24 July 2024 - Case of the Month #540
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Kelly Magliocca, Emory University School of Medicine, Atlanta, Georgia, USA for contributing this case and discussion and to Dr. Bin Xu, Memorial Sloan Kettering Cancer Center, New York, New York, USA for reviewing the discussion.

Case of the Month #540
Clinical history:
A 15 year old boy presented with nasal obstruction and epistaxis.
Gross and microscopic images:



What is your diagnosis?
Diagnosis: Sinonasal tract angiofibroma (STA)
Test question (answer at the end):
Which of the following modalities is most commonly used in the diagnosis and preoperative evaluation of sinonasal tract angiofibroma (STA)?
Discussion:
Sinonasal tract angiofibroma (STA) is an uncommon locally destructive sinonasal neoplasm representing < 1% of head and neck tumors. Prior nomenclature "juvenile nasopharyngeal angiofibroma" has been discontinued as evidence suggests the tumor originates in the posterolateral region of the nasal cavity rather than tissues of the nasopharynx. Similarly, since the tumor is not exclusive to juvenile populations, use of the term "juvenile" is not recommended. STA occurs almost exclusively in the male population (Laryngoscope 2013;123:859, Head Neck Pathol 2018;12:52).
The male predominance and the peak incidence during adolescence suggest a hormonal influence in STA. While androgen receptors have been detected in these, a subset of this disease occurs in prepubertal patients leaving open the possibility that other mechanisms of pathogenesis may have a role (Head Neck Pathol 2018;12:52, Acta Otolaryngol 2015;135:51). Dysregulation of the Wnt signaling pathway has been implicated in the pathogenesis of STA (Am J Pathol 2001;158:1073).
Nasal obstruction and epistaxis are the two most common presenting symptoms. With tumor progression, facial swelling, cranial nerve palsies, conductive hearing deficits, sleep disordered breathing, trismus, diplopia and proptosis may be seen (Cancers (Basel) 2023;15:5022).
Imaging modalities such as contrast enhanced computed tomography (CT) and magnetic resonance imaging (MRI) are used to delineate the extent of tumor and plan surgical intervention. MRI is commonly used because of its excellent soft tissue contrast and its ability to delineate the extent of the tumor and its relationship to adjacent structures including intracranial extension. A tumor in the pterygopalatine fossa may cause widening of the pterygoid plates and anterior displacement (bowing) of the posterior wall of the maxillary sinus, known as the Holmann-Miller sign. Arteriographic studies help to delineate feeding vessels, often the internal maxillary artery, and are useful in preoperative embolization (J Otolaryngol Head Neck Surg 2023;52:85, Am J Surg 1973;126:547).
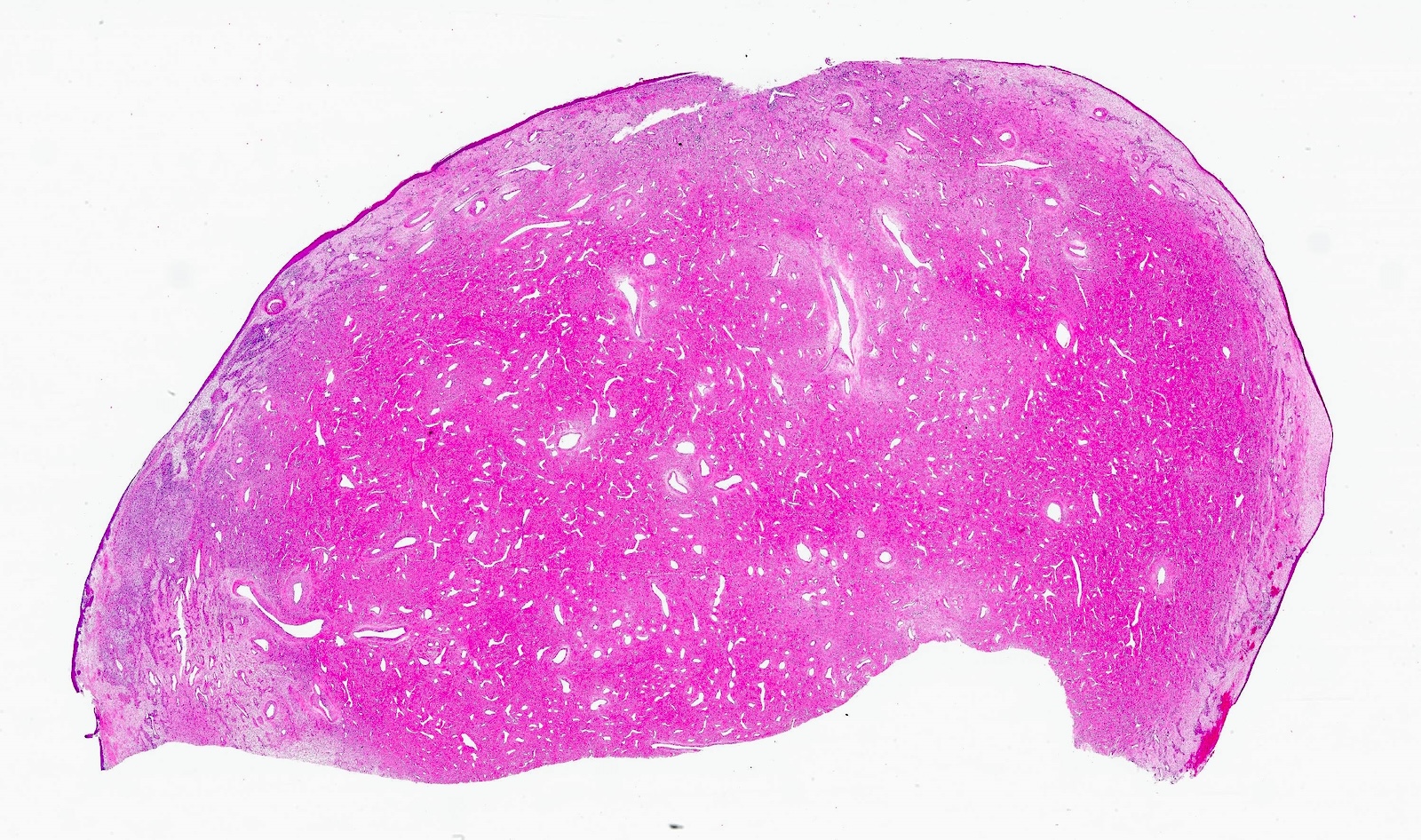
STA is macroscopically lobulated, polypoid or pedunculated with a cut surface demonstrating variably sized vascular channels within a dense fibrotic background (Head Neck Pathol 2018;12:52). STA is an unencapsulated neoplasm characterized by a fibrocollagenous stromal proliferation with a prominent admixture of variably sized vascular spaces. The predominant stromal cells are bipolar or spindle shaped fibroblasts with plump vesicular nuclei and indistinct nucleoli set within a fibrocollagenous background. Mild nuclear pleomorphism and multinucleated floret or giant cells may be seen, however, mitotic figures are generally absent. Both stromal cellularity and density of fibrotic stroma can vary. Areas of edema can be seen alongside dense fibrous tissue and coarsely collagenized matrix. Inflammation is generally limited to scattered mast cells, except near areas of surface ulceration.
The vascular component consists of numerous thin walled vessels and larger, irregular staghorn channels. Many vessels lack a complete muscular layer, distinguishing them from typical blood vessels. Vessel walls lack elastic fibers and are distinctive in having a smooth muscle layer, which may be incomplete and varies in thickness. Endothelial cells form a single layer and are flat or plump in appearance. Embolized tumors show areas of necrosis and intravascular foreign material. Evidence of preoperative embolization may be seen in tissue sections, in the form of intravascular fibrin thrombi containing foreign material or tumor infarction. Longstanding tumors tend to be more fibrous and less vascular.
While smooth muscle actin (SMA) or other smooth muscle markers highlight smooth muscle surrounding some vascular channels, CD31, CD34 or ERG highlight endothelial cells. AR is positive in stroma cells, although the expression may be focal and weak (Acta Otolaryngol 2015;135:51, Mod Pathol 1998;11:1122). Nuclear beta catenin staining in stromal cells (fibroblasts) is present in 70 - 90% of cases (J Laryngol Otol 2016;130:907).
Definitive management of STA generally involves surgical resection while minimizing morbidity. Endoscopic approaches have been used more commonly in the last 2 decades due to reduced morbidity compared to open surgical techniques. Open surgical approaches (e.g. lateral rhinotomy, infratemporal, transmaxillary, Le Fort I, with or without endoscopic assistance) are typically reserved for more advanced disease states that would present difficulty for complete endoscopic excision. Prior to any surgical management, preoperative vascular embolization is generally employed to reduce intraoperative blood loss. STA is a benign neoplasm but radiotherapy is occasionally employed for clinical scenarios in which surgical resection is associated with high morbidity, such as a bulky intracranial component. Related to the young age of affected patients and concerns of radiation associated morbidity, proton therapy has emerged as a promising modality, offering targeting of the tumor while minimizing damage to surrounding tissues (Cancers (Basel) 2023;15:5022, Int Forum Allergy Rhinol 2024;14:149, Paediatr Anaesth 2023;33:510, Eur Arch Otorhinolaryngol 2023;280:2081, Laryngoscope 2013;123:859).
The prognosis for patients with STA is favorable with rates of recurrence generally reported to range up to 25%, although size, location, intracranial extension and possibly treatment modality may impact recurrence rate (Laryngoscope 2013;123:859, Otolaryngol Head Neck Surg 2014;150:350, Laryngoscope 2013;123:1125, Otolaryngol Head Neck Surg 2019;161:352). Routine clinical follow up including examination and imaging may assist in detection and management of recurrence. Rare examples of malignancy developing after radiation treatment have been reported (Case Rep Oncol Med 2018;2018:5695803). Spontaneous regression after puberty may rarely occur (Ann Otol Rhinol Laryngol 1992;101:469). Radiographic and clinical staging systems are used to guide treatment and determine recurrence risk (J Neurol Surg B Skull Base 2017;78:63).
Test question answer:
B. Magnetic resonance imaging (MRI). MRI is a common imaging modality for evaluating STA due to its excellent soft tissue contrast and ability to delineate the extent of the tumor and its relationship to adjacent structures (including intracranial extension). Answer A is incorrect since FNA biopsy is not routinely recommended due to the highly vascular nature of the neoplasm. Occasionally, severe hemorrhage can occur with minor manipulation due to the number of vascular channels, the lack of a predictable muscular layer or lack of an elastic layer or paucity of elastic fibers within the dense stroma. Answer C is incorrect because PET scans are generally not used for primary diagnostic evaluation of STA. Answer D is incorrect because ultrasonography is not commonly used for assessing STA due to limited visualization of deep structures.
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Kelly Magliocca, Emory University School of Medicine, Atlanta, Georgia, USA for contributing this case and discussion and to Dr. Bin Xu, Memorial Sloan Kettering Cancer Center, New York, New York, USA for reviewing the discussion.
Website news:
(1) PathologyOutlines.com’s Jobs report for the 2023 calendar year has been posted on our Jobs page. PathologyOutlines.com listed 1,501 full or part time pathologist job postings, which form the basis for the statistics within the report. Click here for full details of the report.
(2) We have posted our most recent What’s New in Adrenal Gland Pathology newsletter by Drs. Carol N. Rizkalla and Maria Tretiakova. This edition of our What’s New in Pathology newsletter focuses on updates from the WHO 5th edition for adrenal cortex. You can read our past newsletters and subscribe to all of our future What’s New in Pathology newsletters on our Newsletters page.
(3) On May 6, 2024, the U.S. Food and Drug Administration (FDA) published the highly anticipated final rule on laboratory developed tests. Read the recently updated topic on LDTs at pathologyoutlines.com/topic/managementlabdevelopedtests.html, written by Dr. Moira P. Larsen and our editor-in-chief, Dr. Patricia Tsang.
Visit and follow our Blog to see recent updates to the website.
(1) PathologyOutlines.com’s Jobs report for the 2023 calendar year has been posted on our Jobs page. PathologyOutlines.com listed 1,501 full or part time pathologist job postings, which form the basis for the statistics within the report. Click here for full details of the report.
(2) We have posted our most recent What’s New in Adrenal Gland Pathology newsletter by Drs. Carol N. Rizkalla and Maria Tretiakova. This edition of our What’s New in Pathology newsletter focuses on updates from the WHO 5th edition for adrenal cortex. You can read our past newsletters and subscribe to all of our future What’s New in Pathology newsletters on our Newsletters page.
(3) On May 6, 2024, the U.S. Food and Drug Administration (FDA) published the highly anticipated final rule on laboratory developed tests. Read the recently updated topic on LDTs at pathologyoutlines.com/topic/managementlabdevelopedtests.html, written by Dr. Moira P. Larsen and our editor-in-chief, Dr. Patricia Tsang.
Visit and follow our Blog to see recent updates to the website.
Case of the Month #540
Clinical history:
A 15 year old boy presented with nasal obstruction and epistaxis.
Gross and microscopic images:
What is your diagnosis?
Click here for diagnosis, test question and discussion:
Diagnosis: Sinonasal tract angiofibroma (STA)
Test question (answer at the end):
Which of the following modalities is most commonly used in the diagnosis and preoperative evaluation of sinonasal tract angiofibroma (STA)?
- Fine needle aspiration (FNA)
- Magnetic resonance imaging (MRI)
- Positron emission tomography (PET) scan
- Ultrasonography (US)
Discussion:
Sinonasal tract angiofibroma (STA) is an uncommon locally destructive sinonasal neoplasm representing < 1% of head and neck tumors. Prior nomenclature "juvenile nasopharyngeal angiofibroma" has been discontinued as evidence suggests the tumor originates in the posterolateral region of the nasal cavity rather than tissues of the nasopharynx. Similarly, since the tumor is not exclusive to juvenile populations, use of the term "juvenile" is not recommended. STA occurs almost exclusively in the male population (Laryngoscope 2013;123:859, Head Neck Pathol 2018;12:52).
The male predominance and the peak incidence during adolescence suggest a hormonal influence in STA. While androgen receptors have been detected in these, a subset of this disease occurs in prepubertal patients leaving open the possibility that other mechanisms of pathogenesis may have a role (Head Neck Pathol 2018;12:52, Acta Otolaryngol 2015;135:51). Dysregulation of the Wnt signaling pathway has been implicated in the pathogenesis of STA (Am J Pathol 2001;158:1073).
Nasal obstruction and epistaxis are the two most common presenting symptoms. With tumor progression, facial swelling, cranial nerve palsies, conductive hearing deficits, sleep disordered breathing, trismus, diplopia and proptosis may be seen (Cancers (Basel) 2023;15:5022).
Imaging modalities such as contrast enhanced computed tomography (CT) and magnetic resonance imaging (MRI) are used to delineate the extent of tumor and plan surgical intervention. MRI is commonly used because of its excellent soft tissue contrast and its ability to delineate the extent of the tumor and its relationship to adjacent structures including intracranial extension. A tumor in the pterygopalatine fossa may cause widening of the pterygoid plates and anterior displacement (bowing) of the posterior wall of the maxillary sinus, known as the Holmann-Miller sign. Arteriographic studies help to delineate feeding vessels, often the internal maxillary artery, and are useful in preoperative embolization (J Otolaryngol Head Neck Surg 2023;52:85, Am J Surg 1973;126:547).
STA is macroscopically lobulated, polypoid or pedunculated with a cut surface demonstrating variably sized vascular channels within a dense fibrotic background (Head Neck Pathol 2018;12:52). STA is an unencapsulated neoplasm characterized by a fibrocollagenous stromal proliferation with a prominent admixture of variably sized vascular spaces. The predominant stromal cells are bipolar or spindle shaped fibroblasts with plump vesicular nuclei and indistinct nucleoli set within a fibrocollagenous background. Mild nuclear pleomorphism and multinucleated floret or giant cells may be seen, however, mitotic figures are generally absent. Both stromal cellularity and density of fibrotic stroma can vary. Areas of edema can be seen alongside dense fibrous tissue and coarsely collagenized matrix. Inflammation is generally limited to scattered mast cells, except near areas of surface ulceration.
The vascular component consists of numerous thin walled vessels and larger, irregular staghorn channels. Many vessels lack a complete muscular layer, distinguishing them from typical blood vessels. Vessel walls lack elastic fibers and are distinctive in having a smooth muscle layer, which may be incomplete and varies in thickness. Endothelial cells form a single layer and are flat or plump in appearance. Embolized tumors show areas of necrosis and intravascular foreign material. Evidence of preoperative embolization may be seen in tissue sections, in the form of intravascular fibrin thrombi containing foreign material or tumor infarction. Longstanding tumors tend to be more fibrous and less vascular.
While smooth muscle actin (SMA) or other smooth muscle markers highlight smooth muscle surrounding some vascular channels, CD31, CD34 or ERG highlight endothelial cells. AR is positive in stroma cells, although the expression may be focal and weak (Acta Otolaryngol 2015;135:51, Mod Pathol 1998;11:1122). Nuclear beta catenin staining in stromal cells (fibroblasts) is present in 70 - 90% of cases (J Laryngol Otol 2016;130:907).
Definitive management of STA generally involves surgical resection while minimizing morbidity. Endoscopic approaches have been used more commonly in the last 2 decades due to reduced morbidity compared to open surgical techniques. Open surgical approaches (e.g. lateral rhinotomy, infratemporal, transmaxillary, Le Fort I, with or without endoscopic assistance) are typically reserved for more advanced disease states that would present difficulty for complete endoscopic excision. Prior to any surgical management, preoperative vascular embolization is generally employed to reduce intraoperative blood loss. STA is a benign neoplasm but radiotherapy is occasionally employed for clinical scenarios in which surgical resection is associated with high morbidity, such as a bulky intracranial component. Related to the young age of affected patients and concerns of radiation associated morbidity, proton therapy has emerged as a promising modality, offering targeting of the tumor while minimizing damage to surrounding tissues (Cancers (Basel) 2023;15:5022, Int Forum Allergy Rhinol 2024;14:149, Paediatr Anaesth 2023;33:510, Eur Arch Otorhinolaryngol 2023;280:2081, Laryngoscope 2013;123:859).
The prognosis for patients with STA is favorable with rates of recurrence generally reported to range up to 25%, although size, location, intracranial extension and possibly treatment modality may impact recurrence rate (Laryngoscope 2013;123:859, Otolaryngol Head Neck Surg 2014;150:350, Laryngoscope 2013;123:1125, Otolaryngol Head Neck Surg 2019;161:352). Routine clinical follow up including examination and imaging may assist in detection and management of recurrence. Rare examples of malignancy developing after radiation treatment have been reported (Case Rep Oncol Med 2018;2018:5695803). Spontaneous regression after puberty may rarely occur (Ann Otol Rhinol Laryngol 1992;101:469). Radiographic and clinical staging systems are used to guide treatment and determine recurrence risk (J Neurol Surg B Skull Base 2017;78:63).
Test question answer:
B. Magnetic resonance imaging (MRI). MRI is a common imaging modality for evaluating STA due to its excellent soft tissue contrast and ability to delineate the extent of the tumor and its relationship to adjacent structures (including intracranial extension). Answer A is incorrect since FNA biopsy is not routinely recommended due to the highly vascular nature of the neoplasm. Occasionally, severe hemorrhage can occur with minor manipulation due to the number of vascular channels, the lack of a predictable muscular layer or lack of an elastic layer or paucity of elastic fibers within the dense stroma. Answer C is incorrect because PET scans are generally not used for primary diagnostic evaluation of STA. Answer D is incorrect because ultrasonography is not commonly used for assessing STA due to limited visualization of deep structures.