
13 May 2021 - Case of the Month #503
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Kelly Magliocca, Emory University, Atlanta, Georgia (USA), for contributing this case and writing the discussion and to Dr. Bin Xu, Memorial Sloan Kettering Cancer Center, New York (USA), for reviewing the discussion.
Advertisement
Case of the Month #503
Clinical history:
A 54 year old man presented with a 2.5 cm lytic mandibular lesion.
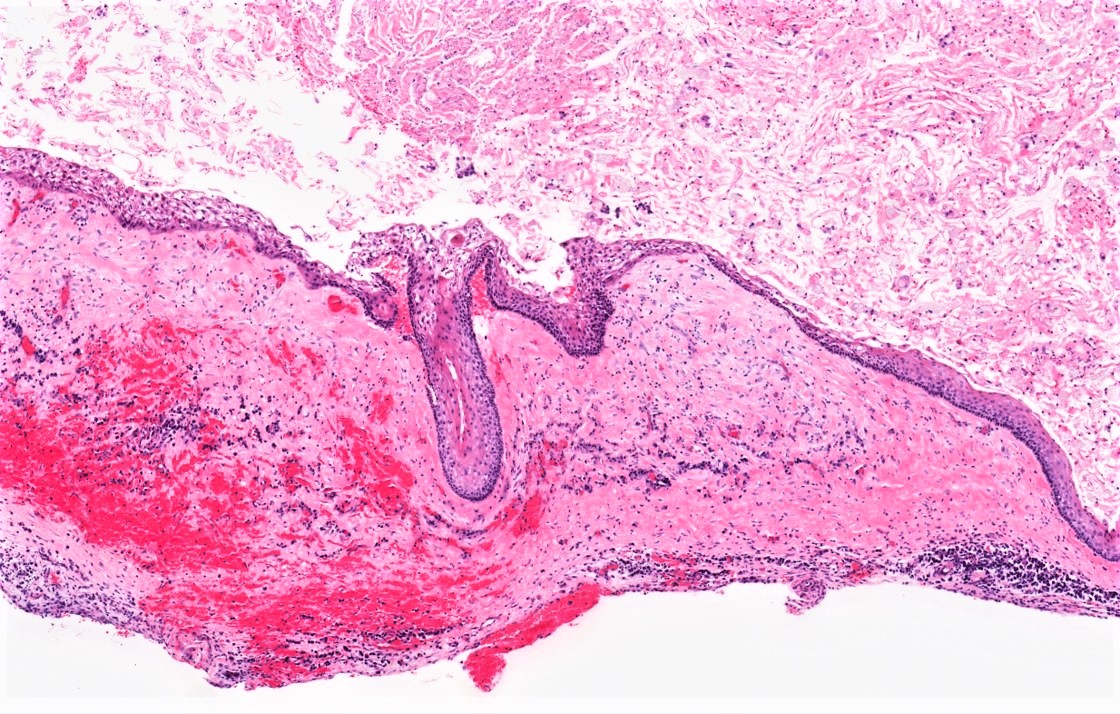
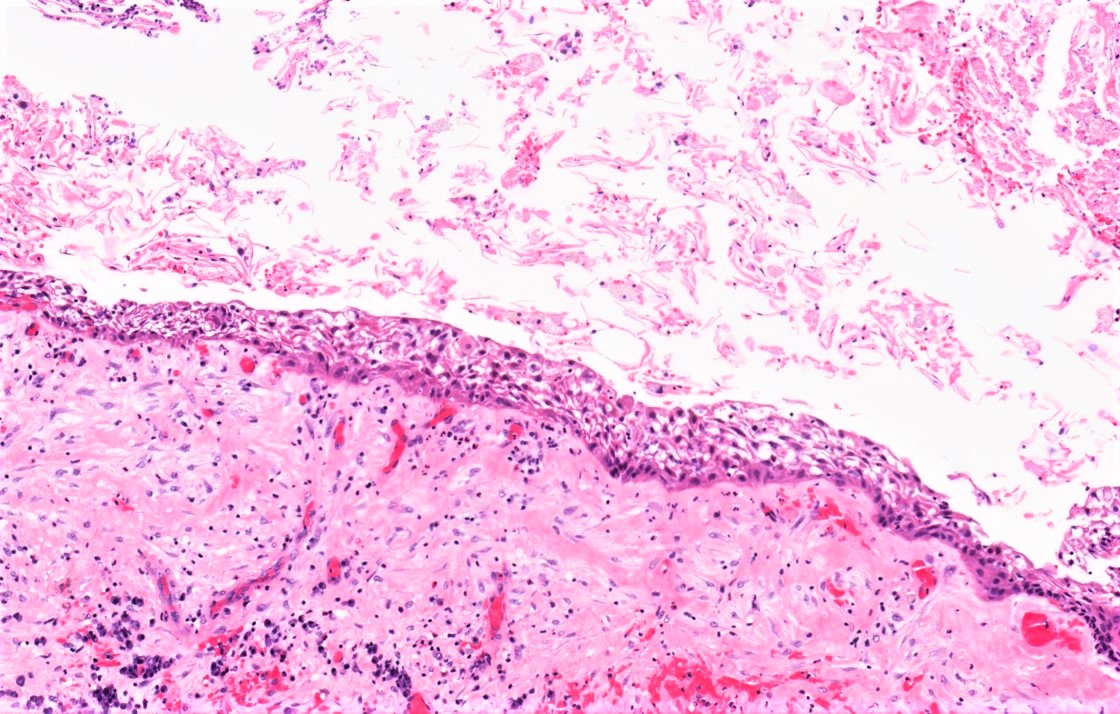
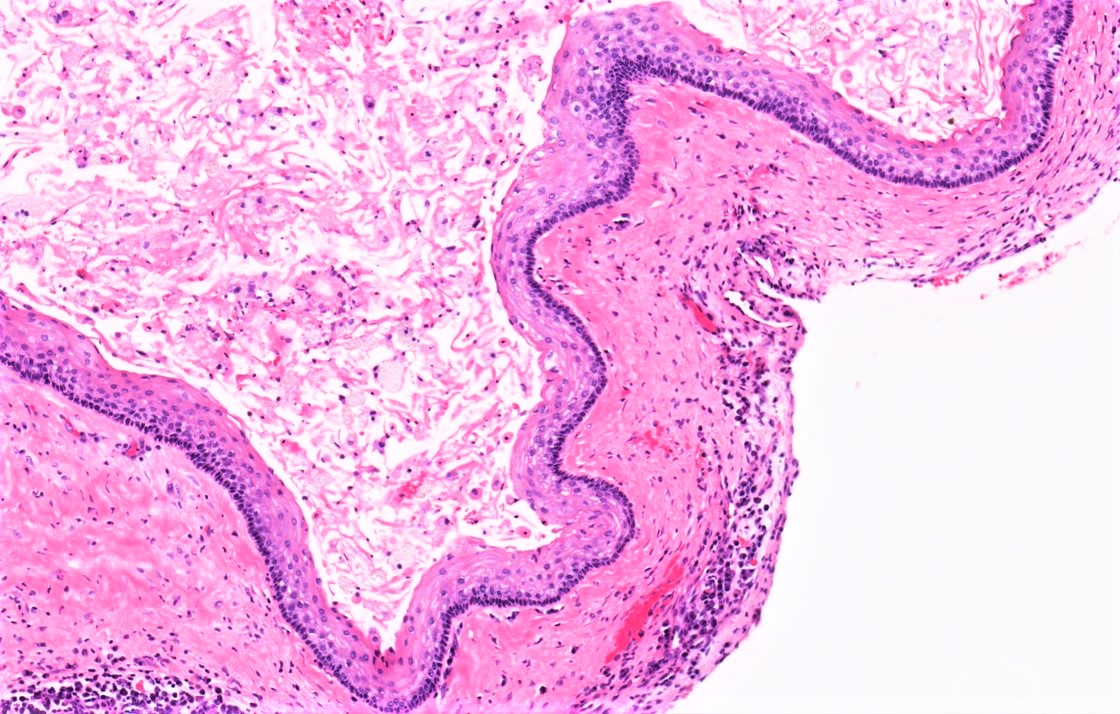
Histopathology images:

What is your diagnosis?
Diagnosis: Odontogenic keratocyst
Test question (answer at the end):
Which of the following sites is most commonly involved in by odontogenic keratocyst?
A. Gingiva
B. Mandible
C. Maxillary sinus
D. Anterior maxilla
Discussion:
Odontogenic keratocyst (OKC) is an odontogenic cyst arising from odontogenic epithelial remnants. In most cases, OKC presents as an isolated lytic lesion within bone, most commonly in the posterior mandible. Multiple OKCs can be associated with nevoid basal cell carcinoma syndrome (NBCCS) (Gorlin-Goltz syndrome). The presence of multiple OKCs can be the first clue to the diagnosis of NBCCS, particularly when presenting in the first decade of life (Am J Med Genet A 2011;155A:2091).
Microscopically, odontogenic keratocyst is characterized by a stratified squamous epithelial lining featuring a hyperchromatic, palisaded cuboidal basal layer. Rete ridge formation is generally absent, although budding of the basal layer can be seen in some cases. The parakeratin surface of the cyst often exhibits corrugation. In the setting of inflammation, the diagnostic features of OKC can be lost and the cyst lining tends toward a nonkeratinizing edematous stratified squamous epithelial lining. Detached keratin debris may be abundant; it is not required for diagnosis.
The leading entity in the differential diagnosis of OKC is orthokeratinized odontogenic cyst (OOC). OOC features abundant detached lamellated orthokeratin and a stratified squamous epithelial lining with a prominent granular layer. The basal layer palisading and hyperchromatism seen in OKC are absent in OOC (Oral Surg Oral Med Oral Pathol 1981;51:609). In fact, the microscopic appearance of the lining of OOC is very similar to that seen lining a cholesteatoma of the middle ear. OOC has no association with NBCCS and is far less likely to recur after treatment.
Treatment of OKC most commonly involves enucleation and curettage. OKC can locally recur and most often requires clinical and radiographic surveillance to assist in the evaluation for local recurrence (Oral Surg Oral Med Oral Pathol Oral Radiol 2019;127:282).
Test question answer:
B. The mandible is most commonly involved site among the anatomic sites listed.
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Kelly Magliocca, Emory University, Atlanta, Georgia (USA), for contributing this case and writing the discussion and to Dr. Bin Xu, Memorial Sloan Kettering Cancer Center, New York (USA), for reviewing the discussion.
Advertisement
Case of the Month #503
Clinical history:
A 54 year old man presented with a 2.5 cm lytic mandibular lesion.
Histopathology images:
What is your diagnosis?
Click here for diagnosis, test question and discussion:
Diagnosis: Odontogenic keratocyst
Test question (answer at the end):
Which of the following sites is most commonly involved in by odontogenic keratocyst?
A. Gingiva
B. Mandible
C. Maxillary sinus
D. Anterior maxilla
Discussion:
Odontogenic keratocyst (OKC) is an odontogenic cyst arising from odontogenic epithelial remnants. In most cases, OKC presents as an isolated lytic lesion within bone, most commonly in the posterior mandible. Multiple OKCs can be associated with nevoid basal cell carcinoma syndrome (NBCCS) (Gorlin-Goltz syndrome). The presence of multiple OKCs can be the first clue to the diagnosis of NBCCS, particularly when presenting in the first decade of life (Am J Med Genet A 2011;155A:2091).
Microscopically, odontogenic keratocyst is characterized by a stratified squamous epithelial lining featuring a hyperchromatic, palisaded cuboidal basal layer. Rete ridge formation is generally absent, although budding of the basal layer can be seen in some cases. The parakeratin surface of the cyst often exhibits corrugation. In the setting of inflammation, the diagnostic features of OKC can be lost and the cyst lining tends toward a nonkeratinizing edematous stratified squamous epithelial lining. Detached keratin debris may be abundant; it is not required for diagnosis.
The leading entity in the differential diagnosis of OKC is orthokeratinized odontogenic cyst (OOC). OOC features abundant detached lamellated orthokeratin and a stratified squamous epithelial lining with a prominent granular layer. The basal layer palisading and hyperchromatism seen in OKC are absent in OOC (Oral Surg Oral Med Oral Pathol 1981;51:609). In fact, the microscopic appearance of the lining of OOC is very similar to that seen lining a cholesteatoma of the middle ear. OOC has no association with NBCCS and is far less likely to recur after treatment.
Treatment of OKC most commonly involves enucleation and curettage. OKC can locally recur and most often requires clinical and radiographic surveillance to assist in the evaluation for local recurrence (Oral Surg Oral Med Oral Pathol Oral Radiol 2019;127:282).
Test question answer:
B. The mandible is most commonly involved site among the anatomic sites listed.
