19 January 2022 - Case of the Month #511
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Daniel Athanazio, Federal University of Bahia, Salvador, Bahia, Brazil and the Genitourinary Pathology Society (GUPS), for contributing this case and discussion and to Dr. Debra Zynger, Ohio State University, Columbus, Ohio, USA for reviewing the discussion.

Advertisement
Case of the Month #511
Clinical history:
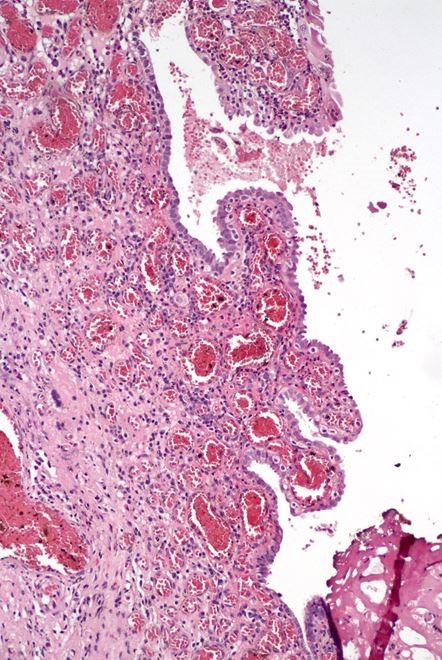
A woman in her 80s with gross hematuria and a clinical suspicion of chronic cystitis underwent cystoscopy which showed multifocal erythema and erosions. She had no prior bladder surgery or instrumentation. She underwent transurethral resection, which showed several papillary lesions, the largest 2.6 mm.
Histopathology images:



What is your diagnosis?
Diagnosis: Nephrogenic adenoma (metaplasia)
Test question (answer at the end):
Which statement is true about nephrogenic adenoma?
A. Can have a flat, single cell layer growth pattern
B. Consists almost exclusively of papillary growth pattern
C. p63 is often positive
D. Stromal invasion is common
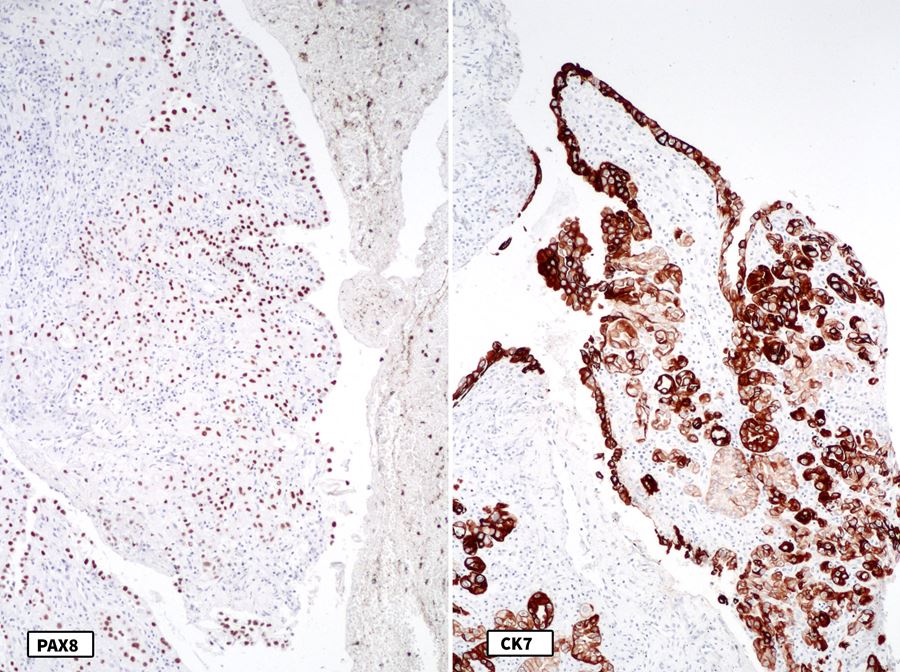
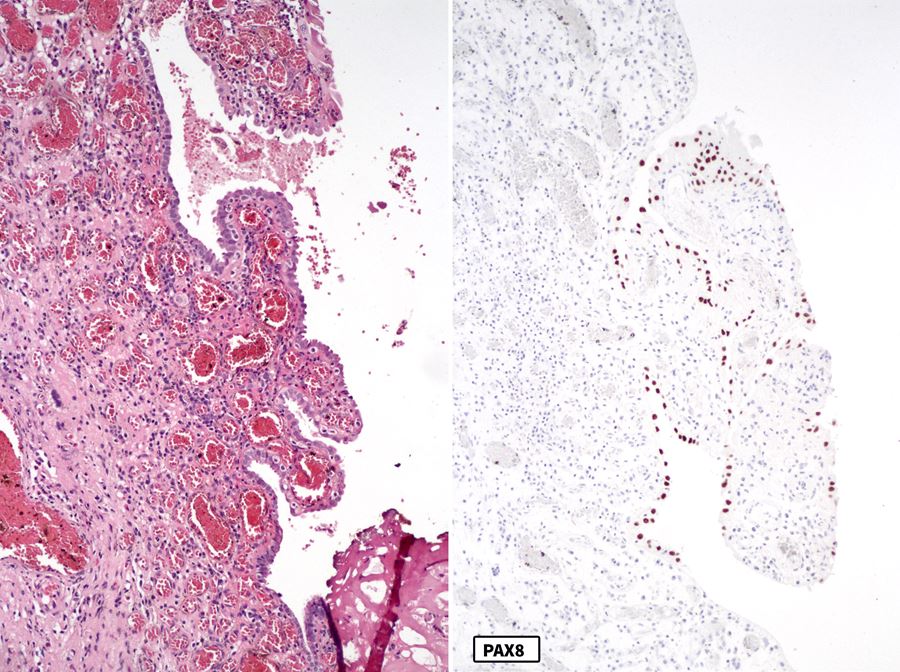
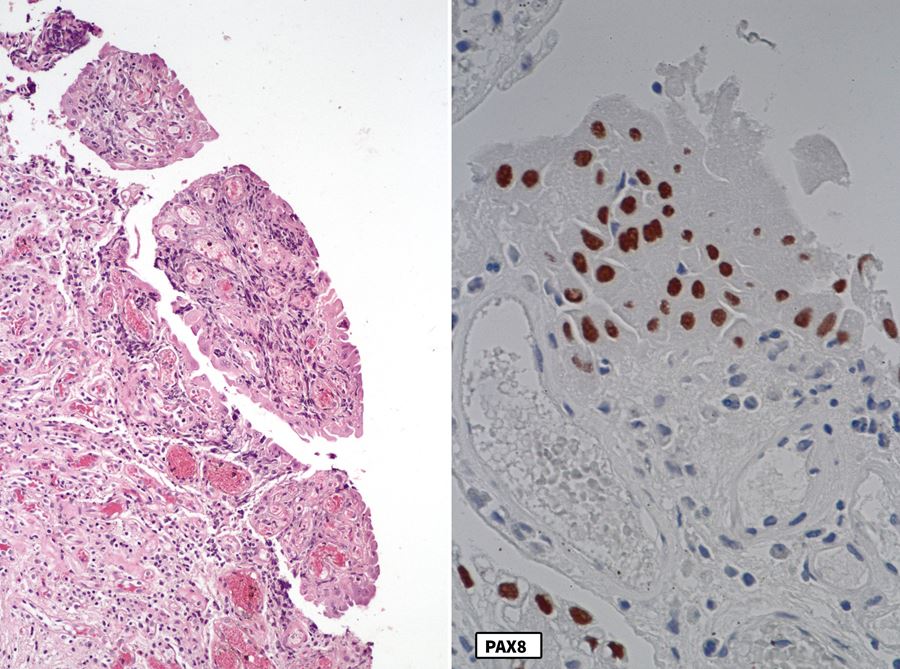
Stains:
Discussion:
Nephrogenic adenoma (metaplasia) is a non-neoplastic polypoid, papillary, fungating or velvety lesion found in urothelial lined tissue, such as the bladder or prostate. It occurs after urothelial injury and is more common in men. Although previously thought to be a clonal neoplasm, it actually is derived from displaced renal tubular epithelial cells (N Engl J Med 2002;347:653).
Nephrogenic adenoma has multiple growth patterns, including papillary, tubular and solid, which were all present in this case. The tubular pattern mimics prostatic adenocarcinoma and microcystic urothelial carcinoma. Typically, a hyalinized rim surrounds the tubules. It can also grow as flat, single layer of cells - a distinct morphologic presentation of nephrogenic adenoma that has been recently described (see second figure in Stains) (Mod Pathol 2013;26:792). This pattern can mimic urothelial carcinoma in situ. Clear cells are rare and there is no mitotic activity. The proliferation may focally involve the muscularis propria.
The cells are diffusely positive for PAX8 and cytokeratin 7 and negative for GATA3 and p63 (not shown). Note that these lesions may be positive for AMACR and negative for basal cell markers, causing confusion with prostatic adenocarcinoma.
Treatment is transurethral resection and as the lesions can recur, follow up may be recommended.
Test question answer:
A. Can have a flat, single cell layer growth pattern
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Daniel Athanazio, Federal University of Bahia, Salvador, Bahia, Brazil and the Genitourinary Pathology Society (GUPS), for contributing this case and discussion and to Dr. Debra Zynger, Ohio State University, Columbus, Ohio, USA for reviewing the discussion.
Advertisement
Case of the Month #511
Clinical history:
A woman in her 80s with gross hematuria and a clinical suspicion of chronic cystitis underwent cystoscopy which showed multifocal erythema and erosions. She had no prior bladder surgery or instrumentation. She underwent transurethral resection, which showed several papillary lesions, the largest 2.6 mm.
Histopathology images:
What is your diagnosis?
Click here for diagnosis, test question and discussion:
Diagnosis: Nephrogenic adenoma (metaplasia)
Test question (answer at the end):
Which statement is true about nephrogenic adenoma?
A. Can have a flat, single cell layer growth pattern
B. Consists almost exclusively of papillary growth pattern
C. p63 is often positive
D. Stromal invasion is common
Stains:
PAX8 / CK7
PAX8
PAX8
Discussion:
Nephrogenic adenoma (metaplasia) is a non-neoplastic polypoid, papillary, fungating or velvety lesion found in urothelial lined tissue, such as the bladder or prostate. It occurs after urothelial injury and is more common in men. Although previously thought to be a clonal neoplasm, it actually is derived from displaced renal tubular epithelial cells (N Engl J Med 2002;347:653).
Nephrogenic adenoma has multiple growth patterns, including papillary, tubular and solid, which were all present in this case. The tubular pattern mimics prostatic adenocarcinoma and microcystic urothelial carcinoma. Typically, a hyalinized rim surrounds the tubules. It can also grow as flat, single layer of cells - a distinct morphologic presentation of nephrogenic adenoma that has been recently described (see second figure in Stains) (Mod Pathol 2013;26:792). This pattern can mimic urothelial carcinoma in situ. Clear cells are rare and there is no mitotic activity. The proliferation may focally involve the muscularis propria.
The cells are diffusely positive for PAX8 and cytokeratin 7 and negative for GATA3 and p63 (not shown). Note that these lesions may be positive for AMACR and negative for basal cell markers, causing confusion with prostatic adenocarcinoma.
Treatment is transurethral resection and as the lesions can recur, follow up may be recommended.
Test question answer:
A. Can have a flat, single cell layer growth pattern