
Anus & perianal area
Carcinoma
Adenocarcinoma
Author: Raul S. Gonzalez, M.D.
Editorial Board Member: Xiaoyan Liao, M.D., Ph.D.
Deputy Editor-in-Chief: Aaron R. Huber, D.O.

Last author update: 23 May 2023
Last staff update: 6 February 2025 (update in progress)
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Adenocarcinoma anus


Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Diagrams / tables | Clinical features | Diagnosis | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Gonzalez RS. Adenocarcinoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/anusadenocarcinoma.html. Accessed April 2nd, 2025.
Definition / general
- Rare adenocarcinoma that primarily involves the anal canal (not rectal adenocarcinomas with downward spread)
Essential features
- Rare, primary gland forming malignancy of the anus
- May arise from anal glands, from congenital anorectal duplications or along a fistula tract
- Must be distinguished from adenocarcinoma secondarily involving anus (e.g., rectal carcinoma)
Terminology
- Also known as perianal adenocarcinoma or perianal gland adenocarcinoma
- The term anal duct adenocarcinoma is not recommended
ICD coding
- ICD-10: C21.0 - malignant neoplasm of anus, unspecified
Epidemiology
- 5% of anorectal malignancies (JCO Oncol Pract 2020;16:635)
- Slightly more common in white men (Cancer Med 2019;8:3855)
Sites
- Anus (by definition)
Pathophysiology
- May arise from anal glands, from congenital anorectal duplications or along a fistula tract (Dis Colon Rectum 1998;41:992)
- May demonstrate HPV 18 DNA but not HPV 16 DNA (Mod Pathol 1991;4:58)
- Accordingly, rare cases are linked to HPV infection and are positive for p16 (Mod Pathol 2020;33:944, Int J Surg Pathol 2021;29:672, Br J Cancer 2018;118:1302)
- Rare nonanal gland type, nonfistula associated anal carcinomas have recently been recognized (Pathol Int 2021;71:715)
Etiology
- Proposed etiologic associations include chronic fistula, anal Crohn's disease and anal sexual intercourse (Semin Surg Oncol 1994;10:235)
Diagrams / tables
Images hosted on other servers:

Classification
of anal
adenocarcinoma
Clinical features
- May present in fistula tract or as a vaginal cyst
- Often a long history of perianal fistulas, abscesses, surgery
- Indolent course with gradual progression
Diagnosis
- Gross examination and tissue sampling
Prognostic factors
- Poor prognosis associated with advanced T and N category disease and higher histologic grade (Int J Radiat Oncol Biol Phys 2003;56:1274)
Case reports
- 42 year old man with anal tenderness (Medicine (Baltimore) 2021;100:e27083)
- 70 year old man with firm perianal nodule (BMJ Open Gastroenterol 2021;8:e000661)
- 72 year old man with Crohn's disease and perianal fistula (Cureus 2022;14:e31339)
- 84 year old man with adenocarcinoma arising from an anal gland (Int J Surg Case Rep 2014;5:234)
Treatment
- Standard treatment includes abdominoperineal resection; adding chemotherapy and radiation improves outcome (Int J Radiat Oncol Biol Phys 2003;56:1274)
Clinical images
Images hosted on other servers:

Irregular mucosa and angioectasia
Gross description
- Anal canal tumors are nodular, ulcerated, 3 - 4 cm or more, invade deeply into wall and spread proximally and distally into submucosa of distal rectum and proximal anus
Gross images
Images hosted on other servers:

Anal canal cancer
Microscopic (histologic) description
- Adenocarcinomas with an intestinal type appearance involving the anus are likely of rectal origin and should be regarded as such
- True anal gland adenocarcinomas form haphazardly dispersed small glands with scant mucin production that invade the wall of the anorectal area without an intraluminal component (Cancer 2001;92:2045)
- Fistula associated adenocarcinomas are often mucinous (> 50% of tumor volume consists of mucin); granulomatous reaction to mucin may be present
- May contain melanin pigment, perhaps due to tumor cell phagocytosis of melanin from melanocytes (Am J Surg Pathol 1981;5:711)
- Single neoplastic cells may colonize the overlying and adjacent squamous mucosa (Paget disease)
- HPV related cases show papillary or villiform structures lined by columnar cells that often contain abundant mucin (Mod Pathol 2020;33:944)
Microscopic (histologic) images
Contributed by Raul S. Gonzalez, M.D.
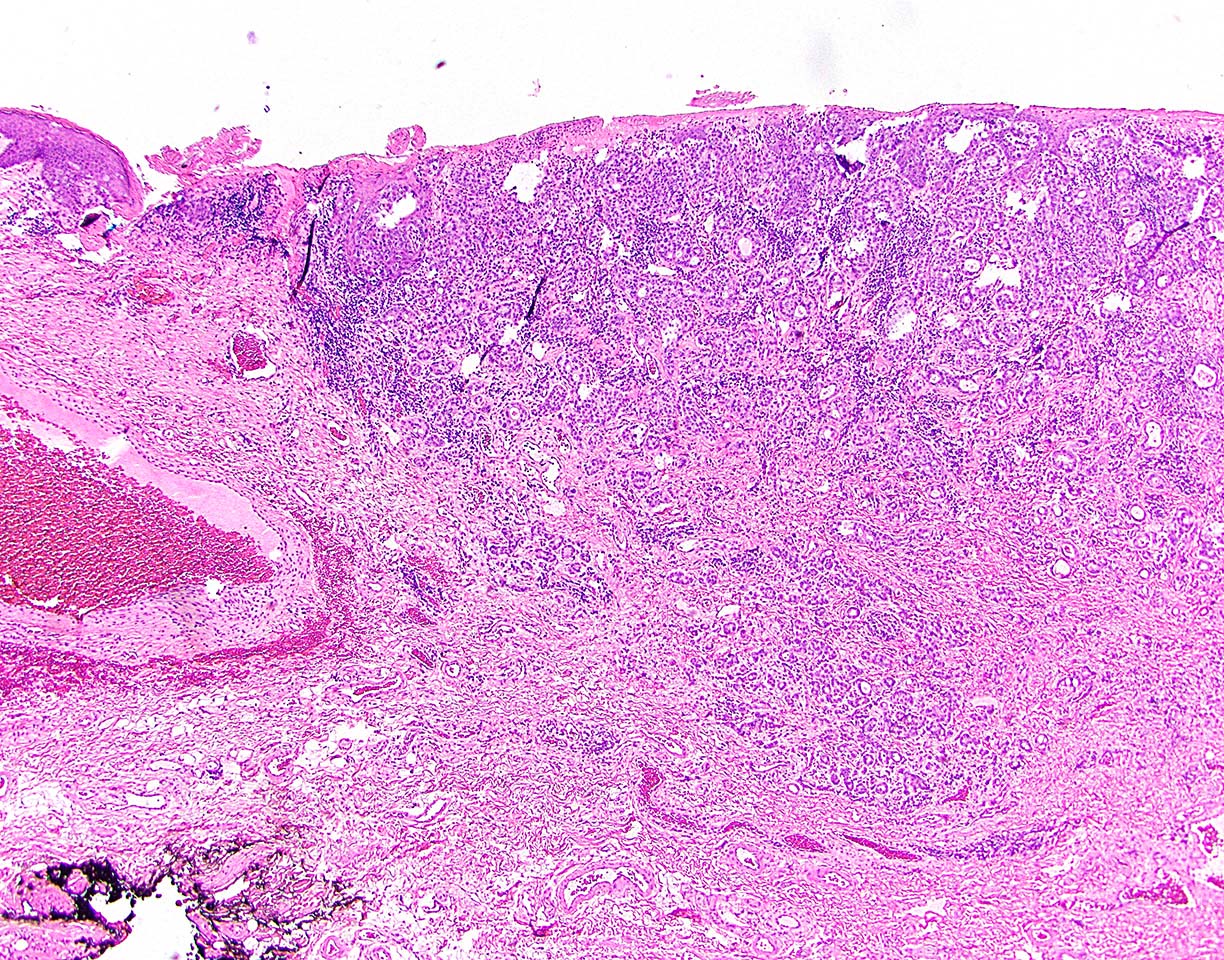
Infiltrating, gland forming
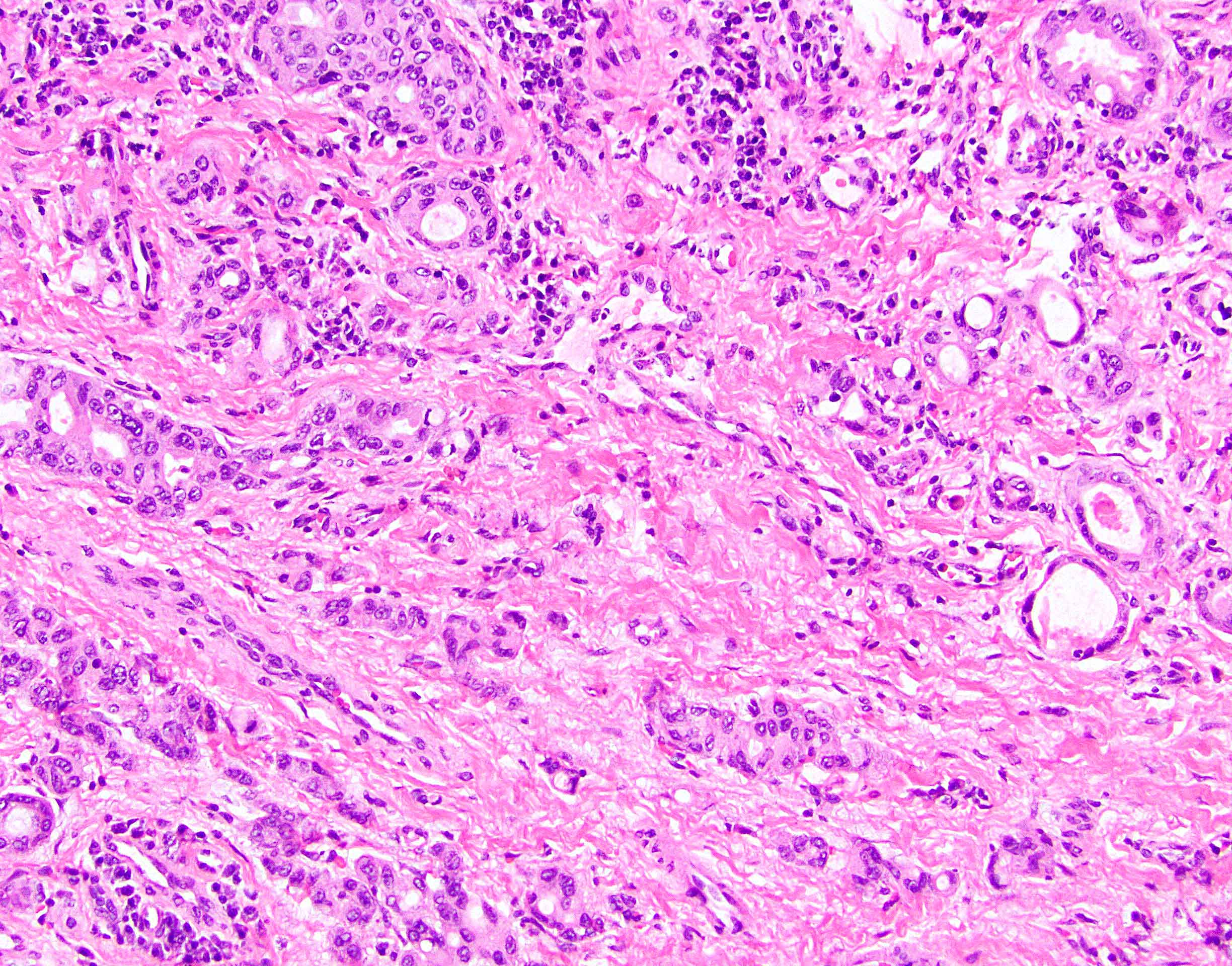
Infiltrating glands
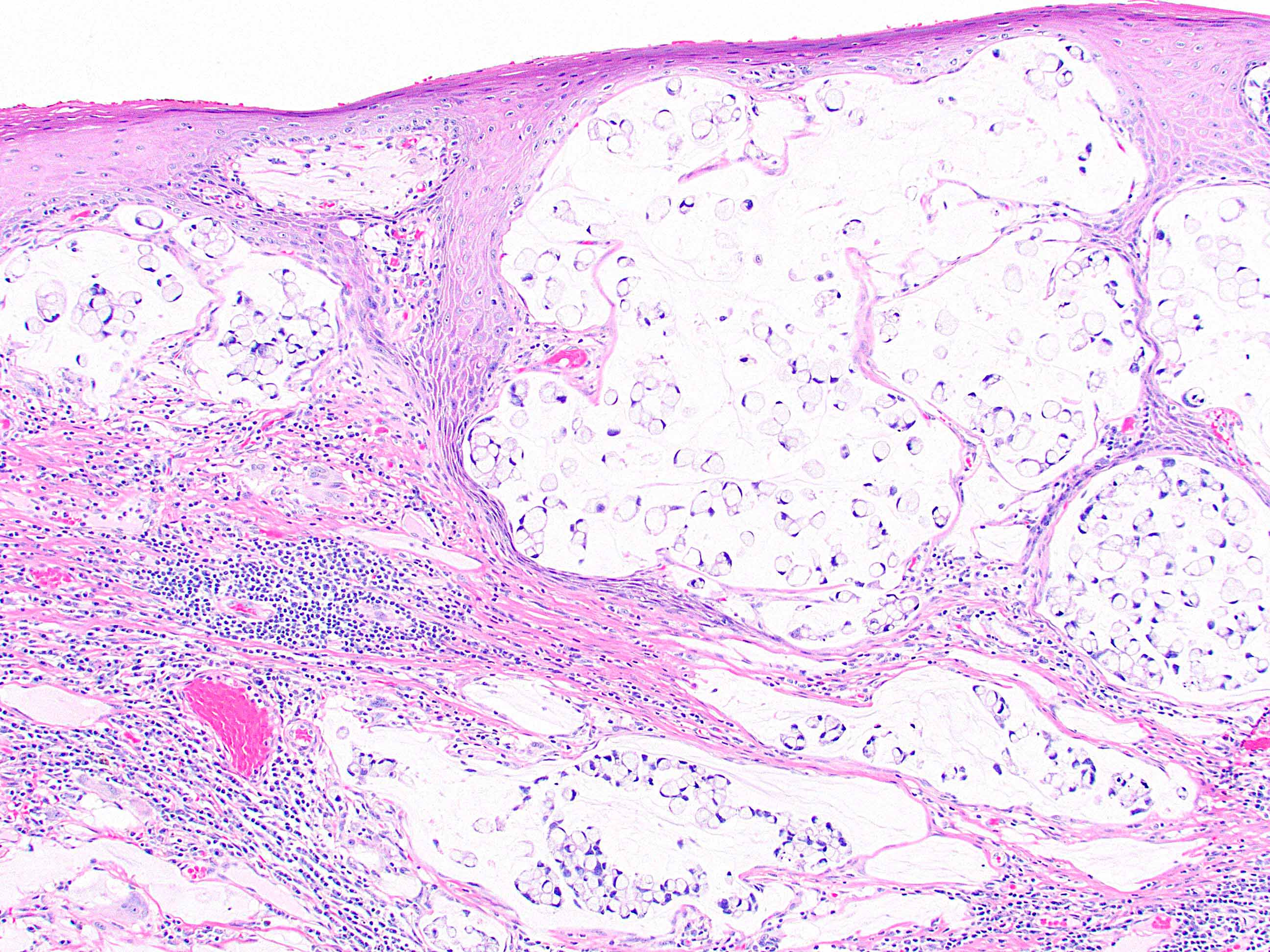
Mucinous and signet ring
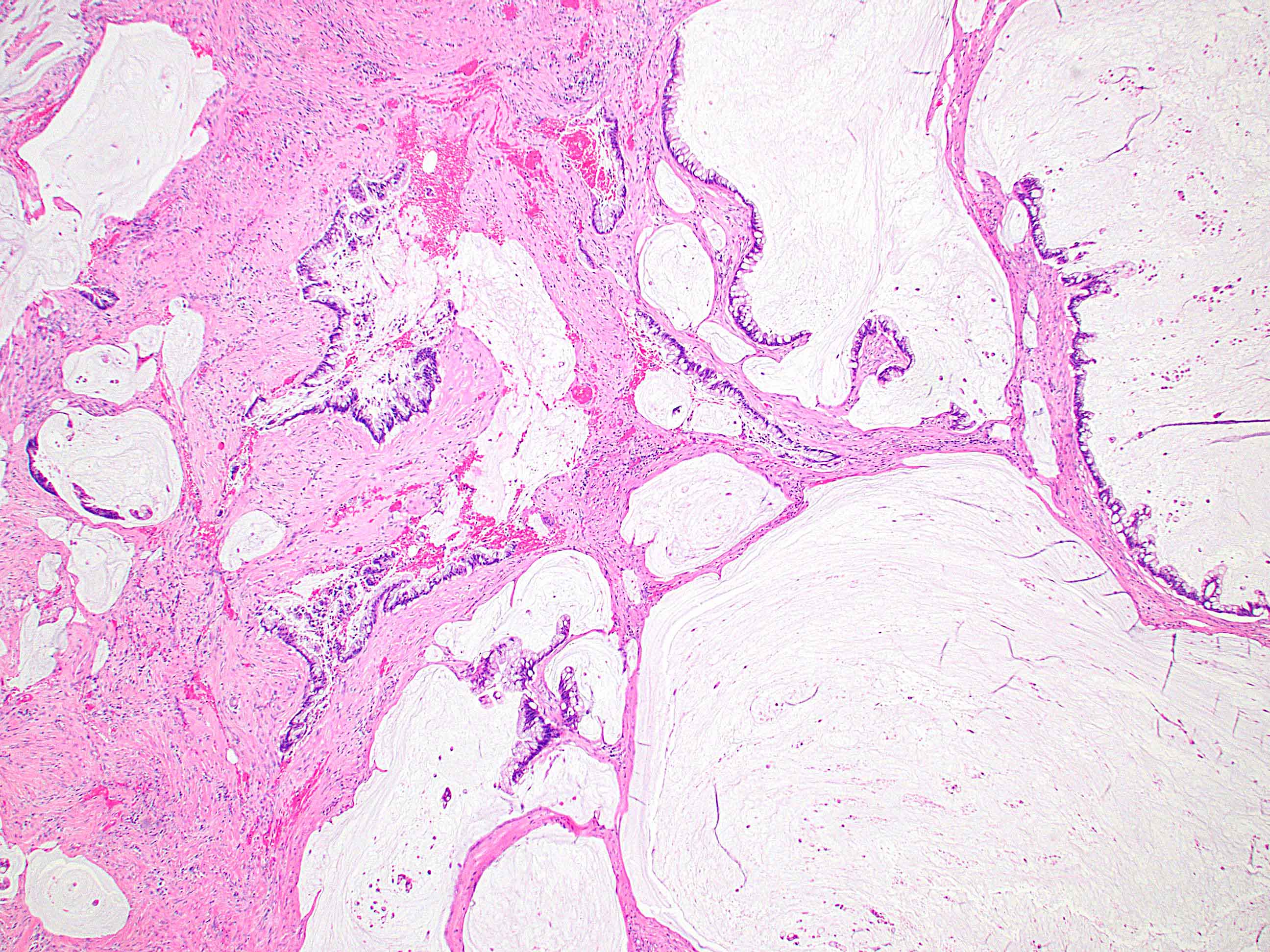
Fistula tract associated
Positive stains
Negative stains
- CK20, CDX2, usually p16 (Arch Pathol Lab Med 2007;131:1304)
Molecular / cytogenetics description
- KRAS mutations in 47%, NRAS mutations in 6% (Br J Cancer 2018;118:1302)
Sample pathology report
- Anus, resection:
- Anal adenocarcinoma, moderately differentiated (see synoptic report)
Differential diagnosis
- Anal mucoepidermoid carcinoma:
- Rare (J Gastroenterol 2001;36:508)
- Secondary involvement by rectal adenocarcinoma:
- More common than primary anal adenocarcinoma
- Usually CK20+
- May require clinical correlation
- Squamous cell carcinoma:
- Far more common at this location
- Distinguishable microscopically
- Secondary involvement by gynecologic tract adenocarcinoma:
Additional references
Board review style question #1
Which of the following is true about primary anal adenocarcinoma?
- Advanced stage cases paradoxically have a better prognosis
- It can arise in a fistula tract
- It is more common in women
- It is more common than secondary involvement by rectal carcinoma
Board review style answer #1
B. It can arise in a fistula tract. This may occur in patients with Crohn's disease. Overall, anal adenocarcinoma is more common in men and advanced stage indicates poor prognosis. It is rare and secondary anal involvement by rectal carcinoma is more common.
Comment Here
Reference: Anal adenocarcinoma
Comment Here
Reference: Anal adenocarcinoma
Board review style question #2
Primary anal adenocarcinoma is usually positive for which of the following immunohistochemical stains?
- CDX2
- CK7
- CK20
- p16
Board review style answer #2
B. CK7. Only rare cases of anal adenocarcinoma are positive for p16. Rectal carcinoma involving the anus is positive for CDX2 and CK20.
Comment Here
Reference: Anal adenocarcinoma
Comment Here
Reference: Anal adenocarcinoma
