22 November 2023 - Case of the Month #533
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Drs. Azadeh Khayyat and Julie Jorns, Medical College of Wisconsin, Milwaukee, Wisconsin, USA for contributing this case and discussion and to Dr. Gary Tozbikian, Ohio State University Wexner Medical Center, Columbus, Ohio, USA for reviewing the discussion.

Paid advertisement
Case of the Month #533
Clinical history:
A premenopausal woman with family history of breast cancer in paternal and maternal grandmothers presented for first screening mammogram and was found to have a subcentimeter mass with calcifications for which she underwent stereotactic guided core biopsy.
Radiology and histopathology images:



What is your diagnosis?
Diagnosis: Ductal carcinoma in situ (DCIS), solid type, with microcalcifications, confined to a fibroadenoma (0.5 cm), nuclear grade 2; lobular neoplasia (atypical lobular hyperplasia / lobular carcinoma in situ), with involvement of a fibroadenoma
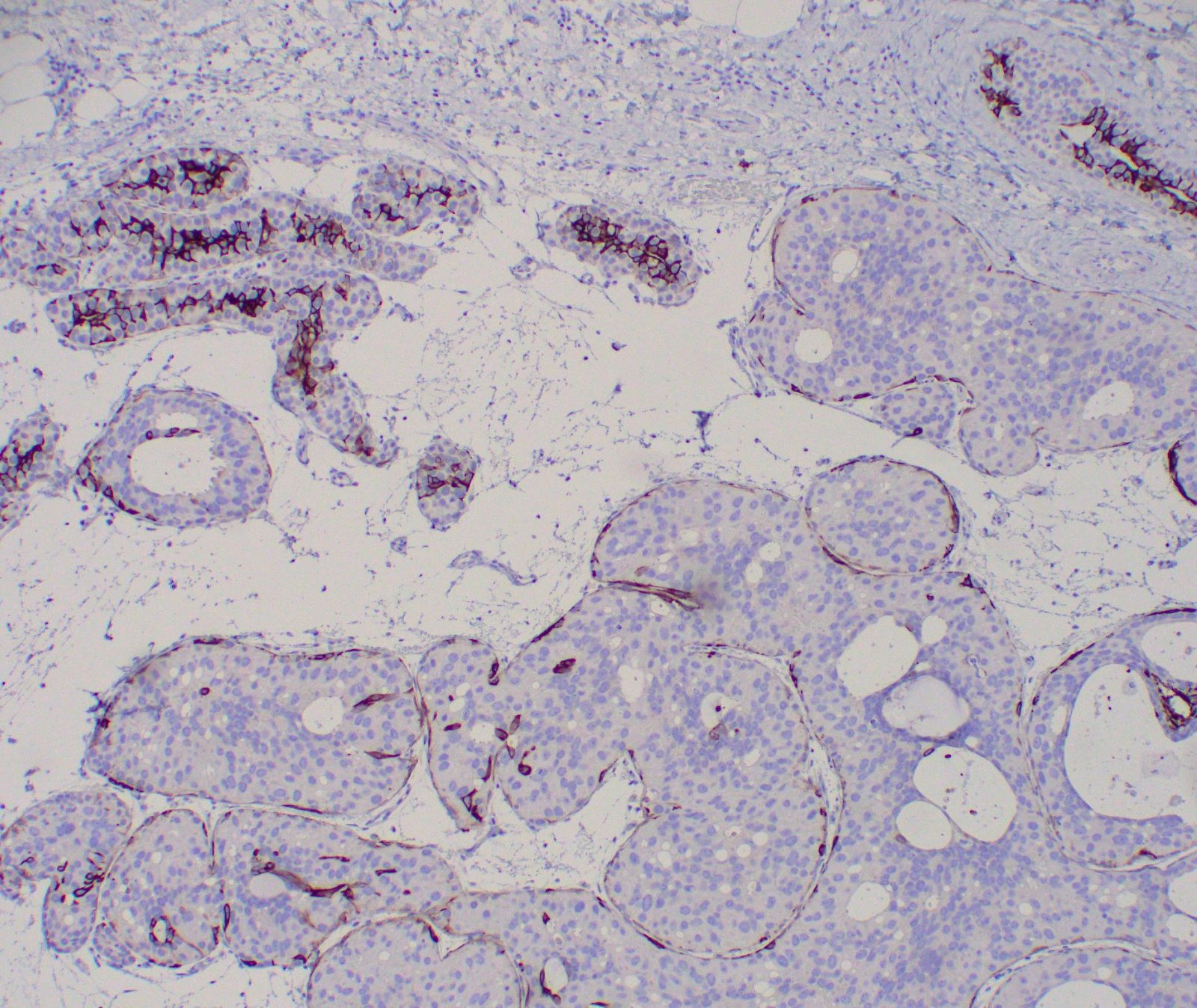
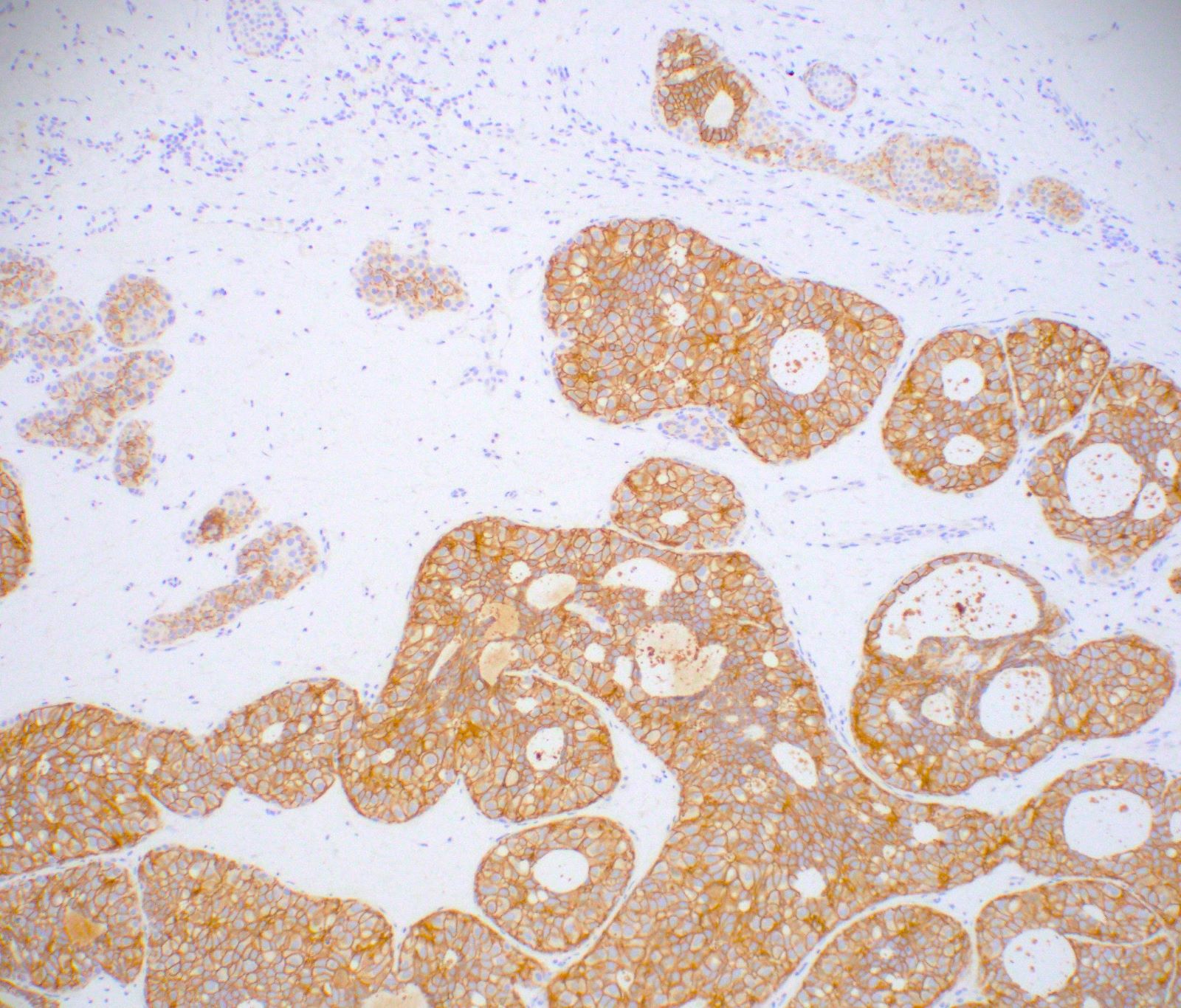
Comment: Immunohistochemistry shows DCIS to be E-cadherin positive and cytokeratin 5/6 negative, while lobular neoplasia is E-cadherin and cytokeratin 5/6 negative, supporting the diagnoses. DCIS is (> 95%, strong) estrogen receptor positive. Controls are appropriate.
Test question (answer at the end):
Fibroadenomas harbor epithelial atypia or malignancy at approximately what rate?
Stains:

Discussion:
Ductal carcinoma in situ (DCIS) is a malignant growth of breast ductal epithelial cells limited to the ductal lobular system without invasion into the surrounding stroma. DCIS is a precursor to invasive breast carcinoma. When compared to the general population, there is a 2 - 8.6 times increased chance of development of ipsilateral invasive breast cancer. On mammogram, pleomorphic calcifications are frequently associated with high grades of DCIS; however, fine or granular calcifications are more common in low grades of DCIS and their distribution is typically clustered or linear. Lobular neoplasia (spectrum of atypical lobular hyperplasia / lobular carcinoma in situ of classic type) also portends an increased bilateral invasive breast cancer risk (4 - 10 times) and does not typically have a breast imaging correlate.
Fibroadenomas infrequently harbor epithelial atypia or carcinoma, with a rate of 1.97% in a recent large study of 1523 consecutive fibroadenomas by Krishnamurthy et al. (Breast Dis 2019;38:97). In their study, there was a relatively equal distribution of atypical ductal hyperplasia (6/30), lobular carcinoma in situ (LCIS) (8/30), DCIS (10/30) and invasive carcinoma (6/30), with LCIS being confined to the fibroadenoma in 62.5% and DCIS being confined to the fibroadenoma in 10% of cases (Breast Dis 2019;38:97). In our case, DCIS was confined to the fibroadenoma and harbored the calcifications noted on mammogram, whereas lobular neoplasia was seen both within and outside of the fibroadenoma.
Test question answer:
B. 2%. The classification and behavior of fibroepithelial tumors of the breast including fibroadenoma and phyllodes tumor is driven by the stroma. However, epithelial changes may be seen and are thought to occur by chance or are driven by unrelated risk factor(s). Thus, epithelial atypia and malignancy is uncommon, with a recent large study by Krishnamurthy et al. showing a rate of ~2% (Breast Dis 2019;38:97).
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Drs. Azadeh Khayyat and Julie Jorns, Medical College of Wisconsin, Milwaukee, Wisconsin, USA for contributing this case and discussion and to Dr. Gary Tozbikian, Ohio State University Wexner Medical Center, Columbus, Ohio, USA for reviewing the discussion.
Paid advertisement
Website news:
(1) New editorial board appointments: Dr. Lucy Ma was appointed to our Editorial Board for Gynecologic Pathology. Dr. David Escobar was recently to the Editorial Board for Gastrointestinal Pathology.
(2) The third quarter Jobs report for 2023 has been posted on our Jobs page. For this quarter, there were 382 job postings at PathologyOutlines.com for full or part time pathologists, which form the basis for the statistics within the report. Click here for full details of the report.
(3) Thank you to everyone who stopped by our booth at CAP 2023 in Chicago. At PathologyOutlines.com, we are all about quality information and we love sharing our platform with you. Head over to our testimonials page at pathologyoutlines.com/Testimonialsgen.html to see the inspiring video testimonials from some of our visitors.
Visit and follow our Blog to see recent updates to the website.
(1) New editorial board appointments: Dr. Lucy Ma was appointed to our Editorial Board for Gynecologic Pathology. Dr. David Escobar was recently to the Editorial Board for Gastrointestinal Pathology.
(2) The third quarter Jobs report for 2023 has been posted on our Jobs page. For this quarter, there were 382 job postings at PathologyOutlines.com for full or part time pathologists, which form the basis for the statistics within the report. Click here for full details of the report.
(3) Thank you to everyone who stopped by our booth at CAP 2023 in Chicago. At PathologyOutlines.com, we are all about quality information and we love sharing our platform with you. Head over to our testimonials page at pathologyoutlines.com/Testimonialsgen.html to see the inspiring video testimonials from some of our visitors.
Visit and follow our Blog to see recent updates to the website.
Case of the Month #533
Clinical history:
A premenopausal woman with family history of breast cancer in paternal and maternal grandmothers presented for first screening mammogram and was found to have a subcentimeter mass with calcifications for which she underwent stereotactic guided core biopsy.
Radiology and histopathology images:
What is your diagnosis?
Click here for diagnosis, test question and discussion:
Diagnosis: Ductal carcinoma in situ (DCIS), solid type, with microcalcifications, confined to a fibroadenoma (0.5 cm), nuclear grade 2; lobular neoplasia (atypical lobular hyperplasia / lobular carcinoma in situ), with involvement of a fibroadenoma
Comment: Immunohistochemistry shows DCIS to be E-cadherin positive and cytokeratin 5/6 negative, while lobular neoplasia is E-cadherin and cytokeratin 5/6 negative, supporting the diagnoses. DCIS is (> 95%, strong) estrogen receptor positive. Controls are appropriate.
Test question (answer at the end):
Fibroadenomas harbor epithelial atypia or malignancy at approximately what rate?
- 0.2%
- 2%
- 20%
- 50%
Stains:
Estrogen receptor
Cytokeratin 5/6
E-cadherin
Discussion:
Ductal carcinoma in situ (DCIS) is a malignant growth of breast ductal epithelial cells limited to the ductal lobular system without invasion into the surrounding stroma. DCIS is a precursor to invasive breast carcinoma. When compared to the general population, there is a 2 - 8.6 times increased chance of development of ipsilateral invasive breast cancer. On mammogram, pleomorphic calcifications are frequently associated with high grades of DCIS; however, fine or granular calcifications are more common in low grades of DCIS and their distribution is typically clustered or linear. Lobular neoplasia (spectrum of atypical lobular hyperplasia / lobular carcinoma in situ of classic type) also portends an increased bilateral invasive breast cancer risk (4 - 10 times) and does not typically have a breast imaging correlate.
Fibroadenomas infrequently harbor epithelial atypia or carcinoma, with a rate of 1.97% in a recent large study of 1523 consecutive fibroadenomas by Krishnamurthy et al. (Breast Dis 2019;38:97). In their study, there was a relatively equal distribution of atypical ductal hyperplasia (6/30), lobular carcinoma in situ (LCIS) (8/30), DCIS (10/30) and invasive carcinoma (6/30), with LCIS being confined to the fibroadenoma in 62.5% and DCIS being confined to the fibroadenoma in 10% of cases (Breast Dis 2019;38:97). In our case, DCIS was confined to the fibroadenoma and harbored the calcifications noted on mammogram, whereas lobular neoplasia was seen both within and outside of the fibroadenoma.
Test question answer:
B. 2%. The classification and behavior of fibroepithelial tumors of the breast including fibroadenoma and phyllodes tumor is driven by the stroma. However, epithelial changes may be seen and are thought to occur by chance or are driven by unrelated risk factor(s). Thus, epithelial atypia and malignancy is uncommon, with a recent large study by Krishnamurthy et al. showing a rate of ~2% (Breast Dis 2019;38:97).