

Prostate gland and seminal vesicles
Prostatic urethra
Male urethral carcinoma
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: Male urethral carcinoma


Prostatic urethra
Male urethral carcinoma
Last staff update: 25 November 2024
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: Male urethral carcinoma

Table of Contents
Definition / general | Essential features | Epidemiology | Sites | Pathophysiology | Clinical features | Diagnosis | Radiology description | Prognostic factors | Case reports | Treatment | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Differential diagnosisCite this page: Chavez J, Zynger DL. OLD Male urethral carcinoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/oldtopics/prostatemaleurethracarcinoma.html. Accessed December 26th, 2024.
Definition / general
- Rare primary neoplasm of epithelial origin
- Secondary involvement by urothelial carcinoma of the bladder is much more common than primary (Eur Urol 2013;64:823)
Essential features
- Urethral carcinoma is usually due to secondary involvement
- Primary urethral carcinoma is rare and the most frequent histologic types are urothelial carcinoma, squamous cell carcinoma and adenocarcinoma (not otherwise specified, clear cell)
Epidemiology
- Primary tumor accounts for < 1% of all genitourinary malignancies (Eur Urol 2013;64:823, BJU Int 2014;114:25)
- More common in women than men (Hematol Oncol Clin North Am 2012;26:1291)
- In men, more common in African Americans (Urology 2006;68:1164)
- Urothelial carcinoma is the predominant histologic type (54 - 65%), followed by squamous cell carcinoma (16 - 22%) and adenocarcinoma (10 - 16%) (Urology 2006;68:1164)
- Secondary involvement of urethra post-cystectomy is seen in 3 - 4% of patients (Eur Urol 2013;64:823, Int J Surg 2015;13:148)
Sites
- Type depends on sex and location:
- Male urethra divided into 4 anatomic regions: prostatic, membranous, bulbous and penile
- Prostatic and membranous portions: most commonly urothelial carcinoma and associated with bladder tumors (Semin Diagn Pathol 2015;32:238)
- Bulbous and membranous portions: most commonly squamous cell carcinoma and rarely associated with bladder tumors (Semin Diagn Pathol 2015;32:238)
- Adenocarcinoma presents in both sexes; may originate anywhere along the urethra
- Most commonly associated with diverticula and prostatic adenocarcinoma in men (Bostwick: Urologic Surgical Pathology, 3rd Edition, 2014)
- May arise from urothelial metaplastic mucosa or from periurethral glands in both sexes
- Clear cell adenocarcinoma is found predominantly in women and has a particular association with urethral diverticulum (J Urol 2008;180:2463, Int J Surg Oncol 2015;2015:790235)
- Indistinguishable from clear cell adenocarcinoma of the genital tract
- Male urethra divided into 4 anatomic regions: prostatic, membranous, bulbous and penile
Pathophysiology
- Predisposing factors include:
- Iatrogenic chronic irritation (chronic catheterization / urethroplasty) (Eur Urol 2013;64:823)
- Urethral strictures (BJU Int 2014;114:25)
- Radiation therapy (BJU Int 2008;101:964)
- Chronic urethritis secondary to sexually transmitted diseases
- Recurrent urinary tract infections
Clinical features
- Most patients present with symptoms associated with locally advanced disease (Eur Urol 2013;64:823)
- Gross hematuria or bloody urethral discharge, dysuria, extraurethral mass
- Bladder outlet obstruction, pelvic pain, urethrocutaneous fistula
- Abscess formation, dyspareunia
- Approximately 33% of men and women present with involved regional lymph nodes
Diagnosis
- Clinical examination with palpation of external genitalia for suspicious indurations and pelvic exam in women (Eur Urol 2013;64:823)
- Urinary cytology
- Diagnostic urethroscopy and biopsy
Radiology description
- Aims to assess local extent and detect lymphatic and distant metastatic spread
- Magnetic resonance imaging for evaluating extent of tumor and monitoring response to neoadjuvant chemotherapy (Eur Urol 2013;64:823)
Prognostic factors
- Both sexes (Hematol Oncol Clin North Am 2012;26:1291, Eur Urol 2013;64:823):
- Advanced age (≥ 65 years) and race (African American)
- Stage, grade, nodal involvement and metastasis
- Size and proximal tumor location
- Presence of concomitant bladder cancer
- Type and modality of treatment
- Men:
- Invasion of prostatic stroma signifies worse prognosis (Hematol Oncol Clin North Am 2012;26:1291)
- Lymphovascular, perineural invasion and histologic grade (squamous) (World J Urol 2009;27:169)
- Tumors arising in proximal urethra have worse prognosis than those arising in the distal (pendulous) portion
Case reports
- 39 year old man with a primary enteric type mucinous adenocarcinoma of the urethra (Int Surg 2014;99:669)
- 39 year old white man with metastatic urethral clear cell carcinoma (Clin Genitourin Cancer 2012;10:47)
- 49 year old man with squamous cell carcinoma of the bulbar urethra (J Clin Oncol 2011;29:e733)
Treatment
- Localized disease in men:
- Distal urethrectomy with negative surgical margins as an alternative to previously aggressive surgical excision with penile amputation (Eur Urol 2013;64:823)
- Advanced disease in both sexes:
- Chemotherapy with cisplatinum based agents
- Uncertain value of lymph node dissection (Curr Opin Urol 2015;25:129)
- References: Br J Urol 1998;82:835, Urology 1999;53:1126, Kufe: Cancer Medicine Review, 6th Edition, 2003
Gross images
Contributed by Jesus Adrian Chavez, M.D. and Debra Zynger, M.D.
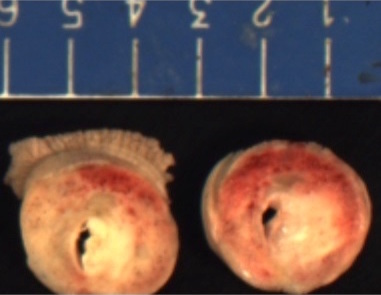
Penile urethra with periurethral involvement
Microscopic (histologic) description
- Urothelial carcinoma
- Cytologically malignant urothelial cells with visible cell membranes, marked nucleomegaly, irregular nuclei, prominent nucleoli, dark chromatin and abundant mitosis (Bostwick: Urologic Surgical Pathology, 3rd Edition, 2014)
- Squamous cell carcinoma
- Sheets of large, pleomorphic tumor cells with focal or abundant keratinization (depending of grade of differentiation), ample cytoplasm, intercellular bridges, high mitotic activity, prominent nuclear atypia
- Adenocarcinoma
- Composed of simple or pseudostratified columnar epithelium, apical cytoplasm and basally located hyperchromatic nuclei (Bostwick: Urologic Surgical Pathology, 3rd Edition, 2014)
- Occasional vacuolated cytoplasm with mucin or can be a true mucinous tumor with mucin pools
- Clear cell adenocarcinoma
- May have glandular, tubulocystic, solid / diffuse, papillary or micropapillary growth patterns
- Cuboidal, variably sized cells with abundant clear or eosinophilic cytoplasm and cytoplasmic vacuoles
- Nuclei that are hyperchromatic, pleomorphic and have prominent nucleoli
- Hobnail changes and extracellular mucoid material may be present
- Mitoses and necrosis are often seen
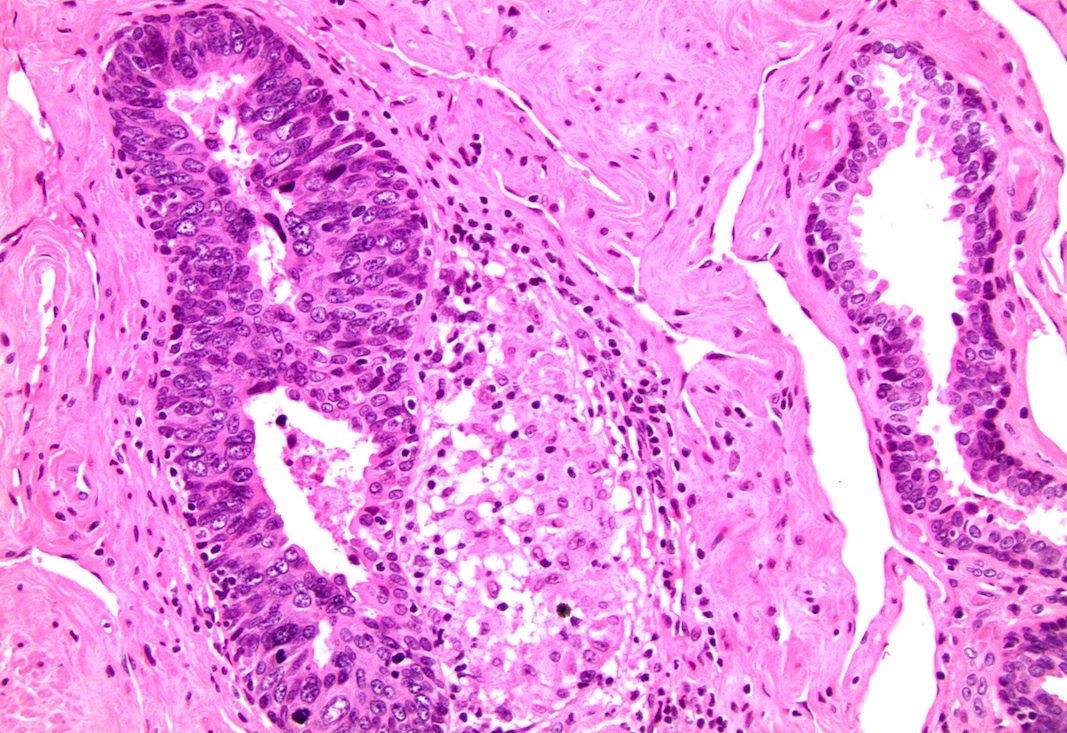
Microscopic (histologic) images
Contributed by Jesus Adrian Chavez, M.D. and Debra Zynger, M.D.
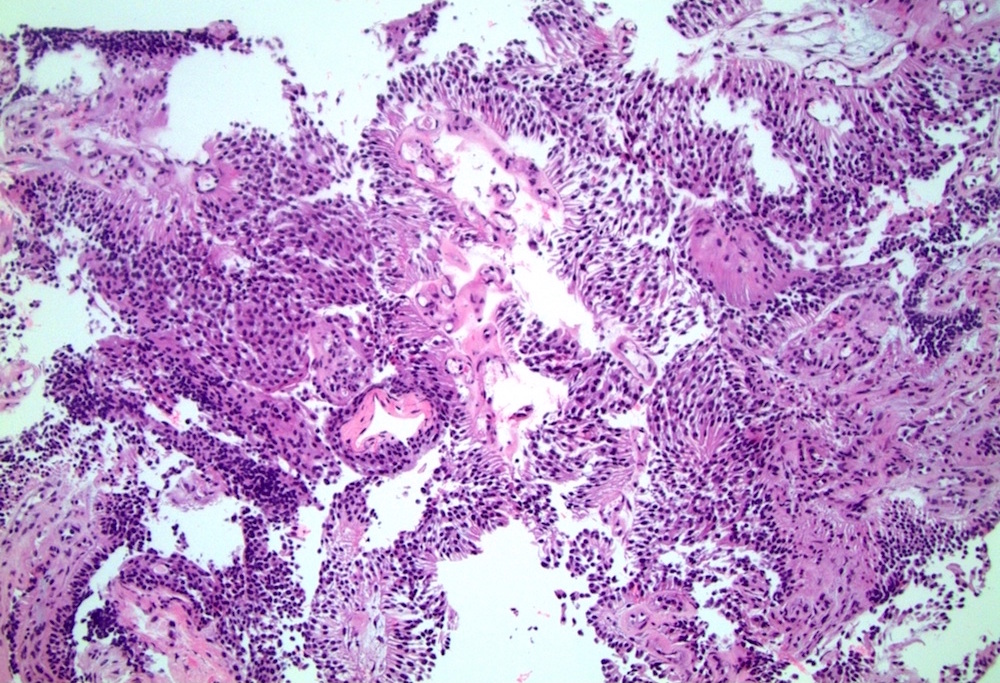
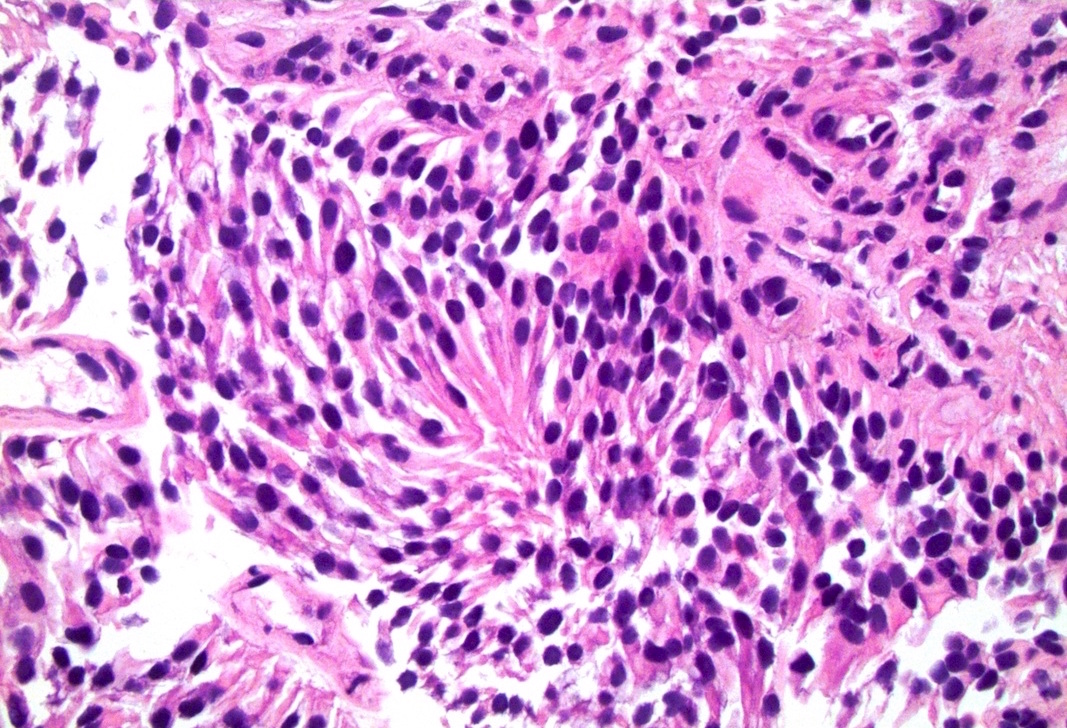
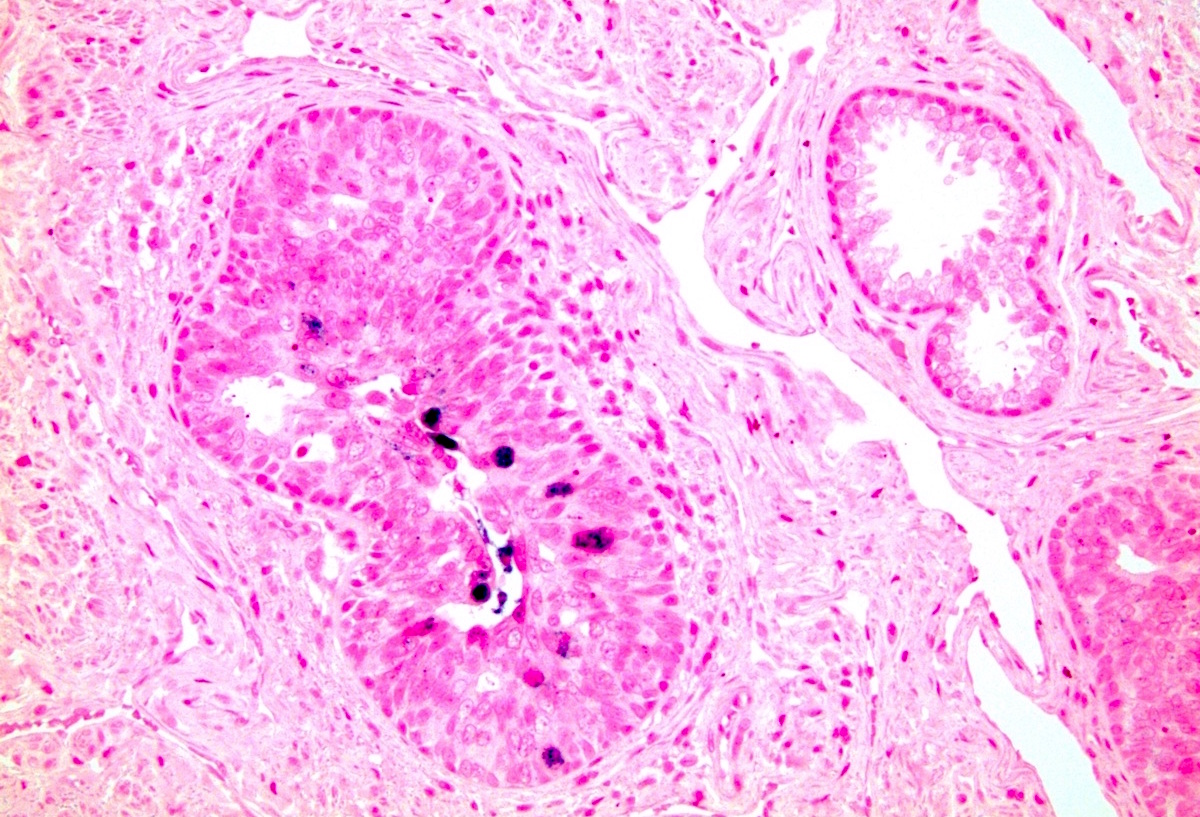
Low grade noninvasive papillary urothelial carcinoma
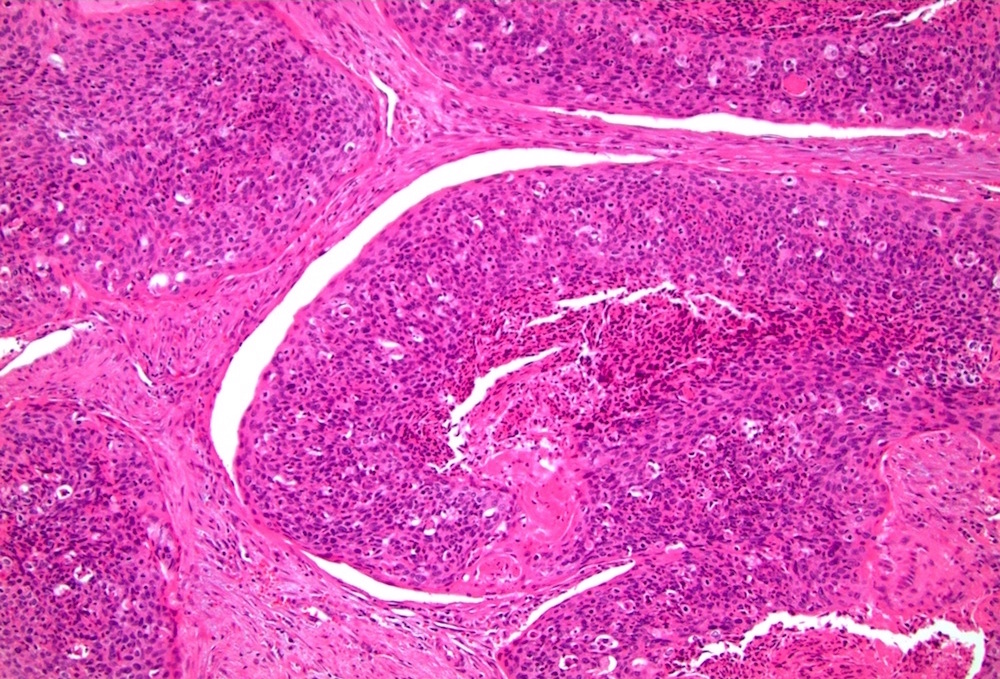
Penile urethra, squamous cell carcinoma
Penile urethra, HPV+ high risk ISH
Necrosis and keratinization
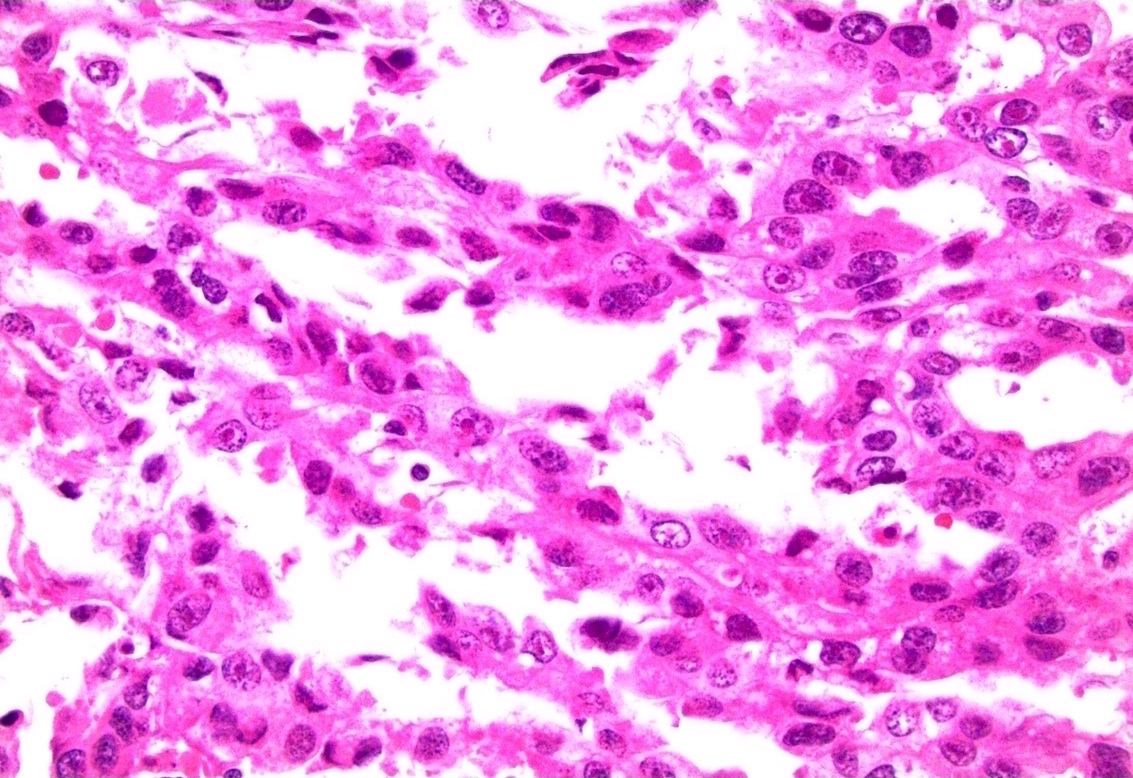
Clear cell adenocarcinoma:
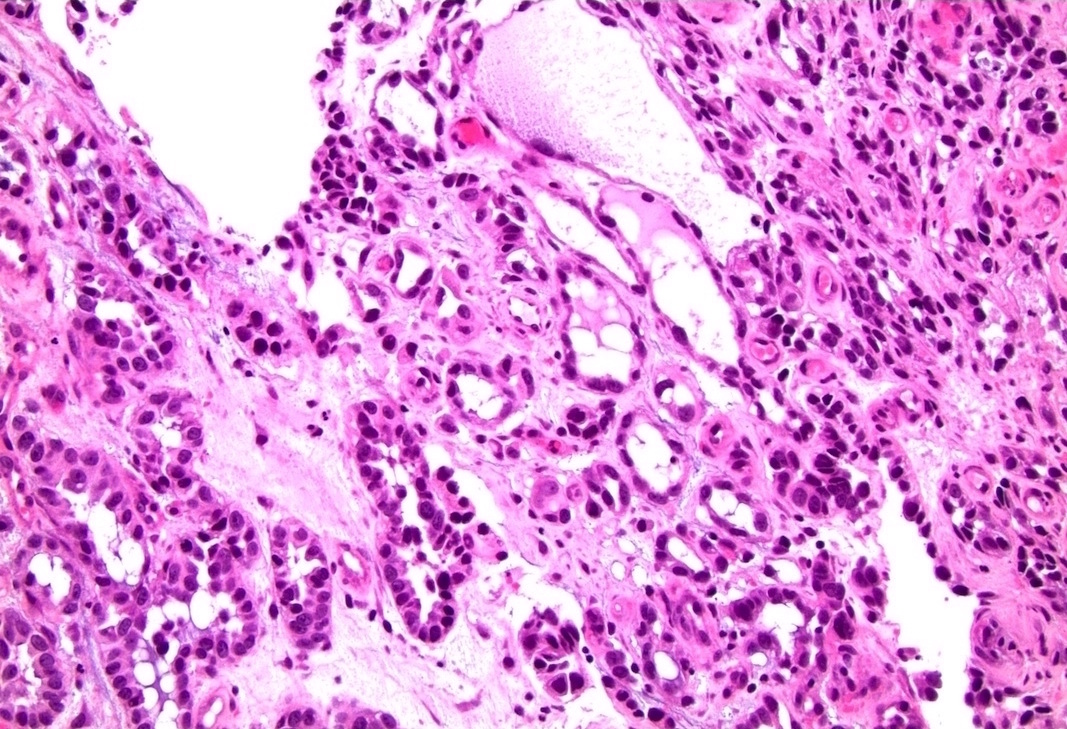
Can mimic nephrogenic metaplasia
With hobnailing
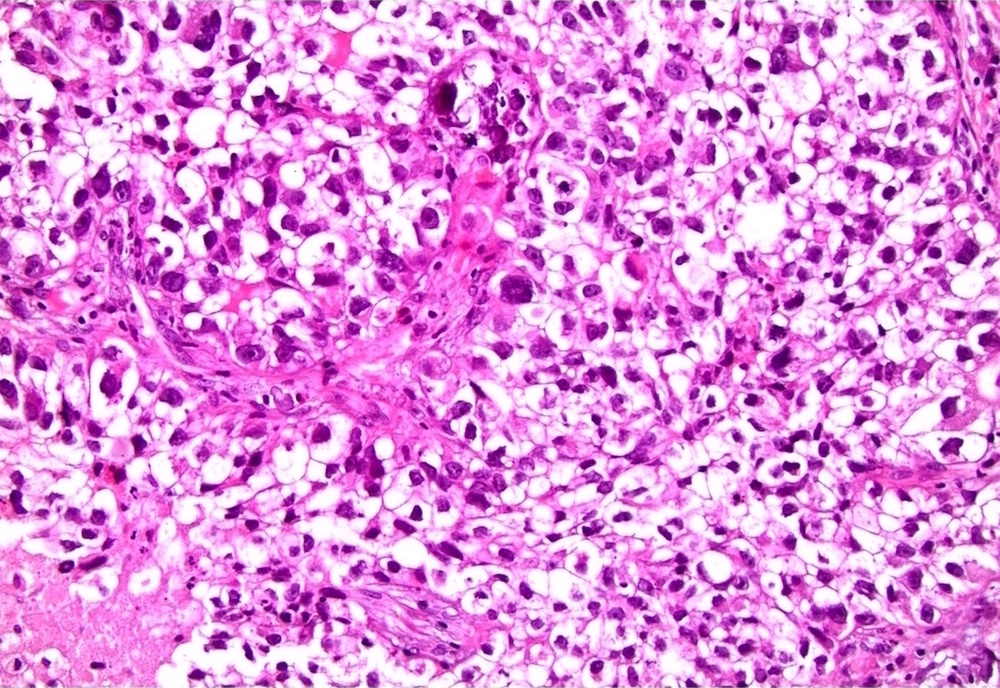
With prominent clear cells and diffuse, sheet-like growth
Positive stains
- Adenocarcinoma
- CK20 (variable), CDX2 (variable), cytoplasmic beta catenin
- Clear cell adenocarcinoma
- AMACR (racemase) (75%), vimentin (75%), p53 (100%) (Virchows Arch 2013;462:193)
- PAX8 (50%), CK7 (50%) (Virchows Arch 2013;462:193)
- Squamous cell carcinoma
- High molecular weight cytokeratin (CK903, CK5/6), p63, p16 (HPV related)
- Urothelial carcinoma
- p53 (80%), CK20 (transurothelial in carcinoma in situ, variable in invasive urothelial carcinoma), CK7 , GATA3, high molecular weight cytokeratin (CK903, CK5/6), p63 (Hum Pathol 2013;44:2760)
Negative stains
- Urothelial carcinoma
- E-cadherin, CD44s, PAX8, PSA, PSAP
- Squamous cell carcinoma
- Adenocarcinoma
- Clear cell adenocarcinoma
Differential diagnosis
- Adenocarcinoma of adjacent anatomic sites (prostate and colon)
- Nephrogenic metaplasia (versus clear cell adenocarcinoma)
- Squamous cell carcinoma of penis with extension
- Urothelial carcinoma of bladder with extension (more frequent than primary)

