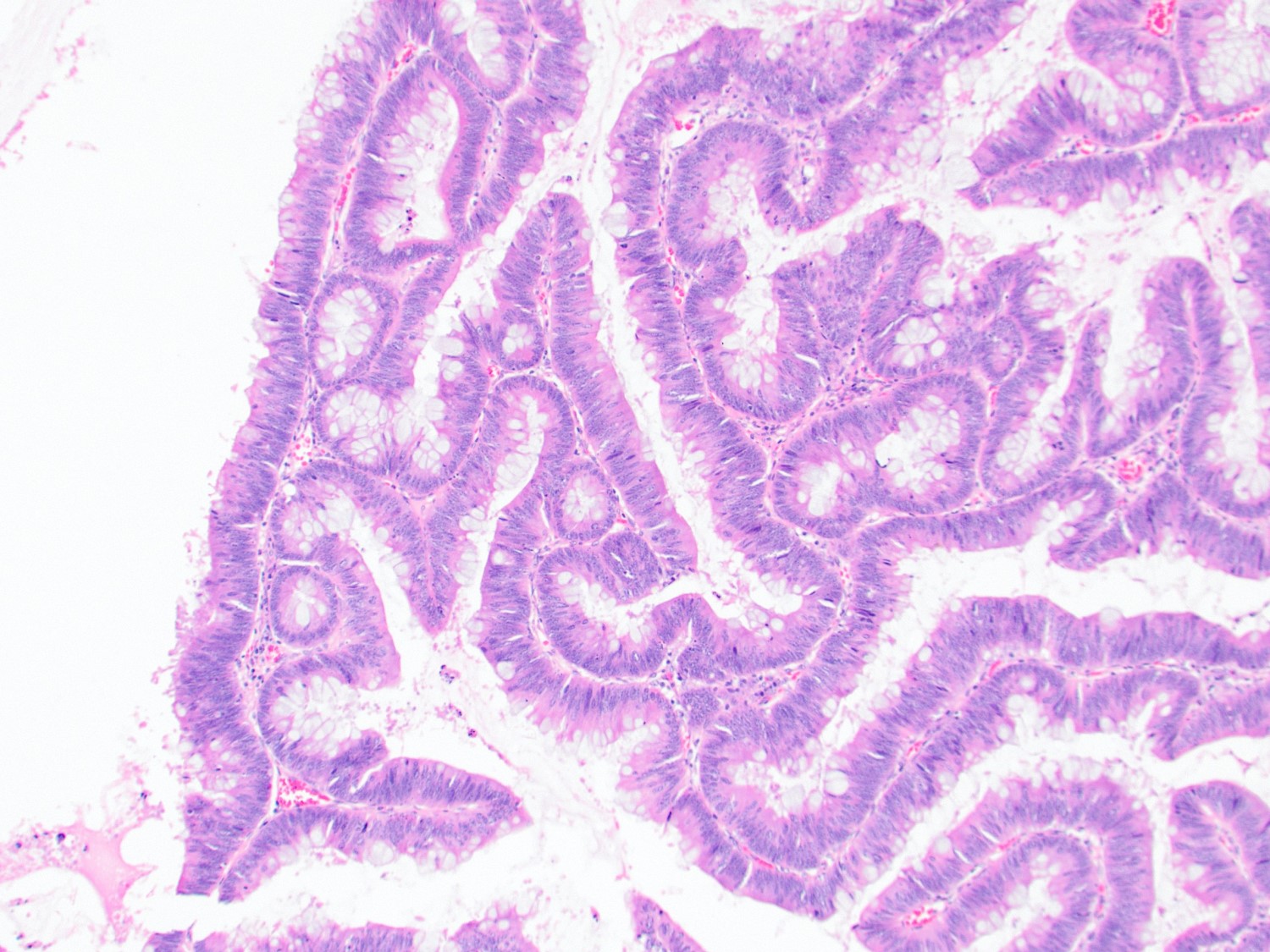
- Epithelial lining may have a somewhat hypermucinous appearance
- Reference: Scand J Gastroenterol 1985;20:512
Microscopic (histologic) images
Contributed by Raul S. Gonzalez, M.D.
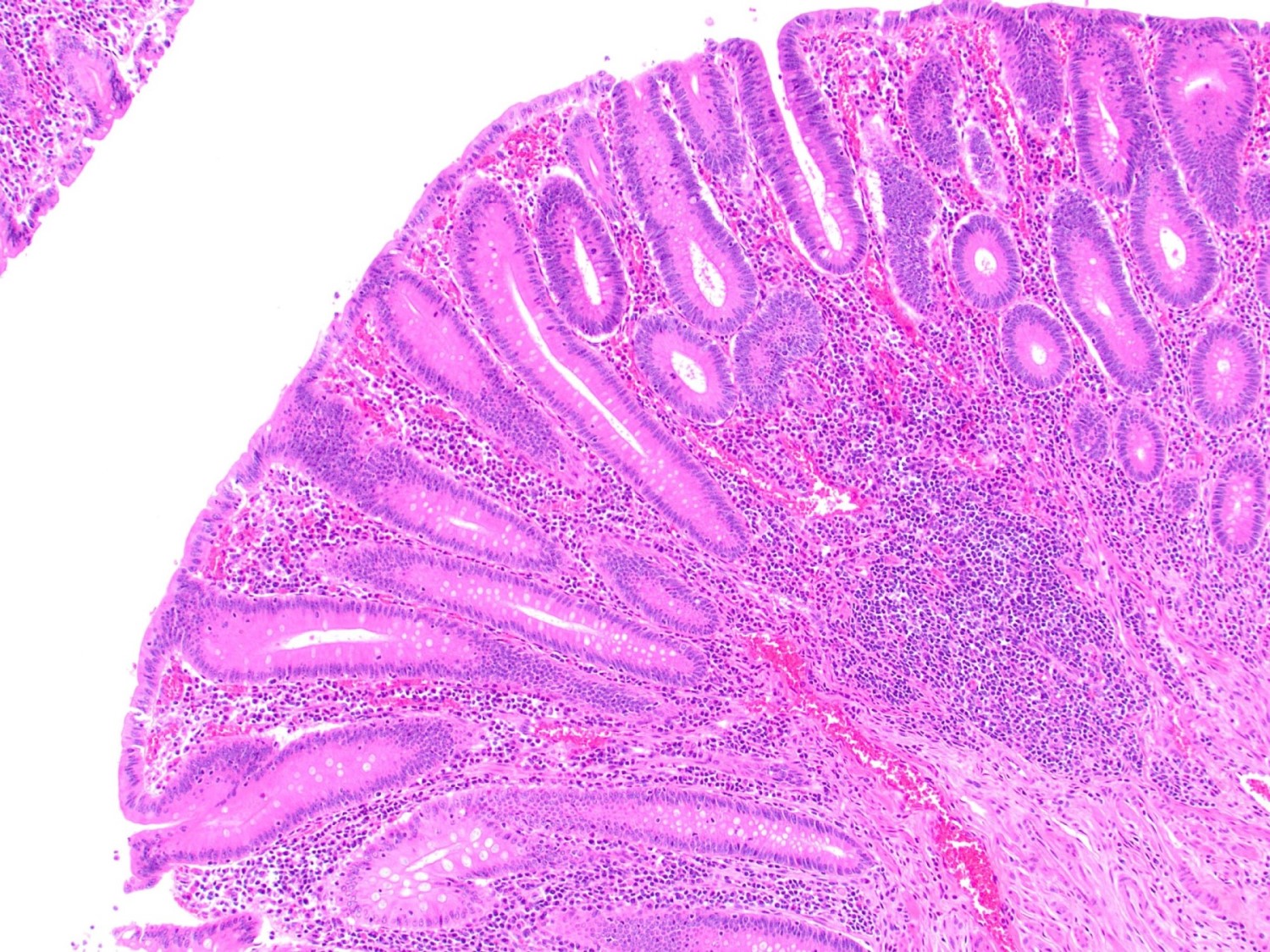
Tubular glands with elongated, hyperchromatic nuclei and crowded glands
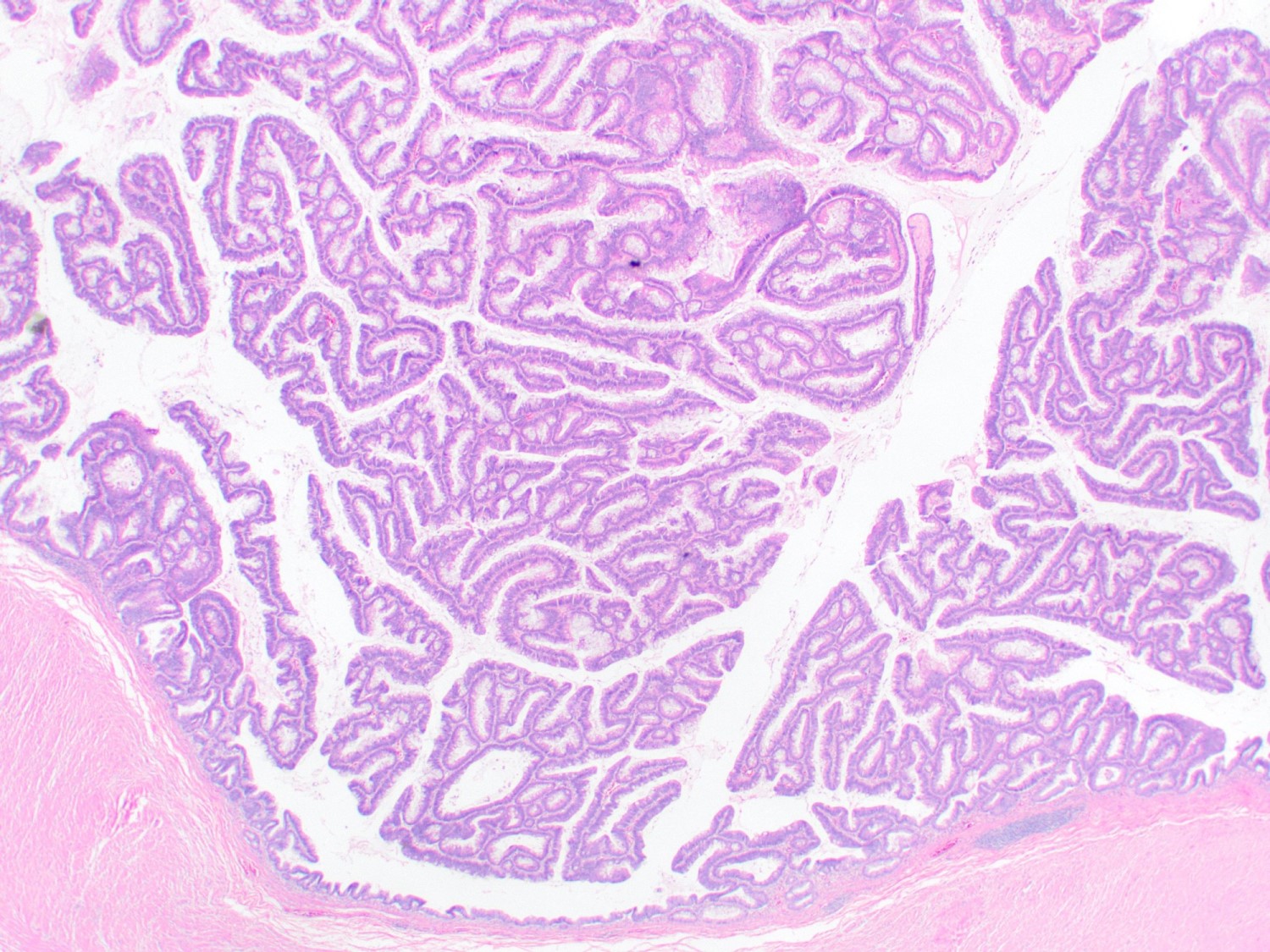
Crowded tubular and villous glands with elongated hyperchromatic nuclei
Mucinous appearance
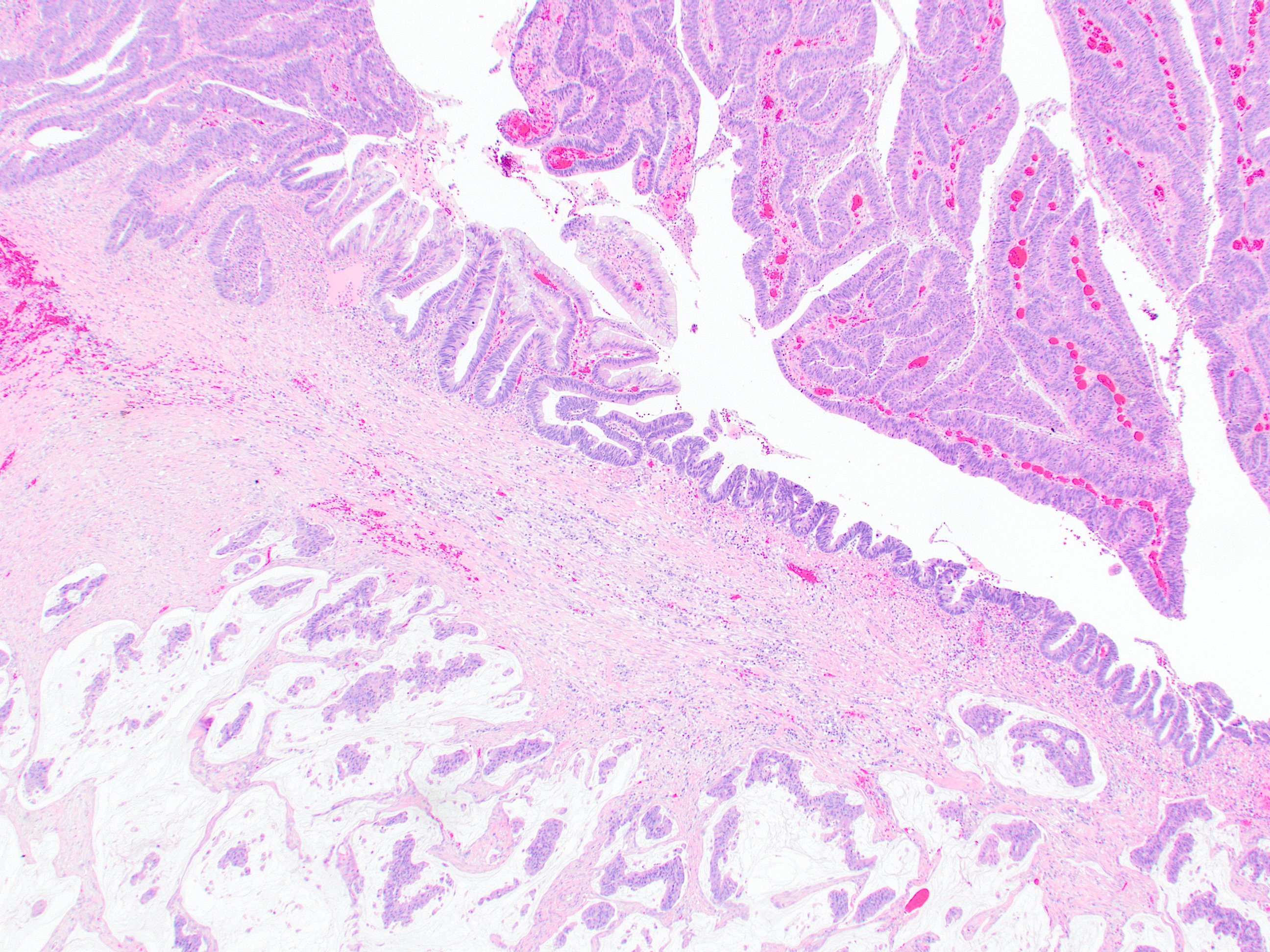
Adenocarcinoma arising in adenoma
Sample pathology report
- Appendix, appendectomy:
- Tubulovillous adenoma (2.1 cm)
- Negative for high grade dysplasia or malignancy
- Margin of resection negative
Differential diagnosis
- Serrated polyp:
- Can show areas of nuclear dysplasia but should also show additional areas of serrated glands with booting architecture and lacking conventional dysplasia
- Appendiceal mucinous neoplasm:
- May have villous areas and cytologic atypia but causes appendiceal dilation without polyp formation grossly
Board review style question #1
Which of the following is true about intestinal type adenomas of the appendix?
- They arise from low grade appendiceal mucinous neoplasms
- They can cause intussusception
- They have no risk of malignant progression
- They only occur in patients with familial adenomatous polyposis
Board review style answer #1
B. They can cause intussusception. Intestinal type adenomas of the appendix can cause appendicitis, bowel obstruction or perforation. They have no precursor lesion and may themselves progress to adenocarcinoma. They can occur sporadically or in patients with polyposis syndromes.
Comment Here
Reference: Tubular adenoma
Comment Here
Reference: Tubular adenoma
