19 November 2021 - Case of the Month #509
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Kyle Haggerty (M.D. candidate) and Dr. David Loeffler, Oregon Health & Science University, Portland, Oregon (USA) for contributing this case and the discussion and to Dr. Debra Zynger, The Ohio State University Wexner Medical Center, Columbus, Ohio (USA), for reviewing the discussion.

Advertisement
Case of the Month #509
Clinical history:
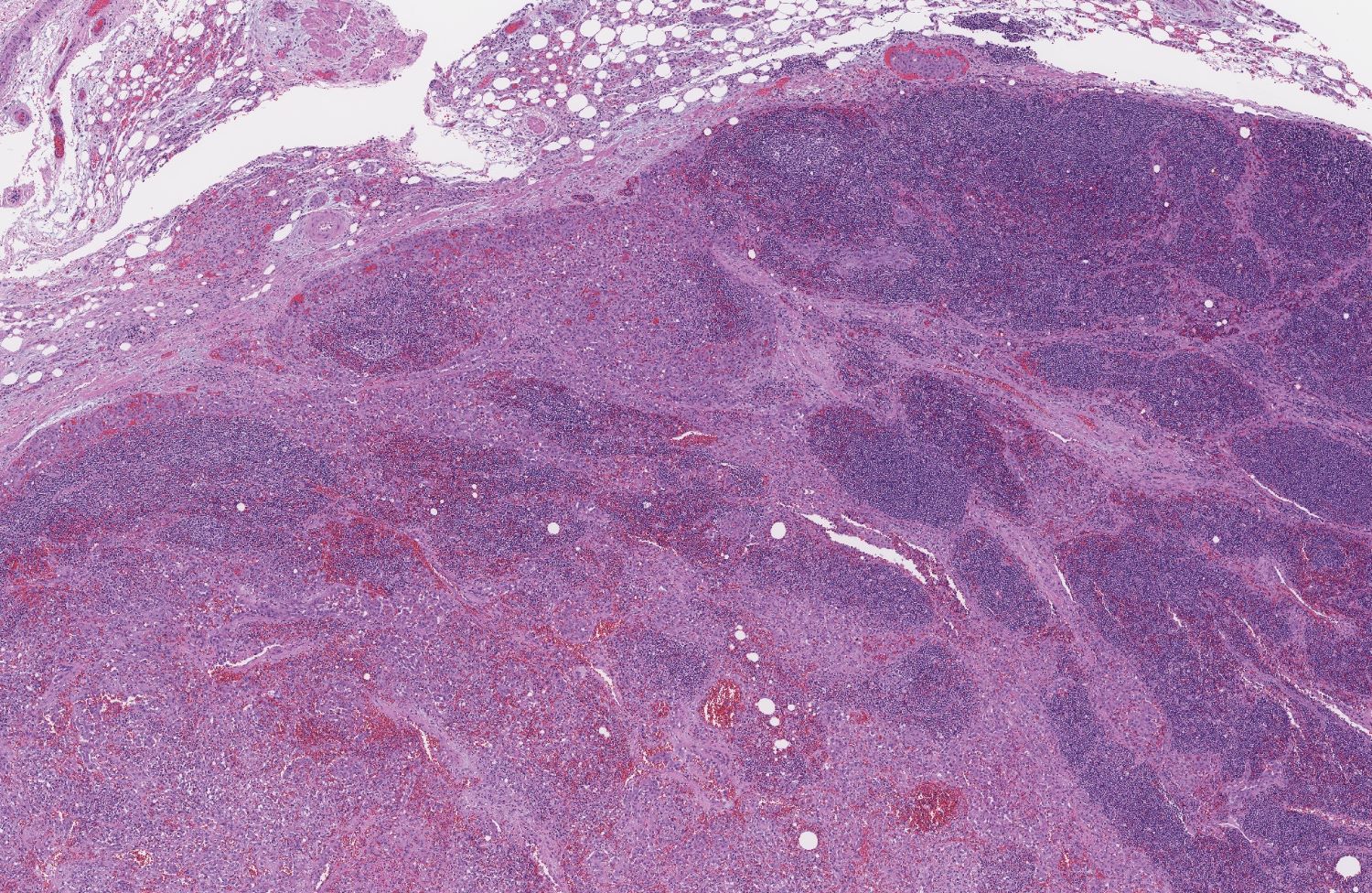
The patient is a 71 year old, otherwise healthy woman, with an incidental finding of an 11.7 cm, heterogeneously enhancing mass involving the right adrenal gland. A core biopsy of the mass was performed and read as an undifferentiated carcinoma, prompting resection. During the operation, the mass was found to be adherent to the right hemidiaphragm, liver and superior vena cava.
Histopathology images:

What is your diagnosis?
Diagnosis: Epithelioid angiosarcoma, involving the adrenal gland
Test question (answer at the end):
Which stain will help differentiate epithelioid angiosarcoma from a poorly differentiated adrenal cortical carcinoma?
A. ERG
B. Pancytokeratin
C. SF1
D. VEGFR3
E. Vimentin
IHC stains obtained:
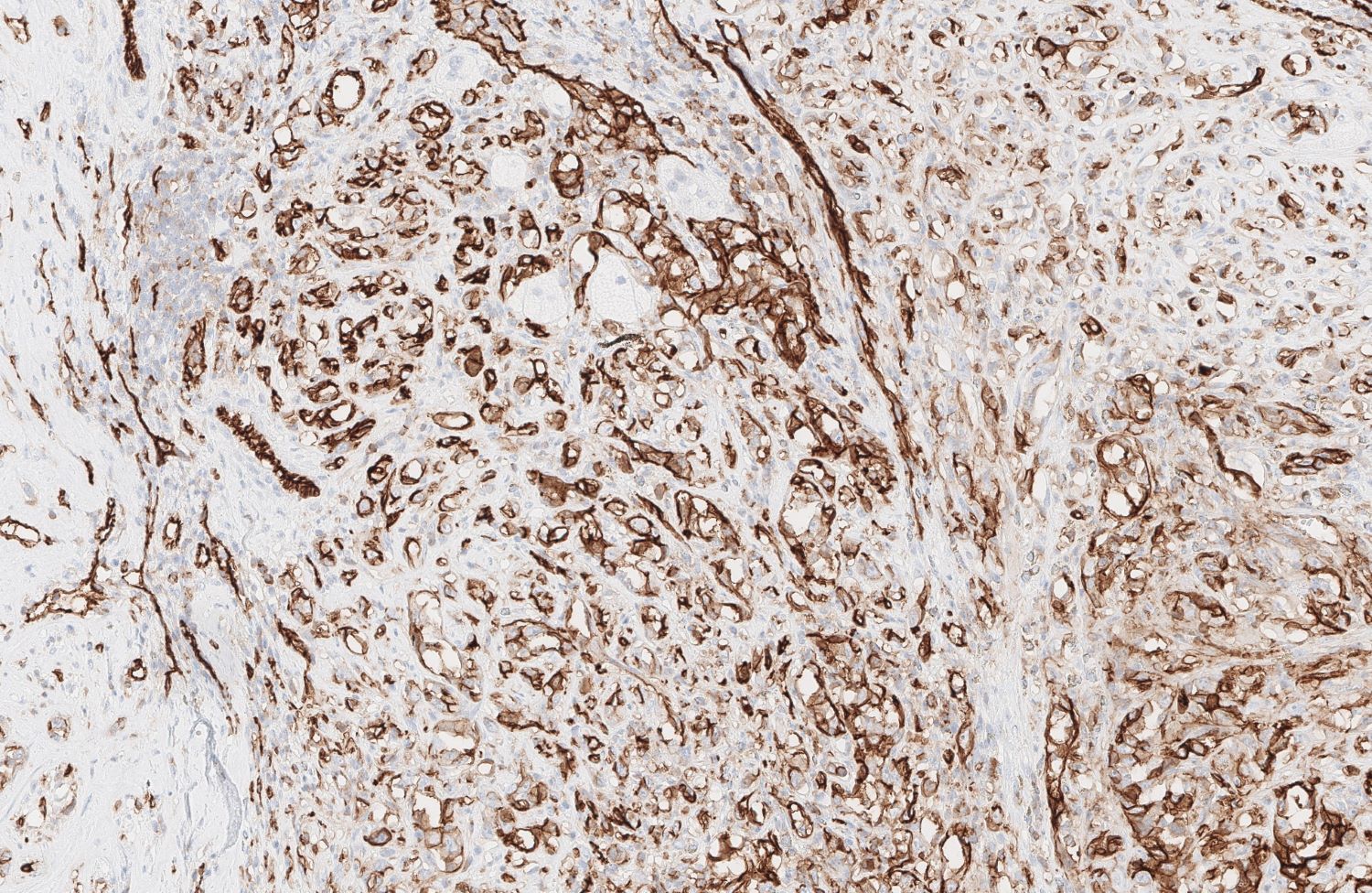
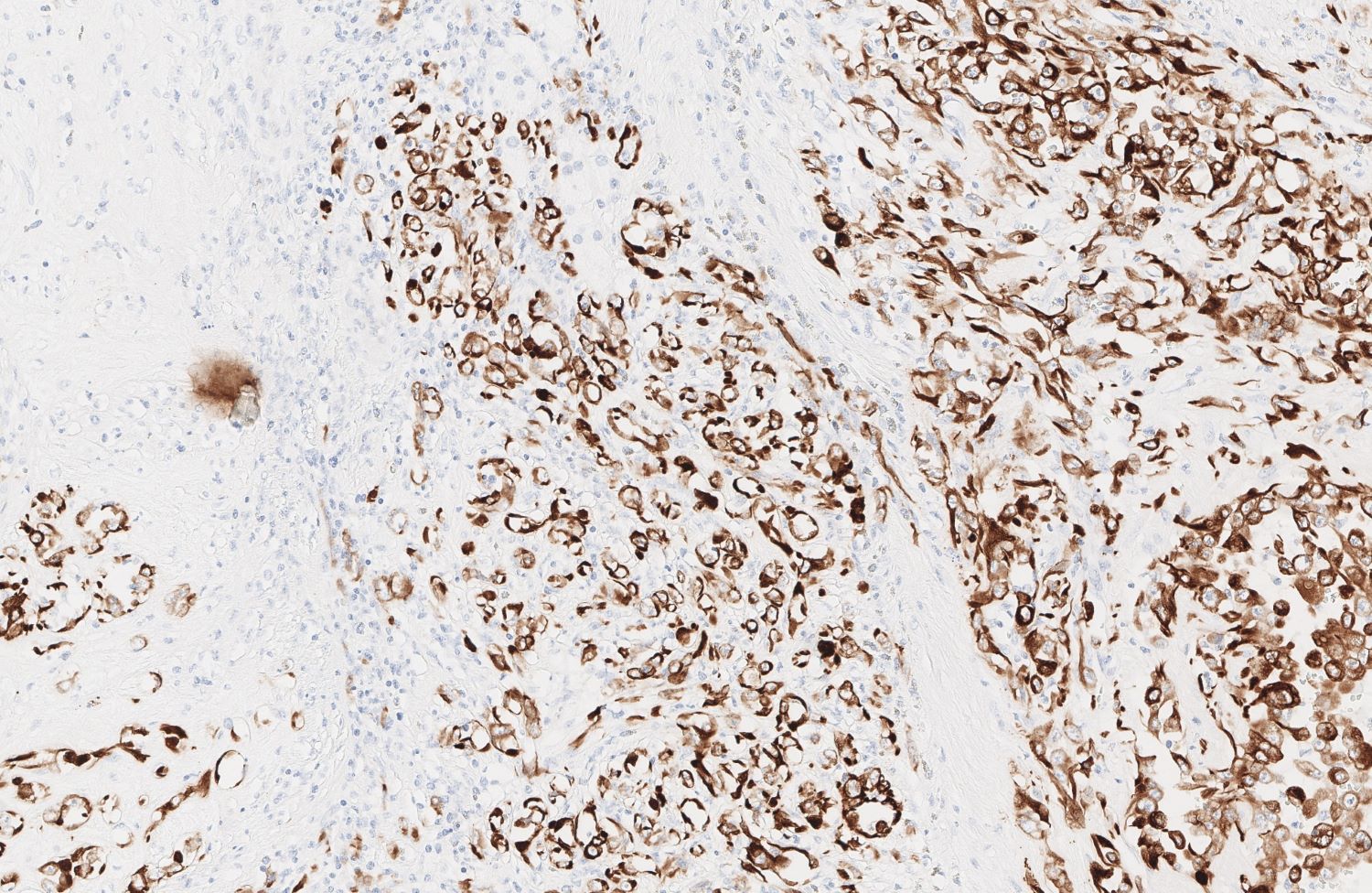
Positive: ERG, CD31, Factor VIII related protein, FLI1, thrombomodulin, CD34, KIT, Vimentin, Keratin
Variable: VEGFR3

Discussion:
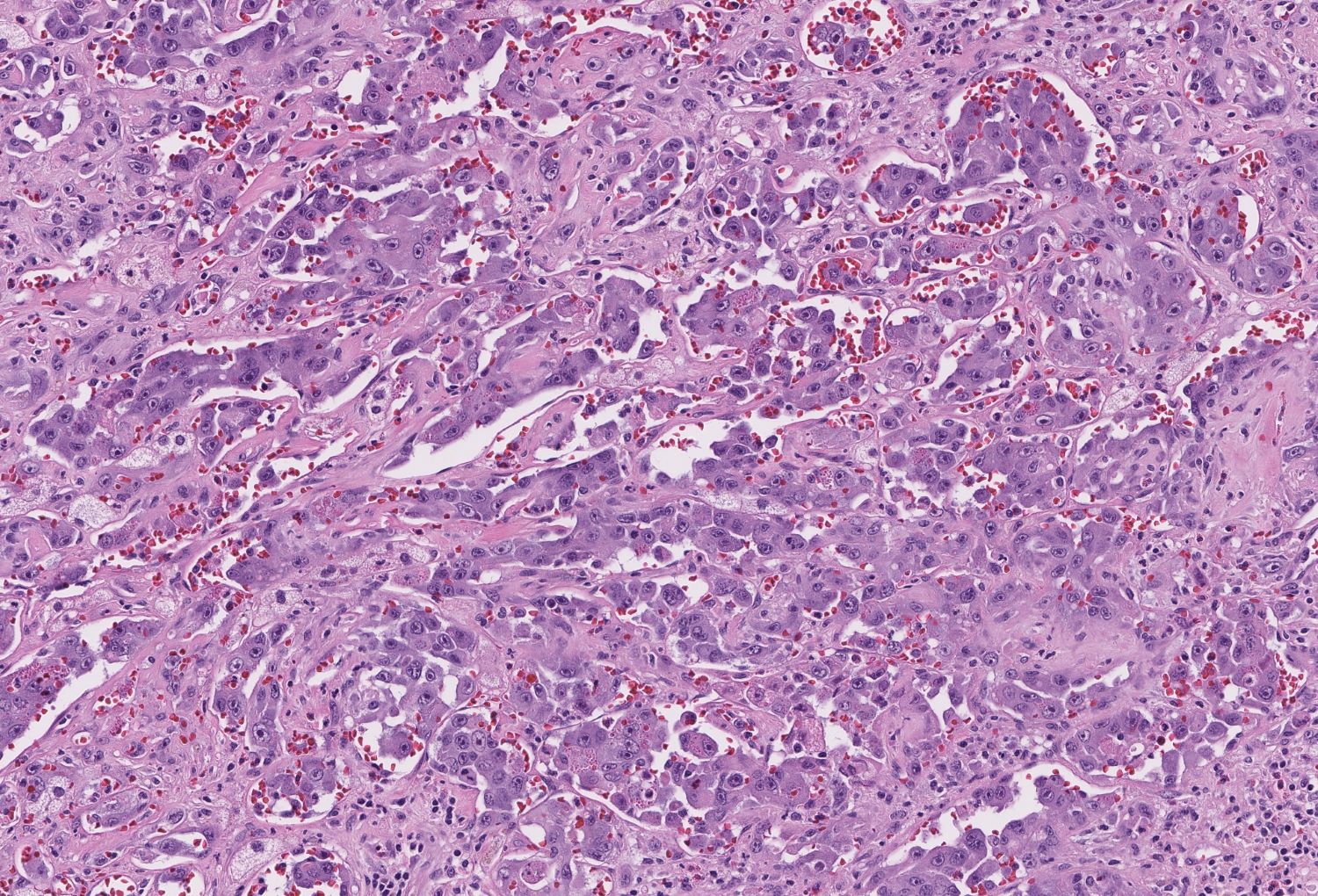
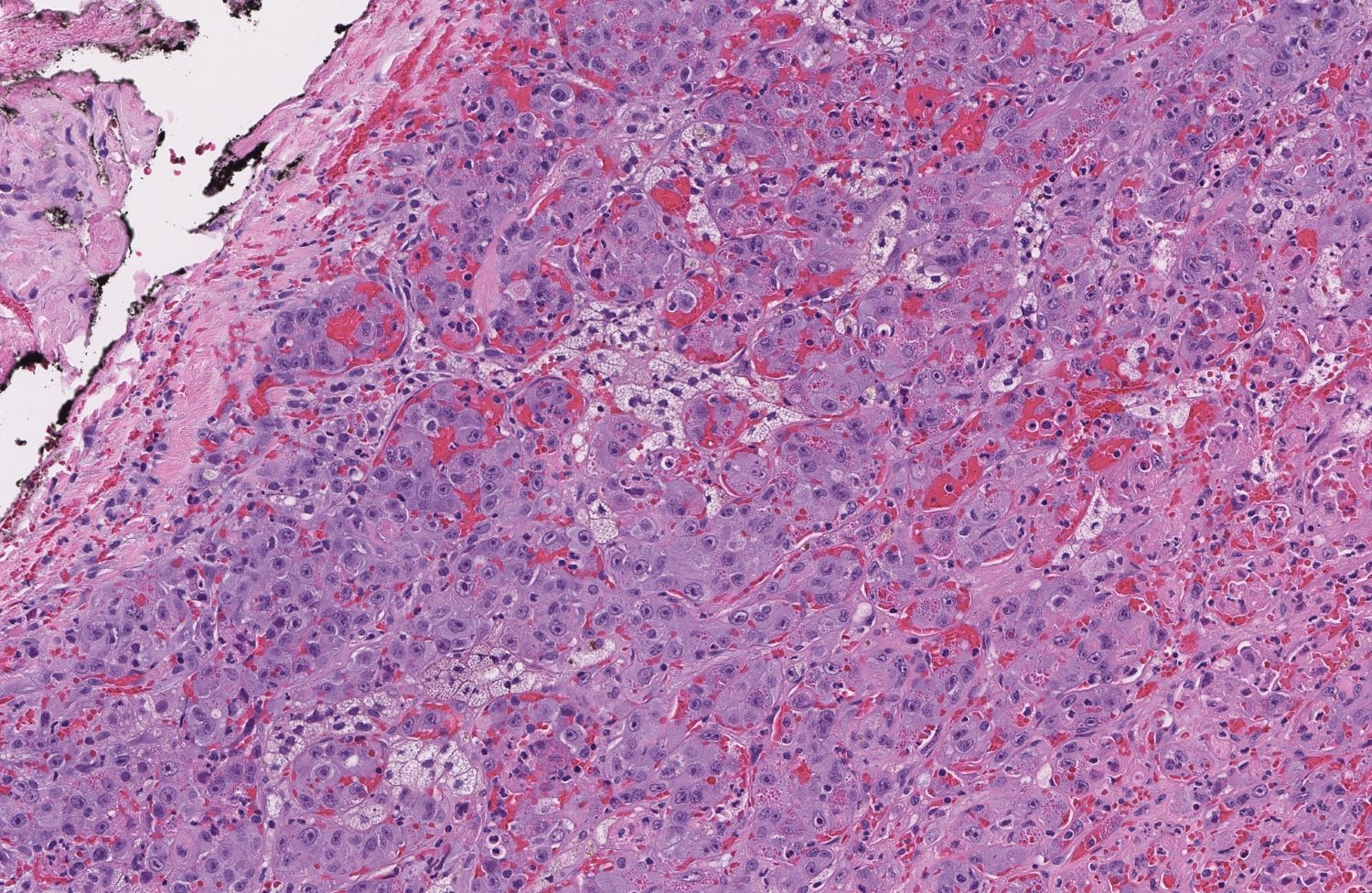
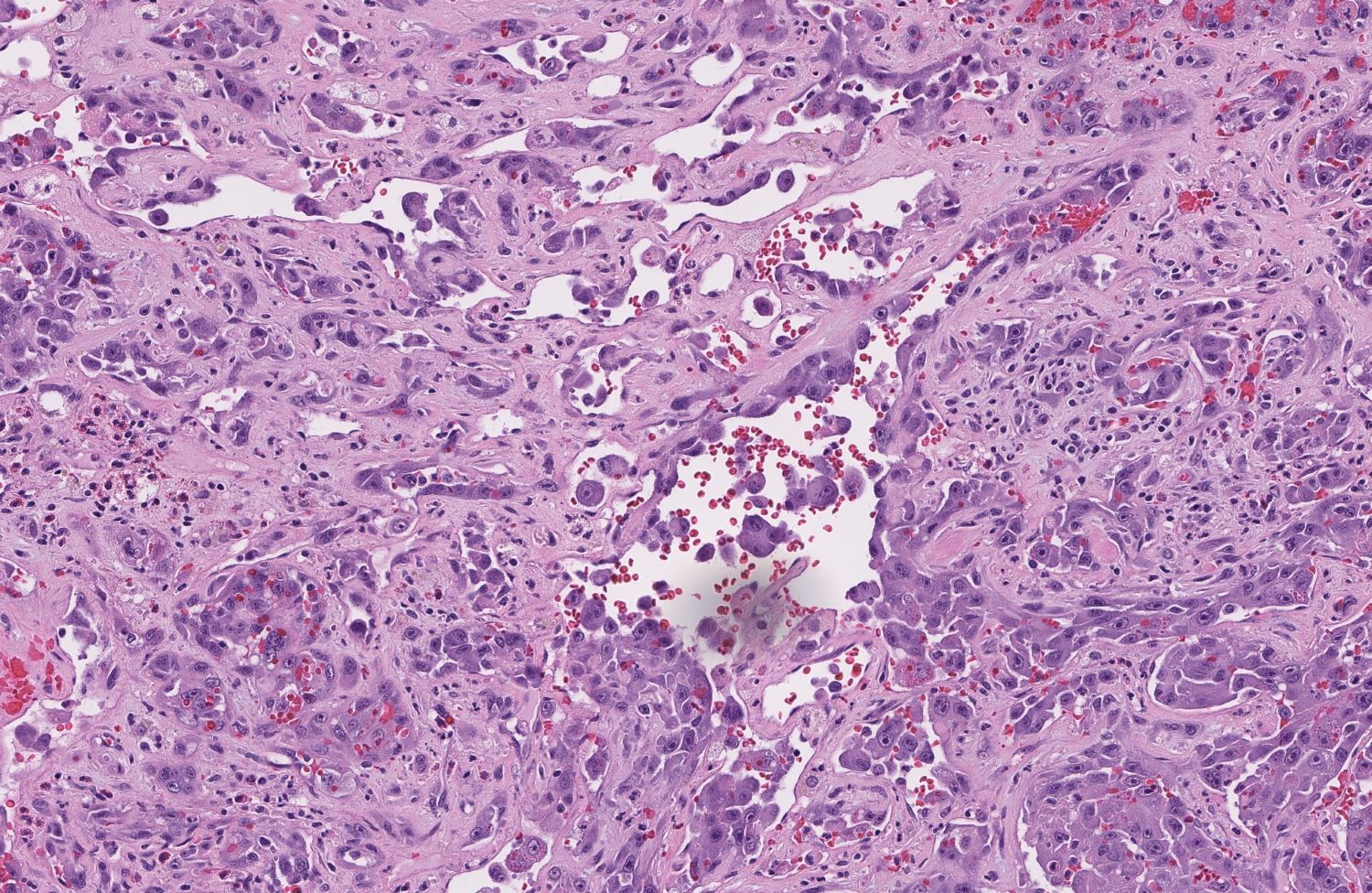
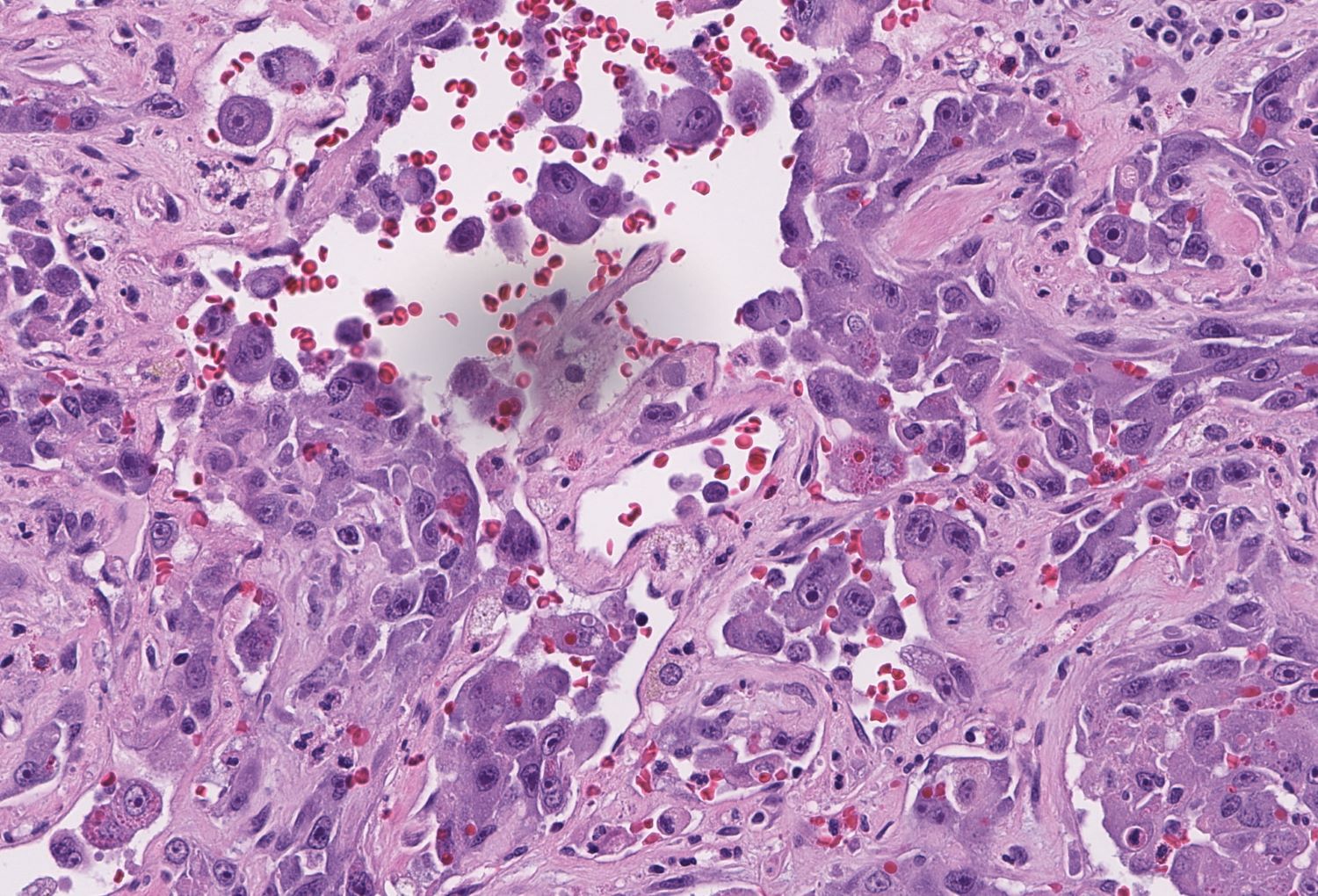
The tumor in this case is highly pleomorphic and was initially diagnosed as undifferentiated carcinoma on biopsy. The differential diagnosis included poorly differentiated adrenal cortical carcinoma, melanoma and sarcoma. On H&E, clues to the final diagnosis are the foci with vasoformative morphology scattered throughout the tumor. Staining shows neoplastic cells positive for ERG and CD31, highlighting vascular structures and the overall vascular differentiation of this tumor.
Adrenal tumors are relatively common, with 4% of abdominal CTs and 8% of autopsies revealing an adrenal mass. The majority of incidentally discovered adrenal masses are small (< 1.0 cm) benign masses, colloquially termed "incidentalomas". Clinical suspicion for malignancy, symptoms of a hyperfunctional adrenal tissue, or mass size > 1.0 cm warrants further workup (Cancer Control 2017;24:198). For our patient, tumor size, heterogeneity and proximity to adjacent structures necessitated further workup and resection.
Angiosarcoma is a rare, aggressive, malignant tumor arising from vascular endothelium. Angiosarcoma of the adrenal gland is exceedingly rare (Am J Surg Pathol 1994;18:62). Less than 1% of all soft tissue sarcomas are angiosarcomas; even that small percentage typically arise from the breast, skin, spleen, bone, kidney, thyroid or liver (Cancer Control 2017;24:198, Arch Pathol Lab Med 2011;135:268, angiosarcoma). Angiosarcomas are most common in older adult males and when they do arise in children or younger adults, the prognosis is notably poor. Risk factors include chronic lymphedema, exposure to polyvinyl chloride (PVC), radiation, sun exposure and arsenic (angiosarcoma).
The histology of angiosarcoma is widely variable. Microscopic features include vasoformative structures with cytologic atypia, layered endothelial cells and multinucleated cells with hyaline globules. Higher grade tumors will have solid areas of polygonal and spindled cells, high mitotic rate and necrosis (angiosarcoma, Stanford University: Angiosarcoma of the Breast [Accessed 27 October 2021]). Angiosarcomas involving the adrenal gland tend to be of the epithelioid variant, as in our case (Cancer Control 2017;24:198). Microscopically, the epithelioid variant of angiosarcoma appears as sheets of epithelioid cells with eosinophilic cytoplasm, vesicular nuclei and prominent nucleoli with or without vasoformative structures. Staining is integral to definitive diagnosis (see “Stains” above) as sarcoma, carcinoma and melanoma may all reasonably be in the differential diagnosis (Arch Pathol Lab Med 2011;135:268).
Unilateral adrenalectomy is currently the recommended treatment option. Due to the aggressive nature of this tumor, survival at 5 years after diagnosis is rare, even with early surgical intervention (angiosarcoma). Given the low incidence, research on treatment is lacking, although adjuvant radiation therapy is recommended (Cancer Control 2017;24:198, Arch Pathol Lab Med 2011;135:268).
Sadly, this patient succumbed to her disease 3 months after resection.
Test question answer:
A. ERG
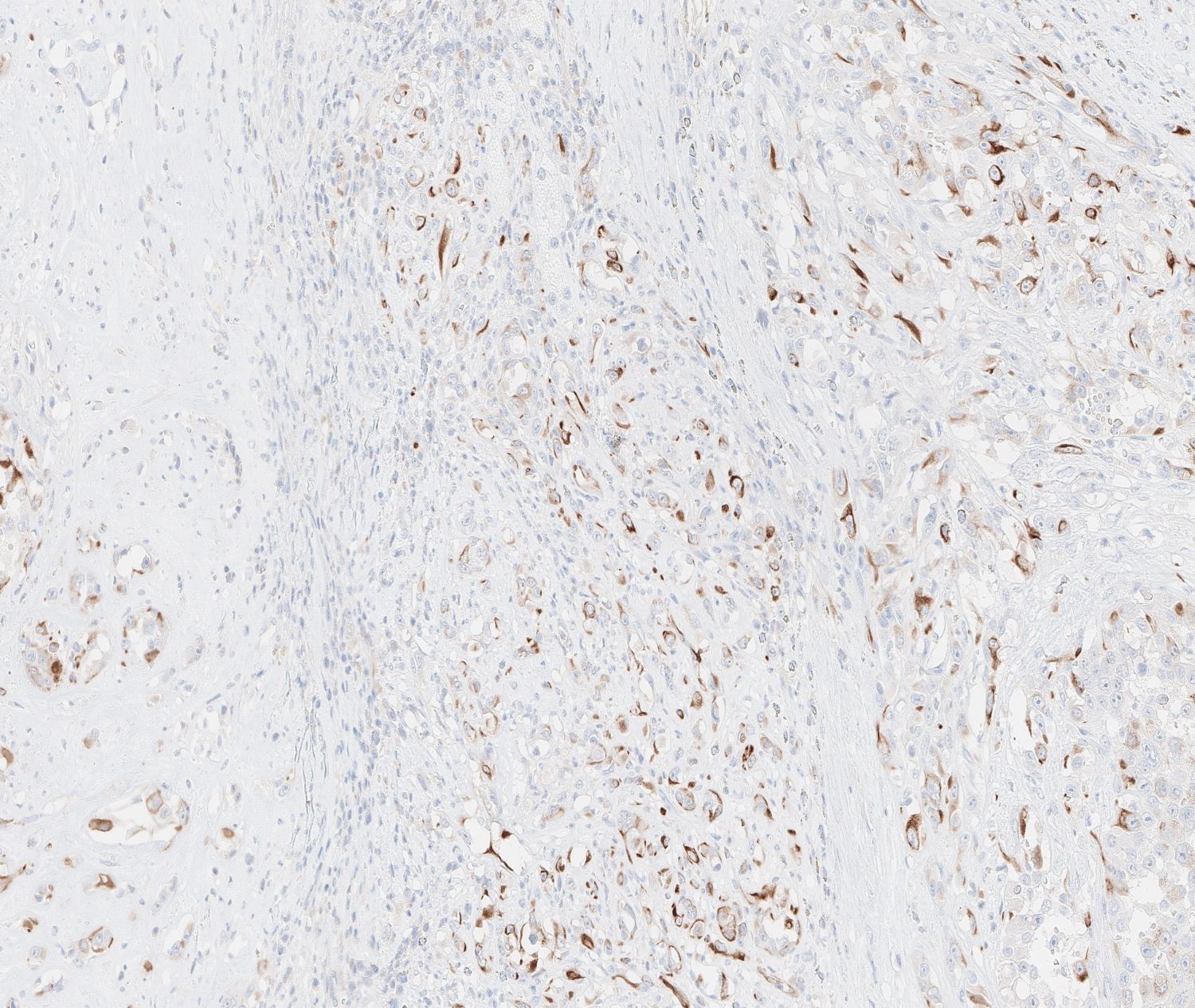
ERG is sensitive and specific for vascular differentiation. Although not on the list of potential answers, CD31 and Factor VIII are also sensitive and specific markers for vascular differentiation and can additionally be useful in this case. Steroidogenic factor 1 (SF1) is a transcription factor that has a role in steroidogenesis and is expressed in the adrenal cortex and other gonadotrophic cells in the pituitary and gonads. While usually a very specific marker, its expression may be lost in up to 12% of adrenal cortical carcinomas (Hum Pathol 2013;44:822). Both epithelioid angiosarcoma and carcinoma will stain positive for pancytokeratin. While VEGFR3 is specific for vascular differentiation, it is less sensitive and will have variable staining in angiosarcoma. While vimentin is quite sensitive for angiosarcoma, it may not be helpful because carcinomas may also stain positive for vimentin.
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Kyle Haggerty (M.D. candidate) and Dr. David Loeffler, Oregon Health & Science University, Portland, Oregon (USA) for contributing this case and the discussion and to Dr. Debra Zynger, The Ohio State University Wexner Medical Center, Columbus, Ohio (USA), for reviewing the discussion.
Advertisement
Case of the Month #509
Clinical history:
The patient is a 71 year old, otherwise healthy woman, with an incidental finding of an 11.7 cm, heterogeneously enhancing mass involving the right adrenal gland. A core biopsy of the mass was performed and read as an undifferentiated carcinoma, prompting resection. During the operation, the mass was found to be adherent to the right hemidiaphragm, liver and superior vena cava.
Histopathology images:
What is your diagnosis?
Click here for diagnosis, test question and discussion:
Diagnosis: Epithelioid angiosarcoma, involving the adrenal gland
Test question (answer at the end):
Which stain will help differentiate epithelioid angiosarcoma from a poorly differentiated adrenal cortical carcinoma?
A. ERG
B. Pancytokeratin
C. SF1
D. VEGFR3
E. Vimentin
IHC stains obtained:
Positive: ERG, CD31, Factor VIII related protein, FLI1, thrombomodulin, CD34, KIT, Vimentin, Keratin
Variable: VEGFR3
CD31
CK7
CKCKT
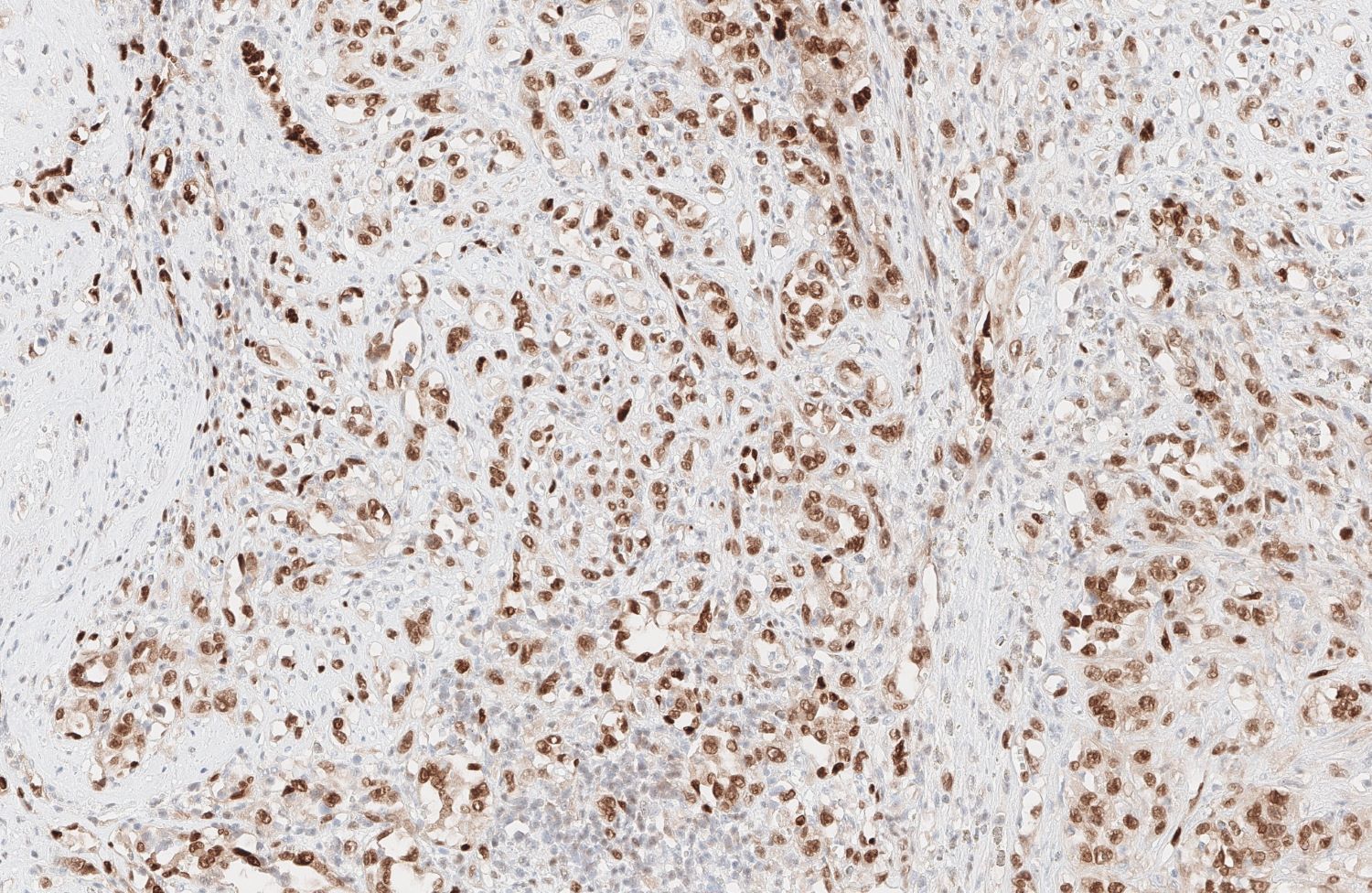
ERG
SF1
Discussion:
The tumor in this case is highly pleomorphic and was initially diagnosed as undifferentiated carcinoma on biopsy. The differential diagnosis included poorly differentiated adrenal cortical carcinoma, melanoma and sarcoma. On H&E, clues to the final diagnosis are the foci with vasoformative morphology scattered throughout the tumor. Staining shows neoplastic cells positive for ERG and CD31, highlighting vascular structures and the overall vascular differentiation of this tumor.
Adrenal tumors are relatively common, with 4% of abdominal CTs and 8% of autopsies revealing an adrenal mass. The majority of incidentally discovered adrenal masses are small (< 1.0 cm) benign masses, colloquially termed "incidentalomas". Clinical suspicion for malignancy, symptoms of a hyperfunctional adrenal tissue, or mass size > 1.0 cm warrants further workup (Cancer Control 2017;24:198). For our patient, tumor size, heterogeneity and proximity to adjacent structures necessitated further workup and resection.
Angiosarcoma is a rare, aggressive, malignant tumor arising from vascular endothelium. Angiosarcoma of the adrenal gland is exceedingly rare (Am J Surg Pathol 1994;18:62). Less than 1% of all soft tissue sarcomas are angiosarcomas; even that small percentage typically arise from the breast, skin, spleen, bone, kidney, thyroid or liver (Cancer Control 2017;24:198, Arch Pathol Lab Med 2011;135:268, angiosarcoma). Angiosarcomas are most common in older adult males and when they do arise in children or younger adults, the prognosis is notably poor. Risk factors include chronic lymphedema, exposure to polyvinyl chloride (PVC), radiation, sun exposure and arsenic (angiosarcoma).
The histology of angiosarcoma is widely variable. Microscopic features include vasoformative structures with cytologic atypia, layered endothelial cells and multinucleated cells with hyaline globules. Higher grade tumors will have solid areas of polygonal and spindled cells, high mitotic rate and necrosis (angiosarcoma, Stanford University: Angiosarcoma of the Breast [Accessed 27 October 2021]). Angiosarcomas involving the adrenal gland tend to be of the epithelioid variant, as in our case (Cancer Control 2017;24:198). Microscopically, the epithelioid variant of angiosarcoma appears as sheets of epithelioid cells with eosinophilic cytoplasm, vesicular nuclei and prominent nucleoli with or without vasoformative structures. Staining is integral to definitive diagnosis (see “Stains” above) as sarcoma, carcinoma and melanoma may all reasonably be in the differential diagnosis (Arch Pathol Lab Med 2011;135:268).
Unilateral adrenalectomy is currently the recommended treatment option. Due to the aggressive nature of this tumor, survival at 5 years after diagnosis is rare, even with early surgical intervention (angiosarcoma). Given the low incidence, research on treatment is lacking, although adjuvant radiation therapy is recommended (Cancer Control 2017;24:198, Arch Pathol Lab Med 2011;135:268).
Sadly, this patient succumbed to her disease 3 months after resection.
Test question answer:
A. ERG
ERG is sensitive and specific for vascular differentiation. Although not on the list of potential answers, CD31 and Factor VIII are also sensitive and specific markers for vascular differentiation and can additionally be useful in this case. Steroidogenic factor 1 (SF1) is a transcription factor that has a role in steroidogenesis and is expressed in the adrenal cortex and other gonadotrophic cells in the pituitary and gonads. While usually a very specific marker, its expression may be lost in up to 12% of adrenal cortical carcinomas (Hum Pathol 2013;44:822). Both epithelioid angiosarcoma and carcinoma will stain positive for pancytokeratin. While VEGFR3 is specific for vascular differentiation, it is less sensitive and will have variable staining in angiosarcoma. While vimentin is quite sensitive for angiosarcoma, it may not be helpful because carcinomas may also stain positive for vimentin.