

Appendix
Other nonneoplastic
Lymphoid hyperplasia
Editorial Board Member: Maryam Kherad Pezhouh, M.D., M.Sc.
Deputy Editor-in-Chief: Aaron R. Huber, D.O.


Last author update: 9 July 2024
Last staff update: 9 July 2024
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: Lymphoid hyperplasia

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Radiology description | Radiology images | Case reports | Treatment | Clinical images | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Azimpouran M, Hutchings D. Lymphoid hyperplasia. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/appendixlymphoidhyperplasia.html. Accessed December 25th, 2024.
Definition / general
- Benign, reversible cellular reaction of the appendix in response to inflammatory conditions, such as viral or bacterial gastroenteritis, giardiasis, mesenteric adenitis or immune disordered state (Ann Surg Treat Res 2022;103:306, Aliment Pharmacol Ther 2012;35:1000)
Essential features
- Benign reactive hyperplasia of lymphoid tissue of the lamina propria
- Clinically may mimic acute appendicitis, leading to appendectomy
Terminology
- Reactive lymphoid hyperplasia (RLH)
- Lymphoid follicular hyperplasia (LFH)
ICD coding
- ICD-10: K38.0 - hyperplasia, hyperplastic, appendix (lymphoid)
Epidemiology
- Most common in the pediatric population but can also occur in adults (Ann Surg Treat Res 2022;103:306)
Sites
- Appendix
Pathophysiology
- Appendix is categorized as a lymphoid organ owing to its significant concentration of lymphoid tissue
- Appendiceal lymphoid tissue is abundant in childhood and diminishes with age
- Lymphoid hyperplasia is frequently observed in cases of viral induced mesenteric adenitis / enteritis
- Upon exposure to an infectious agent, the appendix exhibits a response like other lymphoid tissues (Ulus Travma Acil Cerrahi Derg 2022;28:434)
Etiology
- Viral or bacterial gastroenteritis, giardiasis, mesenteric adenitis or immune disorders (Ann Surg Treat Res 2022;103:306, Aliment Pharmacol Ther 2012;35:1000)
- May be seen in association with adenovirus infection (Infect Dis Clin North Am 2010;24:995)
- May be associated with food hypersensitivity in pediatric patients (Aliment Pharmacol Ther 2012;35:1000)
Clinical features
- Clinical and imaging features may mimic acute appendicitis (Ann Surg Treat Res 2022;103:306)
Diagnosis
- Combination of clinical signs and symptoms with laboratory tests and radiological findings
Laboratory
- Compared to lymphoid hyperplasia, acute appendicitis is associated with higher white blood cell count (WBC), neutrophil count (N), mean platelet volume (MPV) and neutrophil to lymphocyte ratio (NLR), whereas lymphoid hyperplasia is associated with higher platelet distribution width (PDW) (Healthcare (Basel) 2020;8:39)
Radiology description
- Increased appendicular diameter
- Ultrasound
- Nonspecific thickening or enlargement of the hypoechoic lamina propria to a thickness of > 0.8 mm on ultrasound (Can Assoc Radiol J 2019;70:354)
- Reduction in the appendicular lumen (AJR Am J Roentgenol 2016;206:189)
- Noncompressible appendix with increased diameter (up to 6 - 8 mm) that could be misdiagnosed as appendicitis (AJR Am J Roentgenol 2016;206:189)
- Lack of features found in acute appendicitis, including periappendiceal fluid, periappendiceal hypoechoic fat and mural hyperemia on color Doppler (AJR Am J Roentgenol 2016;206:189)
- Computed tomography (CT) scan
- Central lucency and hyperintense thickened outer wall
- Lymphoid tissue may appear as fluid in the appendix
- Lacks periappendiceal fat stranding often found in acute appendicitis (Emerg Radiol 2015;22:643)
- May be associated with intussusception
Radiology images
Images hosted on other servers:

Noncompressible appendix with thickened lamina propria
Case reports
- 63 year old man with nodular lymphoid hyperplasia near appendiceal orifice (Am J Gastroenterol 2018;113:11)
- 69 year old man with polypoid reactive lymphoid hyperplasia near appendiceal orifice (Intern Med 2014;53:1049)
- 71 year old man with appendiceal intussusception associated with lymphoid hyperplasia (World J Gastroenterol 2007;13:4274)
Treatment
- Supportive medical treatment of any associated disease processes
- Appendectomy is unnecessary, though it may occur in cases misdiagnosed as acute appendicitis (Ann Surg Treat Res 2022;103:306)
Clinical images
Images hosted on other servers:

Intussuscepted appendix on colonoscopy
Gross description
- Appendix can appear normal or thick walled
- Cross sections may show narrowing of lumen
Gross images
Contributed by Mahzad Azimpouran, M.D. and Danielle Hutchings, M.D.

Dilated appendix

Grossly unremarkable appendix

Thickened mucosal layer
Microscopic (histologic) description
- Marked hypertrophy of lymphoid follicles within lamina propria
- Cluster of 10 or more lymphoid aggregates, containing lymphoid follicles ≥ 2 mm (AJR Am J Roentgenol 2016;206:189)
- Attenuation of submucosa and muscularis propria (AJR Am J Roentgenol 2016;206:189)
- Concomitant acute appendicitis is uncommon (AJR Am J Roentgenol 2016;206:189, Aust N Z J Surg 1981;51:169)
Microscopic (histologic) images
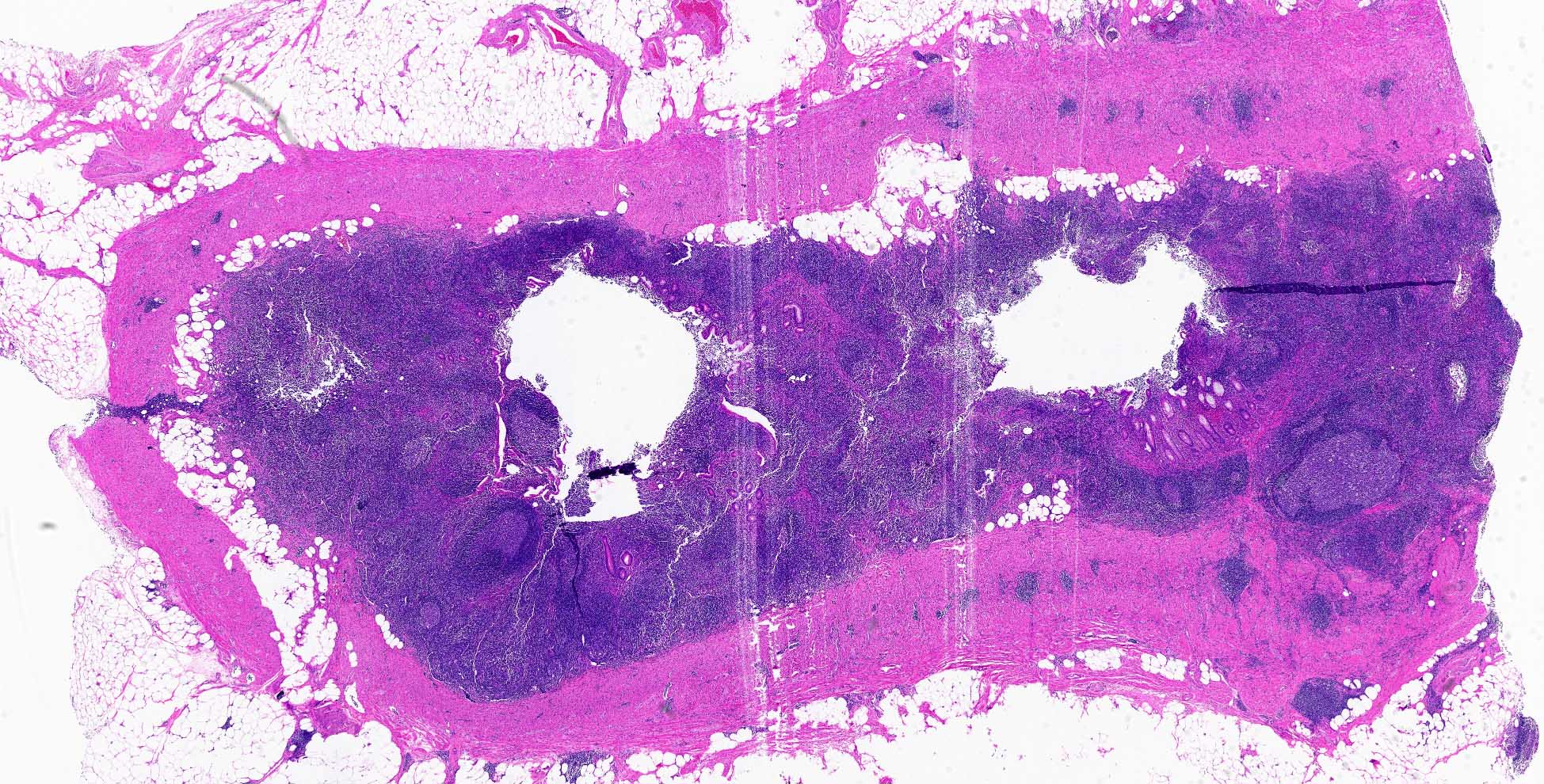
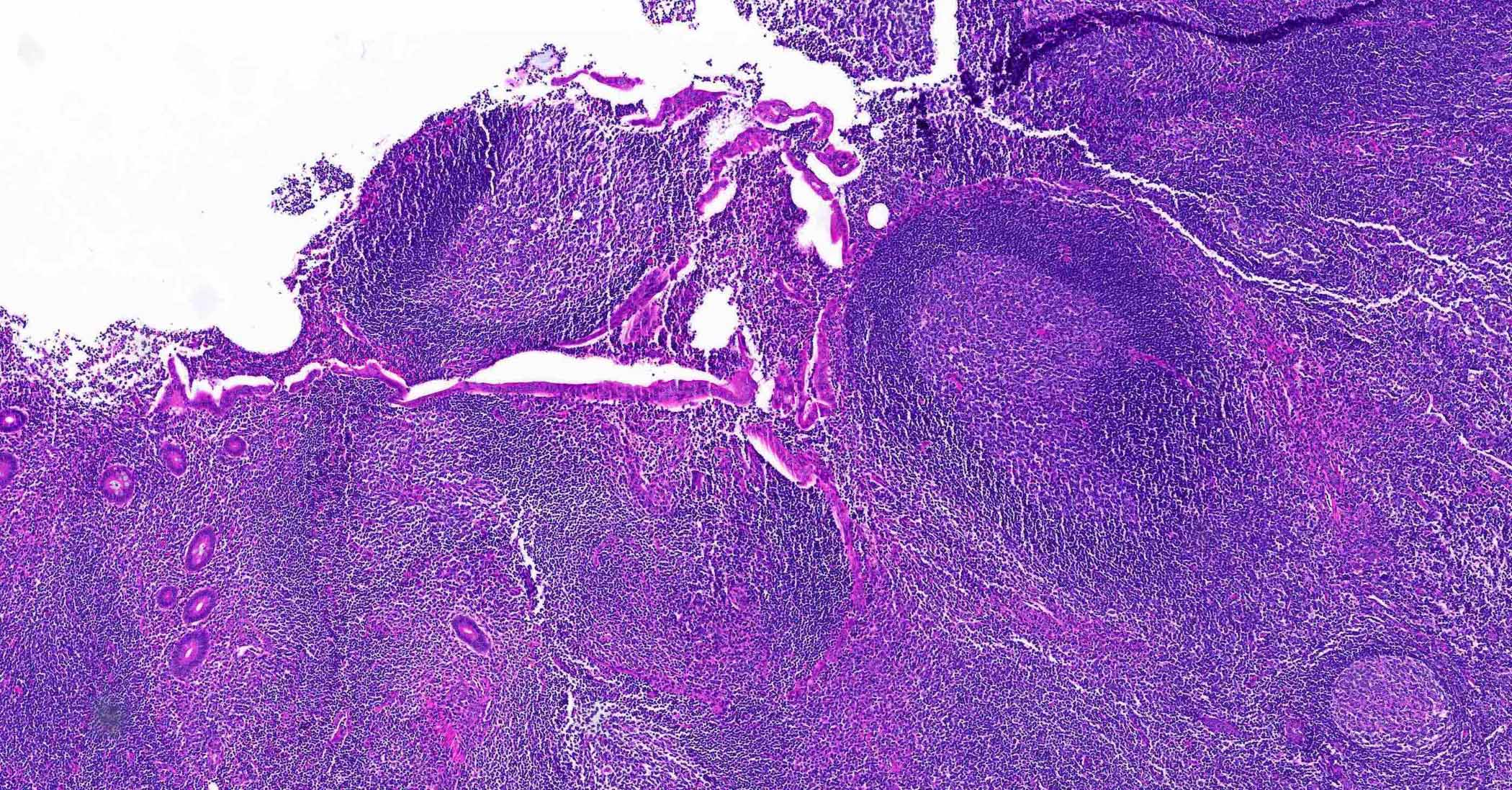
Contributed by Mahzad Azimpouran, M.D. and Danielle Hutchings, M.D.
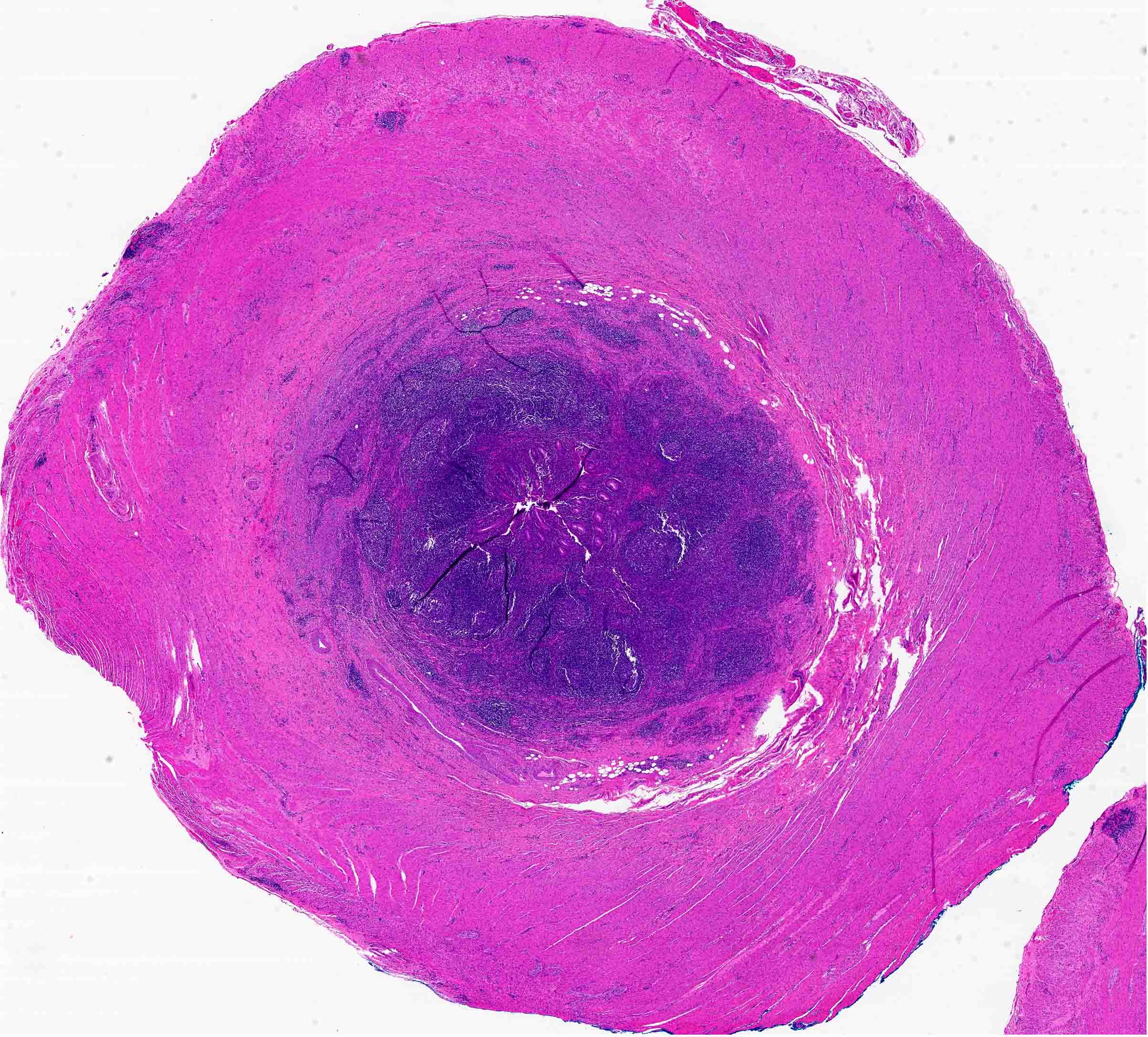
Cross section
Lymphoid hyperplasia of tip
Lymphoid aggregates expanding lamina propria
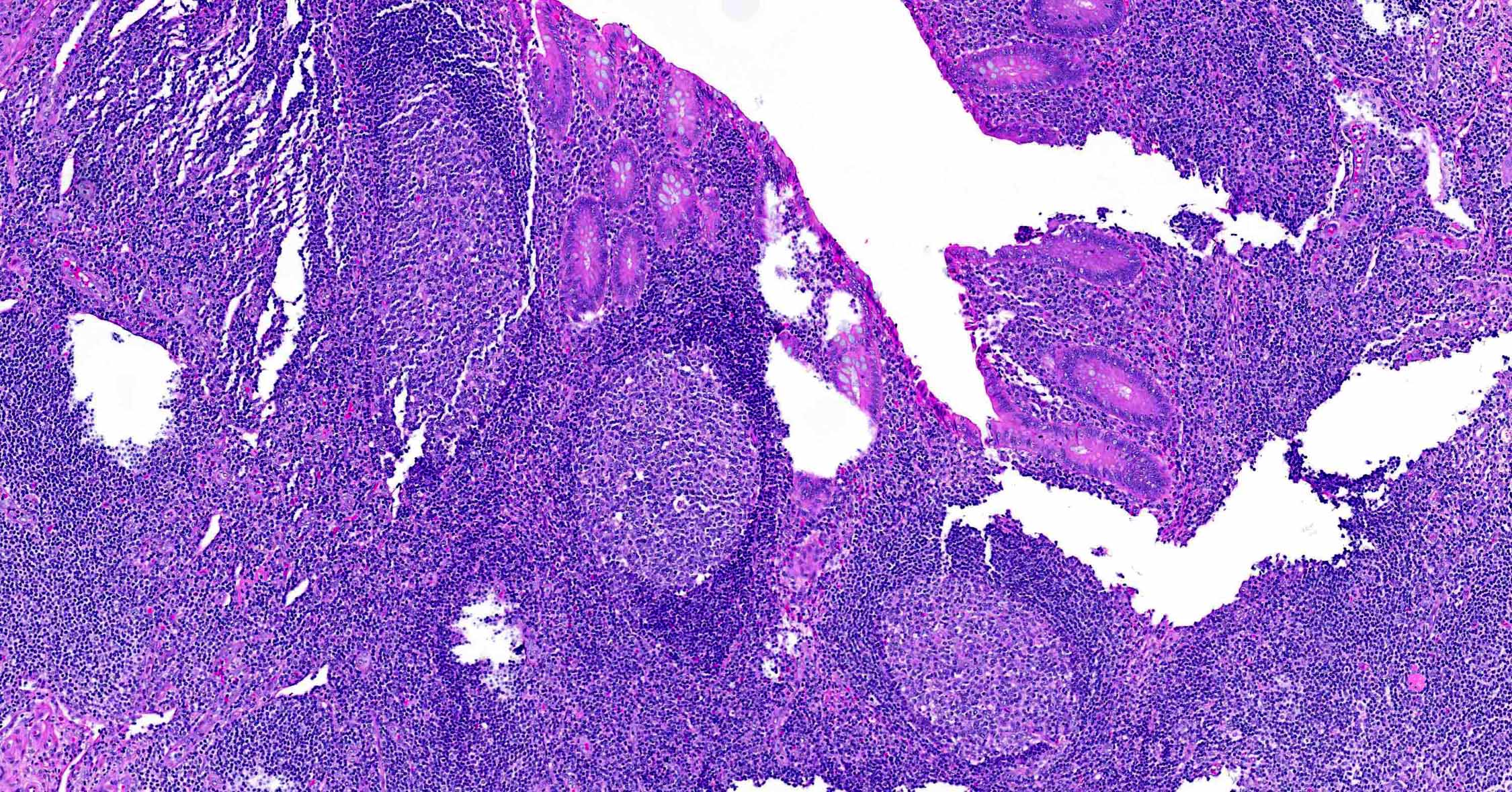
Prominent lymphoid follicles
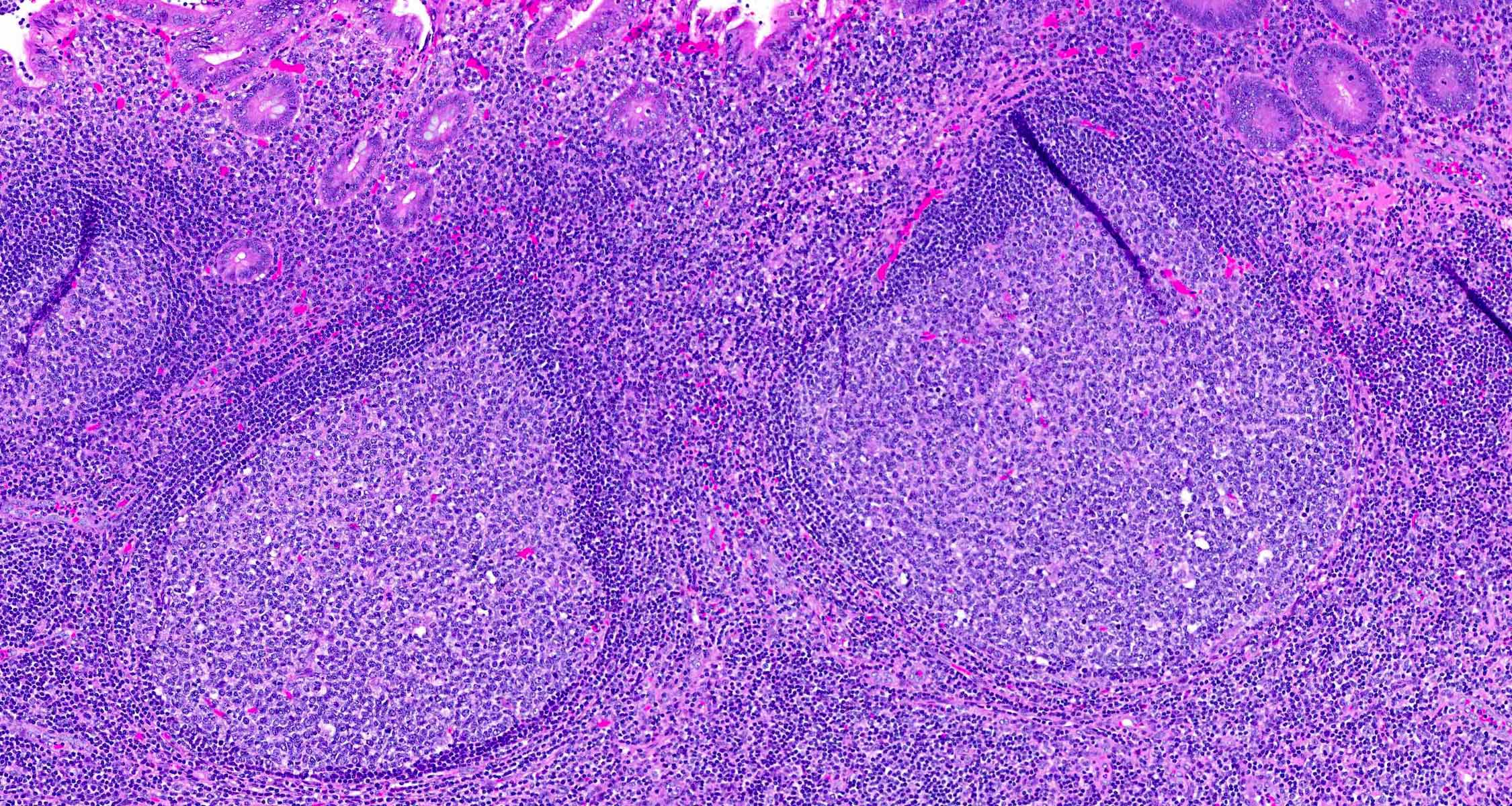
Reactive lymphoid follicles
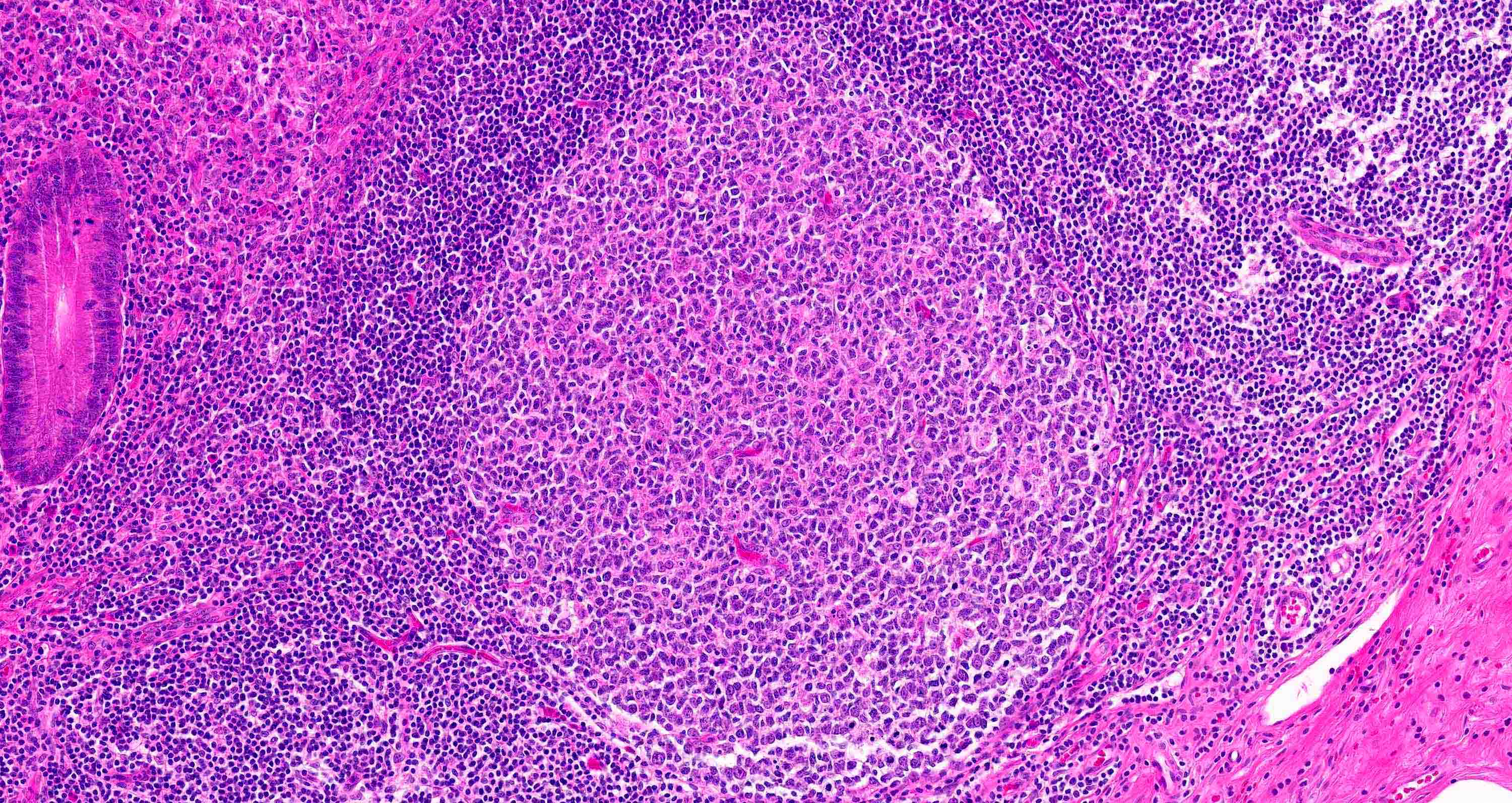
Reactive lymphoid hyperplasia
Sample pathology report
- Appendix, appendectomy:
- Appendix with prominent reactive lymphoid hyperplasia (see comment)
- Comment: No neoplasm identified.
Differential diagnosis
- Acute appendicitis:
- Acute neutrophilic inflammation, including in appendiceal wall
- Granulomatous appendicitis:
- Presence of granulomas
- Interval (delayed) appendectomy:
- Distinction relies mainly on clinical history
Additional references
Board review style question #1
An 11 year old boy undergoes appendectomy for dilated appearing appendix on imaging. What is the most likely diagnosis for the histologic appearance shown above?
- Acute appendicitis
- Granulomatous appendicitis
- Lymphoid hyperplasia
- Lymphoma
Board review style answer #1
C. Lymphoid hyperplasia. The image depicts marked hypertrophy of lymphoid follicles within the lamina propria, which is characteristic of lymphoid hyperplasia. Answer A is incorrect because neutrophilic inflammation is absent. Answer B is incorrect because granulomas are absent. Answer D is incorrect because the lymphoid infiltrate does not efface normal structures and is polymorphic without significant cytologic atypia.
Comment Here
Reference: Lymphoid hyperplasia
Comment Here
Reference: Lymphoid hyperplasia
Board review style question #2
Appendiceal lymphoid hyperplasia is characterized microscopically by which of the following features?
- Epithelioid granulomas
- Prominent lymphoid aggregates containing follicles expanding the lamina propria
- Transmural lymphoid aggregates
- Transmural neutrophilic inflammation
Board review style answer #2
B. Prominent lymphoid aggregates containing follicles expanding the lamina propria. Lymphoid hyperplasia is characterized by prominent lymphoid aggregates containing follicles (typically including clusters > 10) in the lamina propria layer. Answer C is incorrect because in lymphoid hyperplasia, prominent lymphoid aggregates are predominantly restricted to the lamina propria, whereas transmural lymphoid aggregates may be seen with interval (delayed) appendectomy or Crohn's disease. Answer D is incorrect because transmural neutrophilic inflammation is a feature of acute appendicitis, not lymphoid hyperplasia. Answer A is incorrect because epithelioid granulomas are not a feature of lymphoid hyperplasia.
Comment Here
Reference: Lymphoid hyperplasia
Comment Here
Reference: Lymphoid hyperplasia

