
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Brendan C. Dickson, University of Toronto, Toronto, Ontario (Canada), for contributing this case and writing the discussion.
top

Pathologist
POWELL, OHIO (USA). Discovery Life Sciences is a trusted provider of bioanalytic and biospecimen services to hundreds of customers across the U.S. and around the world. The contracting Pathologist will provide (non-clinical) pathology review of FFPE H&E slides (as well as other special stains on occasion) in order to confirm alignment of original clinical pathology records and add other data points of research interest (i.e. % tumor, identification of certain tissue types or cellular structures). This review involves the hand marking of the slides per a specific protocol using super fine permanent markers and the use of company software in which to record the findings. Discovery Life Sciences will provide training in all areas of specific protocols to follow that are unique to DLS. Contractor may be asked to participate in special projects according to their areas of specialization.
Qualifications:
• Board Certification (U.S.) in Pathology (please present copy of certification)
• Participation in Continuing Certification (CC) programs encouraged
• Must reside in Central Ohio / Columbus Metro area
• Strong IHC experience preferred
Hours and Location:
• Flexible work scheduling Mon-Fri. - between 8am and 6pm preferred
• Minimum 12 hours/week preferred, (i.e. 3 x 4 hours shifts), up to 30 hours
• Powell, OH office location
• Work station, microscope, computer and office supplies will be provided
Pay rate: $75/hour
For more information or to apply please contact:
Jon Price
Senior V.P., FFPE Services
Direct Telephone: 256.836.7052
Mobile Telephone: 614-403-2958
Main Telephone: 614-846-2809
Fax: 877-633-6442
Email: on.price@dls.com
Advertisement
Case of the Month #485
Clinical history:
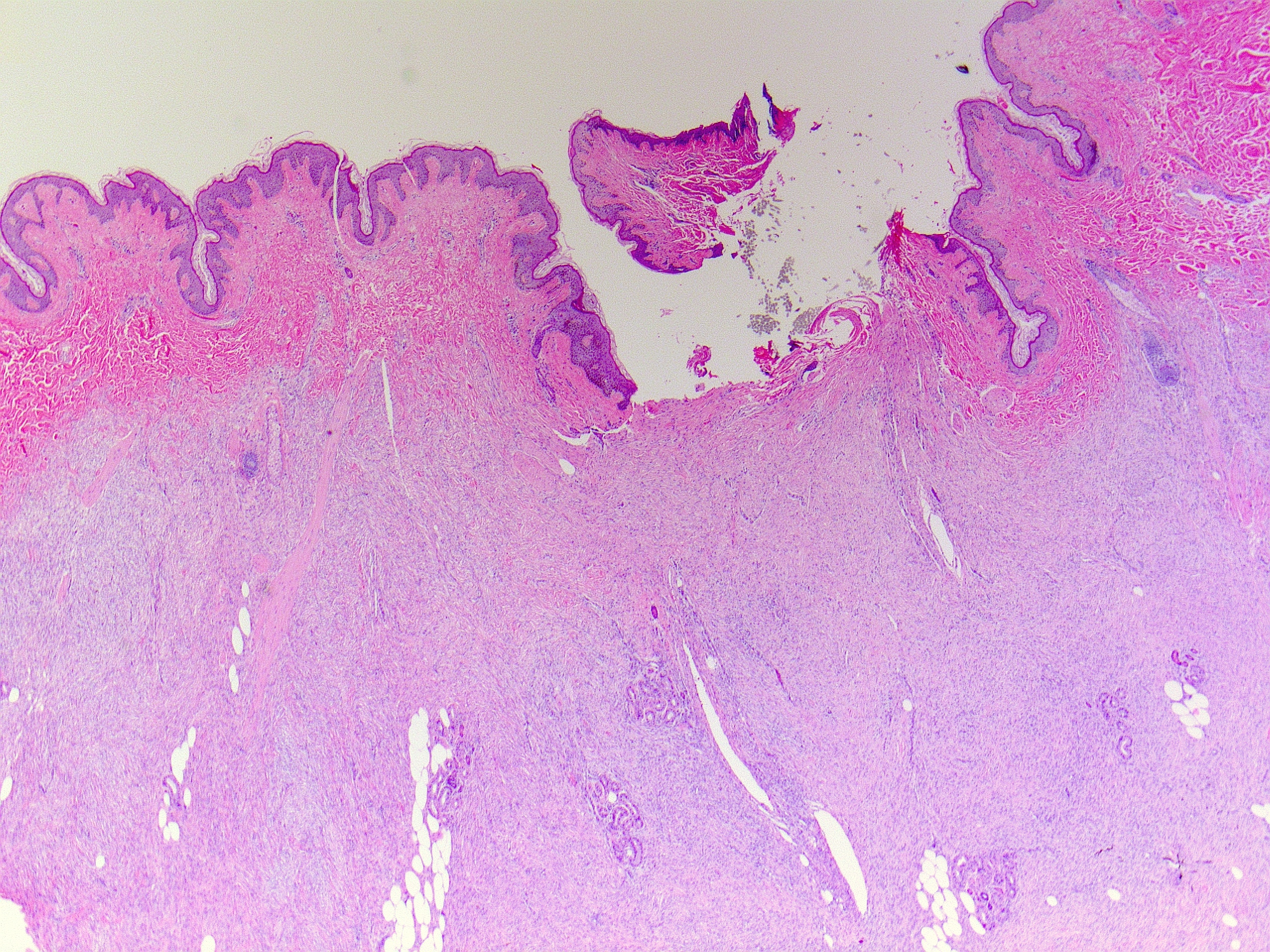
A 30 year old woman presented with a longstanding history of a small abdominal wall mass. The mass had been present since childhood, gradually becoming more protuberant in early adulthood. An excisional biopsy was performed.
Histopathology images:


What is your diagnosis?
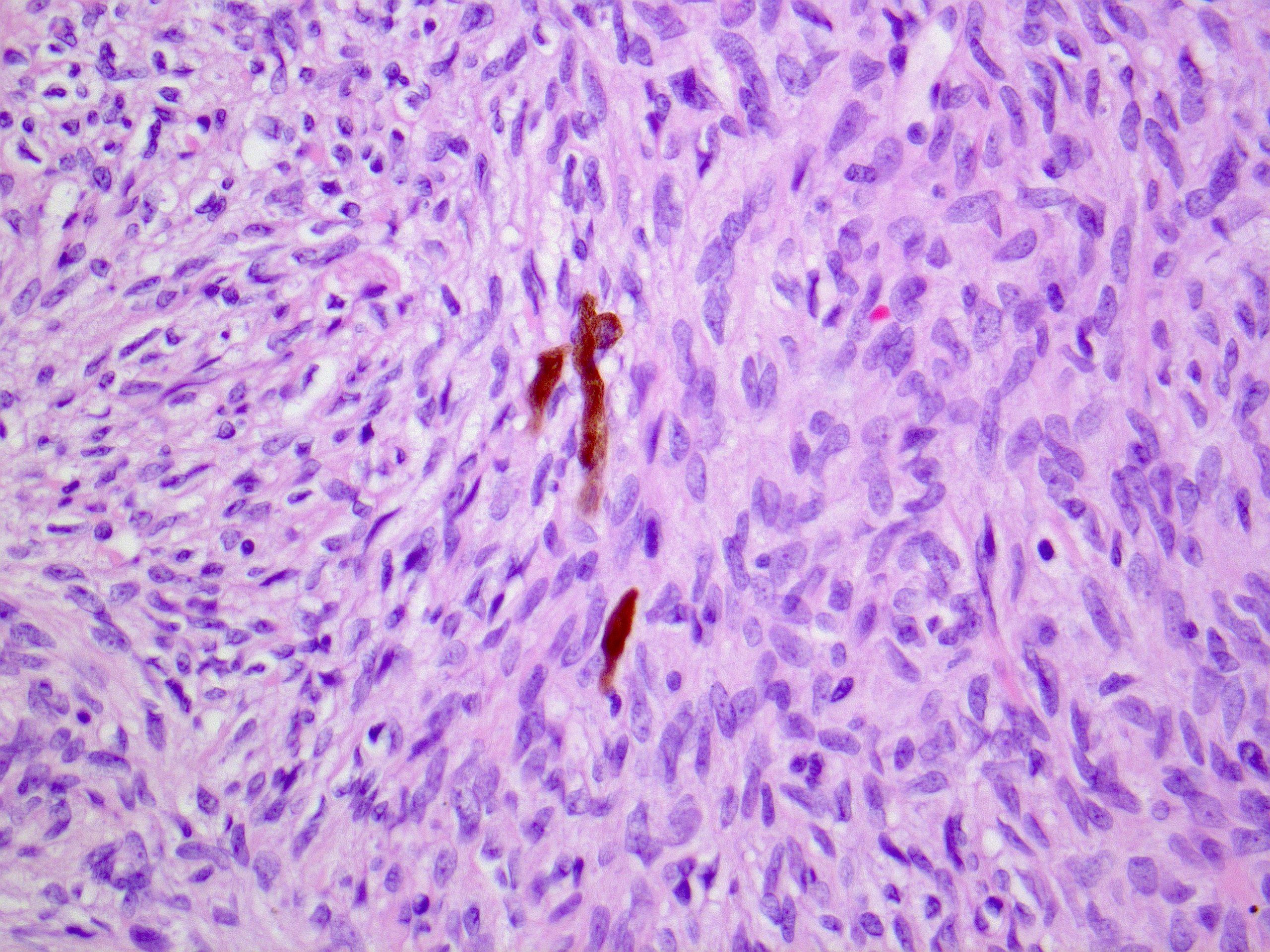
Diagnosis: Pigmented dermatofibrosarcoma protuberans (Bednar tumour)
Test question (answer at the end):
The molecular pathogenesis of most cases of dermatofibrosarcoma protuberans is characterized by the following fusion gene product:
A. COL6A3-PDGFD
B. COL6A3-CSF1
C. COL1A1-PDGFB
D. COL1A1-USP6
Stains:
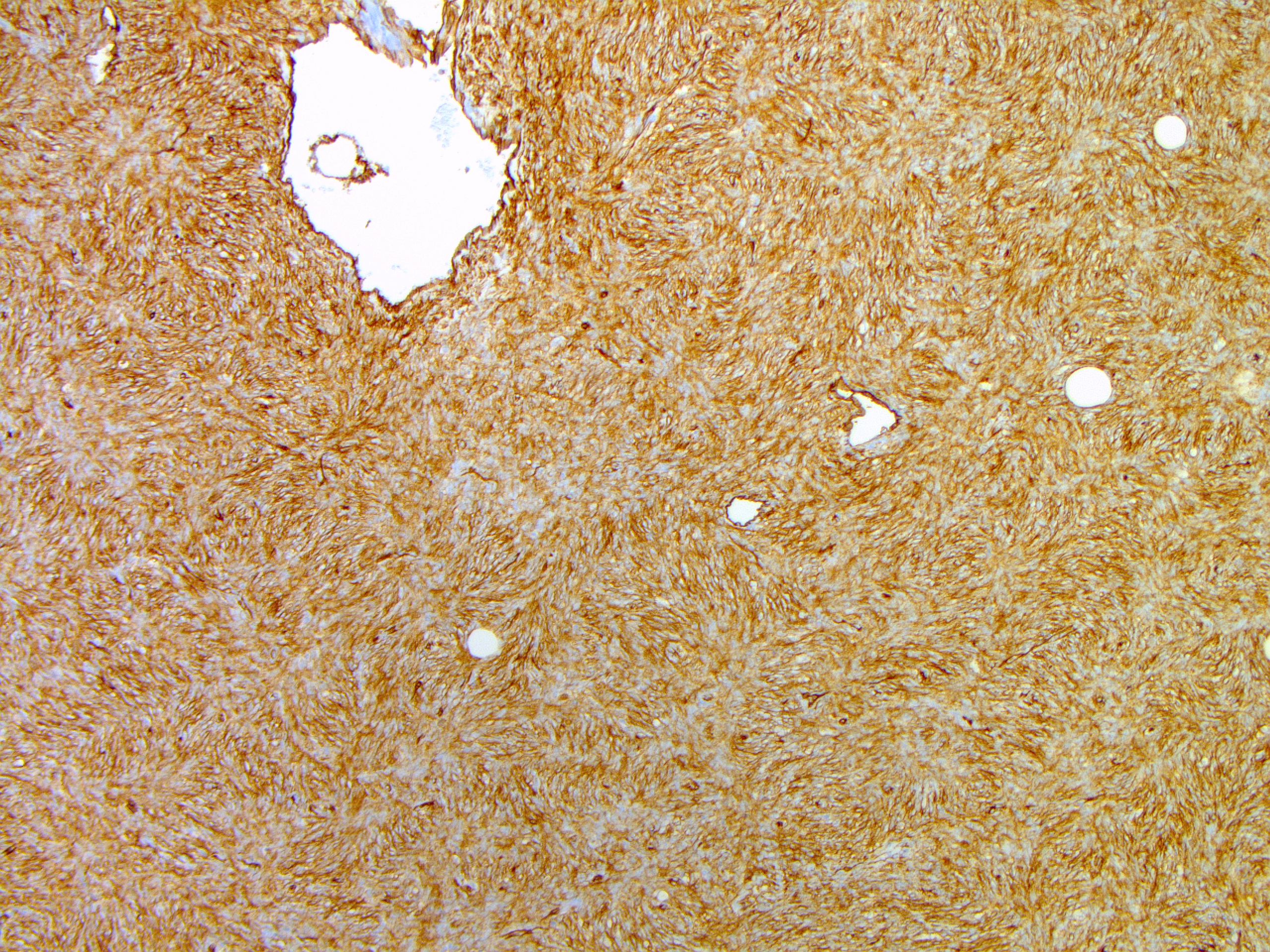
CD34
Discussion:
Dermatofibrosarcoma protuberans is a low grade neoplasm involving the dermis, subcutis or both. Approximately 1 - 5% of all cases contain varying numbers of pigmentated dendritic-like cells (Am J Surg Pathol 1985;9:630). In addition to cases with a conventional morphology (Cancer 1957;10:368), pigmentation may be found in most dermatofibrosarcoma protuberans variants, including fibrosarcomatous dermatofibrosarcoma protuberans (Am J Surg Pathol 1998;22:576), myxoid dermatofibrosarcoma protuberans (Am J Surg Pathol 2007;31:1371) and so called giant cell fibroblastoma (Am J Surg Pathol 1994;18:736).
As with most cases of dermatofibrosarcoma protuberans, the current case was diffusely positive for CD34 and RNA sequencing confirmed the presence of a COL1A1-PDGFB gene fusion. Pigmentation may rarely lead to a clinical impression of a melanocytic neoplasm. Other than this, the presence of pigmentation is of no clinical or pathologic significance (Histopathology 1988;13:631, Genes Chromosomes Cancer 2001;30:305). Treatment typically involves wide local excision at non-critical anatomic sites (2 - 3 cm margin). In some instances, neoadjuvant imatinib treatment may be beneficial (e.g., to downsize large lesions prior to resection) (Wright et al.: Surgical Oncology Manual, 2016).
Test question answer:
C. COL1A1-PDGFB
COL6A3-PDGFD is only rarely encountered in dermatofibrosarcoma protuberans; COL6A3-CSF1 is found in a subset of tenosynovial giant cell tumours; COL1A1-USP6 may be present in myositis ossificans, fibro-osseous pseudotumour of the digits and aneurysmal bone cyst.
