

Major / minor / bidirectional incompatibility
| O | A | B | AB | ||
| O | Compatible | Major | Major | Major | |
| A | Minor | Compatible | Bidirectional | Major | |
| B | Minor | Bidirectional | Compatible | Major | |
| AB | Minor | Minor | Minor | Compatible | |

Category definitions for therapeutic apheresis
| Category | Description |
| I | Apheresis is accepted as first line therapy, either as a primary standalone treatment or in conjunction with treatment modalities |
| II | Apheresis is accepted as second line treatment, either standalone or in conjunction with other treatment modalities |
| III | Apheresis decision should be individualized; the optimum role of apheresis is not established |
| IV | Disorders for which apheresis is ineffective or harmful based on the published data |
Grading recommendations and evidence for therapeutic apheresis
| Description | Methodological quality of supporting evidence | Implications | |
| Grade 1A | Strong recommendation, high quality evidence | Randomized controlled trials without important limitations or overwhelming evidence from observational studies | Strong recommendation; can apply to most patients in most circumstances without reservation |
| Grade 1B | Strong recommendation, moderate quality evidence | Randomized controlled trials with important limitations (inconsistent results, methodological flaws, indirect or imprecise) or exceptionally strong evidence from observational studies | Strong recommendation; can apply to most patients in most circumstances without reservation |
| Grade 1C | Strong recommendation, low quality or very low quality evidence | Observational studies or case series | Strong recommendation but may change when higher quality evidence becomes available |
| Grade 2A | Weak recommendation, high quality evidence | Randomized controlled trials without important limitations or overwhelming evidence from observational studies | Weak recommendation; best action may differ depending on circumstances or patients' or societal values |
| Grade 2B | Weak recommendation, moderate quality evidence | Randomized controlled trials with important limitations (inconsistent results, methodological flaws, indirect or imprecise) or exceptionally strong evidence from observational studies | Weak recommendation; best action may differ depending on circumstances or patients' or societal values |
| Grade 2C | Weak recommendation, low quality or very low quality evidence | Observational studies or case series | Very weak recommendation; other alternatives may be equally reasonable |
- Reference: Curr Opin Hematol 2019;26:461
Contributed by Chinelo P. Onyenekwu, M.D. and Melissa R. George, D.O.
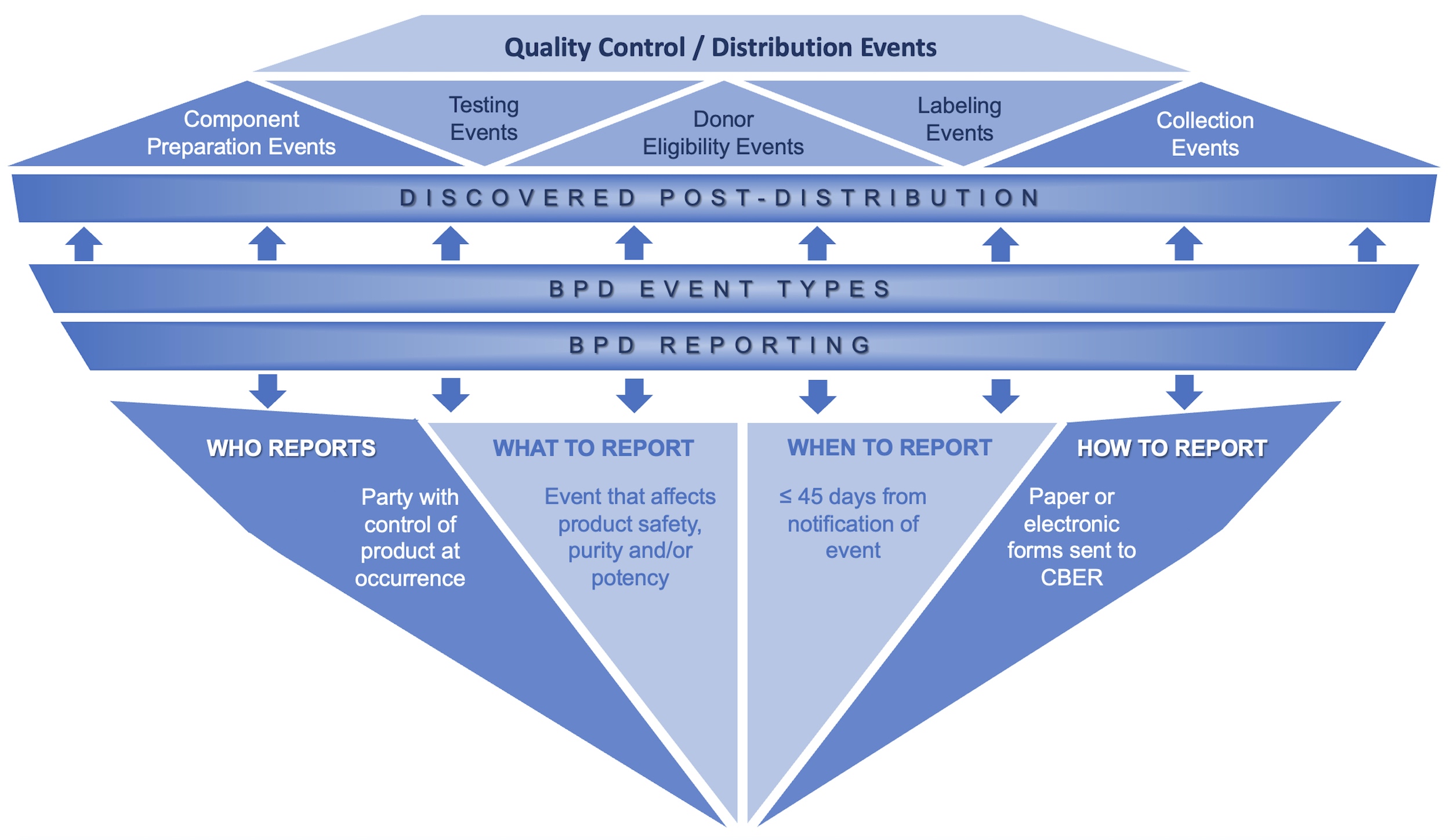
Reporting overview

Reporting responsibility

Reporting process

Labeling events

Quality control / distribution events
Images hosted on other servers:

Chimeric antigen receptor modified
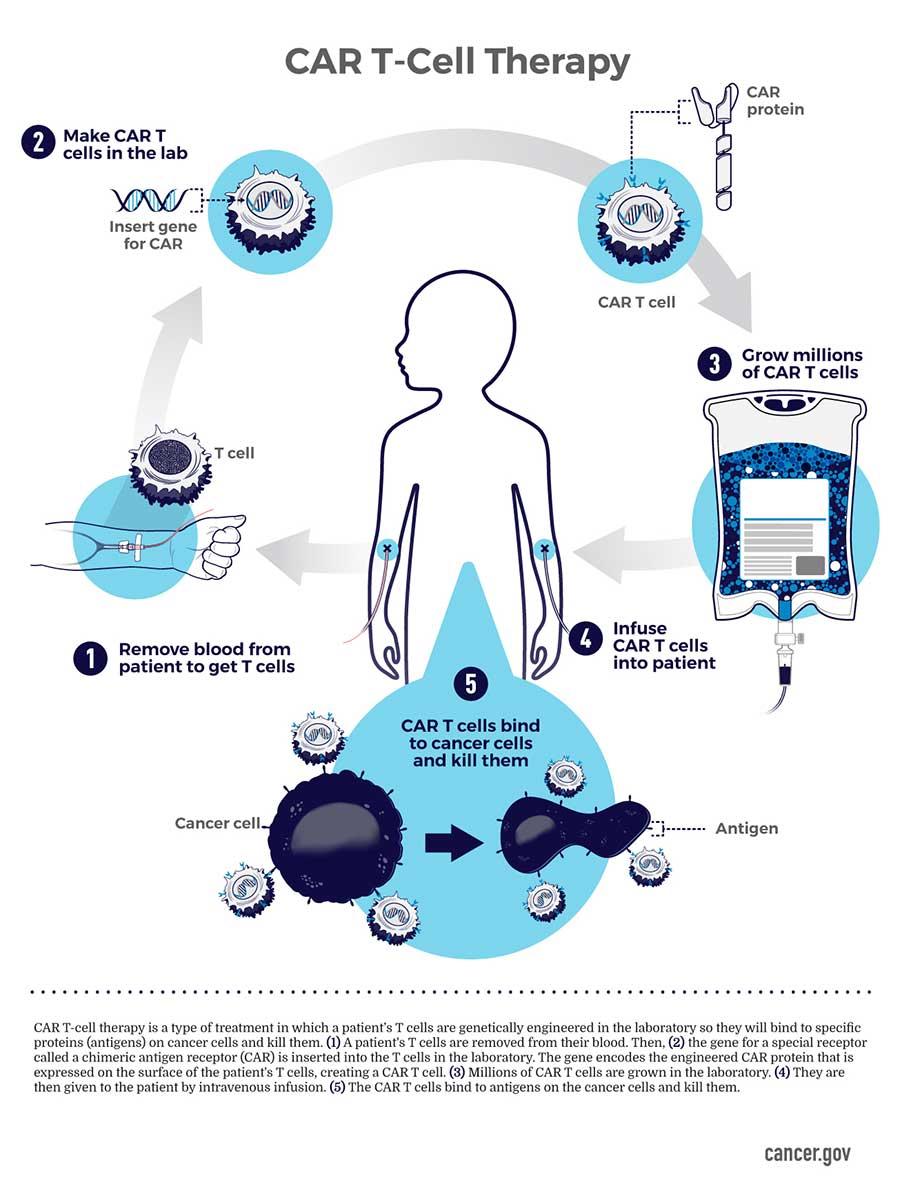
Engineering immune cells

Multiple gene or nongene editing
Table 1: Infusion toxicity by etiology
| DMSO | Cytokines | RBC / hemoglobin | Plasma | Volume | Citrate | |
| Nausea / emesis | X | |||||
| Fever / chills | X | X | X | |||
| Cough | X | X | ||||
| Flushing | X | X | ||||
| Shortness of breath, hypoxia | X | X | X | X | X | |
| Hypotension | X | X | X | |||
| Hypertension | X | X | X | |||
| Bradycardia | X | X | ||||
| Arrythmia | X | X | X | X | ||
| Neurologic | X | X | X | |||
| Gastrointestinal pain | X | X | X |
Images hosted on other servers:
Negative and positive DAT reactions
Contributed by Evelyn M. Potochny, D.O. and Sarah Kesterson, M.D.

General steps in successful FACT accreditation process

FACT common standards categories
NHSN hemovigilance module adverse reaction codes, severity codes and imputability
| Case definition | Severity | Imputability |
| Definitive: the adverse reaction fulfills all of the case definition criteria | Nonsevere: medical intervention (e.g., symptomatic treatment) is required but there is minimal risk of permanent damage to the transfusion recipient | Definite: there is conclusive evidence that the reaction can be attributed to the transfusion |
| Probable: the adverse reaction meets some of the clinical signs and symptoms or radiologic, laboratory evidence or available information but does not meet all definitive case definition criteria | Severe: inpatient hospitalization or prolonged hospitalization is directly attributable to the transfusion reaction, persistent or significant disability or incapacity of the patient as a result of the reaction or a medical or surgical intervention is necessary to preclude permanent damage or impairment of a body function | Probable: there are other potential causes present that could explain the recipient's symptoms but transfusion is the most likely cause of the reaction |
| Possible: the reported clinical signs or symptoms, radiologic or laboratory evidence and available information are not sufficient to meet definitive or probable case definition criteria | Life threatening: major intervention was required after the transfusion reaction (e.g., vasopressors, intubation, transfer to intensive care) to prevent death | Possible: there are other potential causes that are most likely; however, transfusion cannot be ruled out |
| Death: the recipient died as a result of the transfusion reaction | Doubtful: there is evidence clearing in favor of a cause other than the transfusion but transfusion cannot be excluded | |
| Not determined: the severity of the adverse reaction is unknown or not stated | Ruled out: there is conclusive evidence beyond reasonable doubt of a cause other than the transfusion | |
| Not determined: the relationship between the reaction and transfusion is unknown or not stated |


Contributed by Melissa R. George, D.O. and Chinelo P. Onyenekwu, M.D.
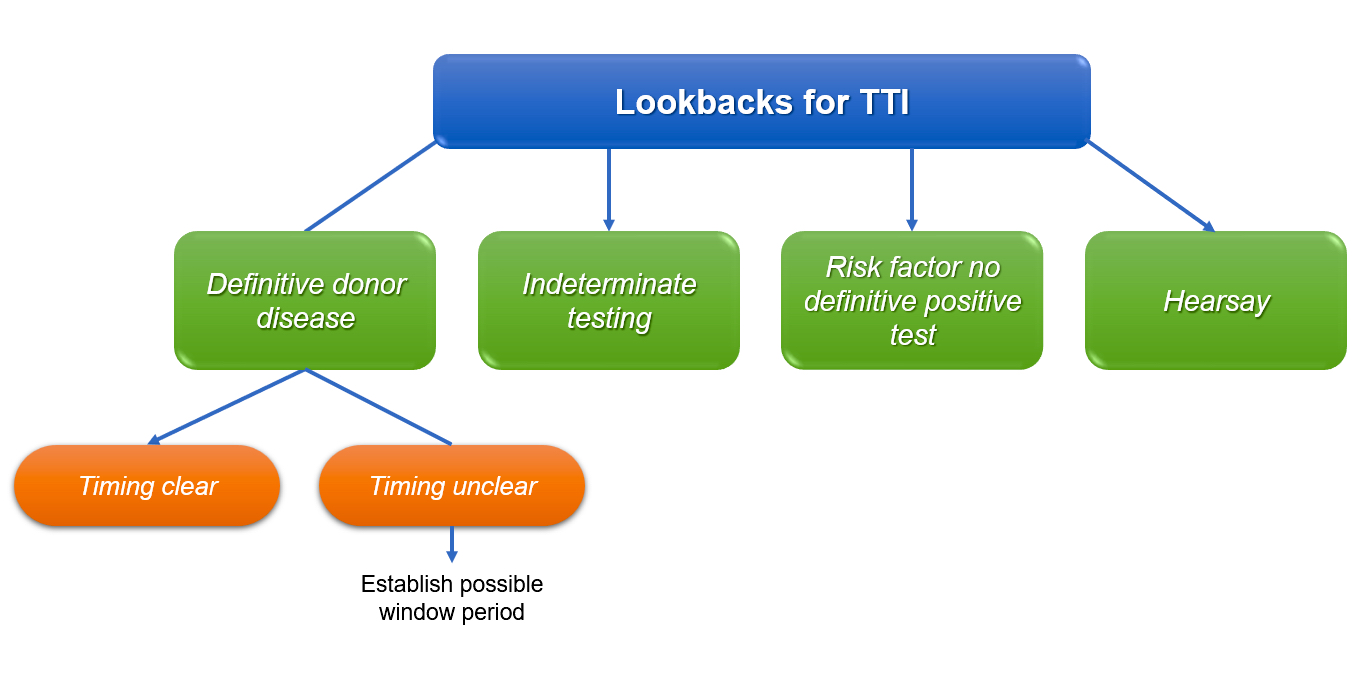
Lookbacks for TTI
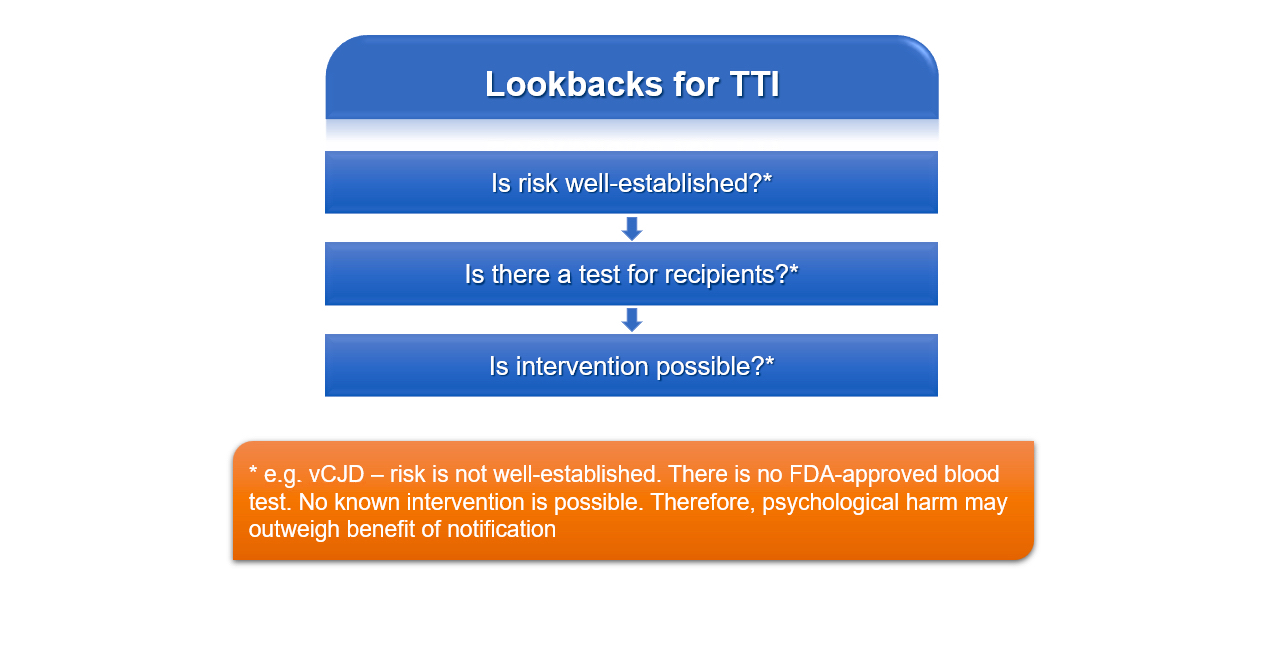
TTIs without approved tests
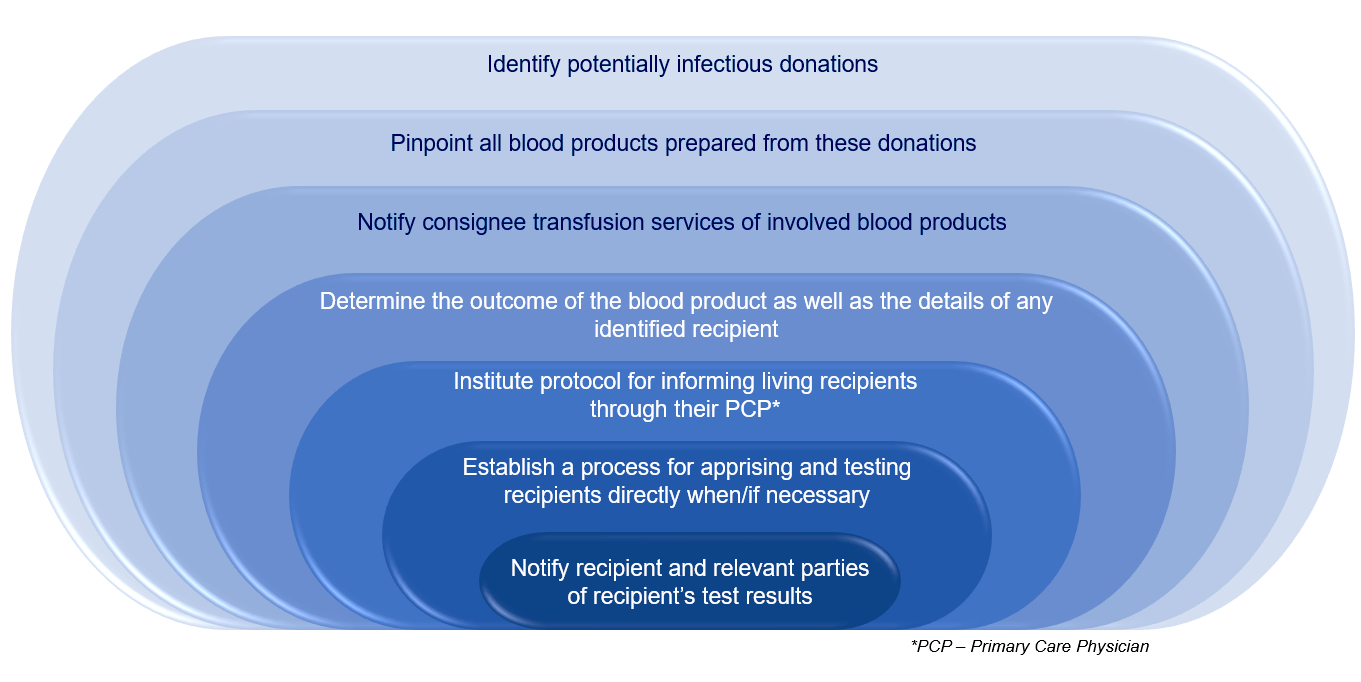
Steps in a lookback
Images hosted on other servers:

Lethal triad of trauma

Trauma induced coagulopathy
Contributed by Chinelo P. Onyenekwu, M.D.
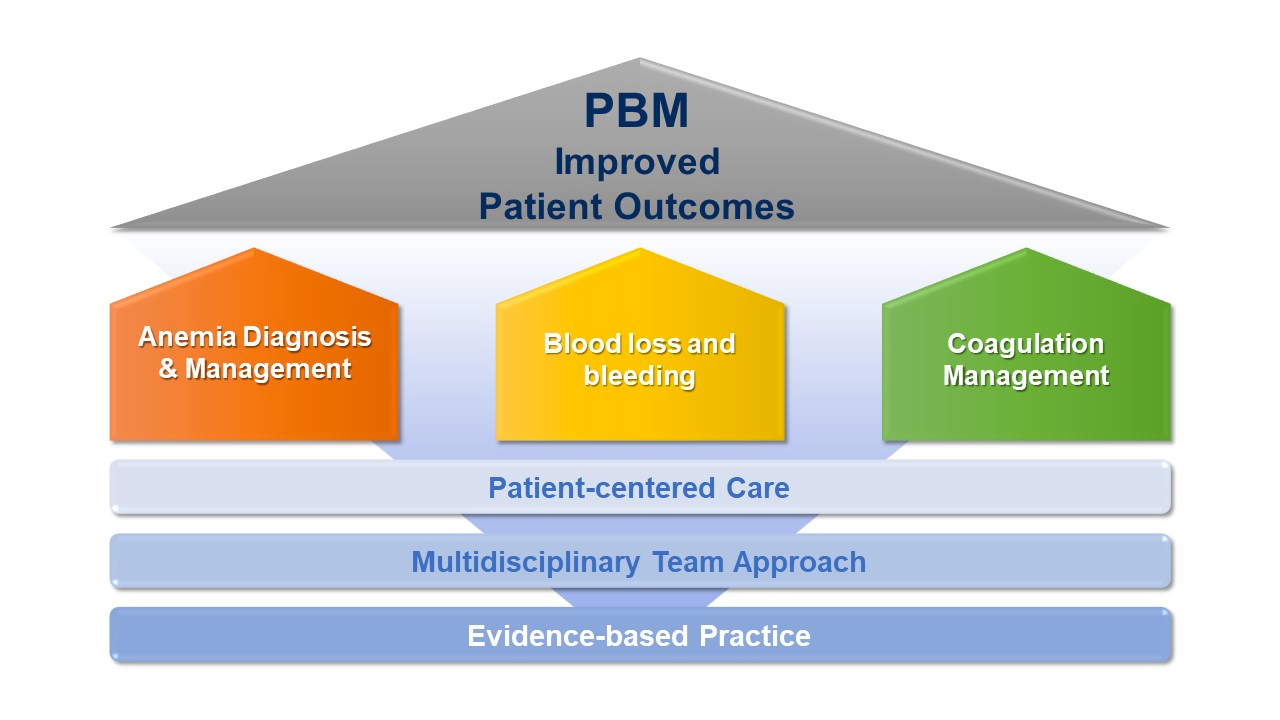
PBM toolbox
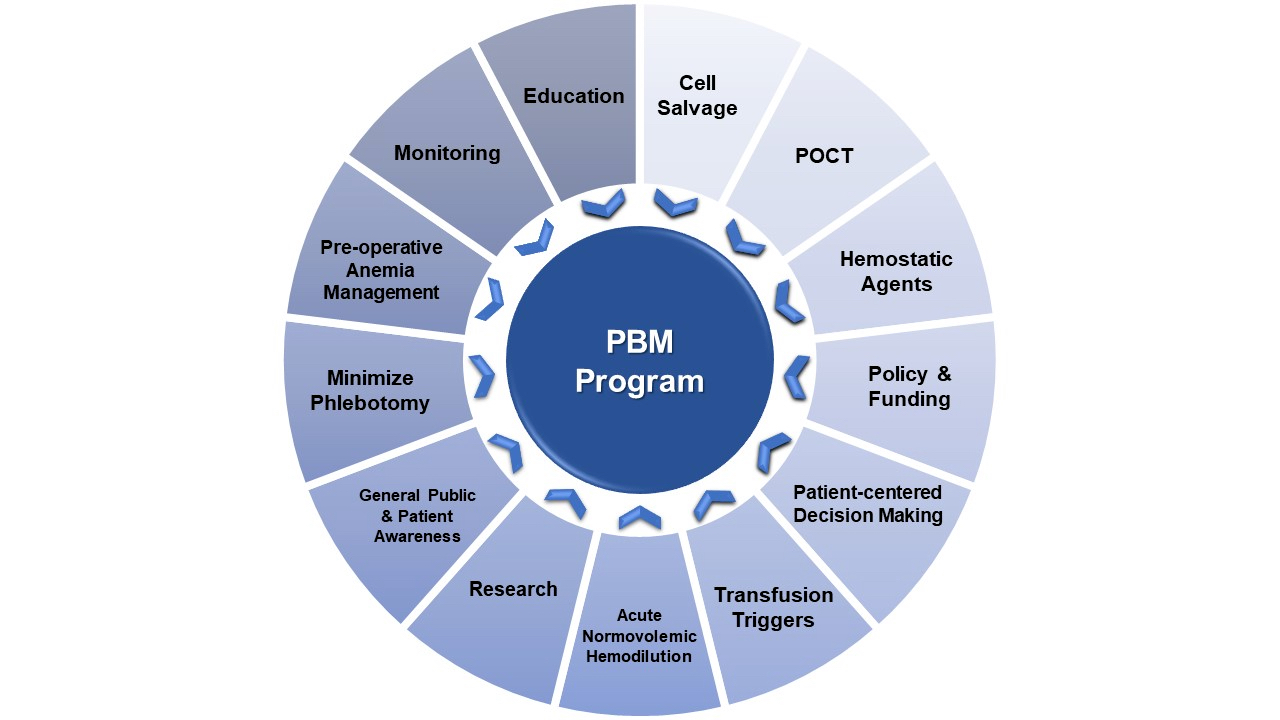
PBM program

Contributed by Yigit Baykara, M.D.

Serological
weak D
Contributed by Evelyn M. Potochny, D.O.
Positive Kleihauer-Betke test
Contributed by Patricia Tsang, M.D., M.B.A.
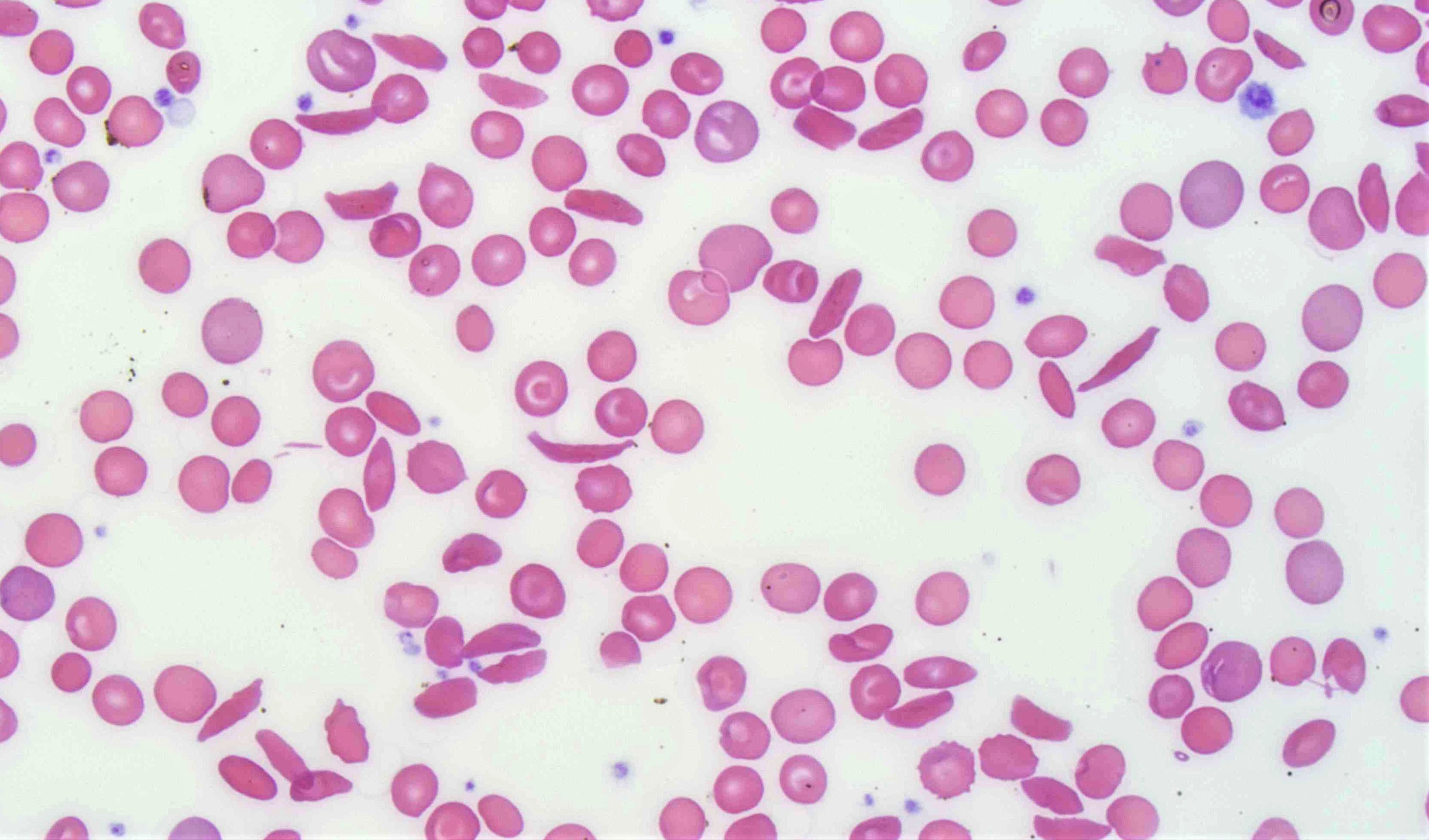
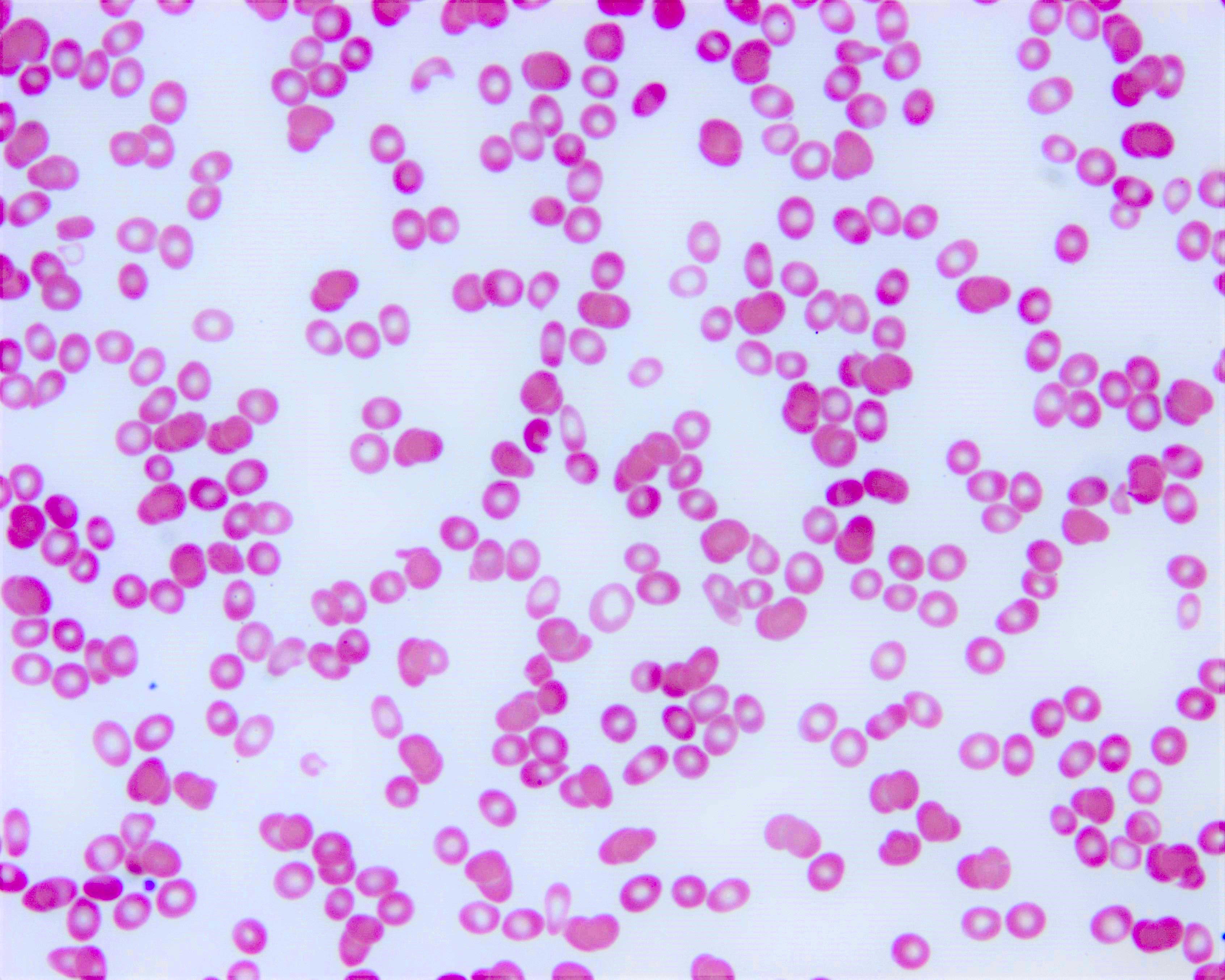
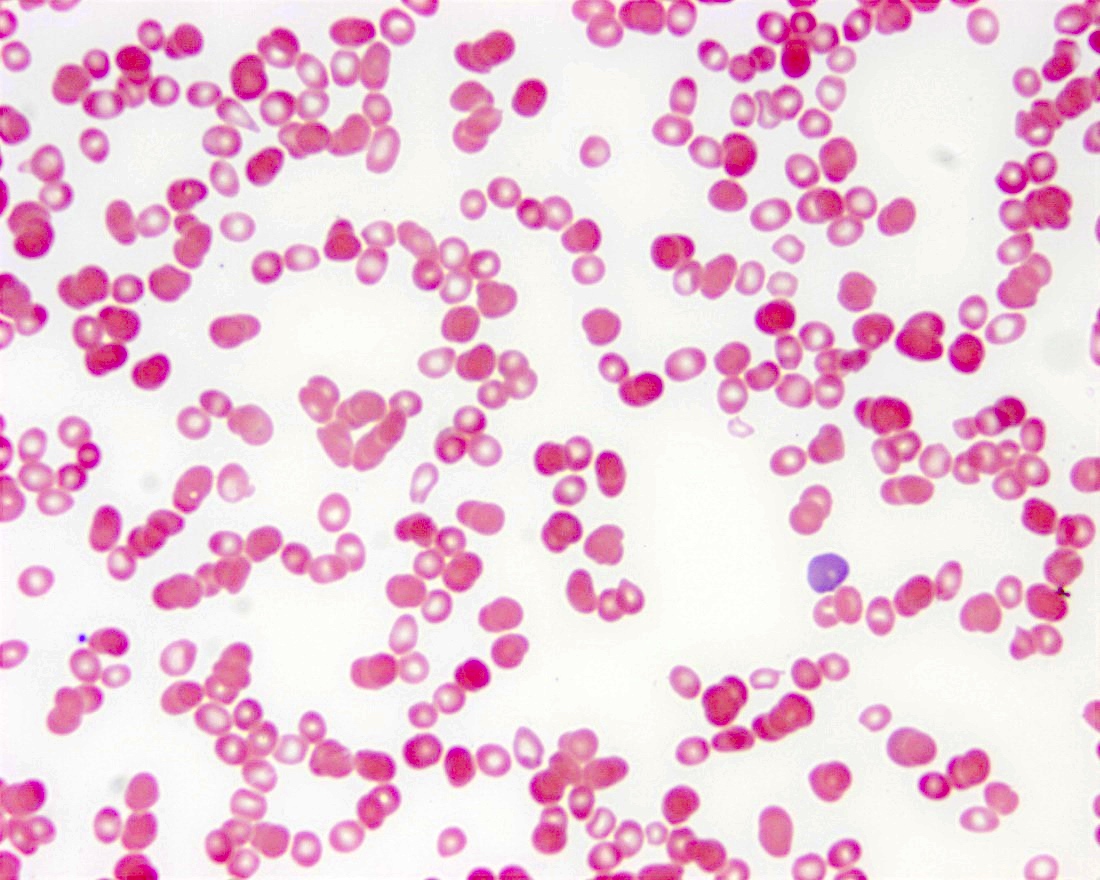
Sickle cell blood smear



Images hosted on other servers:

Pulmonary edema

AABB: 2021
AABB: 2021
Cohn: 2023
Cushing: 2020
Dunbar: 2020
Friedman: 2023
Harmening: 2018
Howard: 2016
Hughes: 2018
Katz Karp: 2020
Key: 2017
Kreuter: 2017
McCullough: 2016
McPherson: 2021
Quillen: 2016
Reid: 2012
Shaz: 2018
Simon: 2022
Talebi: 2016
Vassallo: 2021
Volod: 2023
Find related Pathology books: transfusion, lab medicine, management, hematopathology, other
