19 October 2023 - Case of the Month #532
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Chunyu Cai, University of Texas Southwestern Medical Center, Dallas, Texas, USA for contributing this case and discussion and to Dr. Jared Ahrendsen, Northwestern University Feinberg School of Medicine, Chicago, Illinois, USA for reviewing the discussion.
Case of the Month #532
Clinical history:
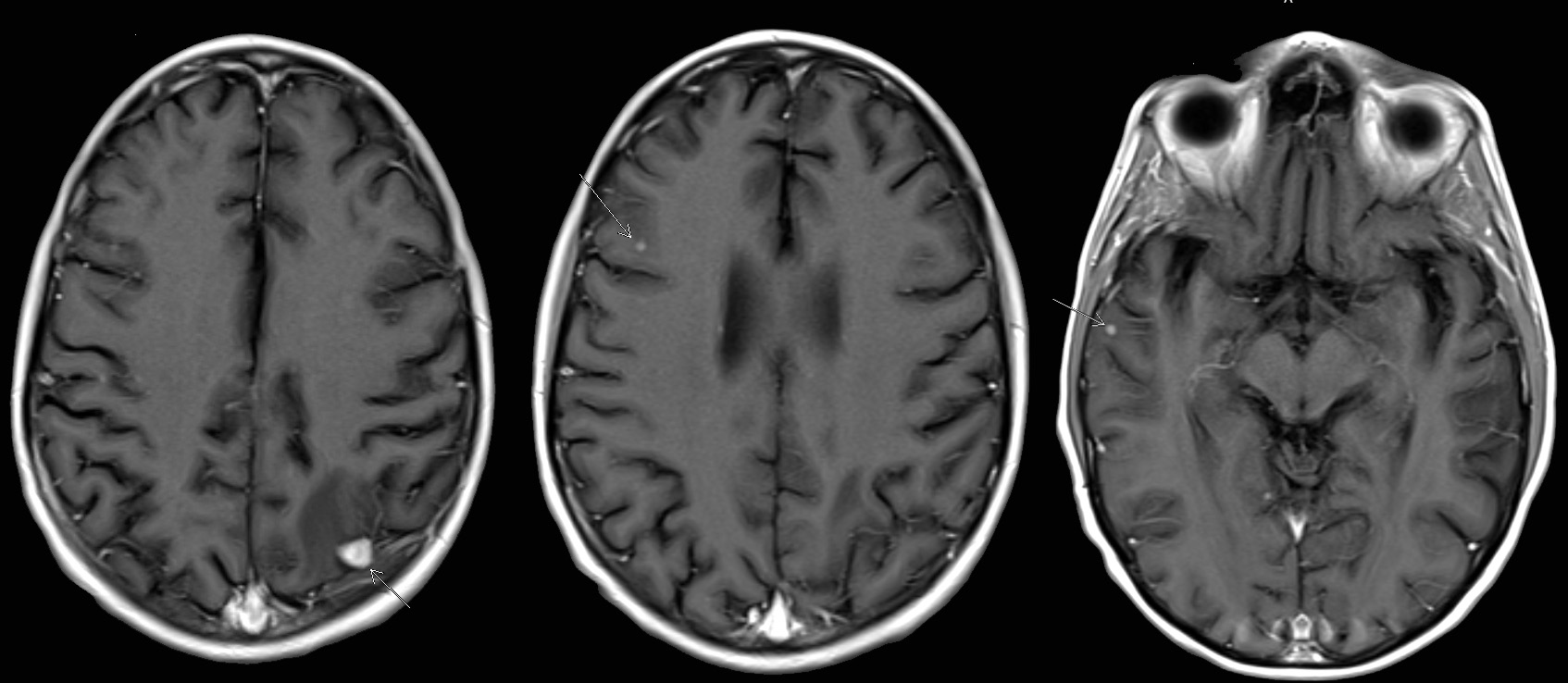
A 52 year old man with a history of HIV infection and Kaposi sarcoma 5 years prior, presented with lower extremity weakness. His CD4 count was low (29). Brain MRI showed multiple enhancing brain lesions, predominantly located at the gray-white interfaces.
Radiology and histopathology images:

What is your diagnosis?
Diagnosis: Mycobacterium associated inflammatory pseudotumor
Test question (answer at the end):
A 52 year old AIDS patient with low CD4 count presented with multiple enhancing brain nodules. Infectious workup revealed disseminated mycobacterium avium intracellulare complex. Biopsy of the brain nodule showed a tumor with mixed spindle and epithelioid cells. What is the mostly likely immunohistochemical profile of this tumor?
A. CD31+, CD68-, SMA-,EBER-, HHV8+
B: CD31-, CD68+, SMA-, EBER-, HHV8-
C: CD31-, CD68-, SMA+, EBER+, HHV8-
D: CD31-, CD68-, S100+, EBER-, HHV8-
Stains:
Discussion:
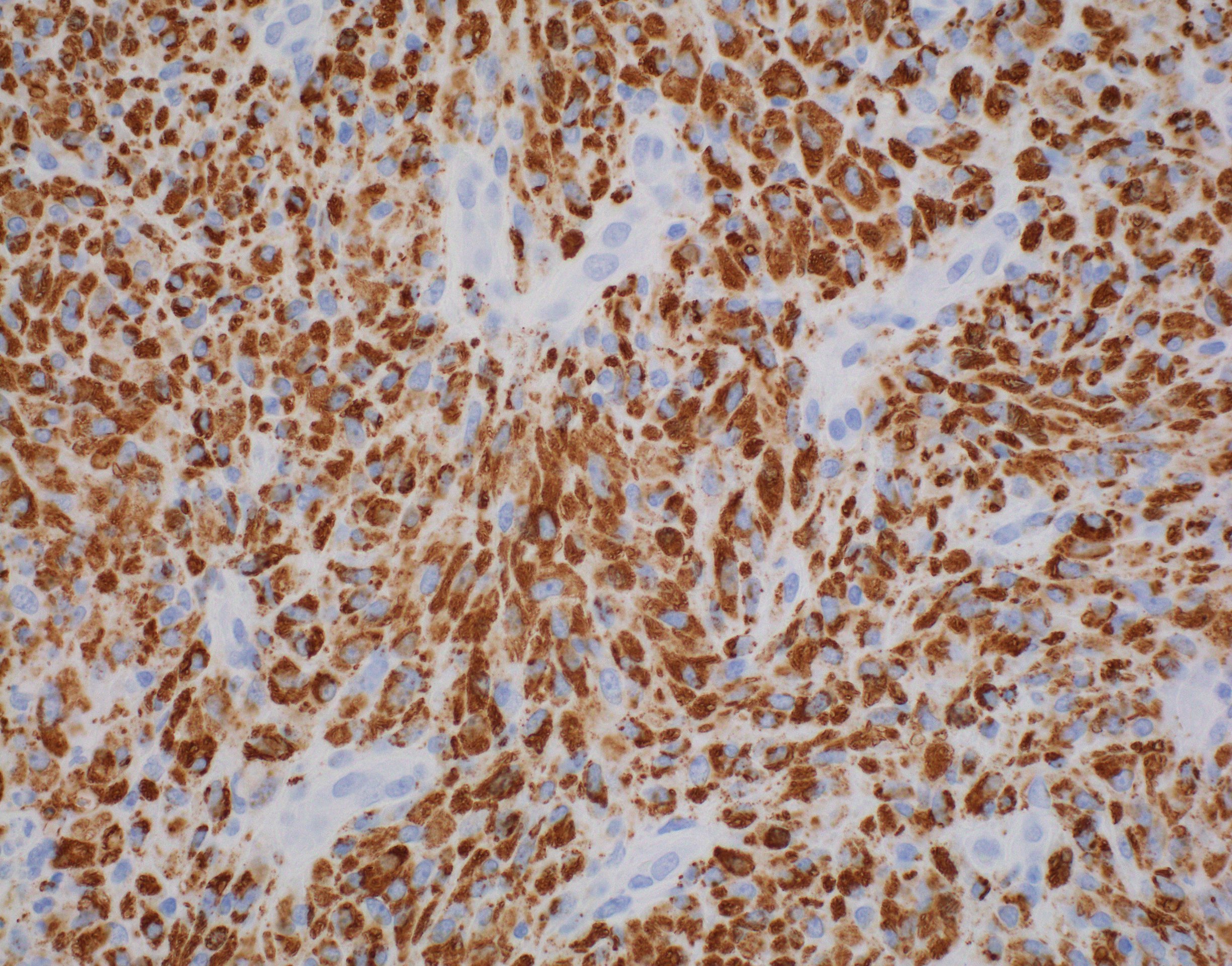
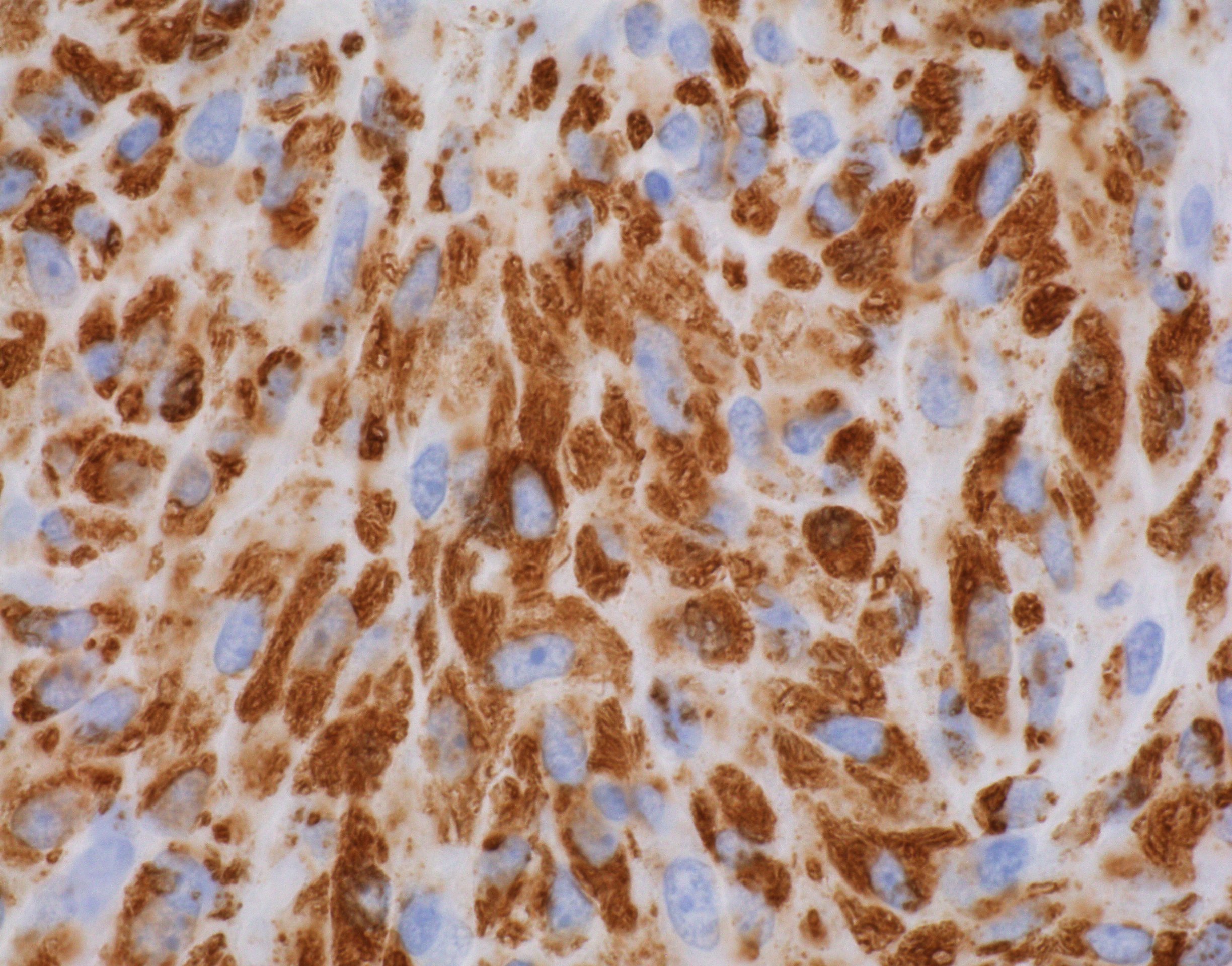
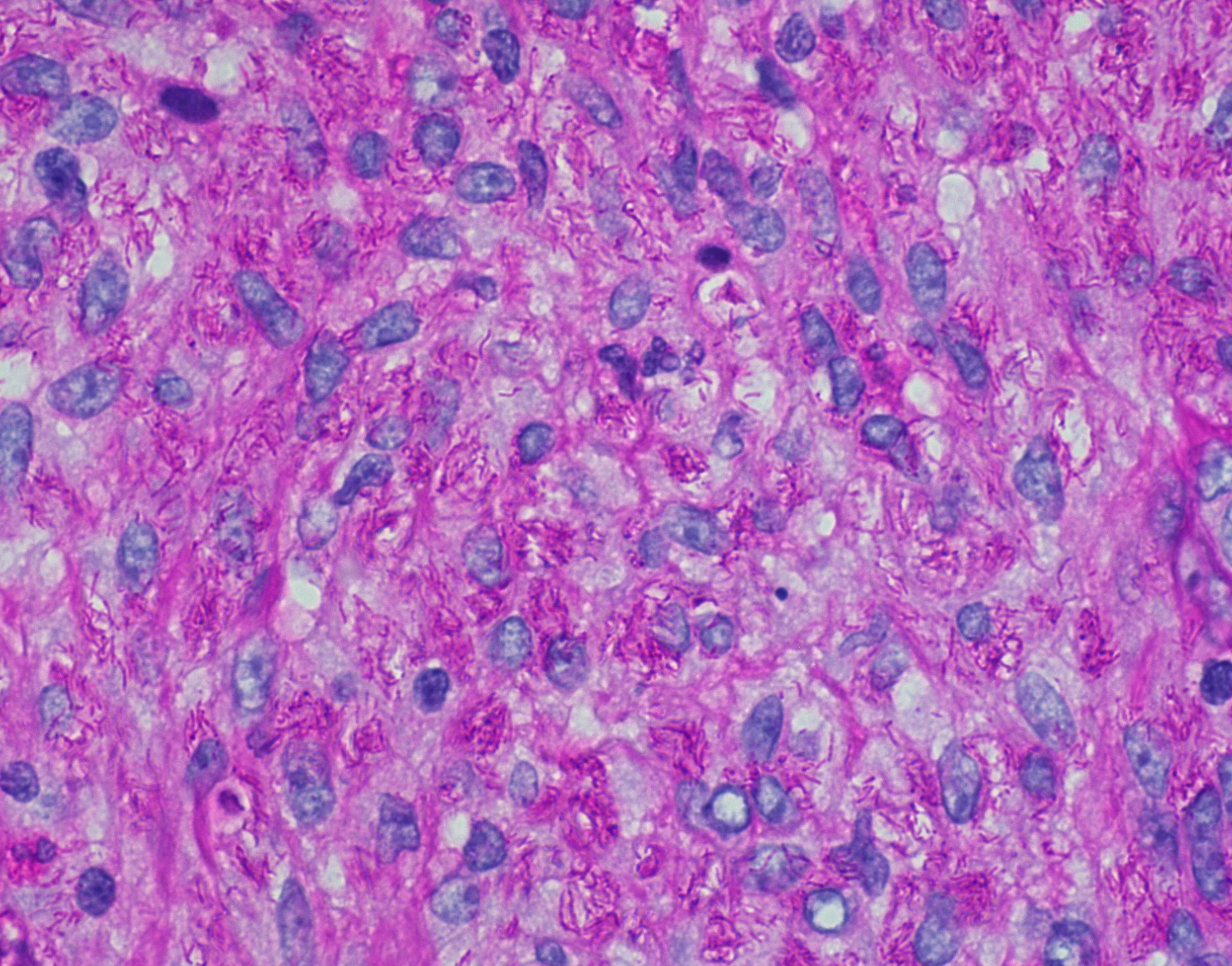
Section shows a spindle cell mass composed of spindle and epithelioid cells intermixed with lymphocytes, neutrophils and plasma cells. No granuloma or caseating necrosis is present. Occasional mitotic figures are present. The spindle and epithelioid tumor cells are diffusely and strongly positive for CD68, patchy for smooth muscle actin and negative for CD34, CD45, HHV8, EBER, desmin, ALK1 IHC. S100 is positive in < 1% of the cells. Ki67 shows a proliferation index of 3 - 5%. Phosphohistone H3 highlights occasional mitotic figures (up to 3/10HPF). These findings excluded the differential considerations of Kaposi sarcoma, EBV associated smooth muscle tumor and inflammatory myofibroblastic tumor.
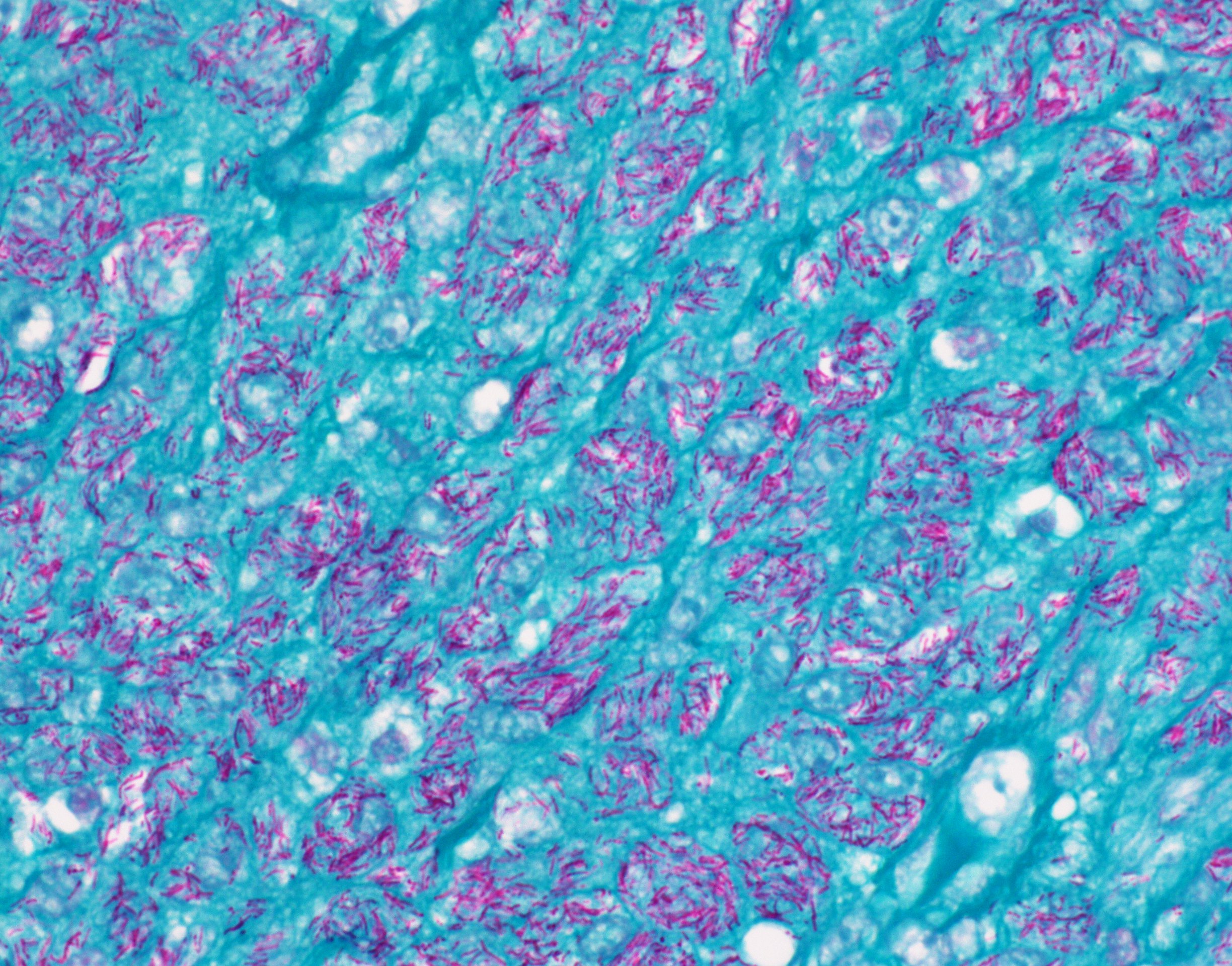
Periodic acid Schiff (PAS) and acid fast bacteria (AFB) stains highlight numerous intracellular mycobacteria bacilli within the mass, which confirm this to be a mycobacteria associated inflammatory pseudotumor. Subsequent culture and workup confirmed disseminated mycobacterium avium intracellulare complex involving multiple systems.
Within the central nervous system, HIV patients can develop several kinds of mixed spindle / epithelioid cell tumors with significant morphological overlap. Those include Kaposi sarcoma, leiomyosarcoma and mycobacterial pseudotumor; all can be multifocal at time of presentation. Mycobacteria pseudotumors often have granular, acidophilic cytoplasm and are strongly positive for CD68 but negative for vascular or smooth muscle markers. These granules are composed of mycobacterium avium intracellulare complex (MAC) which are highlighted by AFB or PAS special stains. Kaposi sarcomas have a more prominent fascicular arrangement of spindle cells and slit-like spaces and are positive for vascular markers CD31 and CD34, as well as herpes virus HHV8 but negative for S100 and CD68 (Am J Surg Pathol 1999;23:656). Primary CNS leiomyosarcomas in the HIV patient setting are mostly EBV driven and positive for EBER in addition to smooth muscle markers. These tumors are thought to arise from the mesenchymal cells of the dura mater or blood vessels and occur in HIV patients with low CD4 counts (Int J Clin Oncol 2011;16:63).
Test question answer:
B. CD31-, CD68+, SMA-, EBER-, HHV8-. This describes mycobacteria pseudotumor. Answer A is incorrect because it describes Kaposi sarcoma. Answer C is incorrect because it describes leiomyosarcoma. Answer D is incorrect because it describes schwannoma.
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Chunyu Cai, University of Texas Southwestern Medical Center, Dallas, Texas, USA for contributing this case and discussion and to Dr. Jared Ahrendsen, Northwestern University Feinberg School of Medicine, Chicago, Illinois, USA for reviewing the discussion.
Case of the Month #532
Clinical history:
A 52 year old man with a history of HIV infection and Kaposi sarcoma 5 years prior, presented with lower extremity weakness. His CD4 count was low (29). Brain MRI showed multiple enhancing brain lesions, predominantly located at the gray-white interfaces.
Radiology and histopathology images:
What is your diagnosis?
Click here for diagnosis, test question and discussion:
Diagnosis: Mycobacterium associated inflammatory pseudotumor
Test question (answer at the end):
A 52 year old AIDS patient with low CD4 count presented with multiple enhancing brain nodules. Infectious workup revealed disseminated mycobacterium avium intracellulare complex. Biopsy of the brain nodule showed a tumor with mixed spindle and epithelioid cells. What is the mostly likely immunohistochemical profile of this tumor?
A. CD31+, CD68-, SMA-,EBER-, HHV8+
B: CD31-, CD68+, SMA-, EBER-, HHV8-
C: CD31-, CD68-, SMA+, EBER+, HHV8-
D: CD31-, CD68-, S100+, EBER-, HHV8-
Stains:
CD68
CD68
PAS
AFB
Discussion:
Section shows a spindle cell mass composed of spindle and epithelioid cells intermixed with lymphocytes, neutrophils and plasma cells. No granuloma or caseating necrosis is present. Occasional mitotic figures are present. The spindle and epithelioid tumor cells are diffusely and strongly positive for CD68, patchy for smooth muscle actin and negative for CD34, CD45, HHV8, EBER, desmin, ALK1 IHC. S100 is positive in < 1% of the cells. Ki67 shows a proliferation index of 3 - 5%. Phosphohistone H3 highlights occasional mitotic figures (up to 3/10HPF). These findings excluded the differential considerations of Kaposi sarcoma, EBV associated smooth muscle tumor and inflammatory myofibroblastic tumor.
Periodic acid Schiff (PAS) and acid fast bacteria (AFB) stains highlight numerous intracellular mycobacteria bacilli within the mass, which confirm this to be a mycobacteria associated inflammatory pseudotumor. Subsequent culture and workup confirmed disseminated mycobacterium avium intracellulare complex involving multiple systems.
Within the central nervous system, HIV patients can develop several kinds of mixed spindle / epithelioid cell tumors with significant morphological overlap. Those include Kaposi sarcoma, leiomyosarcoma and mycobacterial pseudotumor; all can be multifocal at time of presentation. Mycobacteria pseudotumors often have granular, acidophilic cytoplasm and are strongly positive for CD68 but negative for vascular or smooth muscle markers. These granules are composed of mycobacterium avium intracellulare complex (MAC) which are highlighted by AFB or PAS special stains. Kaposi sarcomas have a more prominent fascicular arrangement of spindle cells and slit-like spaces and are positive for vascular markers CD31 and CD34, as well as herpes virus HHV8 but negative for S100 and CD68 (Am J Surg Pathol 1999;23:656). Primary CNS leiomyosarcomas in the HIV patient setting are mostly EBV driven and positive for EBER in addition to smooth muscle markers. These tumors are thought to arise from the mesenchymal cells of the dura mater or blood vessels and occur in HIV patients with low CD4 counts (Int J Clin Oncol 2011;16:63).
Test question answer:
B. CD31-, CD68+, SMA-, EBER-, HHV8-. This describes mycobacteria pseudotumor. Answer A is incorrect because it describes Kaposi sarcoma. Answer C is incorrect because it describes leiomyosarcoma. Answer D is incorrect because it describes schwannoma.