20 March 2025 - Case of the Month #548
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Rahul Koshy and Dr. Julie Jorns, Medical College of Wisconsin, Milwaukee, Wisconsin, USA for contributing this case and discussion and to Dr. Gary Tozbikian, Ohio State University Wexner Medical Center, Columbus, Ohio, USA for reviewing the discussion.

Paid advertisement
Case of the Month #548
Clinical history:
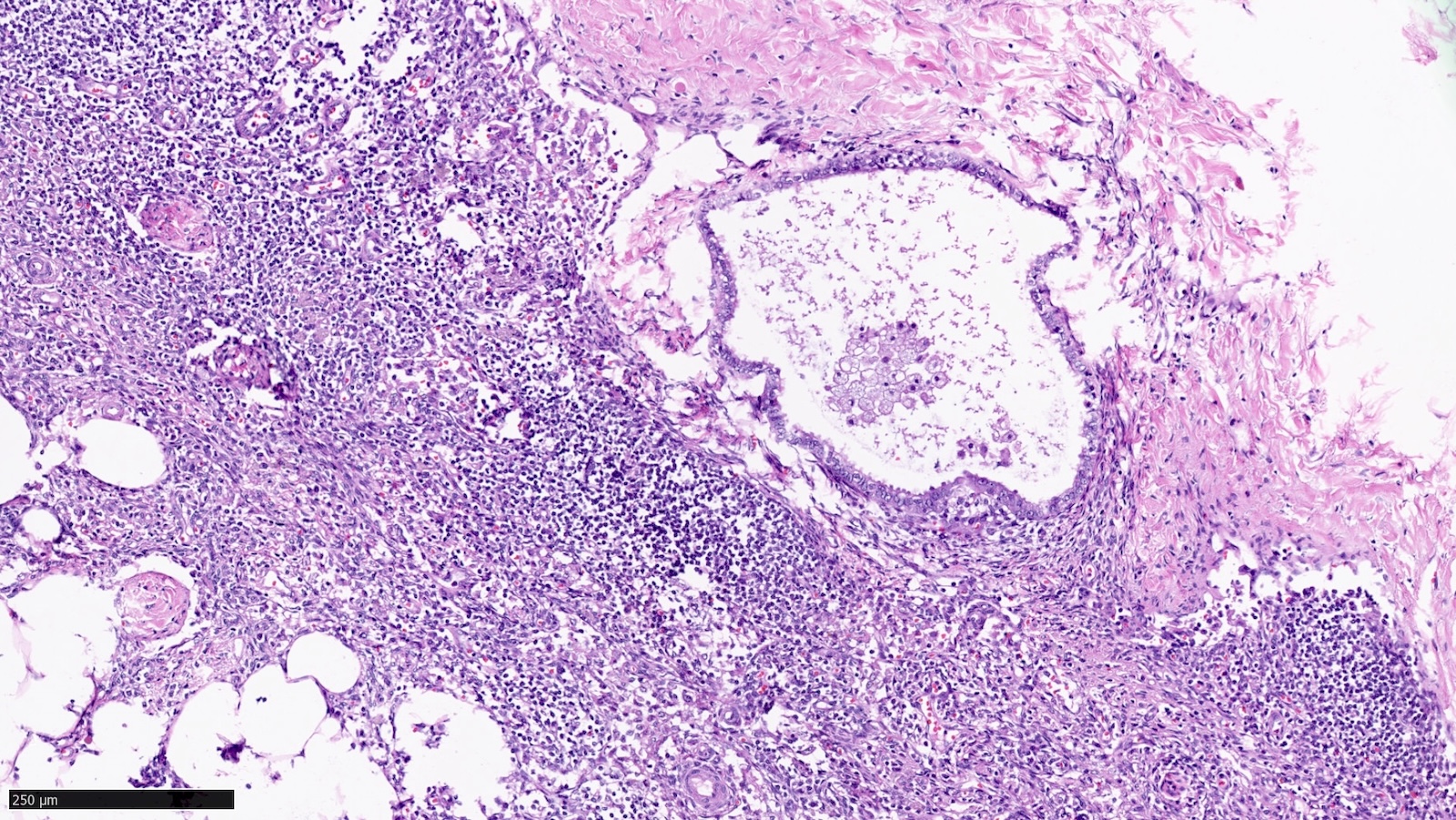
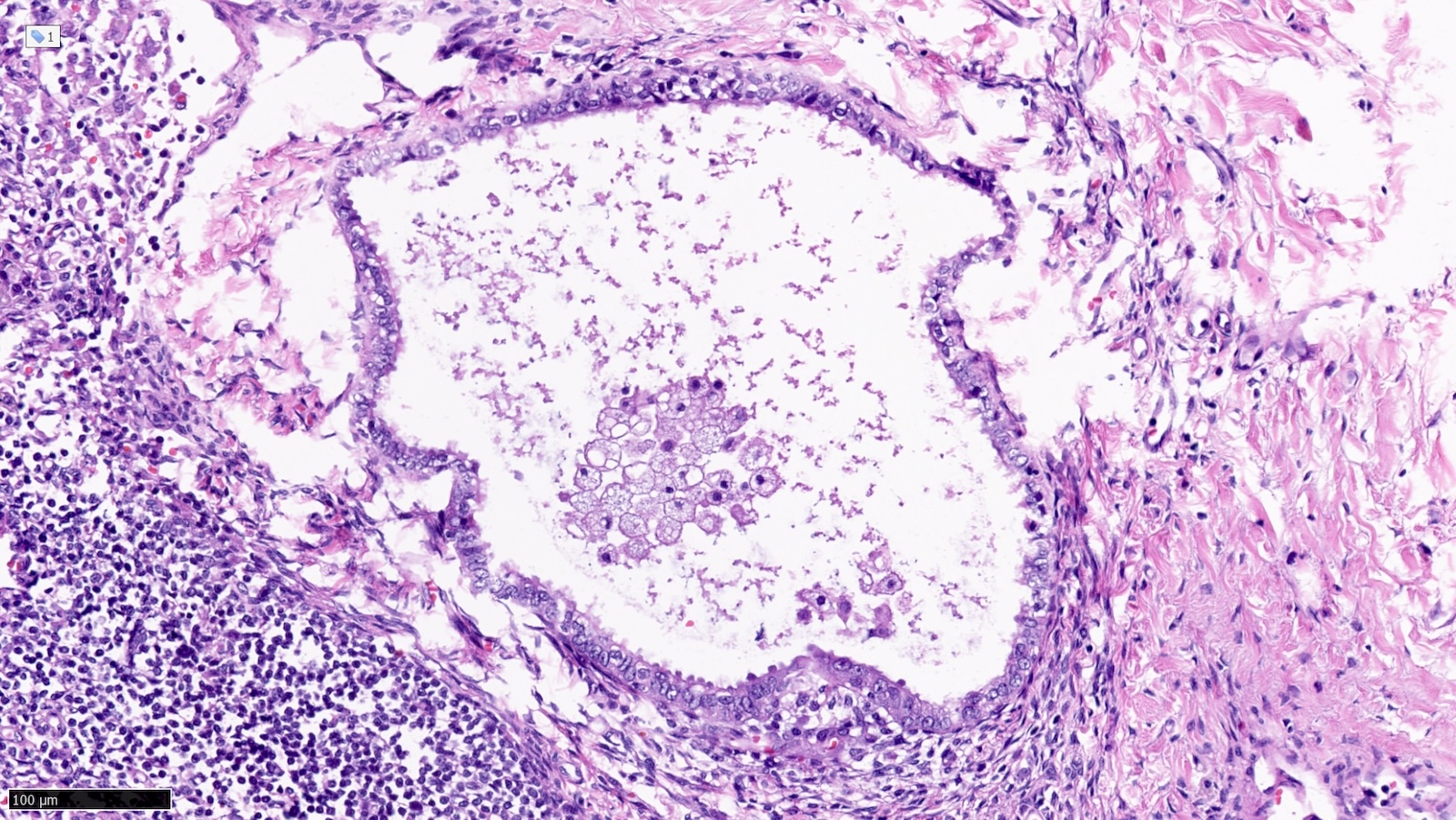
A perimenopausal patient underwent mastectomy which showed invasive lobular carcinoma, modified Bloom-Richardson grade 1 (3 + 1 + 1) with negative margins. Axillary sentinel lymph nodes were submitted for staging. H&E images of one sentinel lymph node excision are shown.
Microscopic images:
What is your diagnosis?
Diagnosis: Endosalpingiosis in an axillary lymph node
Test question (answer at the end):
A patient with breast cancer undergoes sentinel lymph node excision. What is the next step based on the histologic findings shown?
Stains:
Discussion:
Endosalpingiosis is a medical condition characterized by the presence of benign glandular tissue with morphology and immunophenotype resembling the lining of the fallopian tubes. This lesion is identified outside of the fallopian tube and is typically seen in the pelvic and abdominal peritoneum and organs. It has rarely been described in inguinal, mediastinal and axillary lymph nodes (Case Rep Pathol 2016;2016:2856358, Am J Surg Pathol 2010;34:1211, Pathology 2014;46:665, Breast J 2020;26:274). Microscopically, the lesion is composed of glands and tubules with ciliated cuboidal to columnar cells.
The differential diagnosis of endosalpingiosis includes endometriosis and low grade adenocarcinoma. As in this case, endosalpingiosis is often found incidentally because it does not typically cause clinical symptoms like those seen in endometriosis (e.g., pain due to inflammation and bleeding). Endosalpingiosis may be mistaken for carcinoma and lead to misdiagnosis as metastatic disease and incorrect cancer staging. In this case, the origin of the epithelial tissue was confirmed to be Müllerian type with the use of PAX8 (positive) and TRPS1 (negative) immunohistochemical stains.
One possible explanation for the pathogenesis of endosalpingiosis is the theory of Müllerianosis. This theory describes the displacement of Müllerian tissue during embryonic development which may explain its presence in abnormal locations. Other hypotheses for development of endosalpingiosis include direct implantation of normal fallopian tube epithelium, involution of ovarian surface epithelium and metaplastic changes in peritoneal cells (Reprod Sci 2013;20:1030).
Test question answer:
B. Confirm epithelial subtype by immunohistochemistry. The histology of the glandular epithelial structure in the lymph node capsule resembles fallopian tube epithelium. PAX8 (positive) and TRPS1 (negative) immunohistochemical stains would further support Müllerian origin and the diagnosis of endosalpingiosis in an axillary sentinel lymph node. Answers A, C and D are incorrect because the patient should not be staged as pN1mi(sn) or receive additional surgery or radiation therapy to the axilla, respectively.
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Rahul Koshy and Dr. Julie Jorns, Medical College of Wisconsin, Milwaukee, Wisconsin, USA for contributing this case and discussion and to Dr. Gary Tozbikian, Ohio State University Wexner Medical Center, Columbus, Ohio, USA for reviewing the discussion.
Paid advertisement
Website news:
(1) New Deputy Editor-in-Chief for Cytopathology: Dr. Bonnie Choy was recently promoted to Deputy Editor-in-Chief for Cytopathology. Dr. Choy is an Assistant Professor of Pathology at Northwestern University Feinberg School of Medicine, where she serves as the Associate Program Director for the Pathology Residency and Cytopathology Fellowship.
(2) Q4 2024 PathologyOutlines.com Jobs Report: The fourth quarter PathologyOutlines.com Jobs report for 2024 has been posted at pathologyoutlines.com/pathjobs2024q4.html. For this quarter, PathologyOutlines.com listed 388 full or part time pathologist job postings, which form the basis for the statistics within the report.
(3) 2024 Year in Review Video: We have posted a YouTube Shorts video highlighting some of the significant changes that were made to PathologyOutlines.com in 2024. Check it out at youtube.com/shorts/0Jp2F5J2JSw.
Visit and follow our Blog to see recent updates to the website.
(1) New Deputy Editor-in-Chief for Cytopathology: Dr. Bonnie Choy was recently promoted to Deputy Editor-in-Chief for Cytopathology. Dr. Choy is an Assistant Professor of Pathology at Northwestern University Feinberg School of Medicine, where she serves as the Associate Program Director for the Pathology Residency and Cytopathology Fellowship.
(2) Q4 2024 PathologyOutlines.com Jobs Report: The fourth quarter PathologyOutlines.com Jobs report for 2024 has been posted at pathologyoutlines.com/pathjobs2024q4.html. For this quarter, PathologyOutlines.com listed 388 full or part time pathologist job postings, which form the basis for the statistics within the report.
(3) 2024 Year in Review Video: We have posted a YouTube Shorts video highlighting some of the significant changes that were made to PathologyOutlines.com in 2024. Check it out at youtube.com/shorts/0Jp2F5J2JSw.
Visit and follow our Blog to see recent updates to the website.
Case of the Month #548
Clinical history:
A perimenopausal patient underwent mastectomy which showed invasive lobular carcinoma, modified Bloom-Richardson grade 1 (3 + 1 + 1) with negative margins. Axillary sentinel lymph nodes were submitted for staging. H&E images of one sentinel lymph node excision are shown.
Microscopic images:
What is your diagnosis?
Click here for diagnosis, test question and discussion:
Diagnosis: Endosalpingiosis in an axillary lymph node
Test question (answer at the end):
A patient with breast cancer undergoes sentinel lymph node excision. What is the next step based on the histologic findings shown?
- Assign axillary nodal stage (AJCC 8th edition) as pN1mi(sn)
- Confirm epithelial subtype by immunohistochemistry
- Recommend axillary lymph node dissection
- Recommend nodal basin radiation therapy
Stains:
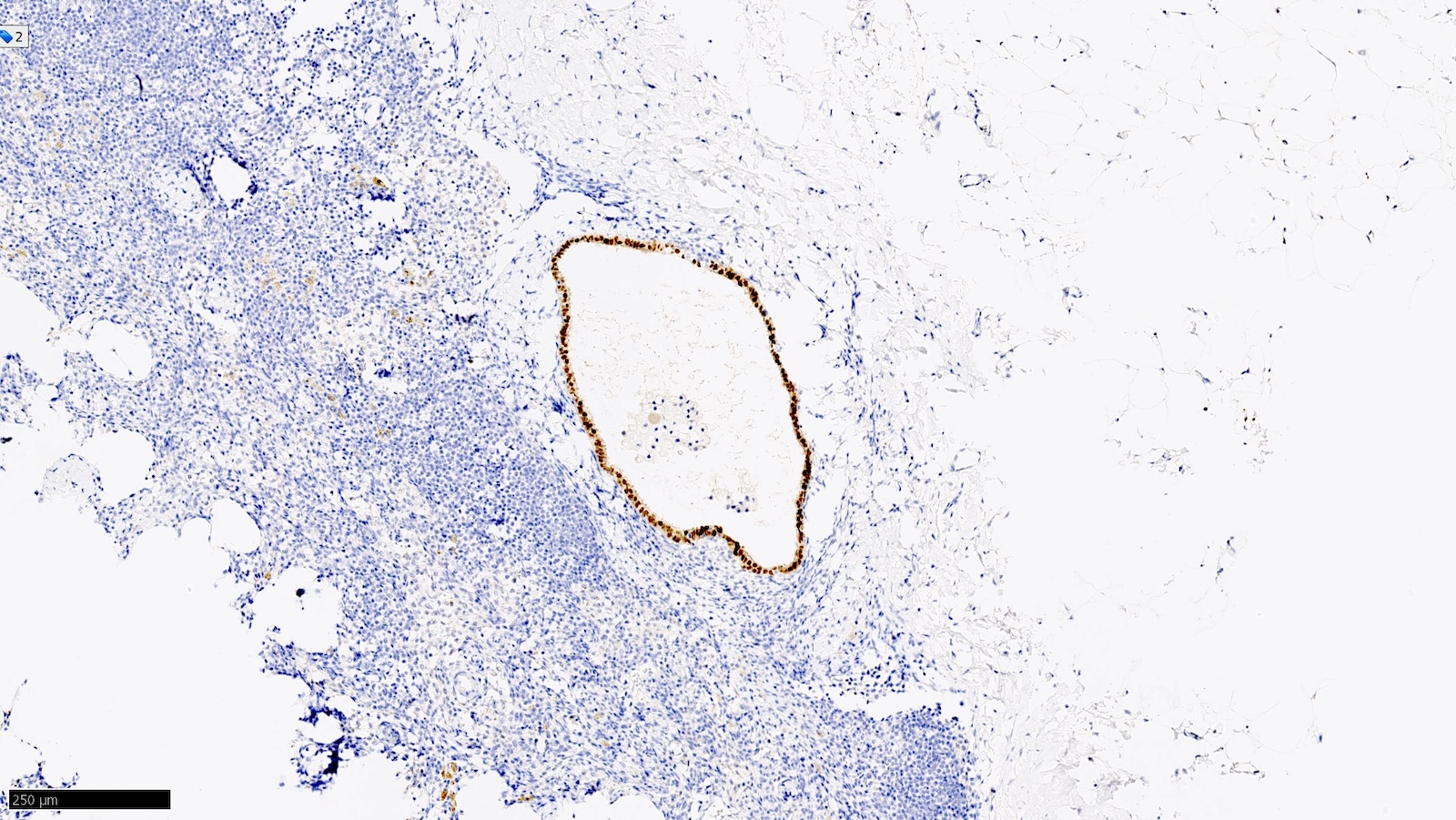
PAX8
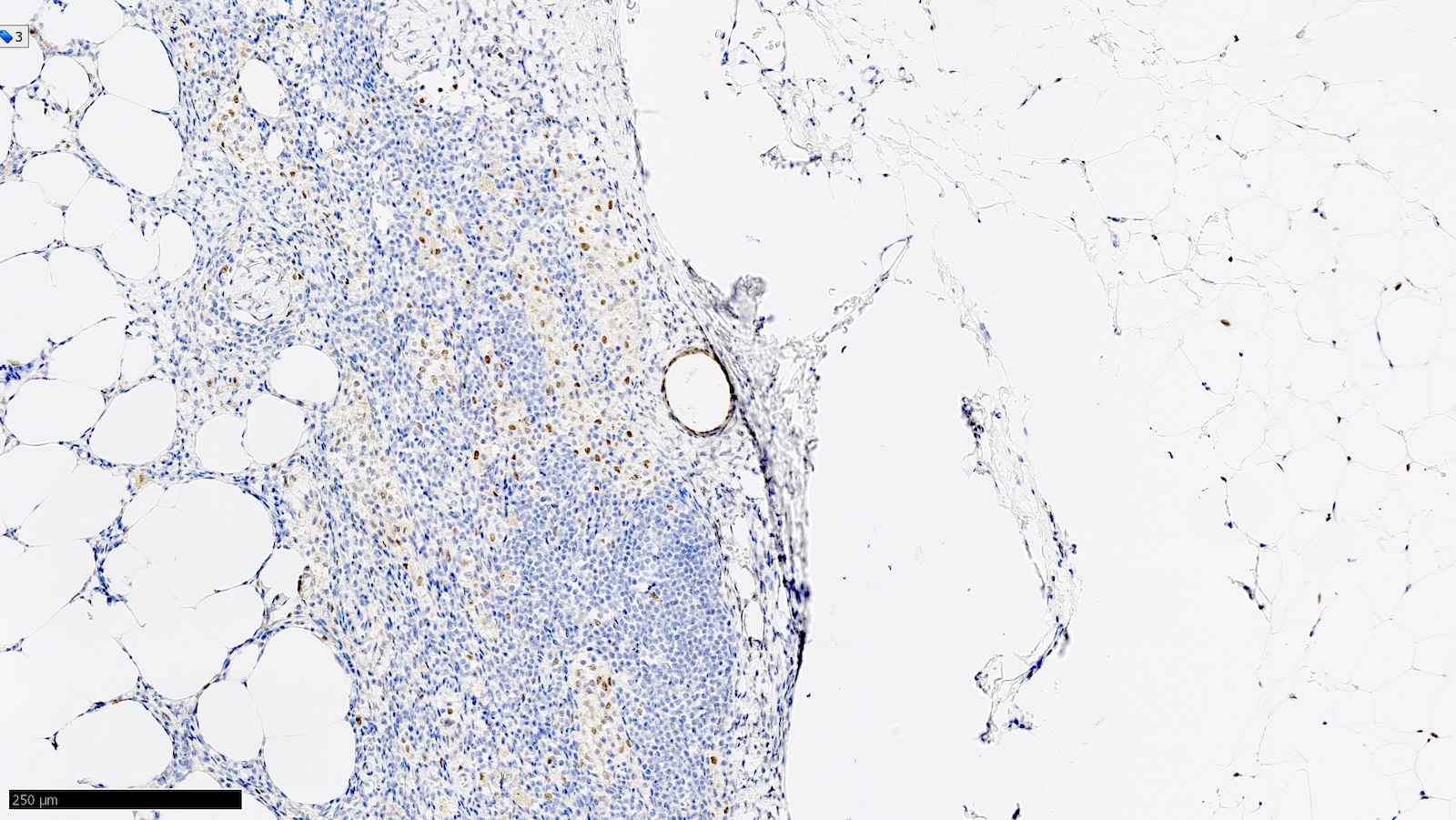
TRPS1
Discussion:
Endosalpingiosis is a medical condition characterized by the presence of benign glandular tissue with morphology and immunophenotype resembling the lining of the fallopian tubes. This lesion is identified outside of the fallopian tube and is typically seen in the pelvic and abdominal peritoneum and organs. It has rarely been described in inguinal, mediastinal and axillary lymph nodes (Case Rep Pathol 2016;2016:2856358, Am J Surg Pathol 2010;34:1211, Pathology 2014;46:665, Breast J 2020;26:274). Microscopically, the lesion is composed of glands and tubules with ciliated cuboidal to columnar cells.
The differential diagnosis of endosalpingiosis includes endometriosis and low grade adenocarcinoma. As in this case, endosalpingiosis is often found incidentally because it does not typically cause clinical symptoms like those seen in endometriosis (e.g., pain due to inflammation and bleeding). Endosalpingiosis may be mistaken for carcinoma and lead to misdiagnosis as metastatic disease and incorrect cancer staging. In this case, the origin of the epithelial tissue was confirmed to be Müllerian type with the use of PAX8 (positive) and TRPS1 (negative) immunohistochemical stains.
One possible explanation for the pathogenesis of endosalpingiosis is the theory of Müllerianosis. This theory describes the displacement of Müllerian tissue during embryonic development which may explain its presence in abnormal locations. Other hypotheses for development of endosalpingiosis include direct implantation of normal fallopian tube epithelium, involution of ovarian surface epithelium and metaplastic changes in peritoneal cells (Reprod Sci 2013;20:1030).
Test question answer:
B. Confirm epithelial subtype by immunohistochemistry. The histology of the glandular epithelial structure in the lymph node capsule resembles fallopian tube epithelium. PAX8 (positive) and TRPS1 (negative) immunohistochemical stains would further support Müllerian origin and the diagnosis of endosalpingiosis in an axillary sentinel lymph node. Answers A, C and D are incorrect because the patient should not be staged as pN1mi(sn) or receive additional surgery or radiation therapy to the axilla, respectively.