

Appendix
Appendicitis
Interval appendicitis
Authors: Pu Ni, M.D., Qingqing Liu, M.D., Ph.D.
Editorial Board Member: Maryam Kherad Pezhouh, M.D., M.Sc.
Deputy Editor-in-Chief: Aaron R. Huber, D.O.


Last author update: 31 May 2023
Last staff update: 14 November 2023
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: Interval appendicitis / interval appendectomy

Table of Contents
Definition / general | Essential features | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Ni P, Liu Q. Interval appendicitis. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/appendixinterval.html. Accessed December 22nd, 2024.
Definition / general
- Histopathologic findings observed in interval appendectomy specimens (Am J Surg Pathol 2003;27:1147)
Essential features
- Interval appendectomy is usually performed in patients with complicated appendicitis (i.e., rupture) who are clinically stable
- These patients are treated with initial antibiotic therapy or drainage followed by a delayed appendectomy (JAAPA 2018;31:35)
- Wide spectrum of histological findings ranges from normal to acute inflammation, granulomatous and xanthogranulomatous inflammation with giant cells, changes mimicking mucinous neoplasms, transmural chronic inflammation with lymphoid aggregates and mural fibrosis and thickening mimicking Crohn's disease (Histopathology 2022;80:965, Semin Diagn Pathol 2004;21:98, Am J Surg Pathol 2003;27:1147)
- Microscopic findings can assist diagnosis when there is a lack of clinical information
- Appendiceal neoplasm can be found in the resection specimen incidentally, more commonly in elderly (Am J Surg 2015;209:442, J Surg Oncol 2019;120:736)
ICD coding
- ICD-10: K36 - other appendicitis
Epidemiology
- Annual incidence of acute appendicitis is ~100 per 100,000 person years in developed countries and complicated appendicitis is seen in 27 - 29% patients (Arch Surg 2011;146:156, JAMA Surg 2020;155:330)
- About half of patients managed with initial nonsurgical methods (antibiotics and abscess drainage) will undergo interval appendectomy (Am J Surg 2015;209:442)
Sites
- Appendix
Pathophysiology
- Patients' defense mechanisms may clear, restrict or enclose the inflammation, resulting in resolution of inflammation or transition from acute to chronic inflammation and formation of an inflammatory mass (phlegmon or plastron) of a contained (circumscribed) abscess (World J Gastrointest Surg 2012;4:83)
Etiology
- Conservative treatment of complicated acute appendicitis
Clinical features
- Clinical symptoms caused by acute appendicitis (e.g., abdominal pain, fever, poor appetite, etc.) usually improve after initial nonsurgical management
- Nonspecific laboratory findings
- Radiological study (ultrasound or CT) before interval appendectomy can reveal and appendix that is normal, inflamed or with residual abscess (J Surg Res 2018;225:90)
- Interval appendectomy is often performed to exclude an appendiceal neoplasm (J Surg Oncol 2019;120:736, Am J Surg 2015;209:442)
Diagnosis
- Clinical history of delayed appendectomy in patients with complicated acute appendicitis
- When clinical history is unclear, diagnosis may be made based on characteristic histological findings
Laboratory
- Nonspecific laboratory findings include normal or variably elevated white blood cell count and C reactive protein and leukocyte shift to left
Radiology description
- Radiological findings after initial nonsurgical management include normal appendix to inflamed appendix, presence of residual abscess or resolution of the abscess (J Surg Res 2018;225:90, Ann Gastroenterol Surg 2019;3:561)
Radiology images
Images hosted on other servers:

Abscess resolved after treatment
Prognostic factors
- Conservative treatment is effective in a high percentage of patients with acute appendicitis, with success rates ranging from 68% to 95% and a relative low recurrence rate of ~10% (Ann Surg 2007;246:741, World J Surg 2010;34:199, Br J Surg 2009;96:473, J Surg Res 2018;225:90)
- Potential rrecurrences usually have a mild clinical course (World J Gastrointest Surg 2012;4:83)
- Surgical management is only reserved for patients with risk factors
- Further diagnostic evaluation may be required for patients > 40 years with anemia and a presumed appendiceal mass to exclude malignancy (Am J Surg 2015;209:442, J Surg Oncol 2019;120:736)
- The most common complications after interval appendectomy include surgical site infection, ileus and intra-abdominal abscess (Ann Palliat Med 2021;10:12546)
Case reports
- 19 year old man with complicated appendicitis (phelgmon) underwent interval appendectomy after failed initial nonoperative treatment (Int J Surg Case Rep 2018;50:75)
- 64 year old woman presented with perforated appendicitis was found to have adenocarcinoma of the appendix (Cureus 2021;13:e13578)
- 69 year old woman with perforated appendicitis underwent initial medical treatment followed by interval appendectomy 3 months later (Int J Surg Case Rep 2022;96:107319)
Treatment
- Routine interval appendectomy following successful conservative management of complicated acute appendicitis is usually not required (World J Gastrointest Surg 2012;4:83)
- Interval appendectomy should be considered in selected patients with risk factors, i.e.
- Patients with retained fecaliths, indicating a high probability of recurrence
- Patients with multiple (> 2 or 3) episodes of acute appendicitis after initial conservative treatment
- Patients > 40 years with anemia
- Patients with a presumed appendiceal mass to exclude malignancy (World J Gastrointest Surg 2012;4:83, J Surg Oncol 2019;120:736)
Clinical images
Images hosted on other servers:

Interval appendectomy
Gross description
- Appendix can be grossly normal or with nonspecific findings such as serosal adhesion or wall thickening
Gross images
Contributed by Pu Ni, M.D. and Qingqing Liu, M.D., Ph.D.

Mildly enlarged appendix
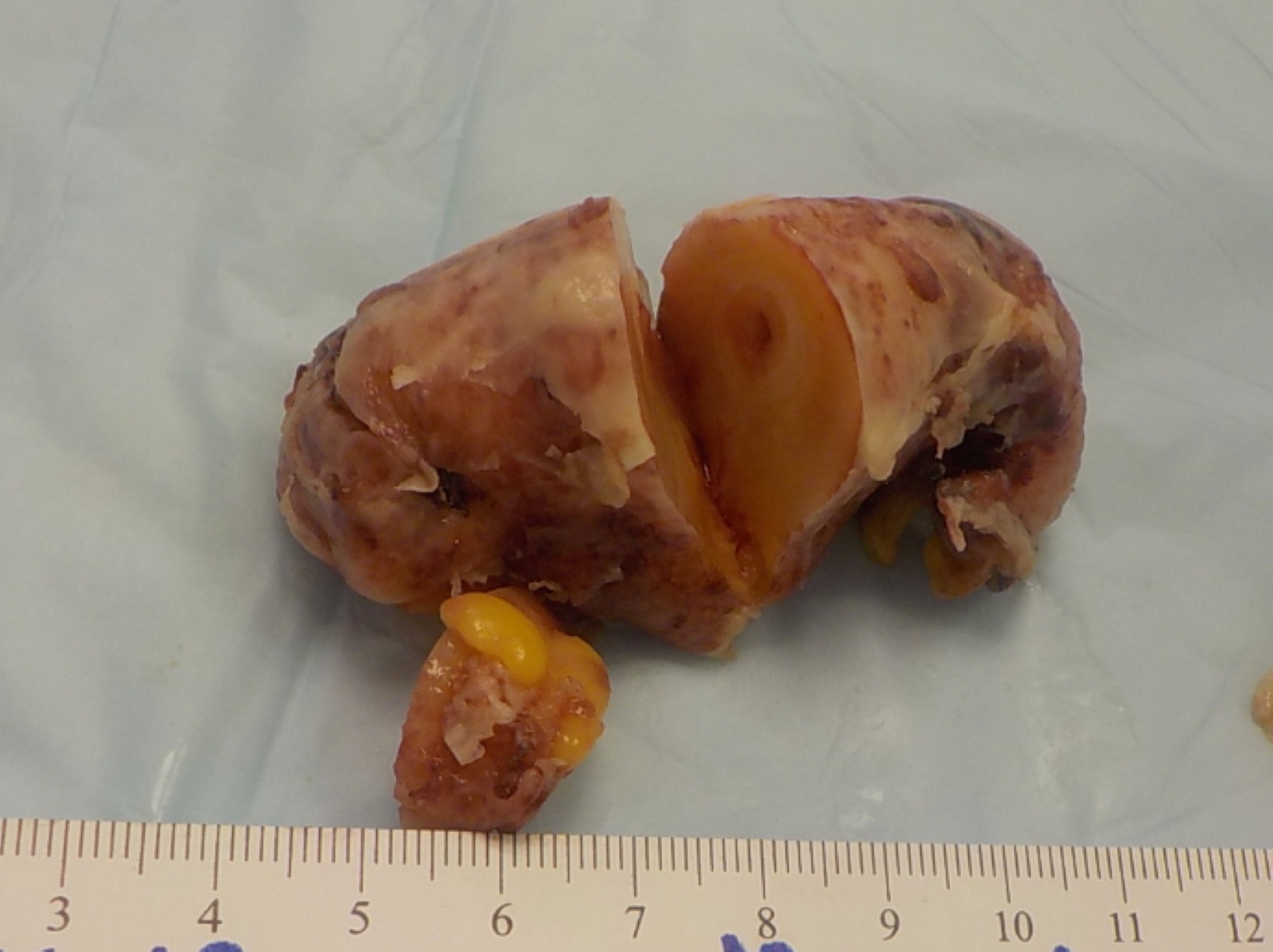
Significantly enlarged appendix
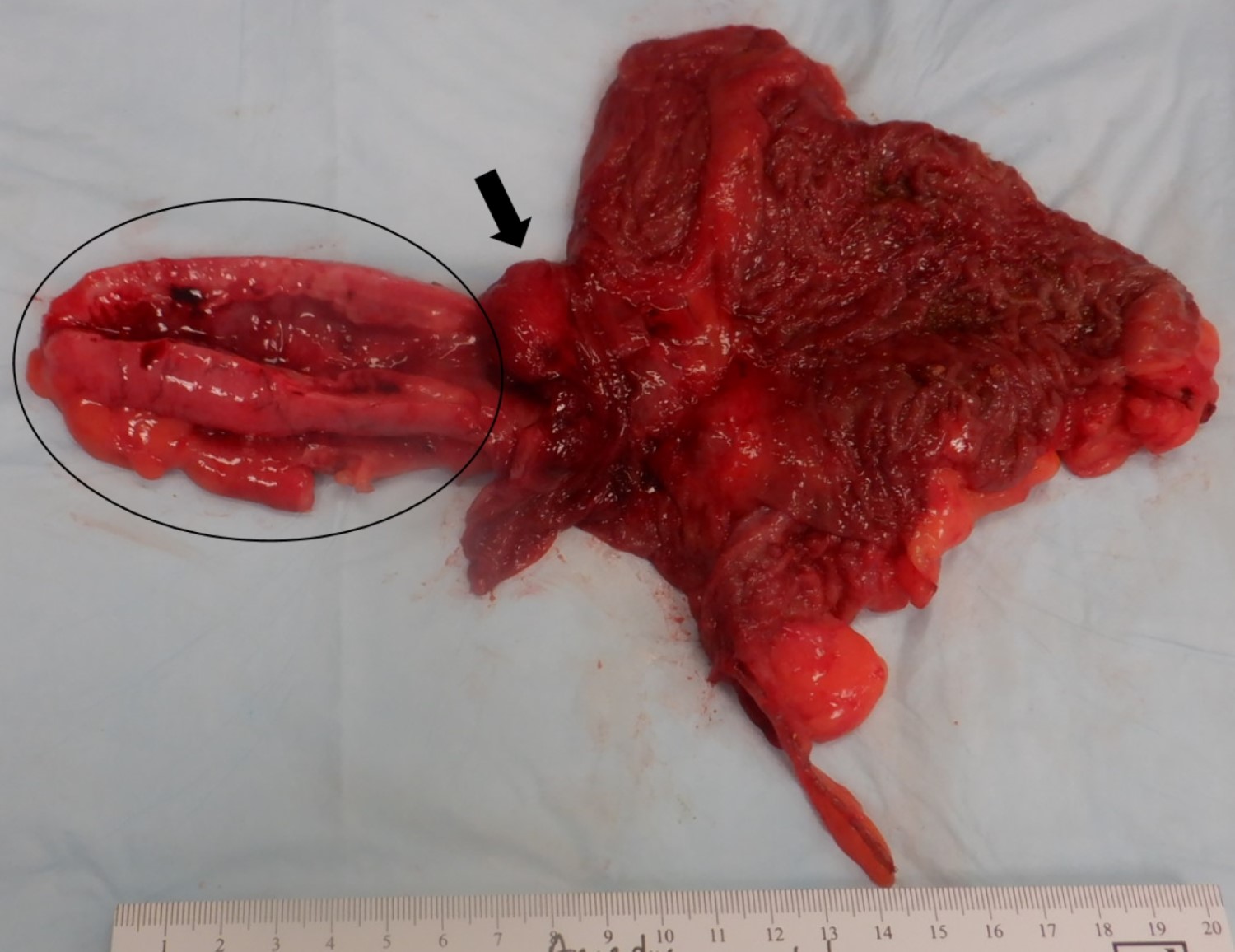
Inflammatory polyp mimicking neoplasm
Microscopic (histologic) description
- Residual acute inflammation may be present as focal cryptitis and crypt abscess (Am J Surg Pathol 2003;27:1147, Histopathology 2022;80:965)
- Chronic inflammation of the appendix (Am J Surg Pathol 2003;27:1147, Histopathology 2022;80:965)
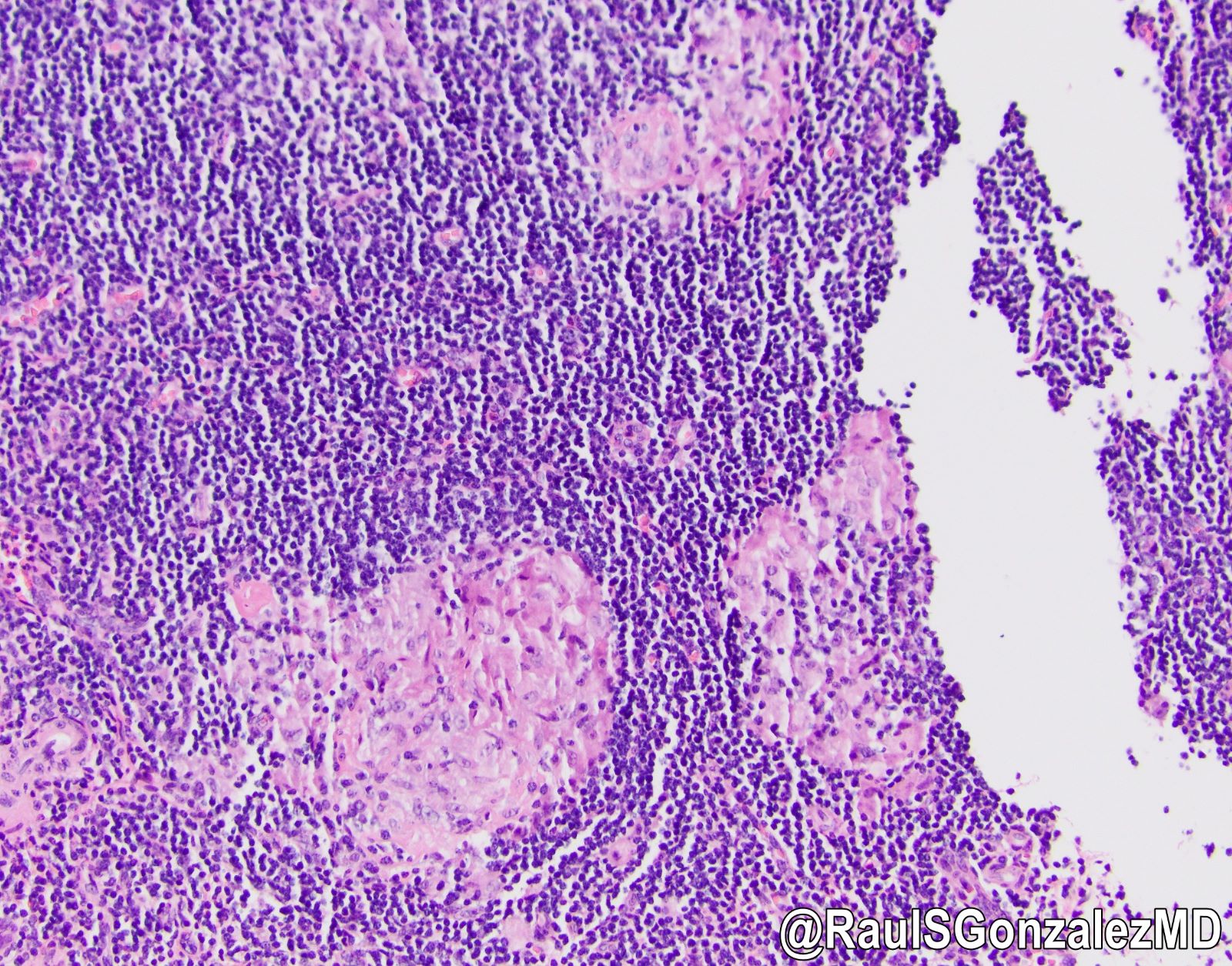
- Scattered granulomas composed of epithelioid histiocytes or loose histiocytic aggregates may be present in all layers of the appendiceal wall; special stains such as GMS, AFB and Gram stain can be used to rule out granuloma associated infections
- Xanthogranulomatous inflammation characterized by foamy macrophages admixed with lymphocytes, plasma cells and other inflammatory cells
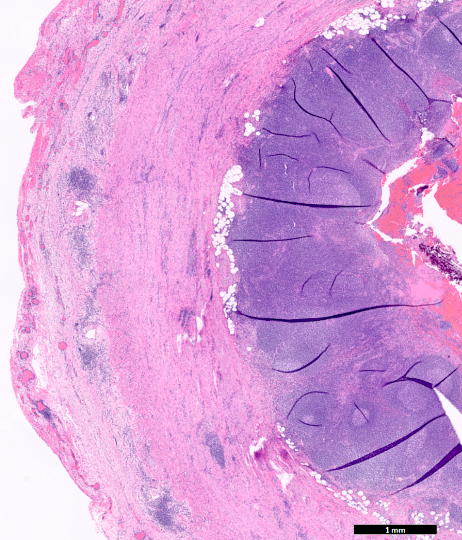
- Crohn's-like features: mucosal architecture distortion, lymphohistiocytic inflammation and transmural chronic inflammation with lymphoid aggregates (string of pearls) and mural fibrosis
- Hemosiderin laden macrophages
- Pulse granulomas may be occasionally seen (Case Rep Gastroenterol 2018;12:765, Arch Pathol Lab Med 2022 Sep 9 [Epub ahead of print])
- Changes mimicking mucinous neoplasms
- Intramural / periappendiceal / intraluminal mucin pool, postinflammatory reactive goblet cell hyperplasia and diverticula
- Appendix is needed to be submitted entirely for histological examination to rule out an appendiceal mucinous neoplasm (Histopathology 2022;80:965, Mod Pathol 2020;33:953)
Microscopic (histologic) images
Contributed by Pu Ni, M.D., Qingqing Liu, M.D., Ph.D. and @RaulSGonzalezMD on Twitter
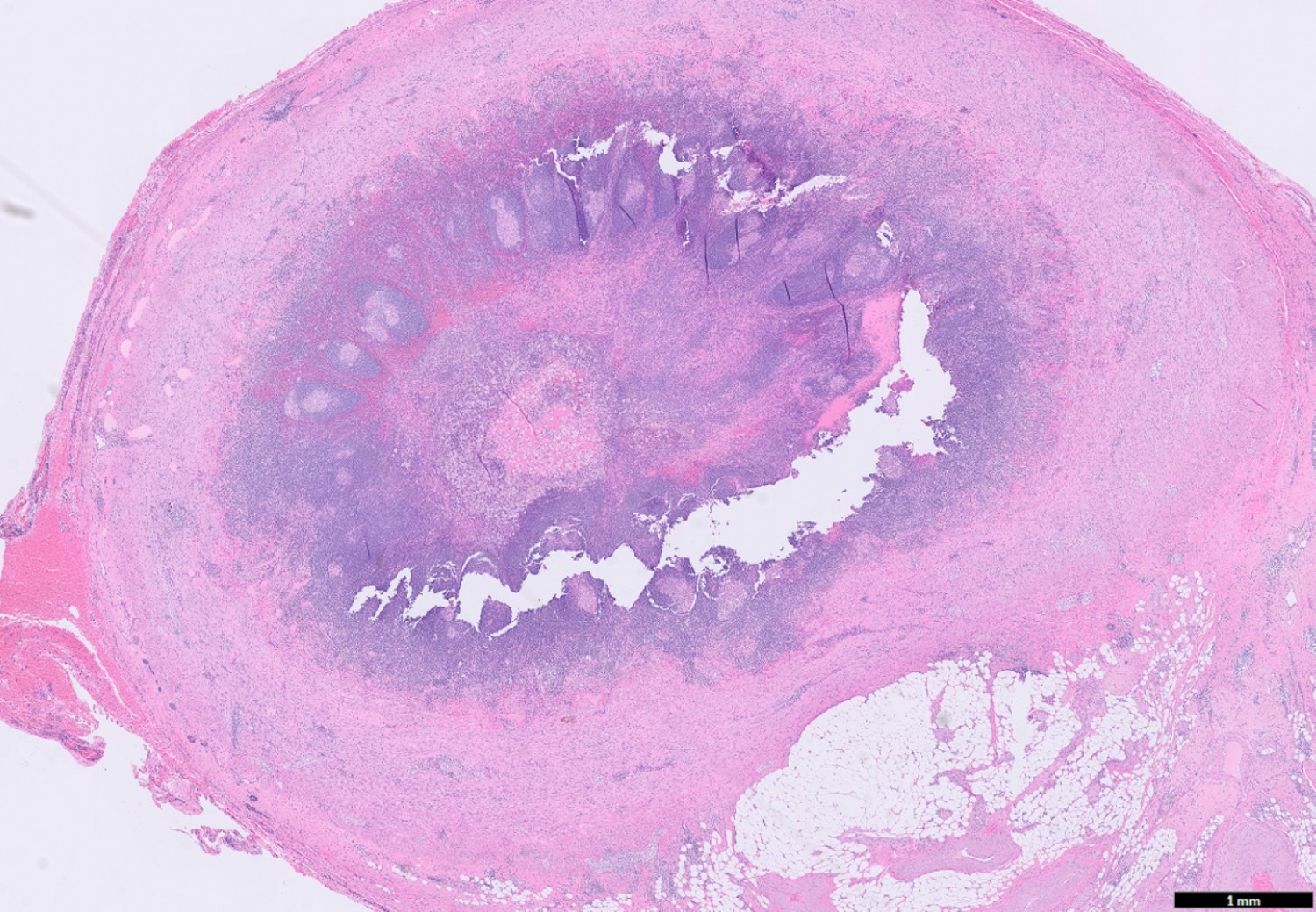
Granulomas and
xanthogranulomatous
inflammation
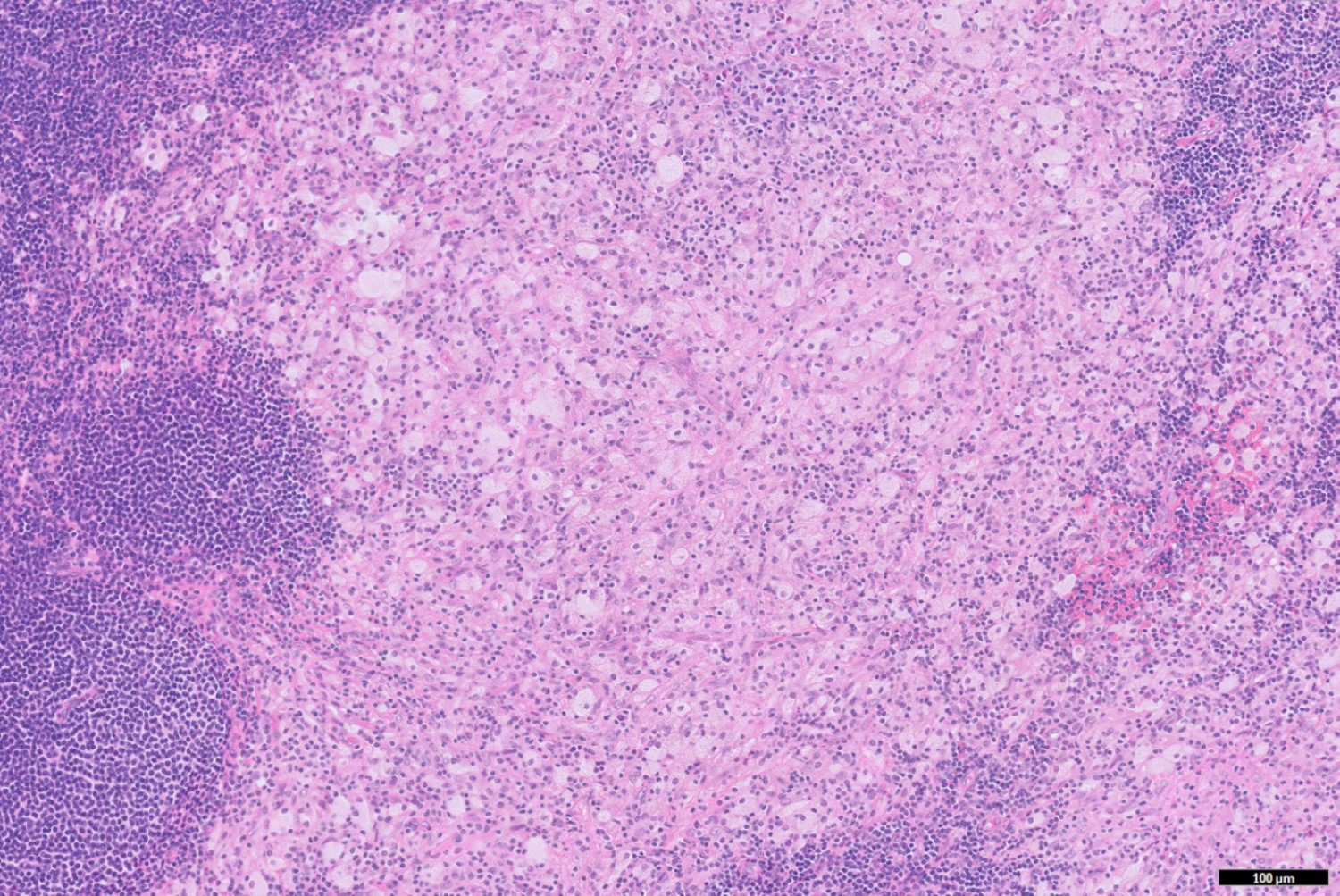
Xanthogranulomatous
inflammation
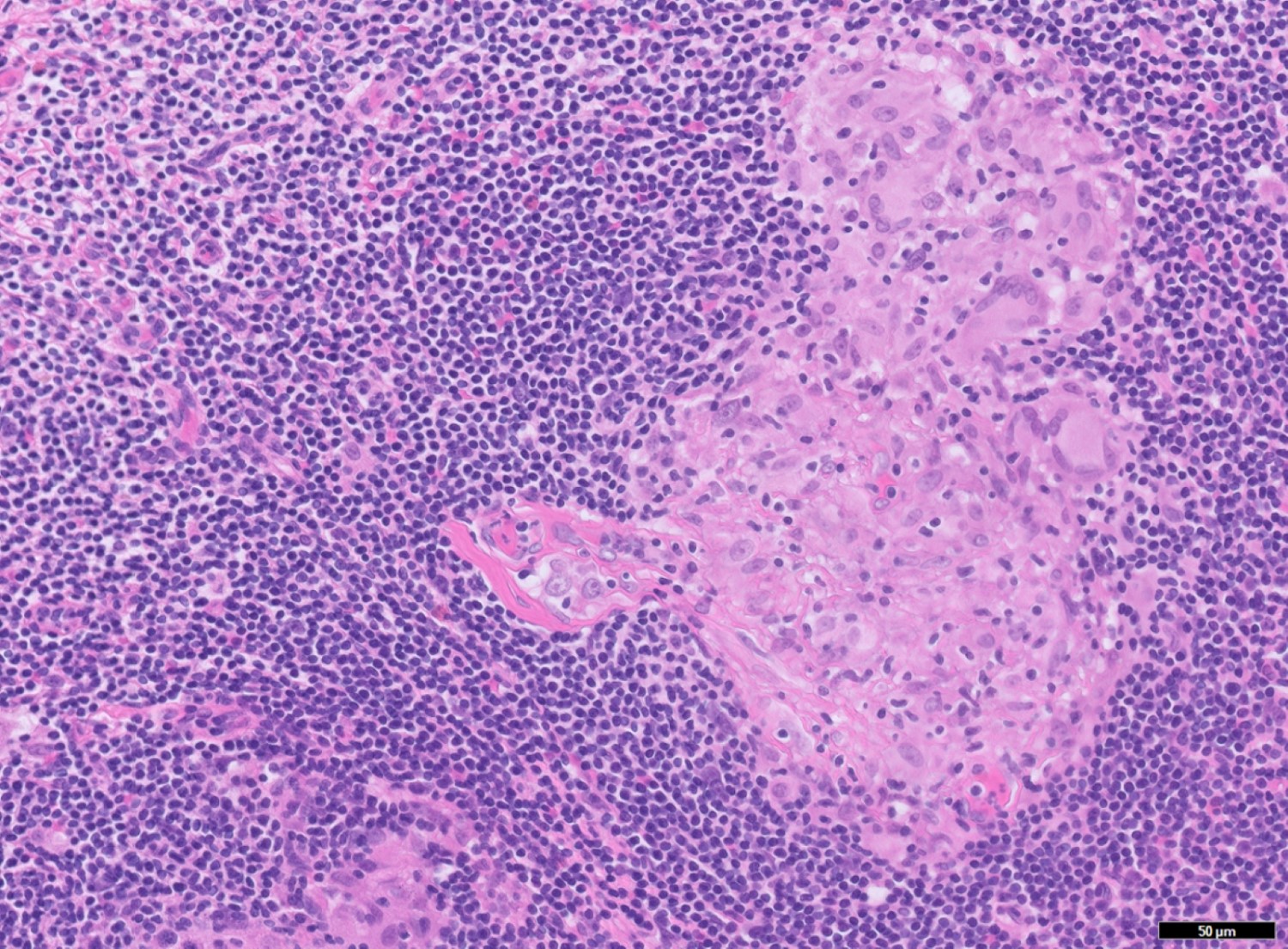
Granulomas
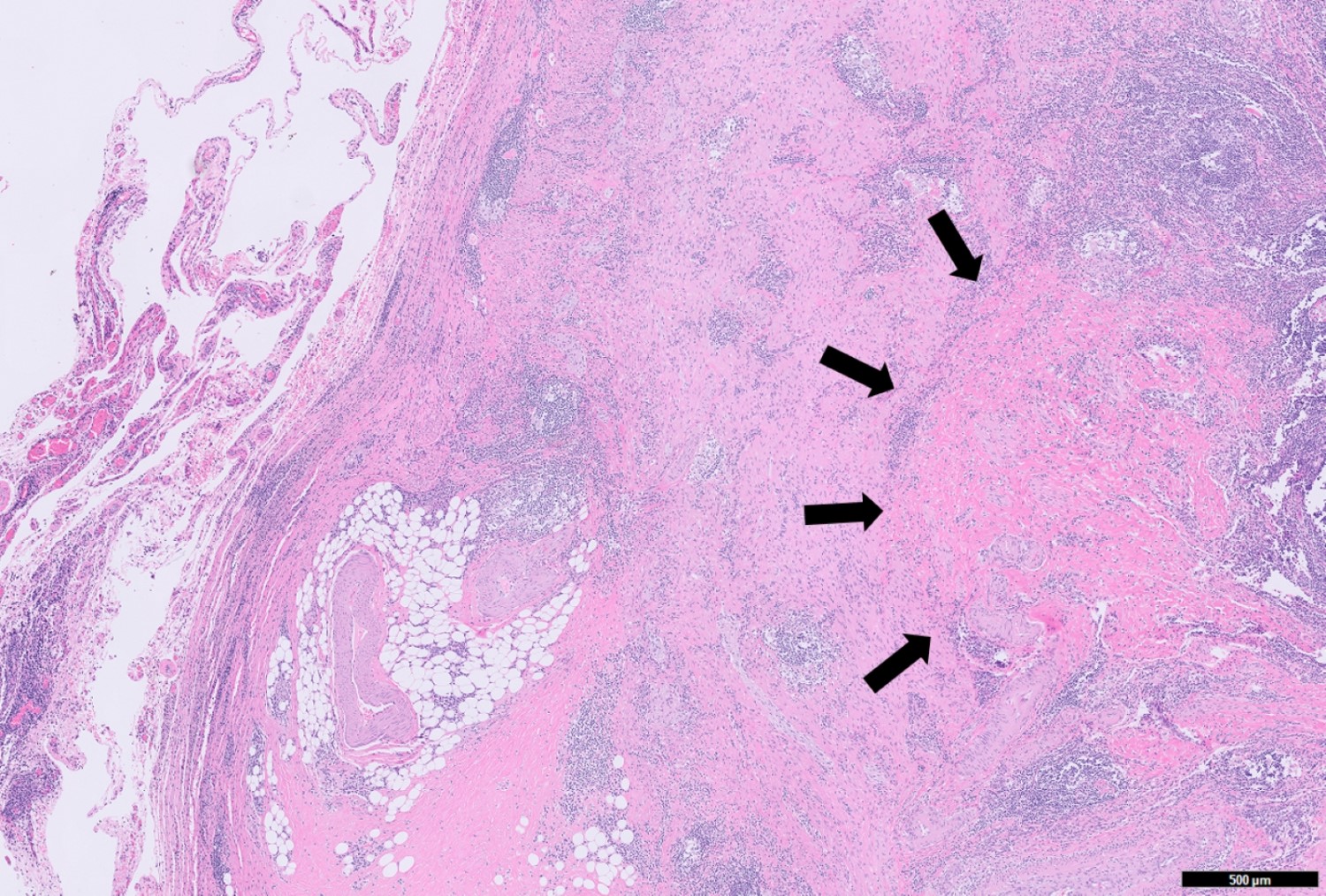
Mural fibrosis
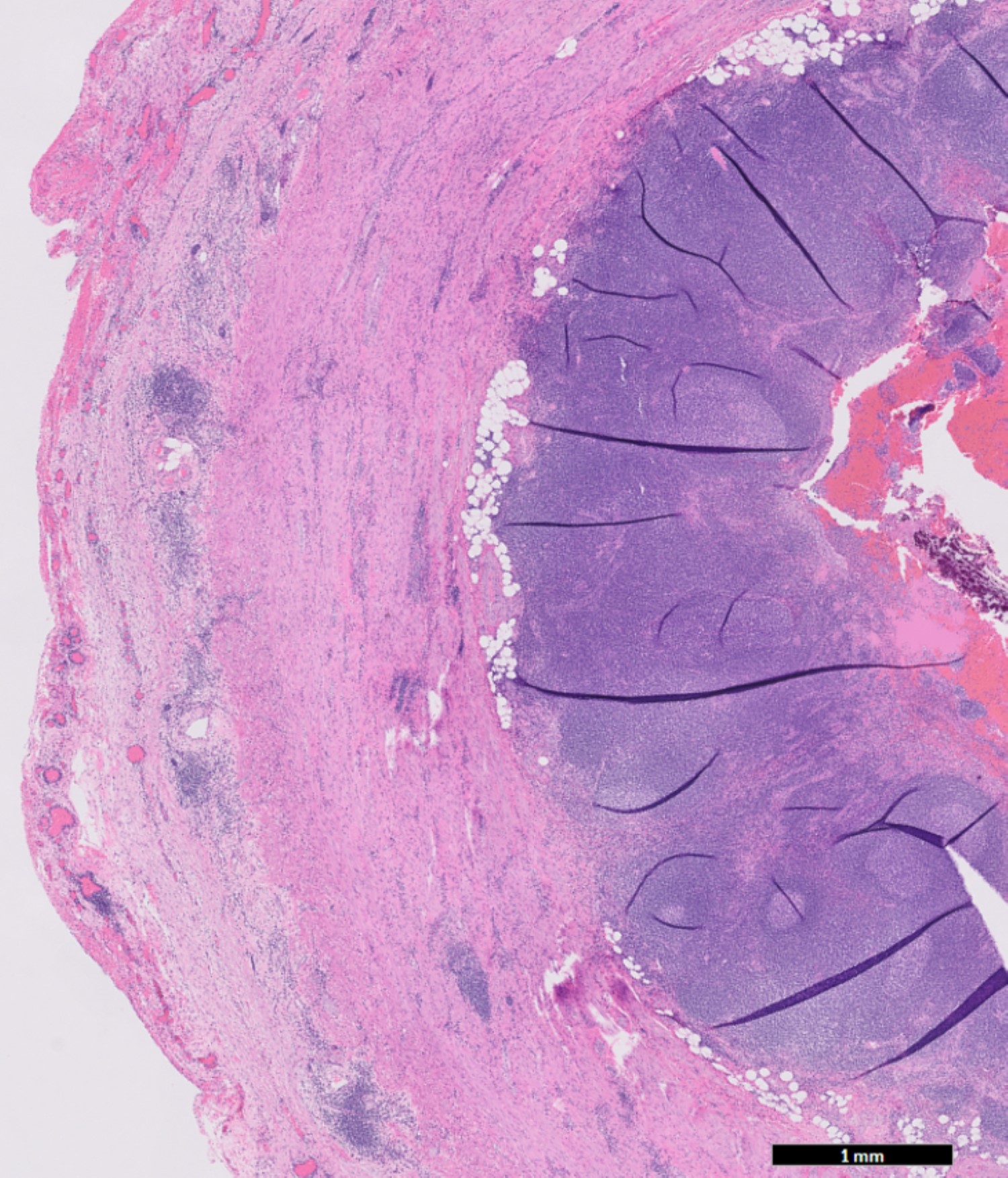
Transmural chronic inflammation
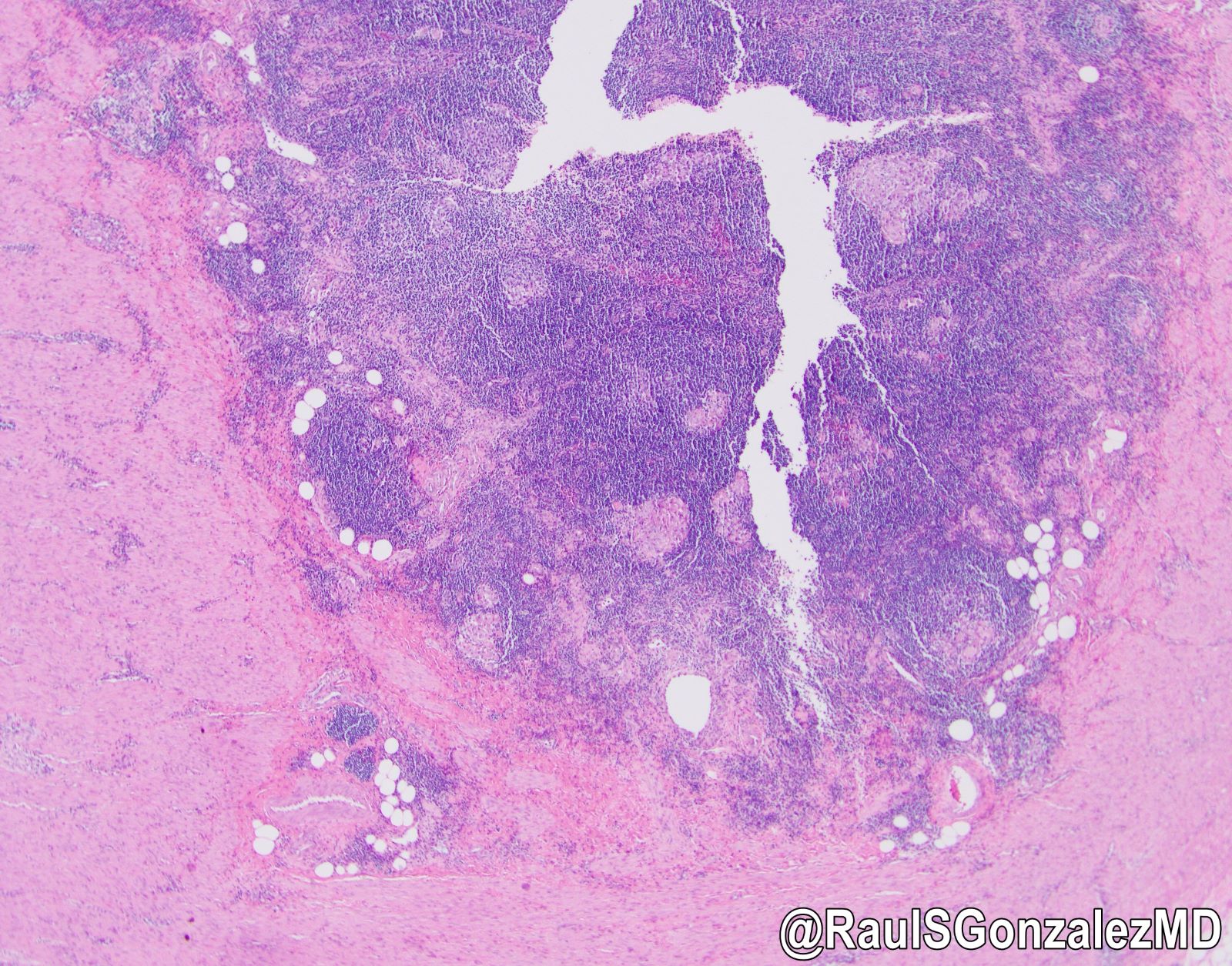
Interval appendicitis
Sample pathology report
- Appendix, interval appendectomy:
- Appendix with active chronic appendicitis featuring transmural chronic inflammation, multiple nonnecrotizing epithelioid cell granulomas, xanthogranulomatous inflammation, pulse granulomas and mural fibrosis, compatible with patient's history of interval appendectomy
- No microorganisms are seen utilizing special stains for Grocott methenamine silver (GMS) and acid fast bacteria (Ziehl-Neelsen)
Differential diagnosis
- Granulomatous appendicitis:
- Parasitic (schistosomiasis, strongyloidiasis), bacterial (Yersinia, mycobacteria, actinomycosis), fungal (candidiasis, histoplasmosis) infections:
- Yersinia spp. is the most common organism causing granulomatous appendicitis (Am J Surg Pathol 2001;25:508)
- Mucosal ulceration, epithelioid granulomas with prominent lymphoid cuff and giant cells, necrotizing granulomas may be present
- Yersinia spp. is the most common organism causing granulomatous appendicitis (Am J Surg Pathol 2001;25:508)
- Ancillary tests (e.g., stool culture, PCR) or clinical features (bloody diarrhea, pediatric population) may help with the diagnosis
- Parasitic (schistosomiasis, strongyloidiasis), bacterial (Yersinia, mycobacteria, actinomycosis), fungal (candidiasis, histoplasmosis) infections:
- Sarcoidosis:
- GI tract is uncommonly involved
- Systemic disease and diagnosis of exclusion
- Presentation of extra-appendiceal involvement may be helpful
- Crohn's disease:
- Clinical history with evidence of Crohn's disease elsewhere in the GI tract
- Appendix involvement can be found in 7 - 40% ileocecal resection specimens in patients with Crohn's disease (Virchows Arch 2002;440:397, Am J Surg Pathol 2021;45:1703)
- Low grade appendiceal neoplasm (LAMN):
- Grossly dilated lumen filled with mucin
- Epithelium with low grade dysplasia, which can be flattened or with undulating changes
- Broad pushing invasion may be present
Board review style question #1
A 65 year old man presented to the emergency room with decreased appetite and right lower abdominal pain. He was noted to have a fever 1 week ago that had resolved at the time of presentation. The patient has no known significant medical history. CT image showed an abscess around the cecum. Antibiotics was initiated and percutaneous drainage was performed. The patient came back 2 months later for appendectomy. The H&E image of the surgical specimen is shown. What is the most likely diagnosis?
- Acute appendicitis
- Adenocarcinoma of the appendix
- Interval appendicitis
- Crohn's disease
- Lymphoma
Board review style answer #1
C. Interval appendicitis. According to the clinical history provided, the patient was presented with acute appendicitis about 2 months ago and came back for a delayed appendectomy. There is no evidence of infection, inflammatory bowel disease or other significant medical history. H&E image showed a benign appendix with transmural chronic inflammation. Both clinical history and histological findings support a diagnosis of interval appendicitis.
Comment Here
Reference: Interval appendicitis
Comment Here
Reference: Interval appendicitis
Board review style question #2
Which of the following descriptions is true regarding interval appendicitis?
- Interval appendicitis is a chronic inflammatory process; thus, acute inflammation should not be identified microscopically
- The main purpose of interval appendectomy is to prevent recurrence of appendicitis
- Most patients with complicated appendicitis will undergo interval appendectomy after initial antibiotic management
- Scattered granulomas and xanthogranulomatous inflammation can be seen in interval appendectomy specimens
- Transmural chronic inflammation and granulomas are characteristic features of Crohn's disease, which is not seen in interval appendicitis
Board review style answer #2
D. Interval appendicitis is characterized by histologic features of a chronic inflammatory process, such as the presence of scattered granulomas, xanthogranulomatous inflammation, and macrophages laden with hemosiderin, among others. Interval appendectomy is performed in selective patients with risk factors but not in most patients (see Treatment section). It has a wide spectrum of histological findings including acute inflammation. Crohn’s-like features can often be seen in interval appendectomy specimen.
Comment Here
Reference: Interval appendicitis
Comment Here
Reference: Interval appendicitis

