

Anus & perianal area
Other tumors
Granular cell tumor
Editorial Board Member: Monika Vyas, M.D.
Deputy Editor-in-Chief: Aaron R. Huber, D.O.


Last author update: 9 January 2024
Last staff update: 9 January 2024
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: Granular cell tumor

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Electron microscopy description | Electron microscopy images | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Kharoud H, Gonzalez RS. Granular cell tumor. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/anusGCT.html. Accessed December 30th, 2024.
Definition / general
- Rare, benign anal neoplasm with neuroectodermal differentiation derived from Schwann cells and composed of epithelioid cells with abundant granular cytoplasm
Essential features
- Benign tumor with neuroectodermal differentiation
- Composed of oval to polyhedral cells with abundant eosinophilic granular cytoplasm
- Positive for S100 and CD68
Terminology
- Older terms, not recommended: Abrikossoff tumor, granular cell myoblastoma, granular cell schwannoma, granular cell nerve sheath tumor
ICD coding
- ICD-O
- ICD-10: D12.9 - benign neoplasm of anus and anal canal
- ICD-11
- 2E8Y & XH09A9 - other specified benign mesenchymal neoplasm & granular cell tumor, NOS
- XH90D3 - granular cell tumor, malignant
Epidemiology
- Granular cell tumors can occur at any age but are more common in adults in the fourth to sixth decades of life (StatPearls: Granular Cell Tumor [Accessed 29 November 2023])
- Strong predilection for women and Black patients (StatPearls: Granular Cell Tumor [Accessed 29 November 2023])
Sites
- Granular cell tumor can arise in various sites, including skin, head and neck, soft tissue, breast, gastrointestinal tract and peripheral nerves (Gastroenterol Hepatol (N Y) 2009;5:798)
- ~5 - 10% arise in the gastrointestinal tract, with the most common site being esophagus (StatPearls: Granular Cell Tumor [Accessed 29 November 2023])
- Very rarely occurs in anus and perianal area (scattered case reports only)
Pathophysiology
- Inactivating somatic mutations in the endosomal pH regulators ATP6AP1 and ATP6AP2 are seen in 72% of granular cell tumors (Nat Commun 2018;9:3533)
- Abnormal RAS-MAPK pathway cell signaling may be linked in granular cell tumors associated with syndromes (Clin Genet 2009;75:185)
Etiology
- Unclear for sporadic tumors
- Patients with multiple tumors may have Noonan syndrome, LEOPARD syndrome or neurofibromatosis type 1 (StatPearls: Granular Cell Tumor [Accessed 29 November 2023])
Clinical features
- Mostly discovered incidentally during endoscopy for other reasons, though may cause symptoms such as perianal discomfort, ulceration and bleeding
- Slow growing, painless anal lesion presenting as a polyp
Diagnosis
- Tissue sampling
Radiology description
- Ultrasound: hypoechoic mass (J Int Med Res 2021;49:300060520982689)
- Magnetic resonance imaging: ovoid and solid mass with low signal intensity on T1 weighted image and high intensity on T2 images (Radiol Case Rep 2019;14:1047)
Radiology images
Images hosted on other servers:

MRI of perianal mass

Ultrasound of perianal mass
Prognostic factors
- Most granular cell tumors are benign and do not recur or spread
- Size > 5 cm and metastatic behavior indicate poor prognosis (J Surg Oncol 2018;118:891)
- Metastatic behavior is the only diagnostic criterion for malignancy (Pathol Res Pract 2011;207:164)
Case reports
- 36 year old woman with slow growing painless lump in perianal region (Curr Probl Diagn Radiol 2017;46:452)
- 46 year old woman with perianal nodular lesion (Tumori 2009;95:538)
- 56 year old man with papule of the anus (Presse Med 2003;32:221)
- 66 year old woman with polypoid lesion in the anus with hemorrhoids (Int Surg 2014;99:45)
- 75 year old woman with granular cell tumor of the internal anal sphincter (Dis Colon Rectum 2000;43:1444)
Treatment
- Local excision
Clinical images
Images hosted on other servers:

Anal polypoid mass

Perianal cutaneous nodule
Gross description
- Poorly circumscribed, firm, tan-yellow to tan-white nodule
Gross images
Images hosted on other servers:

Excision of perianal tumor
Microscopic (histologic) description
- Poorly circumscribed sheets, nests, lobules or ribbons of cells within collagenous stroma
- Longstanding lesions can show desmoplastic stroma (StatPearls: Granular Cell Tumor [Accessed 29 November 2023])
- Monotonous oval to polyhedral to spindled cells with distinct cell borders, abundant eosinophilic granular cytoplasm and rare mitotic figures
- Large eosinophilic dense granules called phagolysosomes are frequently seen (StatPearls: Granular Cell Tumor [Accessed 29 November 2023])
- Nuclei are eccentrically located, with regular nuclear borders and inconspicuous nucleoli (StatPearls: Granular Cell Tumor [Accessed 29 November 2023])
- Perineural invasion can be seen (Am J Dermatopathol 2012;34:800)
- Pseudoepitheliomatous hyperplasia can be seen in the overlying skin (Dig Dis Sci 1981;26:807)
- Atypical cases may show vesicular nucleoli with prominent nucleoli, high N:C ratio, increased mitotic activity and geographic necrosis (Virchows Arch 2016;468:527)
Microscopic (histologic) images
Contributed by Raul S. Gonzalez, M.D.

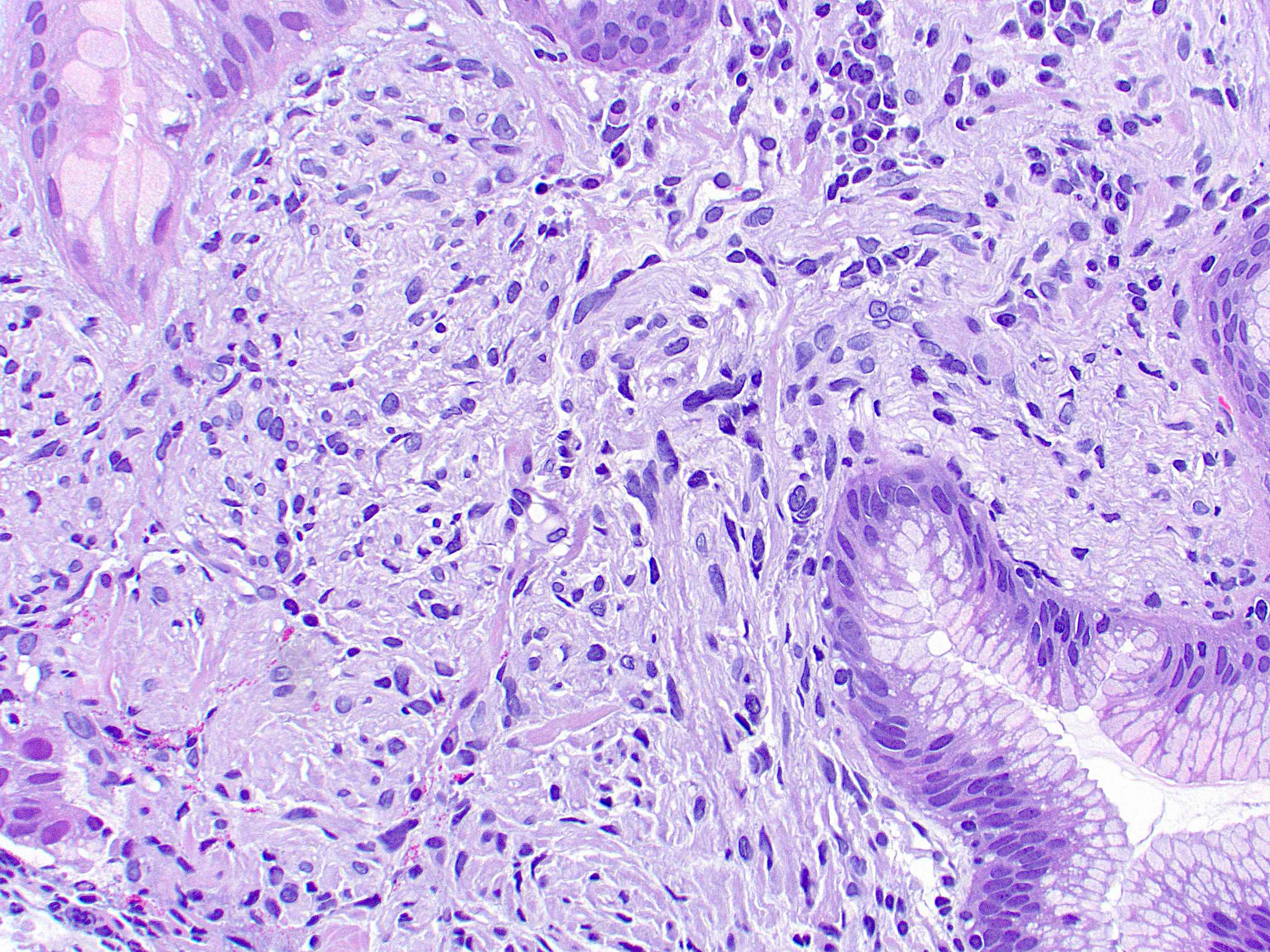
Gastroesophageal junction lesion
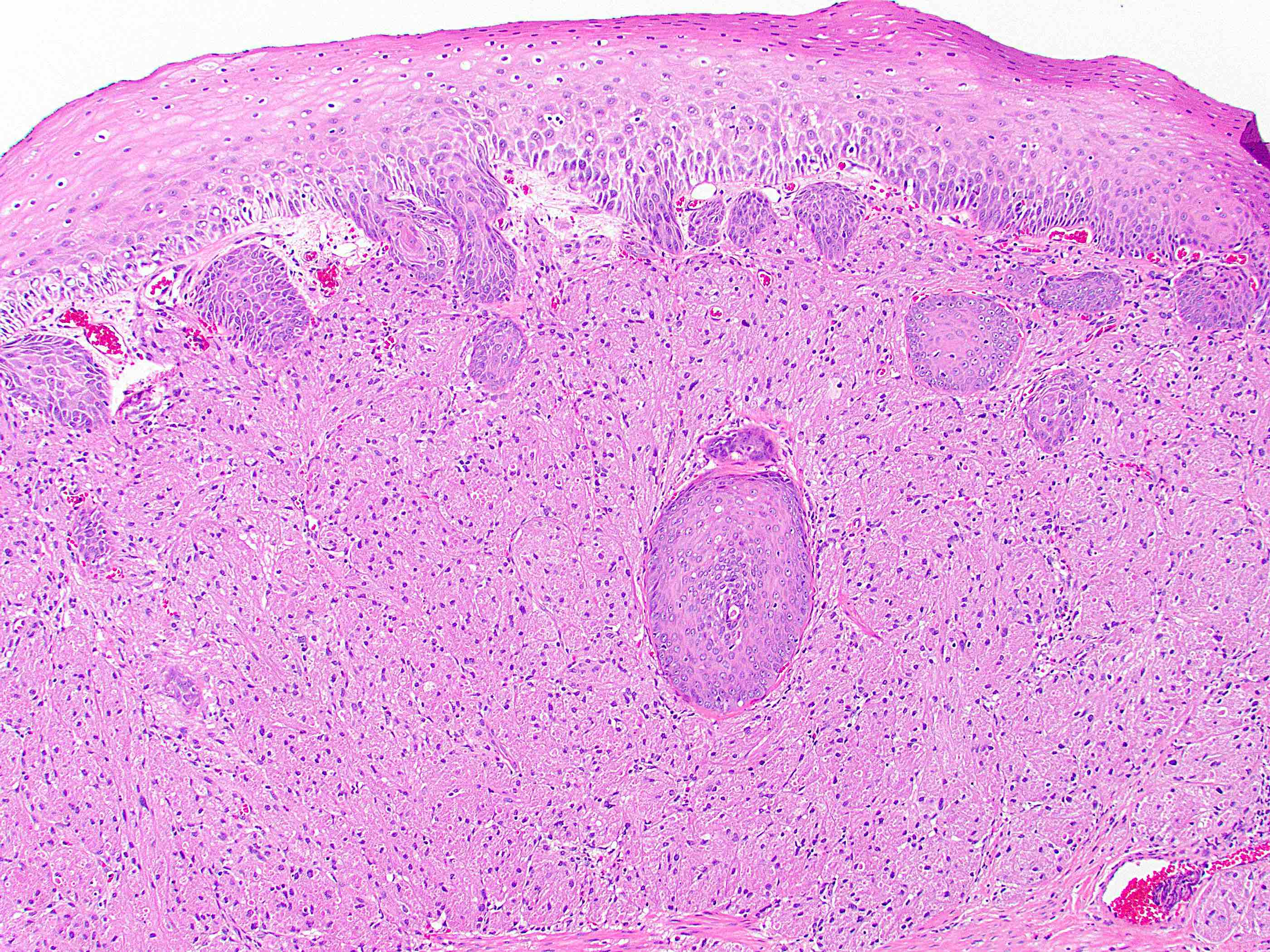
Pseudoepitheliomatous
hyperplasia
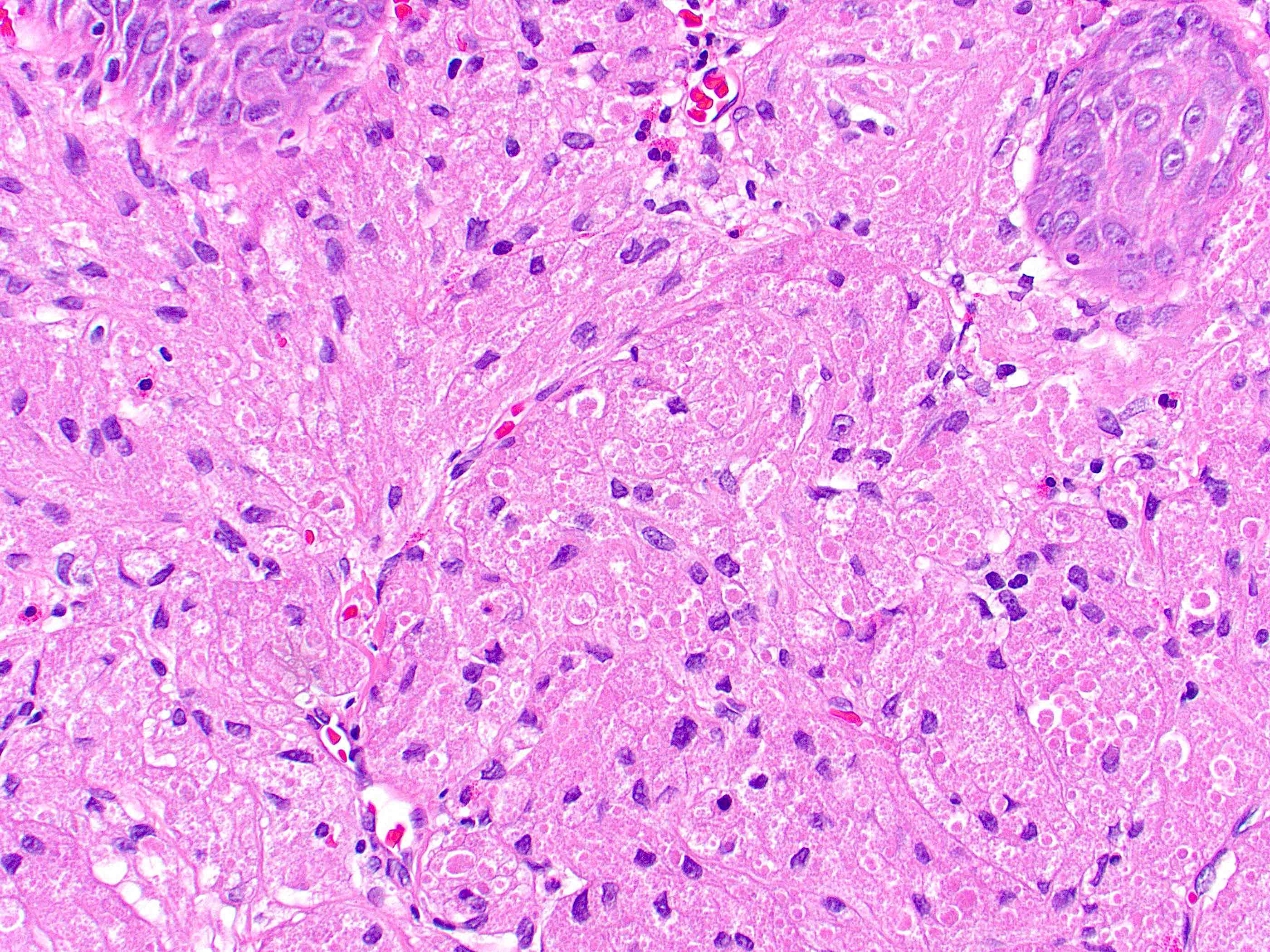
Phagolysosomes
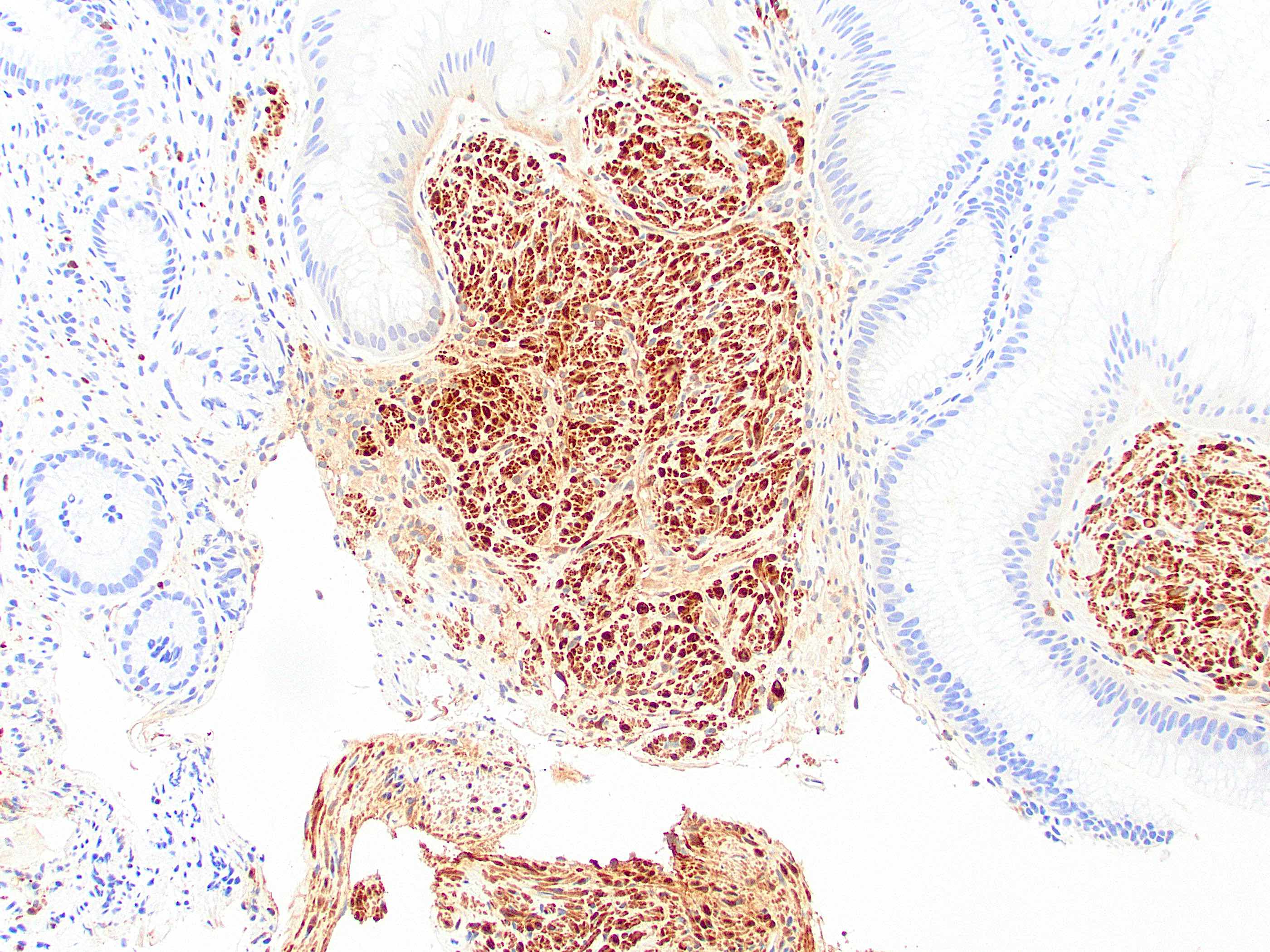
S100
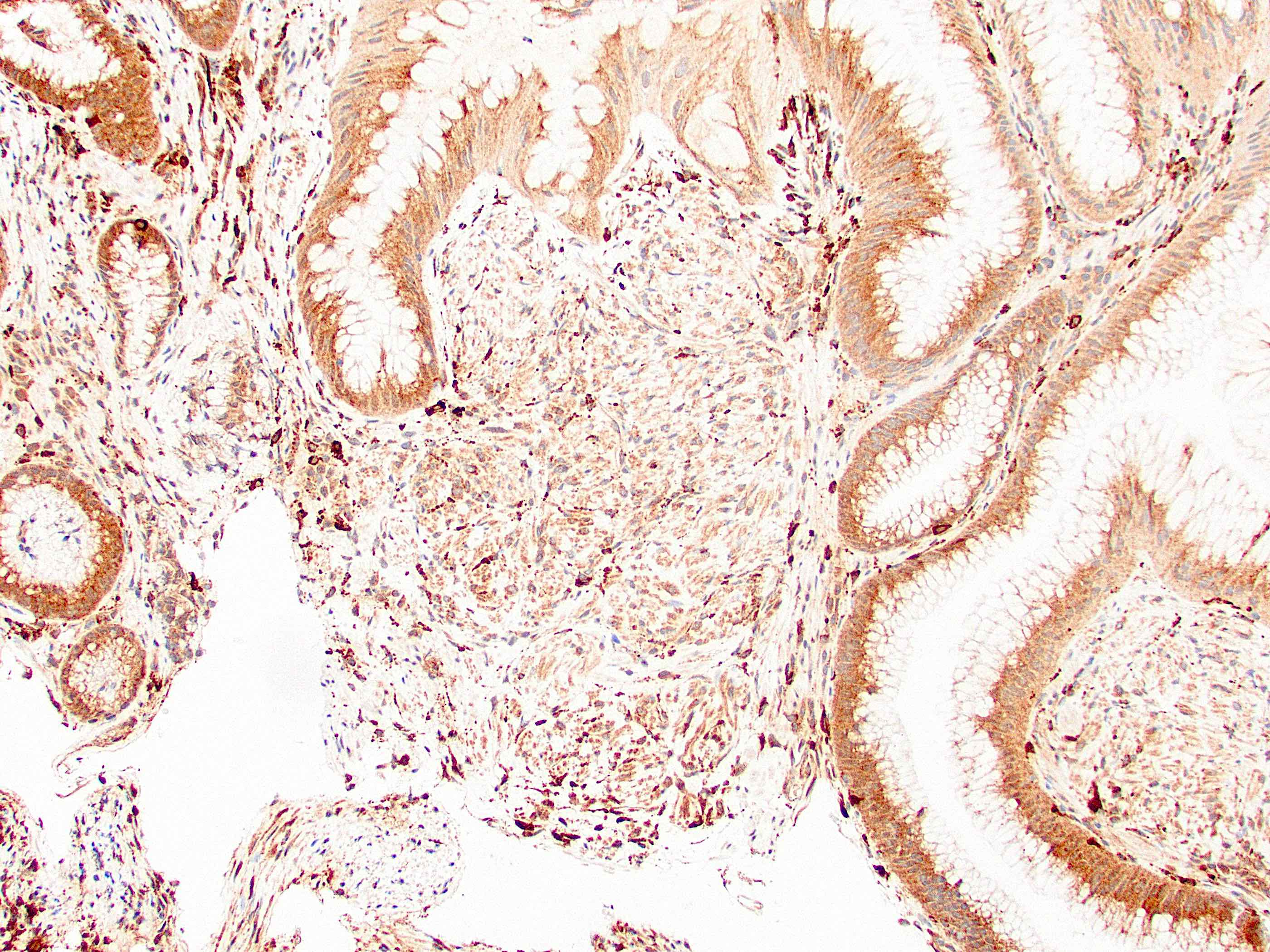
CD68
Positive stains
Negative stains
Electron microscopy description
- Cytoplasmic lysosomes with prominent myelin figures (J Surg Oncol 1980;13:301)
Electron microscopy images
Images hosted on other servers:

Ultrastructural view
Molecular / cytogenetics description
- Soft tissue cases often have loss of function mutations in ATP6AP1 and ATP6AP2; anal cases have not been tested
Sample pathology report
- Anal, mass, resection:
- Granular cell tumor, 1.1 cm (see comment)
- Surgical margins negative for tumor
- Comment: Immunohistochemical stains show the tumor is positive for S100 and CD68. Granular cell tumors are rare in the anus but have been reported.
Differential diagnosis
- Adult rhabdomyoma:
- Benign tumor with skeletal muscle differentiation
- Also shows round cells with eosinophilic cytoplasm
- Cells show multiple nuclei and peripheral cross striations
- Positive for desmin, muscle specific actin, myoD1, myoglobin
- Alveolar soft part sarcoma:
- Squamous cell carcinoma:
- Most common malignancy of anus
- Architecture of pseudoepitheliomatous hyperplasia overlying granular cell tumor may mimic malignancy
- Squamous cell carcinoma shows clear cytologic atypia
Board review style question #1
A 55 year old woman presents with a painless 2 cm perianal mass, which is excised. It is positive for S100 and CD68. Which of the following is the most likely diagnosis?
- Alveolar soft part sarcoma
- Gastrointestinal stromal tumor
- Granular cell tumor
- Squamous cell carcinoma
Board review style answer #1
C. Granular cell tumor. The histologic appearance and immunohistochemical profile are consistent with granular cell tumor. Answers A, B and D are incorrect because the other lesions are negative for S100 and CD68. Alveolar soft part sarcoma and squamous cell carcinoma would show more cytologic atypia and gastrointestinal stromal tumor would likely be spindled.
Comment Here
Reference: Granular cell tumor
Comment Here
Reference: Granular cell tumor
Board review style question #2
Which of the following statements is true for granular cell tumor of the anus?
- It can never metastasize
- It is a fast growing painful lesion that infiltrates into the surrounding structures
- It is the most common site for granular cell tumors in the digestive tract
- It may arise in syndromic patients
Board review style answer #2
D. It may arise in syndromic patients. Multiple granular cell tumors can occur in patients with Noonan syndrome, LEOPARD syndrome and neurofibromatosis 1. The anus is a potential site. Answer B is incorrect because granular cell tumors are slow growing and painless. Answer A is incorrect because they very rarely metastasize. Answer C is incorrect because the esophagus is the most common site for digestive tract granular cell tumors.
Comment Here
Reference: Granular cell tumor
Comment Here
Reference: Granular cell tumor

