22 May 2024 - Case of the Month #538
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Stephanie Skala, University of Michigan, Ann Arbor, Michigan, USA for contributing this case and discussion and to Dr. Gulisa Turashvili, Emory University School of Medicine, Atlanta, Georgia, USA for reviewing the discussion.
Case of the Month #538
Clinical history:
A 58 year old woman presented with an adnexal mass.
Microscopic images:
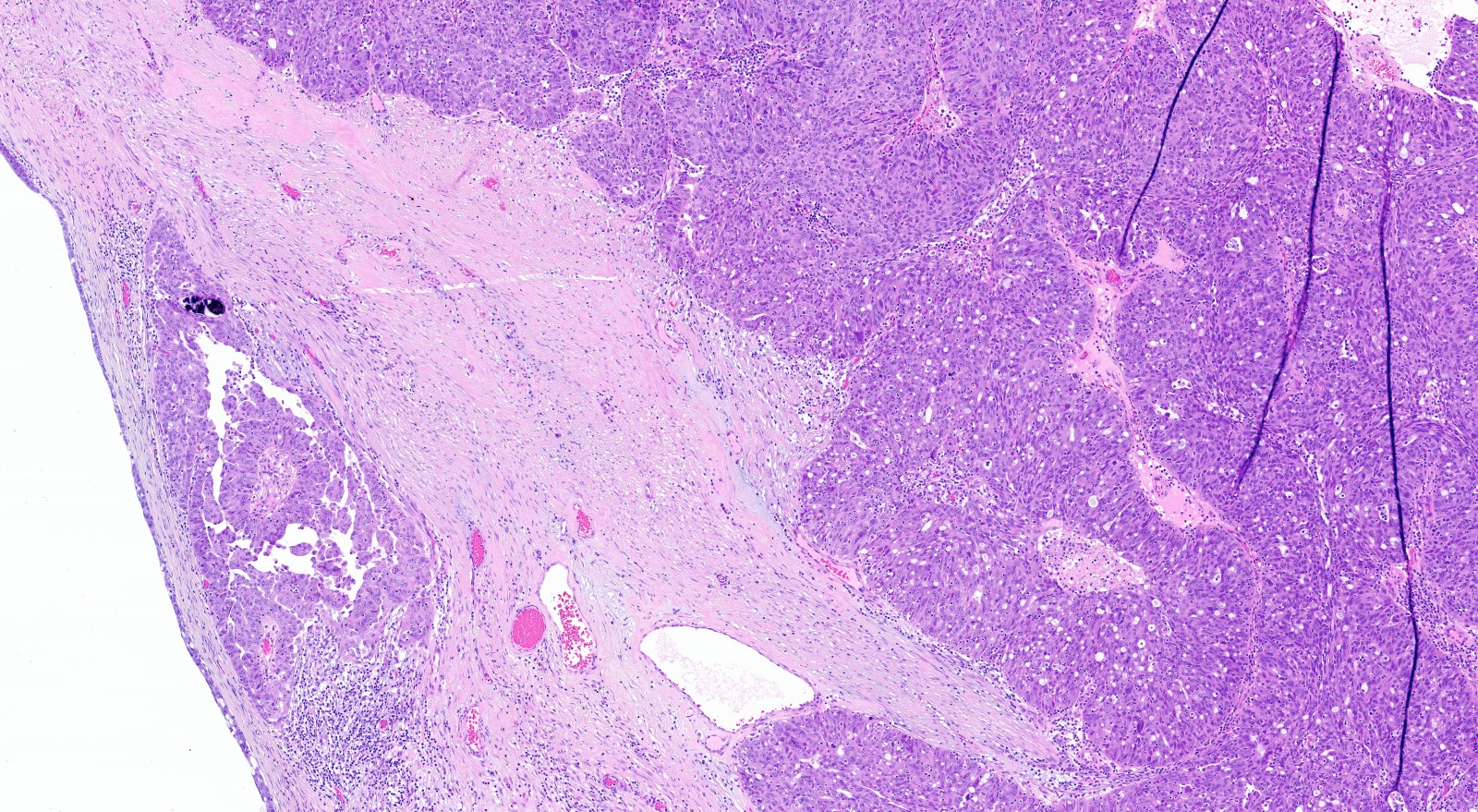
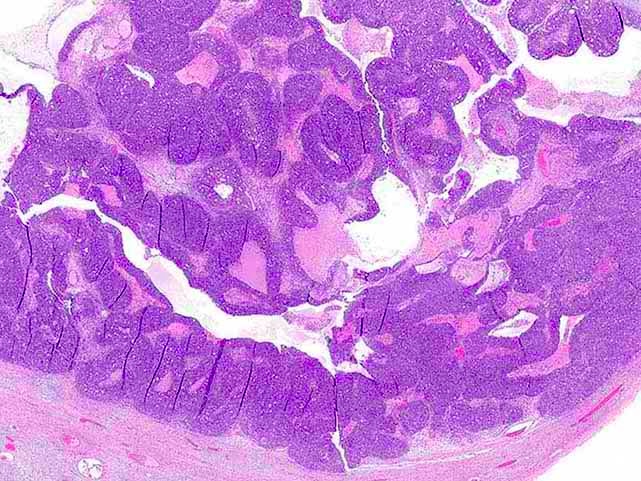

What is your diagnosis?
Diagnosis: High grade serous carcinoma with solid, pseudoendometrioid and transitional (SET) features
Test question (answer at the end):
Which gene is most commonly altered in tubo-ovarian high grade serous carcinoma with solid, pseudoendometrioid and transitional (SET) features?
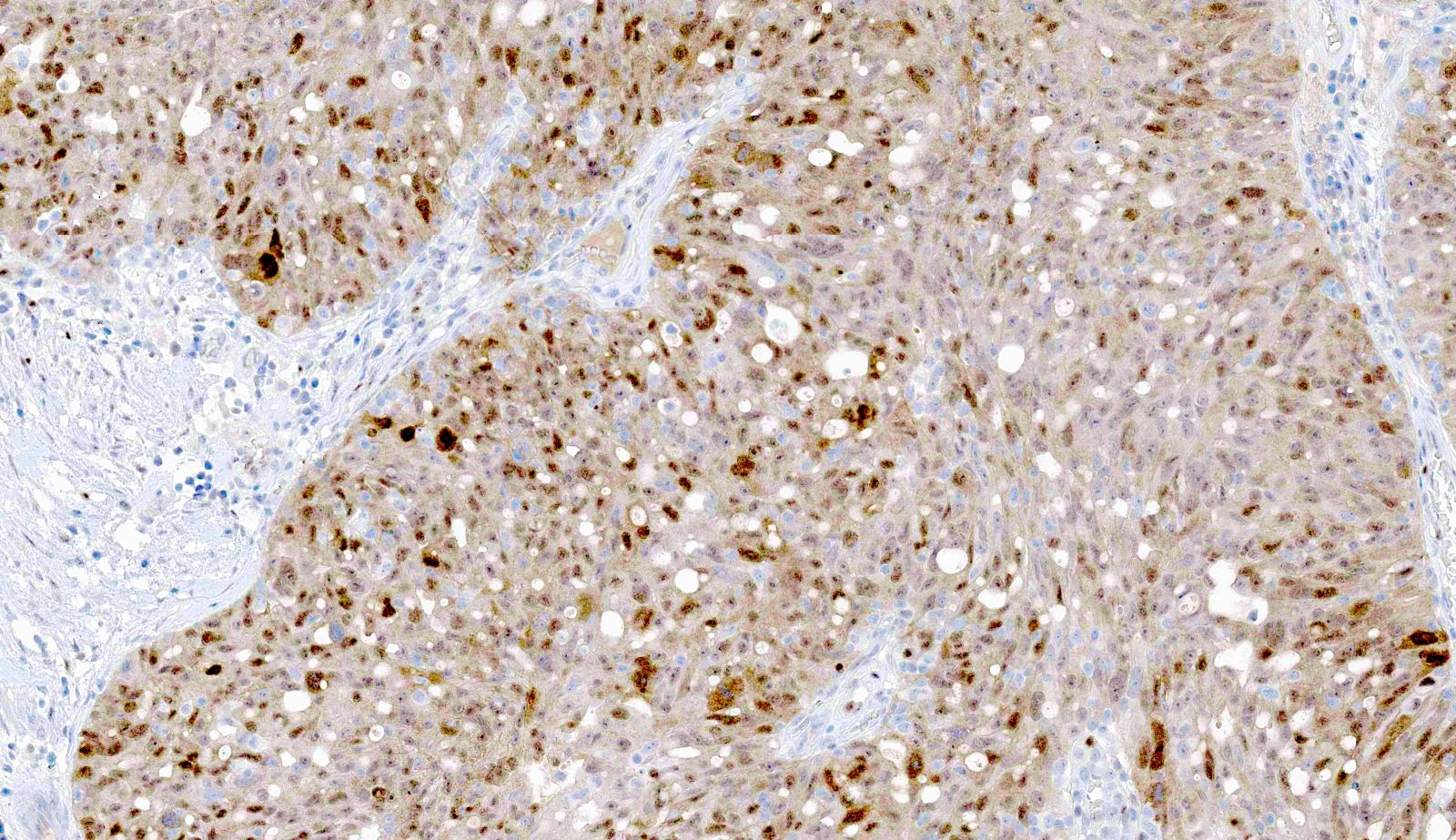
Stains:
Discussion:
Tubo-ovarian high grade serous carcinomas with prominent solid, pseudoendometrioid and transitional cell carcinoma-like morphology (SET features) may be more difficult for pathologists to recognize in comparison to high grade serous carcinomas (HGSCs) with conventional features. So called pseudoendometrioid features are typically characterized by cribriform architecture. HGSCs are usually positive for PAX8, WT1, estrogen receptor, progesterone receptor and p16 by immunohistochemistry, with an aberrant / mutant pattern of p53 staining. Aberrant / mutant staining patterns include overexpression (> 80% of nuclei staining positive), null (complete absence of expression) and, least often, cytoplasmic (with or without nuclear staining) (J Pathol Clin Res 2016;2:247). Of note, < 5% of HGSCs show a non-aberrant / wild type staining pattern due to splice site or truncating mutations resulting in detection of nonfunctional p53 protein. HGSCs with transitional cell carcinoma-like morphology should be differentiated from metastatic urothelial carcinoma. In contrast to HGSC, urothelial carcinoma is usually positive for GATA3 and p63 and negative for WT1 and hormone receptors.
HGSCs with BRCA1 abnormalities more frequently show SET features, higher mitotic indices, more tumor infiltrating lymphocytes (TILs) and geographic or comedonecrosis. HGSCs with BRCA2 abnormalities may show SET features without TILs or necrosis. Among BRCA negative HGSCs, SET features are enriched in younger patients (mean age mid-50s). Perhaps contributing to the diagnostic challenge, HGSCs with predominant SET features are less commonly associated with serous tubal intraepithelial carcinoma (STIC).
While patients with HGSC are often referred to genetic counseling regardless of histomorphology, Poly-ADP ribose polymerase (PARP) inhibitors are more beneficial for treatment of HGSCs with homologous recombination deficiency (HRD), which is measured by the presence of mutations of BRCA genes or other homologous recombination genes or alterations of gene expression leading to genomic instability. In one recent study, the majority of HGSCs with SET features were homologous recombination deficient (HRD), independent of BRCA status, suggesting increased sensitivity to PARP inhibitors. There is also evidence to suggest that HGSC with SET features have more favorable clinical outcomes.
References:
Mod Pathol 2012;25:625, Hum Pathol 2023;141:15, Am J Surg Pathol 2015;39:287
Test question answer:
B. BRCA1. While solid, pseudoendometrioid and transitional (SET) features can be seen in tubo-ovarian high grade serous carcinomas with BRCA2 or RAD51B alterations, answers C and D are incorrect since these features are most commonly seen in tumors with BRCA1 alteration. Answer A is incorrect because ARID1A mutations are commonly seen in endometriosis associated ovarian cancers (endometrioid and clear cell types).
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Stephanie Skala, University of Michigan, Ann Arbor, Michigan, USA for contributing this case and discussion and to Dr. Gulisa Turashvili, Emory University School of Medicine, Atlanta, Georgia, USA for reviewing the discussion.
Website news:
(1) The first quarter PathologyOutlines.com Jobs report for 2024 has been posted here. For this quarter, PathologyOutlines.com listed 398 full or part time pathologist job postings, which form the basis for the statistics within the report.
(2) New Board of Reviewers appointments include Dr. Carla Ellis for Renal Pathology, Dr. Caroline Underwood for Dermatopathology, Dr. Anna Biernacka for Breast Pathology, Dr. Carlos Murga-Zamalloa for Hematopathology and Dr. Jieli (Shirley) Li for Clinical Chemistry.
(3) Dr. Maria Tretiakova, our Deputy Editor-in-Chief for GU Pathology, recently published several articles containing novel and relevant practice information. The articles are available here.
Visit and follow our Blog to see recent updates to the website.
(1) The first quarter PathologyOutlines.com Jobs report for 2024 has been posted here. For this quarter, PathologyOutlines.com listed 398 full or part time pathologist job postings, which form the basis for the statistics within the report.
(2) New Board of Reviewers appointments include Dr. Carla Ellis for Renal Pathology, Dr. Caroline Underwood for Dermatopathology, Dr. Anna Biernacka for Breast Pathology, Dr. Carlos Murga-Zamalloa for Hematopathology and Dr. Jieli (Shirley) Li for Clinical Chemistry.
(3) Dr. Maria Tretiakova, our Deputy Editor-in-Chief for GU Pathology, recently published several articles containing novel and relevant practice information. The articles are available here.
Visit and follow our Blog to see recent updates to the website.
Case of the Month #538
Clinical history:
A 58 year old woman presented with an adnexal mass.
Microscopic images:
What is your diagnosis?
Click here for diagnosis, test question and discussion:
Diagnosis: High grade serous carcinoma with solid, pseudoendometrioid and transitional (SET) features
Test question (answer at the end):
Which gene is most commonly altered in tubo-ovarian high grade serous carcinoma with solid, pseudoendometrioid and transitional (SET) features?
- ARID1A
- BRCA1
- BRCA2
- RAD51B
Stains:
Aberrant p53 expression
Discussion:
Tubo-ovarian high grade serous carcinomas with prominent solid, pseudoendometrioid and transitional cell carcinoma-like morphology (SET features) may be more difficult for pathologists to recognize in comparison to high grade serous carcinomas (HGSCs) with conventional features. So called pseudoendometrioid features are typically characterized by cribriform architecture. HGSCs are usually positive for PAX8, WT1, estrogen receptor, progesterone receptor and p16 by immunohistochemistry, with an aberrant / mutant pattern of p53 staining. Aberrant / mutant staining patterns include overexpression (> 80% of nuclei staining positive), null (complete absence of expression) and, least often, cytoplasmic (with or without nuclear staining) (J Pathol Clin Res 2016;2:247). Of note, < 5% of HGSCs show a non-aberrant / wild type staining pattern due to splice site or truncating mutations resulting in detection of nonfunctional p53 protein. HGSCs with transitional cell carcinoma-like morphology should be differentiated from metastatic urothelial carcinoma. In contrast to HGSC, urothelial carcinoma is usually positive for GATA3 and p63 and negative for WT1 and hormone receptors.
HGSCs with BRCA1 abnormalities more frequently show SET features, higher mitotic indices, more tumor infiltrating lymphocytes (TILs) and geographic or comedonecrosis. HGSCs with BRCA2 abnormalities may show SET features without TILs or necrosis. Among BRCA negative HGSCs, SET features are enriched in younger patients (mean age mid-50s). Perhaps contributing to the diagnostic challenge, HGSCs with predominant SET features are less commonly associated with serous tubal intraepithelial carcinoma (STIC).
While patients with HGSC are often referred to genetic counseling regardless of histomorphology, Poly-ADP ribose polymerase (PARP) inhibitors are more beneficial for treatment of HGSCs with homologous recombination deficiency (HRD), which is measured by the presence of mutations of BRCA genes or other homologous recombination genes or alterations of gene expression leading to genomic instability. In one recent study, the majority of HGSCs with SET features were homologous recombination deficient (HRD), independent of BRCA status, suggesting increased sensitivity to PARP inhibitors. There is also evidence to suggest that HGSC with SET features have more favorable clinical outcomes.
References:
Mod Pathol 2012;25:625, Hum Pathol 2023;141:15, Am J Surg Pathol 2015;39:287
Test question answer:
B. BRCA1. While solid, pseudoendometrioid and transitional (SET) features can be seen in tubo-ovarian high grade serous carcinomas with BRCA2 or RAD51B alterations, answers C and D are incorrect since these features are most commonly seen in tumors with BRCA1 alteration. Answer A is incorrect because ARID1A mutations are commonly seen in endometriosis associated ovarian cancers (endometrioid and clear cell types).