
Adrenal gland & paraganglia
Other tumors
Adenomatoid tumor
Editorial Board Member: Bonnie Choy, M.D.
Deputy Editor-in-Chief: Maria Tretiakova, M.D., Ph.D.

Last author update: 16 September 2021
Last staff update: 12 August 2024
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Adrenal adenomatoid tumor


Table of Contents
Definition / general | Essential features | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Electron microscopy description | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1Cite this page: Lehman KA, Zynger DL. Adenomatoid tumor. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/adrenaladenomatoid.html. Accessed April 3rd, 2025.
Definition / general
- Rare benign nonfunctioning tumor of the adrenal gland of mesothelial origin
Essential features
- Proliferation of gland-like or vascular-like spaces lined by attenuated to columnar mesothelial cells
- Rare nonfunctioning tumor of the adrenal gland typically found incidentally
- Often confused on imaging and microscopy with tumors such as lymphangioma
- Accurate diagnosis relies upon microscopic examination, typically with immunohistochemistry
- Benign, with no reported cases of tumor recurrence following surgical excision
Epidemiology
- M:F = 10:1 (Adv Anat Pathol 2009;16:424)
- Age range 30 - 50 years, with peak incidence ~40 years (Adv Anat Pathol 2009;16:424)
- Extremely uncommon, with ~40 cases reported (Front Endocrinol (Lausanne) 2021;12:692553)
Sites
- Adrenal cortex and medulla
Pathophysiology
- Thought to arise via entrapment of primitive mesenchymal cells from the Müllerian tract within the adrenal gland versus embolized mesothelial cells (Am J Surg Pathol 2003;27:969)
Etiology
- Unknown
Clinical features
- Typically asymptomatic and discovered incidentally
- Rarely, reports of symptoms resulting from elevations in adrenal hormones (homovanillic acid, hyperaldosteronism) secondary to stimulation of normal adrenal parenchyma by tumor (Adv Anat Pathol 2009;16:424)
Diagnosis
- Diagnosis cannot be made using imaging alone, as adrenal adenomatoid tumors lack specific radiologic features
- Surgical excision (preferred) or core biopsy with subsequent histopathologic evaluation necessary for diagnosis
- Easily confused with more common tumors when evaluated via light microscopy so immunohistochemistry plays a key role in accurate diagnosis (Adv Anat Pathol 2009;16:424)
Radiology description
- Nonspecific; misdiagnosed as nonfunctioning adrenocortical tumor or other more common entities
- May be well visualized on CT or MRI, with a wide range of presentations reported on imaging
- Appearance ranges from homogeneous and solid to cystic degeneration or calcifications (Eur Radiol 1999;9:552)
Radiology images
Contributed by Firas G. Petros, M.D.
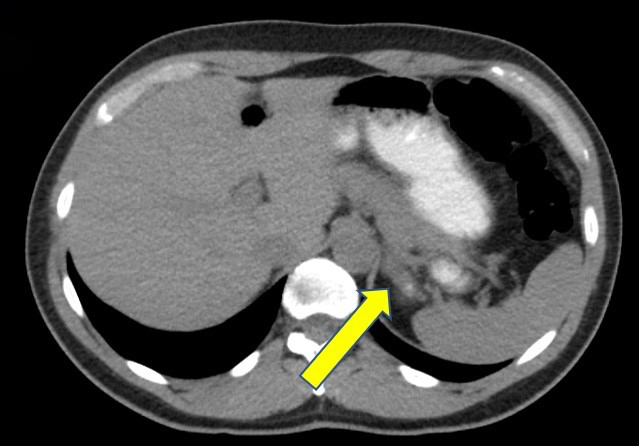
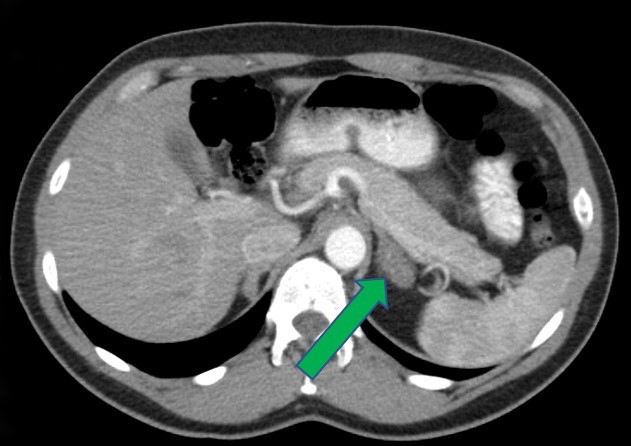
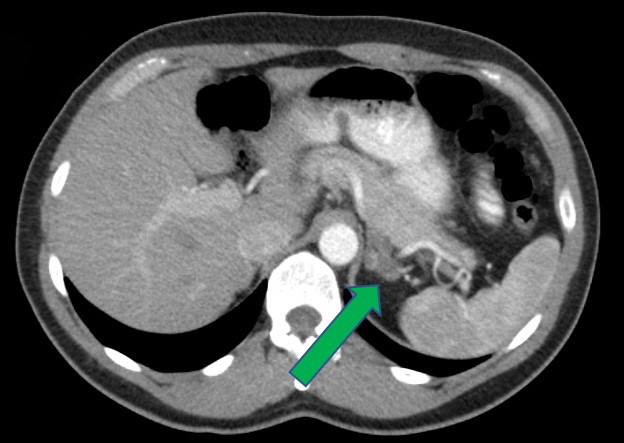

CT of left adrenal mass
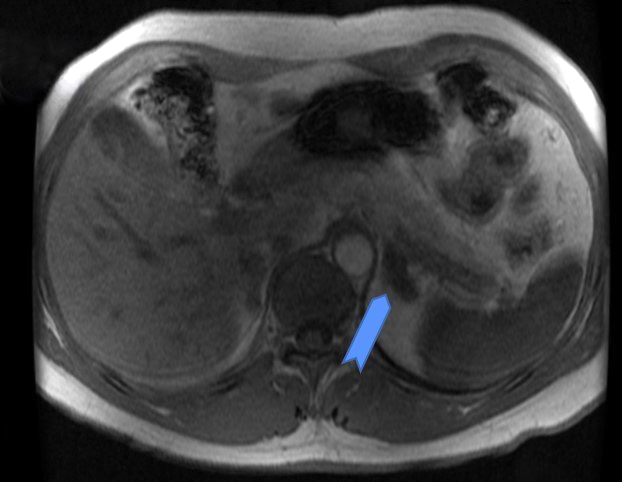


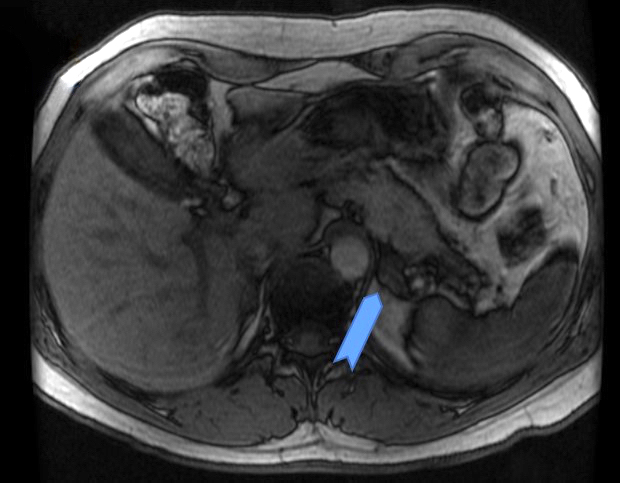
MRI of left adrenal mass
Prognostic factors
- Favorable prognosis, with no reported cases of recurrence following excision
Case reports
- 26 year old man with a large lesion preoperatively diagnosed as hepatic echinococcal cyst (Int J Surg 2008;6:485)
- 30 year old woman with right sided mass noted incidentally on ultrasound (Rare Tumors 2016;8:6506)
- 40 year old man with asymptomatic right sided mass noted incidentally on MRI (BMJ Case Rep 2015;2015:bcr2015211147)
- 54 year old man with renal calculi and incidental adrenal mass associated with elevated urinary homovanillic acid (Urology 2005;65:175)
Treatment
- Complete surgical resection
Gross description
- 0.5 - 19 cm, median 3.8 cm (Front Endocrinol (Lausanne) 2021;12:692553)
- Firm to soft solid but reports of solid cystic and entirely cystic tumors (Adv Anat Pathol 2009;16:424)
Gross images
Contributed by Debra L. Zynger, M.D.

Ill defined spongy lesion
Images hosted on other servers:

White solid and cystic surface

Cystic surface

Cystic spongy surface

Solid gray surface
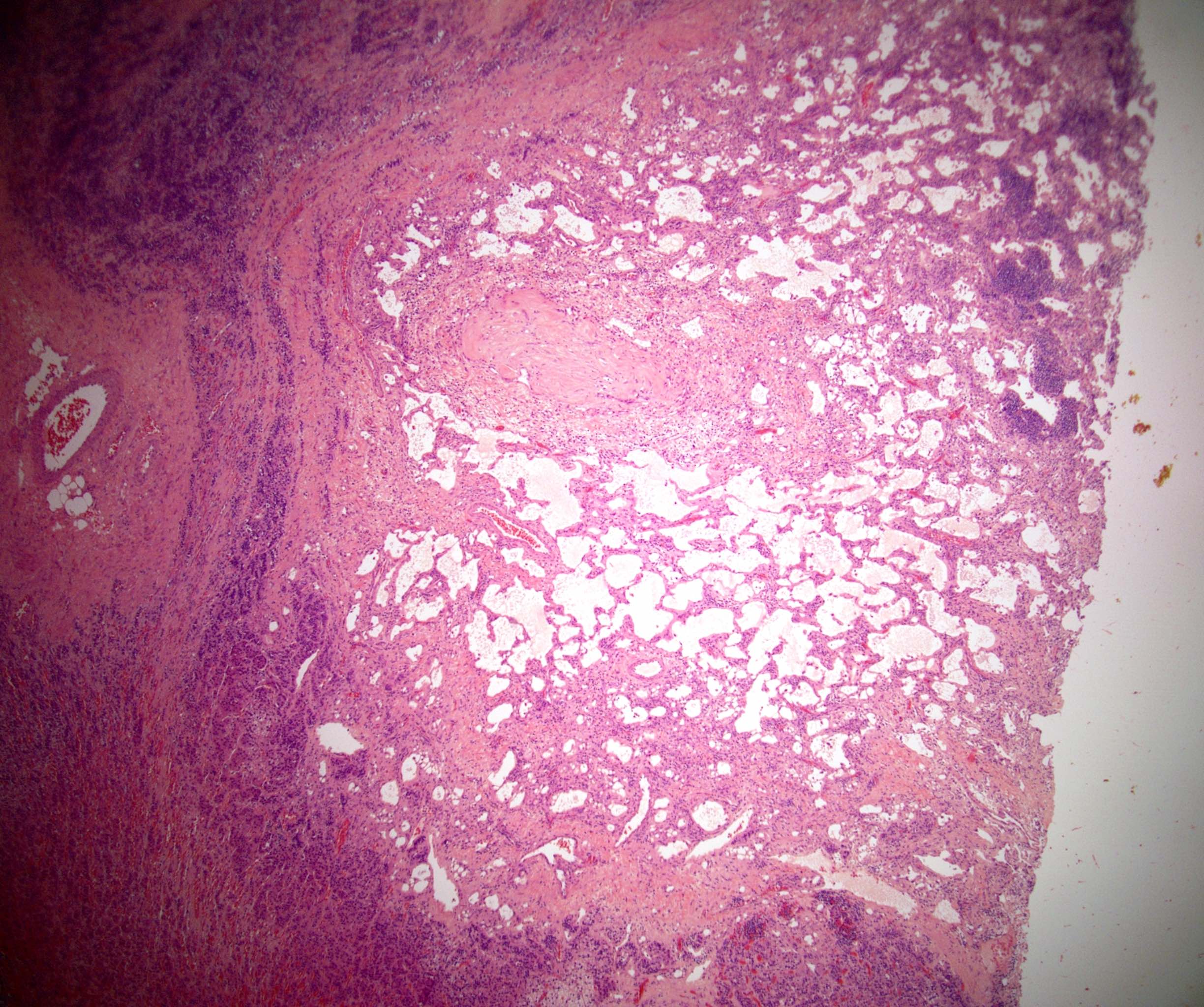
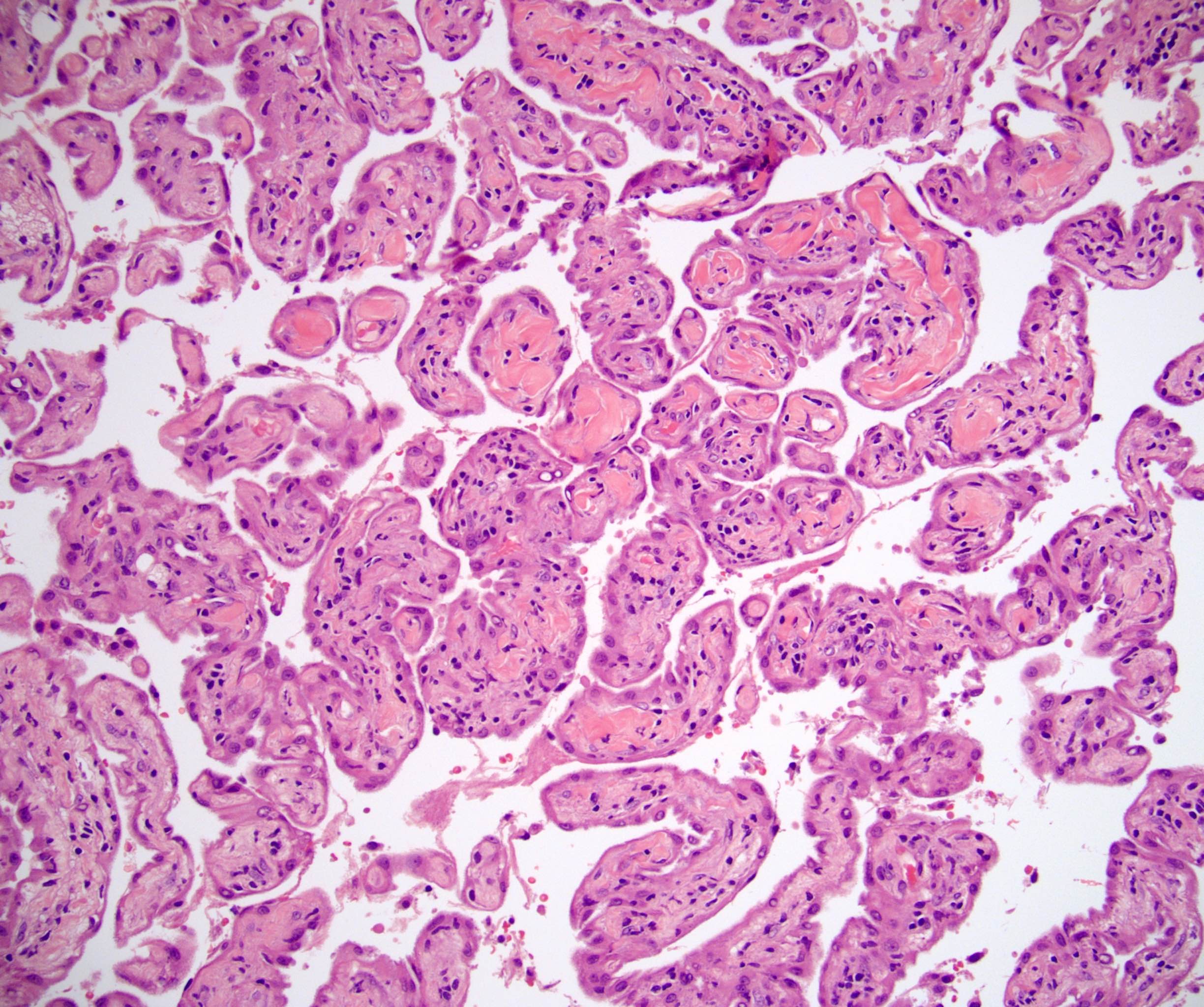
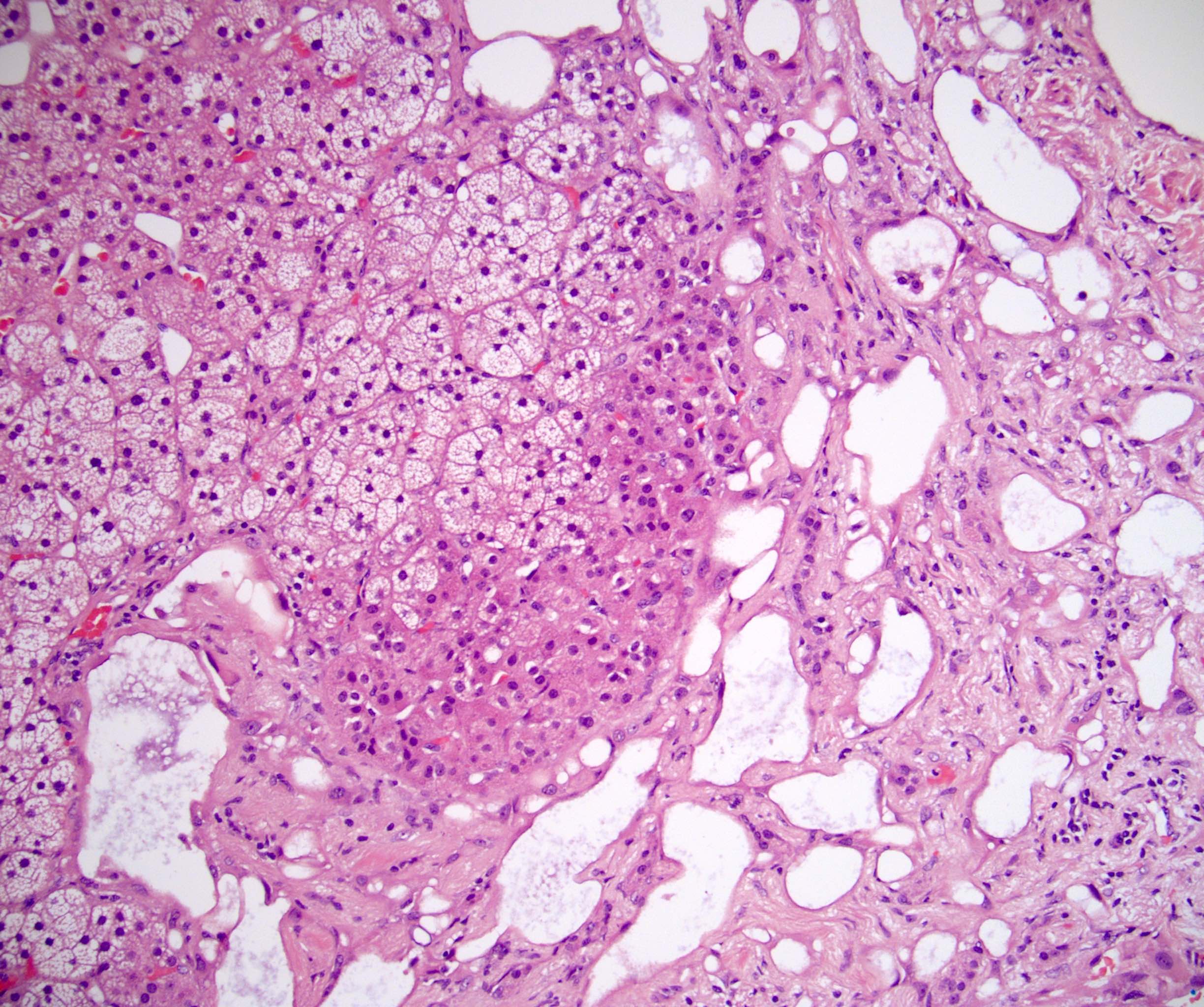
Microscopic (histologic) description
- Well circumscribed to infiltrative into surrounding cortex and medulla
- Can infiltrate into periadrenal adipose
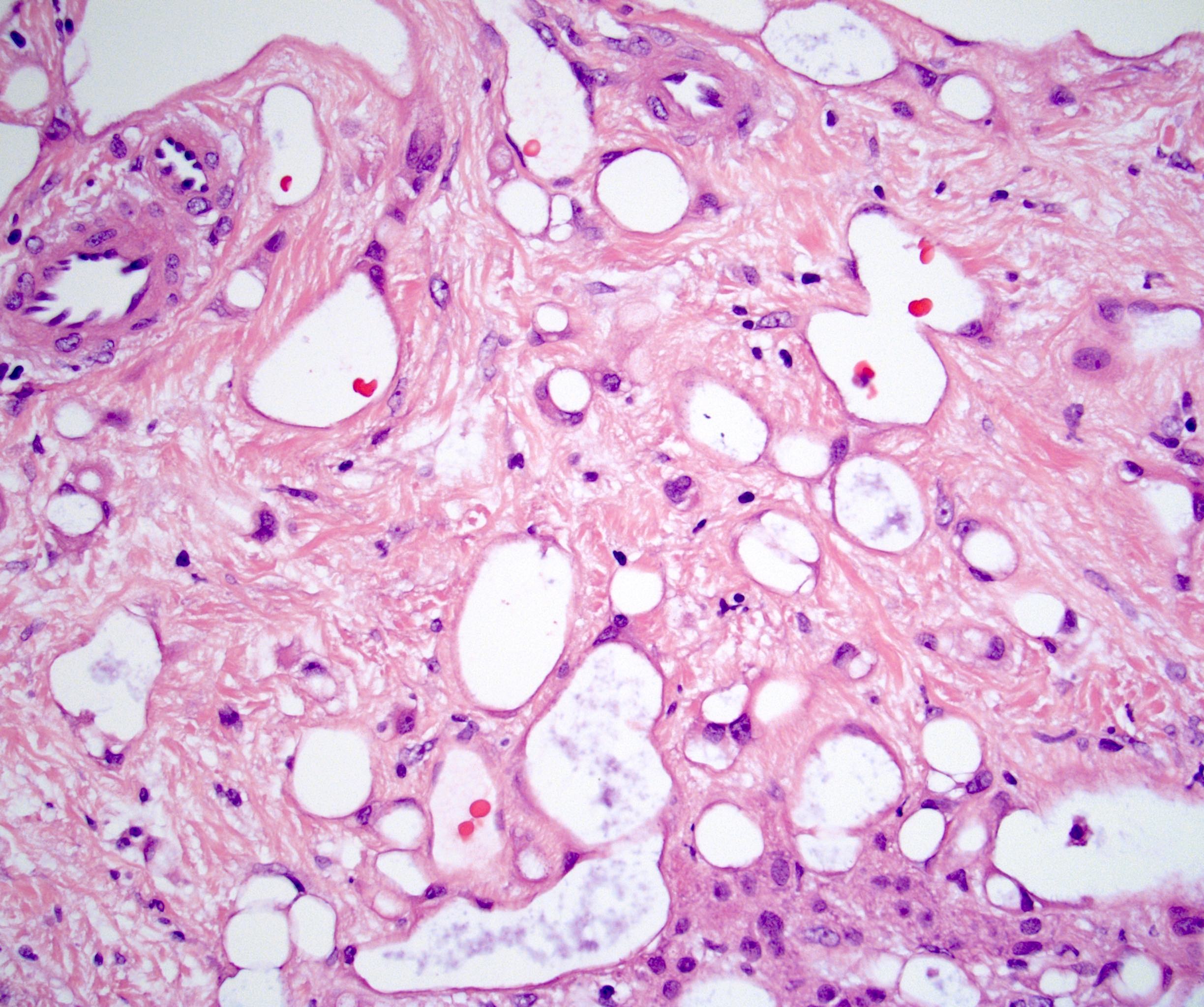
- Growth patterns include microcysts, tubules, macrocysts / cavernous and pseudovascular with papillary and anastomosing structures lined by endothelial-like cells (Adv Anat Pathol 2009;16:424)
- Cells are flattened to hobnailed and bland with no appreciable mitoses
- Lymphoid aggregates and interspersed lymphocytes are frequently present
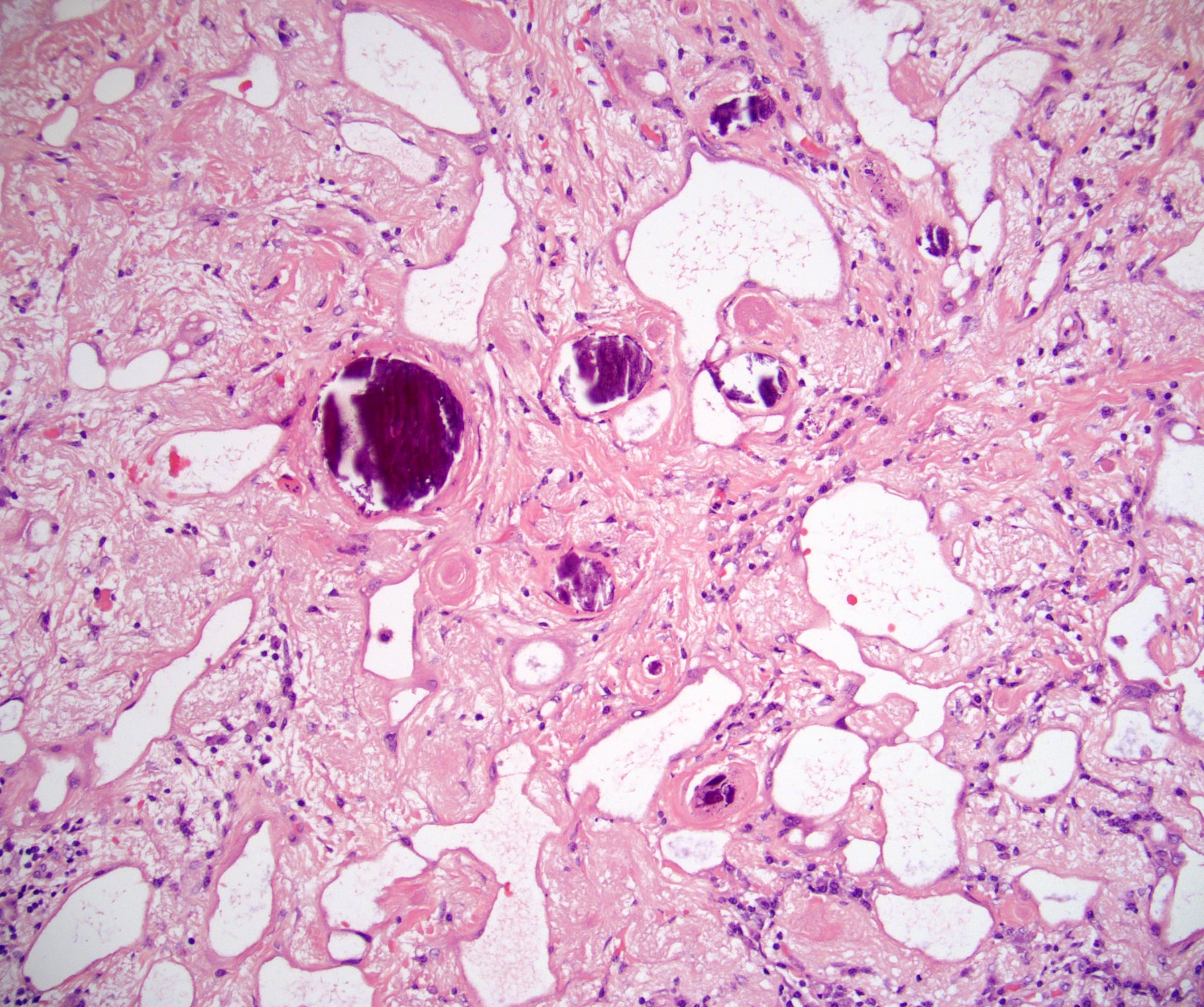
- Dystrophic calcifications are frequent
- Areas with abundant fine calcifications can have an empty, vacuolated appearance
- Surrounding fibrosis may be seen
Microscopic (histologic) images
Contributed by Debra L. Zynger, M.D.
Cystic lesion
Anastomosing channels
Microcysts
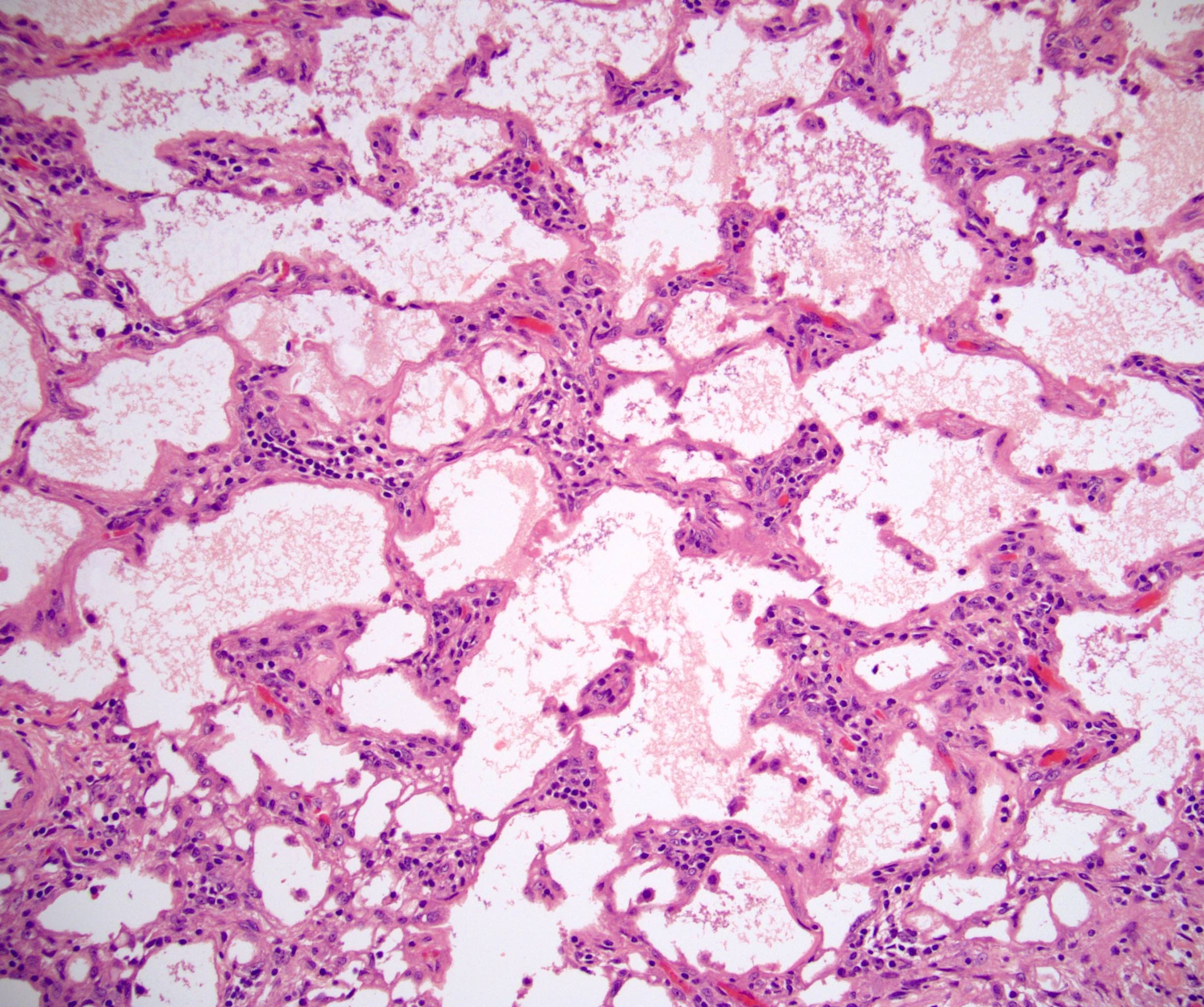
Delicate septae
Tubules and signet rings
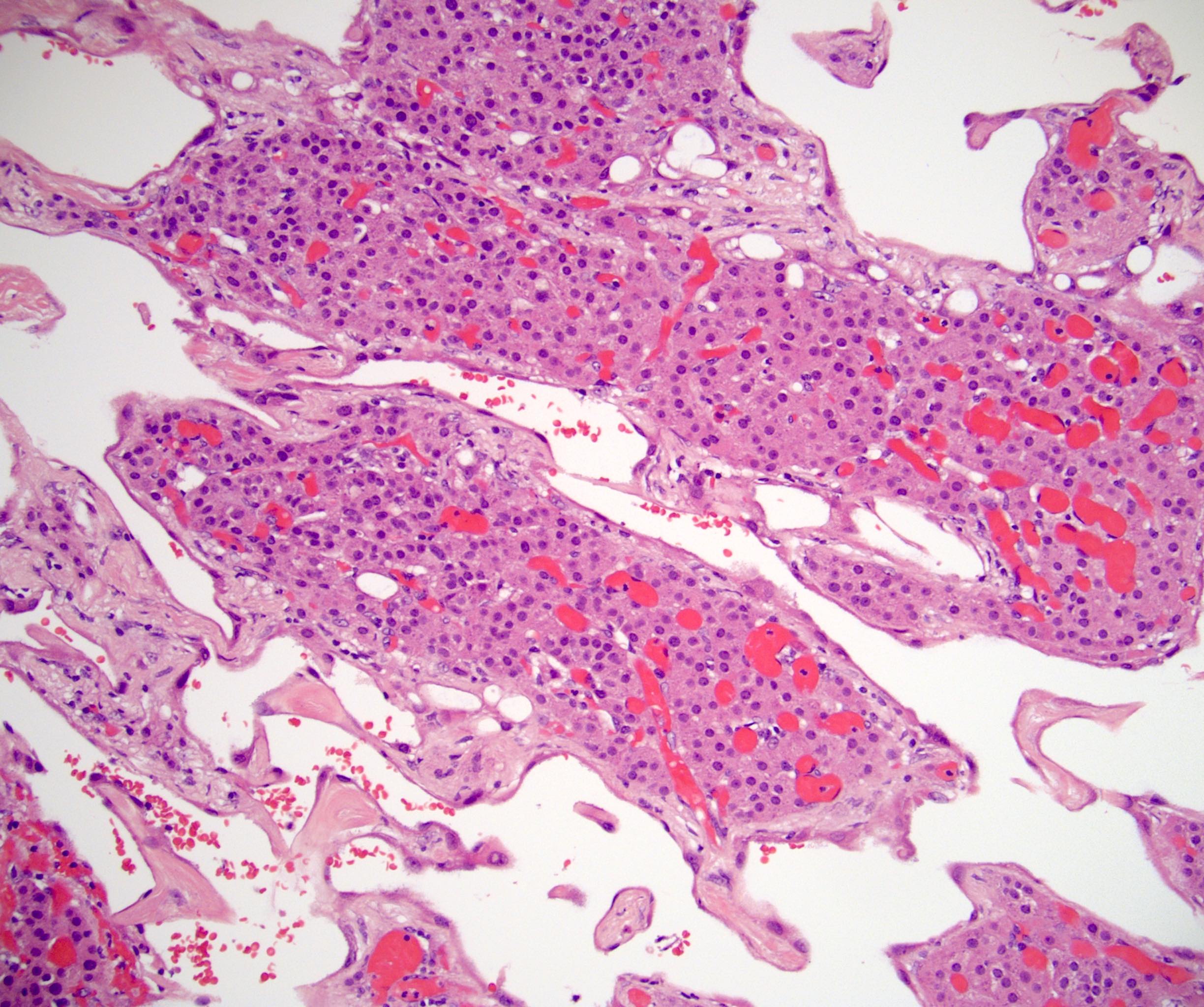
Entrapped cortex
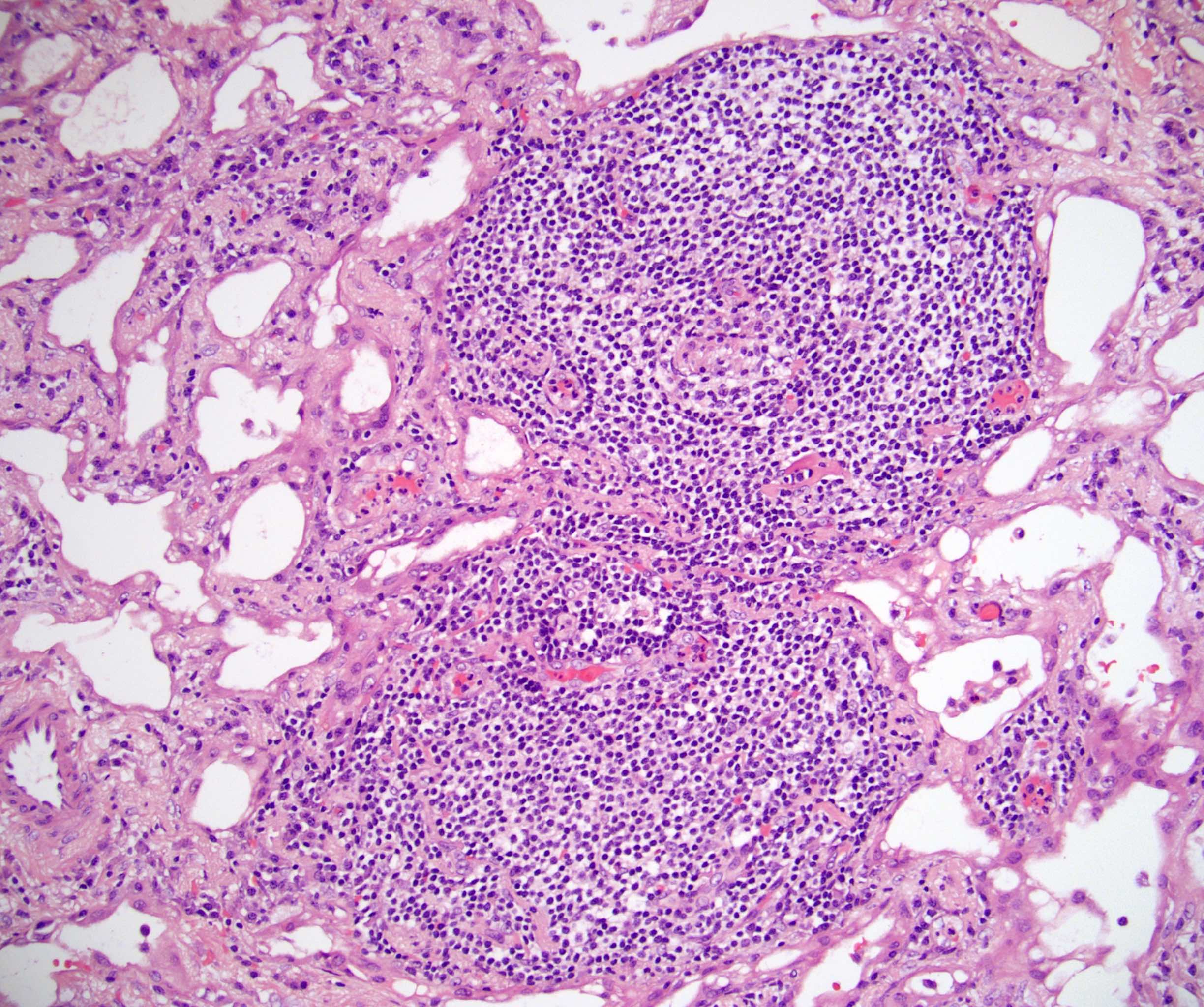
Lymphoid aggregates
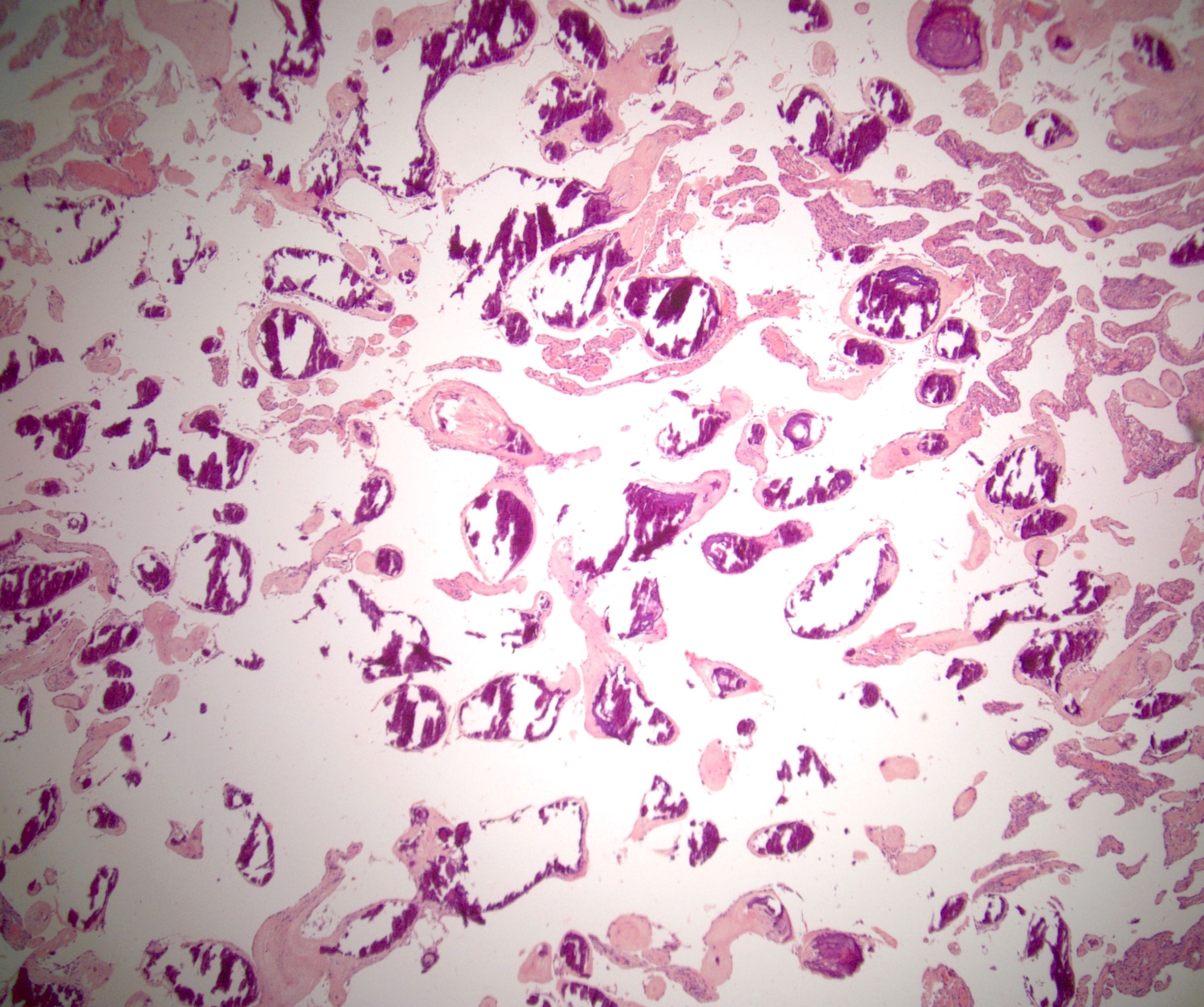
Calcification
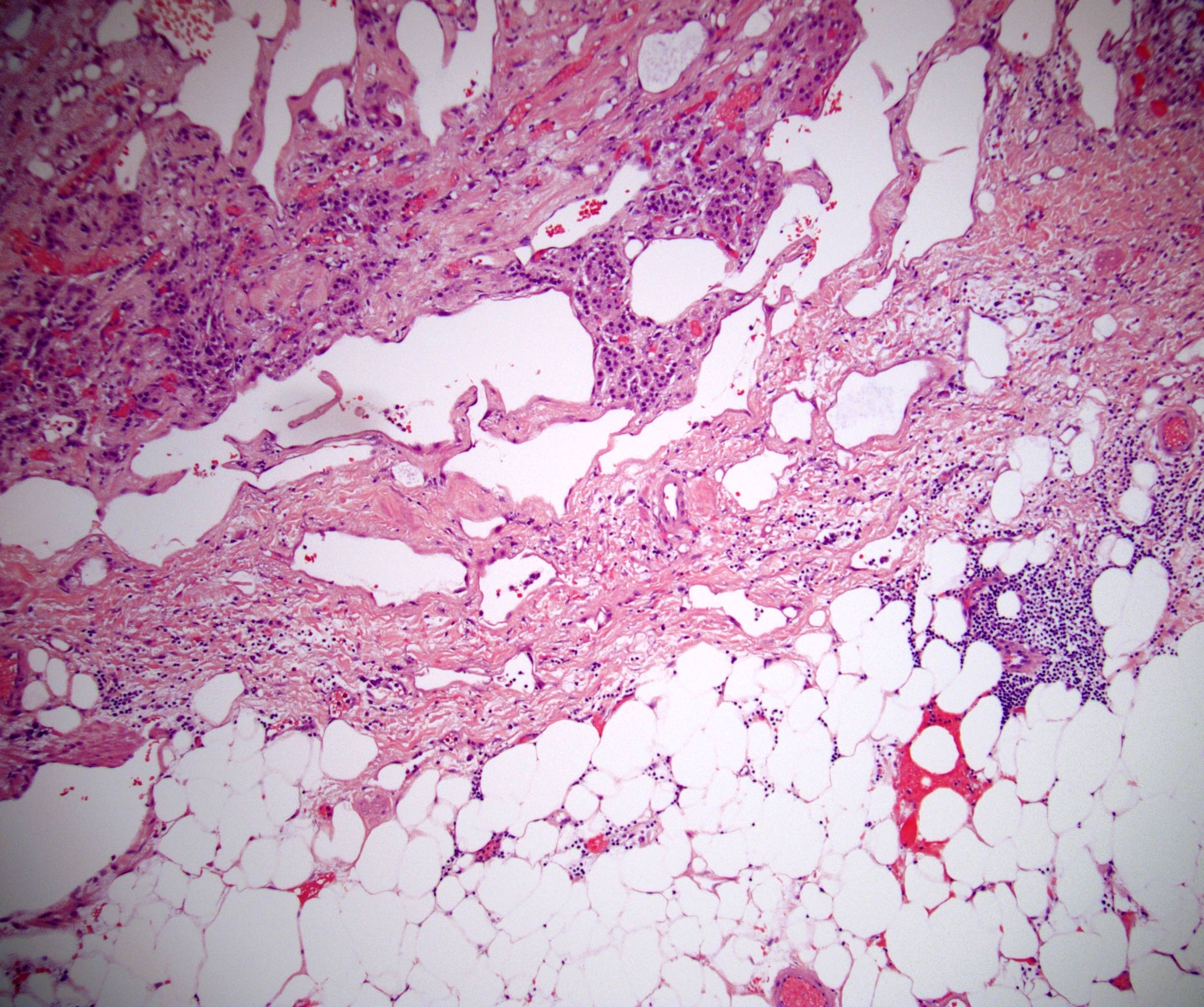
Infiltrative
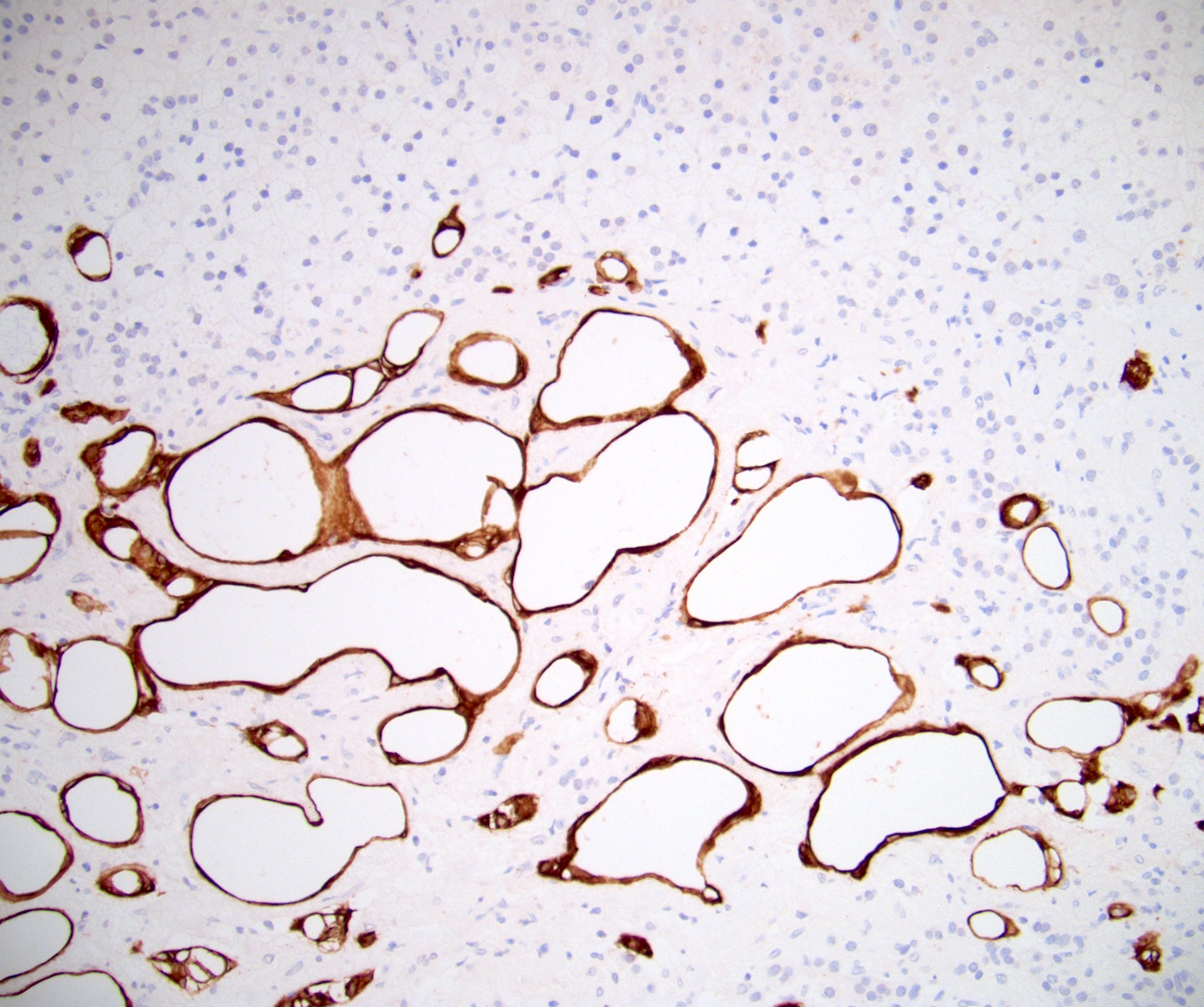
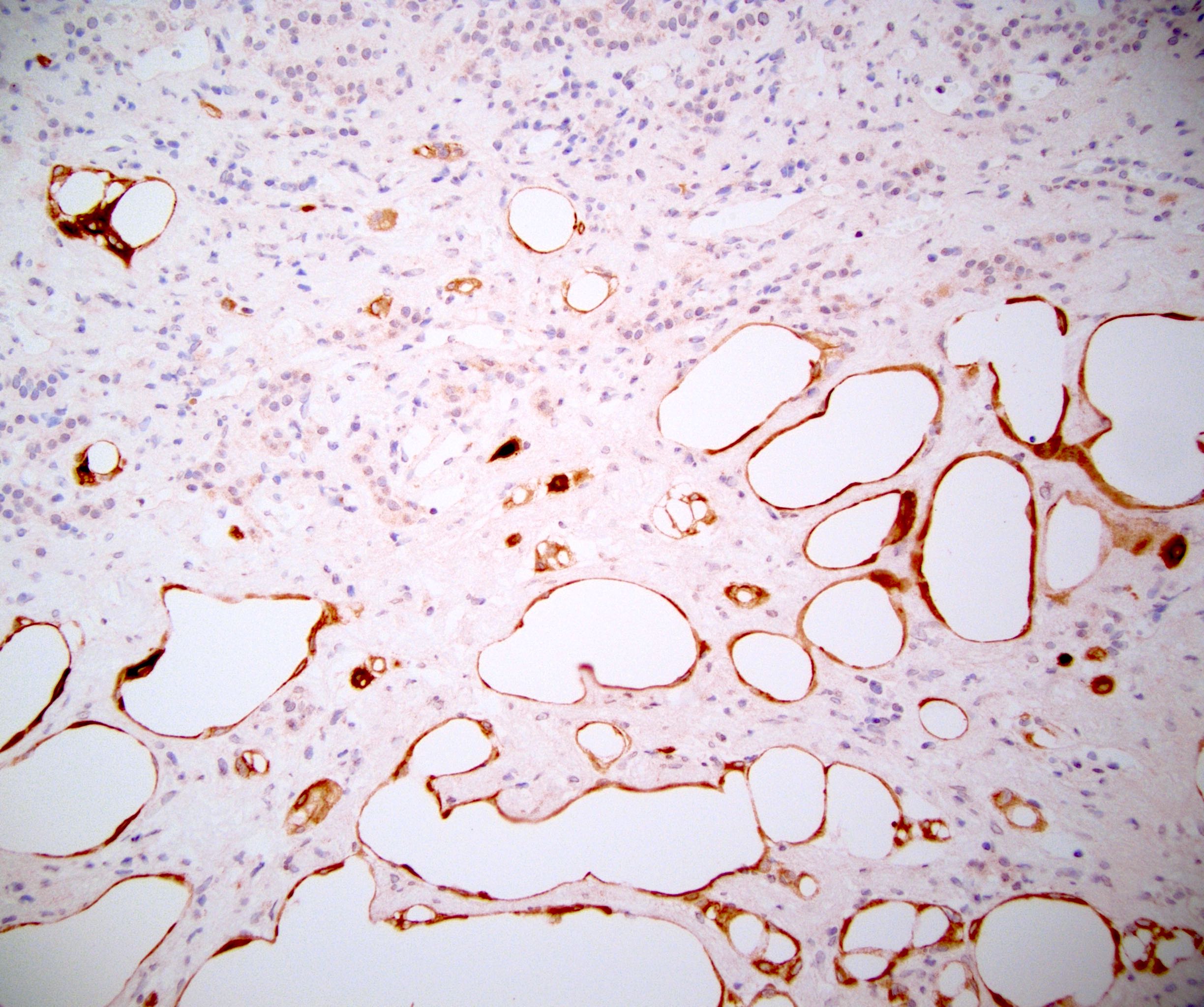
CK7
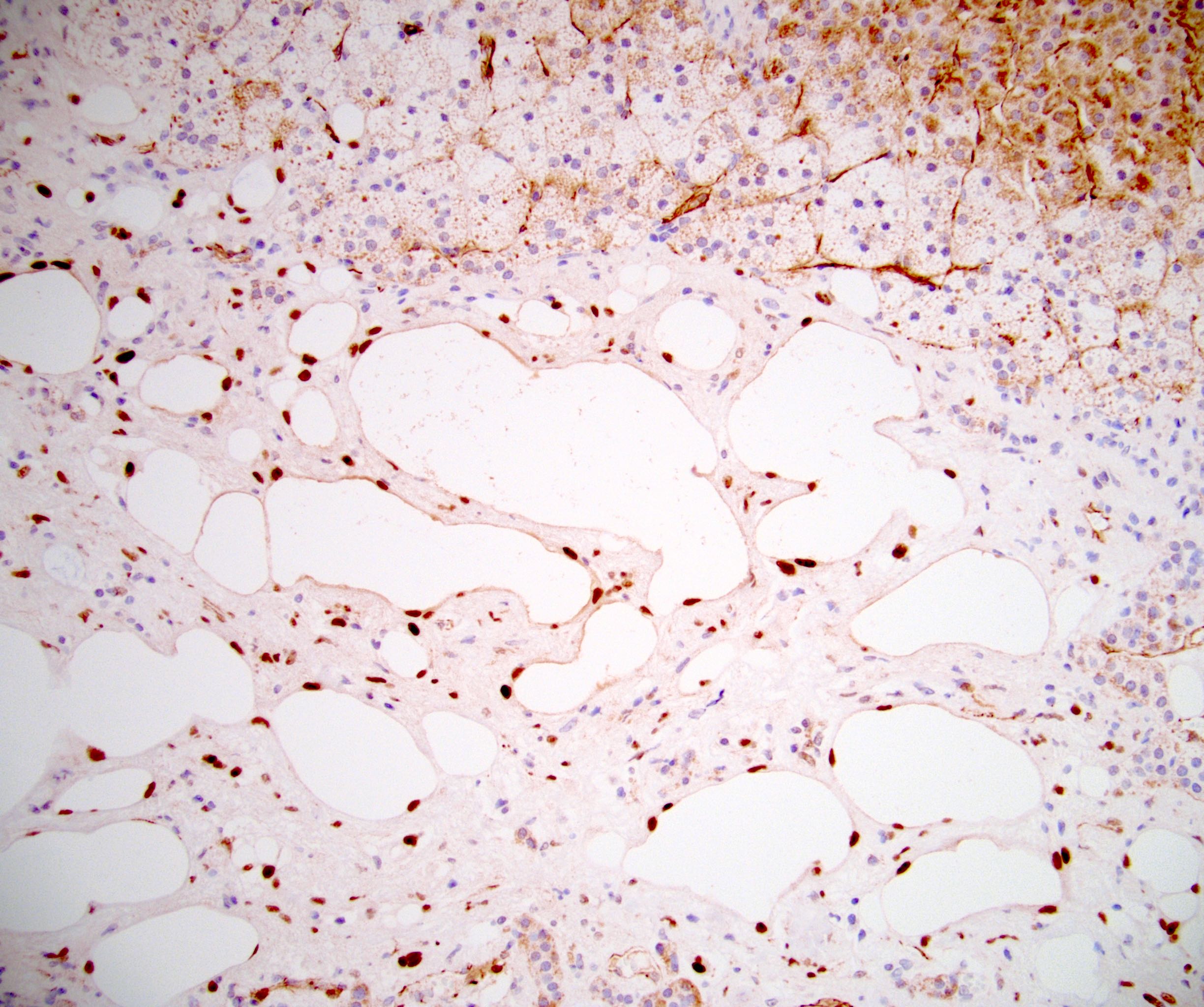
WT1
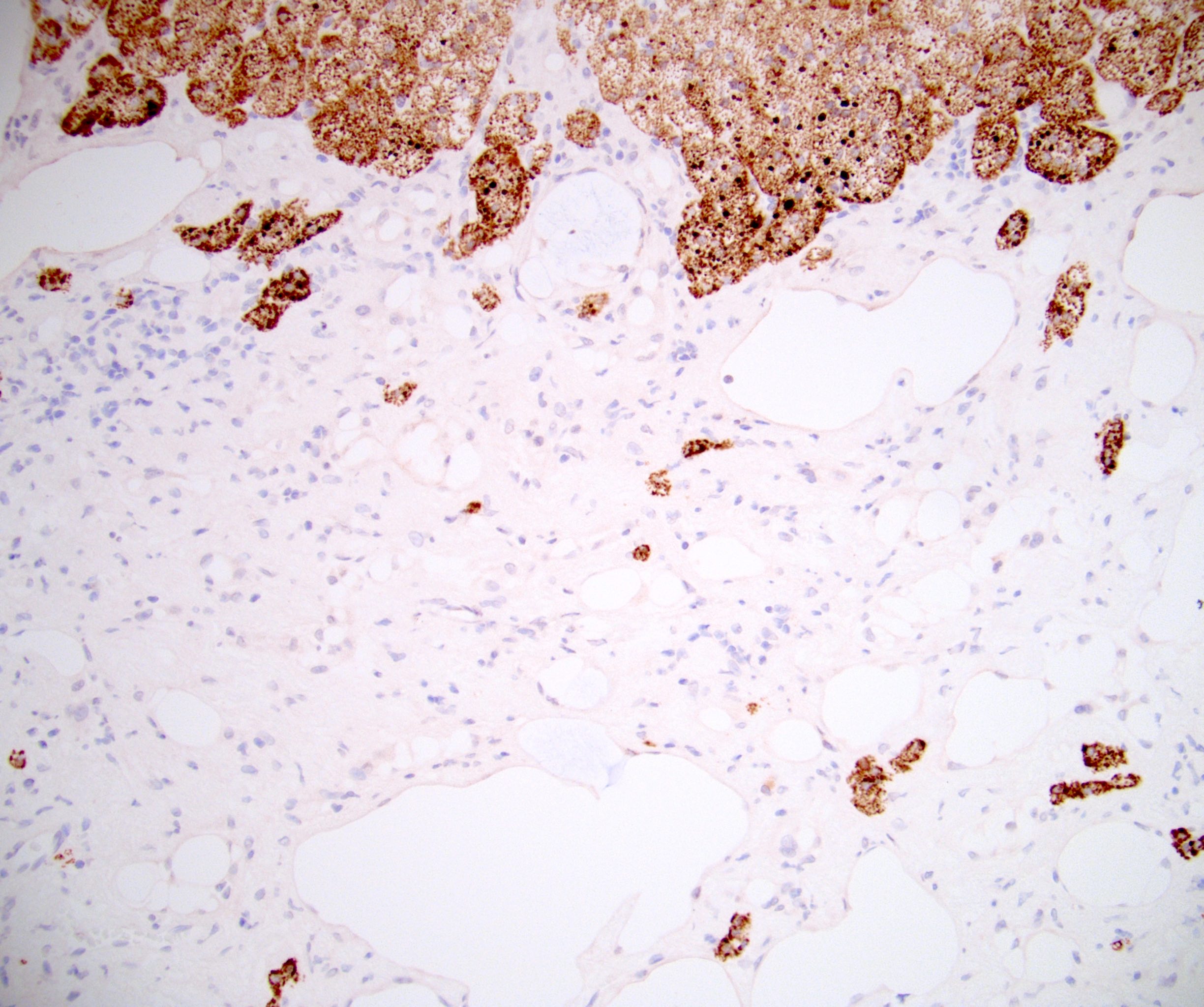
MelanA
Positive stains
Negative stains
Electron microscopy description
- Coelomic type microvilli in all examined cases
- Well formed desmosomes noted in several cases (Adv Anat Pathol 2009;16:424)
Sample pathology report
- Right adrenal gland, robotic adrenalectomy:
- Adenomatoid tumor, 4.8 cm
- Surgical margin, negative for tumor
Differential diagnosis
- Endothelial (vascular) cyst:
- Lymphangioma:
- Exceptionally rare in the adrenal gland
- Most incorrectly classified and are actually adenomatoid tumor (Lack: Tumors of the Adrenal Glands and Extraadrenal Paraganglia - AFIP Atlas of Tumor Pathology Series 4, Volume 8, 2007)
- Positive: CD31, CD34, D2-40
- Negative: AE1 / AE3, CK7, CK5/6, calretinin
- Hemangioma:
- Metastatic adenocarcinoma (particularly signet ring carcinoma):
- History is critical
- Atypia and mitotic activity are present
- Negative: CK5/6, WT1, calretinin
- Adrenal cortical adenoma (with cystic change):
- Myelolipoma:
- Adipose and myeloid elements are part of the lesion
- Lacks epithelial lined microcysts and tubules
- Negative: AE1 / AE3, CK7, CK5/6, calretinin
- Angiosarcoma:
Board review style question #1
A 42 year old man presents for evaluation of right renal stones and is incidentally found to have a 4 cm mass in the left adrenal gland. Laboratory studies are within normal limits and he reports no symptoms other than right flank pain consistent with his known diagnosis. Adrenalectomy is performed and the pathology report subsequently confirms adenomatoid tumor of the adrenal gland (shown above). Positivity for which of the following immunostains (shown above) likely confirmed the diagnosis?
- CD31
- CD34
- CK5/6
- Inhibin
- MelanA
Board review style answer #1
C. CK5/6. Adenomatoid tumor is of mesothelial origin and as such expresses CK5/6. Adrenal cortical lesions express MelanA and inhibin, while vascular lesions express CD31 and CD34.
Comment Here
Reference: Adenomatoid tumor
Comment Here
Reference: Adenomatoid tumor
