12 December 2018 - Case of the Week #470
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Week page. To subscribe or unsubscribe to Case of the Week or our other email lists, click here.
Thanks to Drs. Safa Alshaikh and Aalaa Mohammed, Salmaniya Medical Complex, (Kingdom of Bahrain) for contributing this case, Dr. Ayana Suzuki, Kuma Hospital, Kobe City (Japan) for writing the discussion and Dr. Andrey Bychkov for the Editorial Board review. To contribute a Case of the Week, first make sure that we are currently accepting cases, then follow the guidelines on our main Case of the Week page.

Advertisement
Website news:
(1) For November 2018, we had a record number of sessions per day of 37,912. This is an increase of 29% from the same month in 2017. Thanks for using our website!
(2) We have posted the third quarter jobs report from 2018. It is also accessible from the Jobs page by clicking on the orange link.
(3) As you may know, we receive a commission from Amazon when you use the Amazon links on our website to buy anything through Amazon. Please use them when you do your holiday shopping this season. Thanks in advance!
Visit and follow our Blog to see recent updates to the website.
Case of the Week #470
Clinical history:
A 19 year old woman presented with a right sided neck swelling, which was increasing in size. Ultrasound showed a hyperechoic thyroid nodule, 2 x 1 cm, with foci of cystic changes. Fine needle aspiration was performed followed by total thyroidectomy.
Cytology images:

Histopathology images:

What is your diagnosis?
Diagnosis:
Cribriform morular variant of papillary thyroid carcinoma
Test question (answer at the end):
What syndrome is associated with cribriform morular variant of thyroid carcinoma?
A. Carney complex
B. Familial adenomatous polyposis
C. Cowden syndrome
D. Gardner syndrome
IHC stains:
Discussion:
Cribriform morular variant of papillary thyroid carcinoma (CMV-PTC) is rare, accounting for 0.2% of papillary thyroid carcinoma (PTC) cases (World J Surg 2018;42:3616). It is associated with sporadic or germline mutations of the adenomatous polyposis coli (APC) gene (WHO Classification of Tumours of Endocrine Organs, 4th ed., 2017). It occurs almost exclusively in young adult women. Sporadic cases are usually solitary but cases associated with familial adenomatous polyposis (FAP) are often multifocal (Kakudo: Thyroid FNA Cytology, Differential Diagnoses and Pitfalls, 2016).
CMV-PTC mimics follicular neoplasm or nodular goiter at ultrasound (J Med Ultrason 2015;42:83) but cytological preparation shows hypercellularity with many atypical follicular cells containing numerous intranuclear cytoplasmic inclusions and nuclear grooves, which are diagnostic for PTC. CMV-PTC is encapsulated or circumscribed with mixed cribriform, papillary, solid, tall columnar and morular patterns. The lumen of the cribriform areas usually lacks colloid. The cells have abundant eosinophilic cytoplasm and pseudostratification with hyperchromatic nuclei, grooves and pseudoinclusions. Morules are cell clusters with eddy formations usually seen scattered within the tumor (Acta Cytol 2004;48:431, Acta Cytol 2011;55:13). Perinuclear clearing characteristic of this variant is observed in the morules (Kini: Thyroid Cytopathology, an Atlas and Text, 2nd ed., 2015). Its presence, identified by pale staining of most nuclei accompanied by condensed chromatin at their periphery, is useful for diagnosis (Acta Cytol 2004;48:431, Diagn Cytopathol 2010;38:890). Typically there is no definite ground glass appearance (Ali, Cibas: The Bethesda System for Reporting Thyroid Cytopathology, 2nd ed., 2018). Cytoplasmic lipid may be present (Pathobiology 2017;84:251) with vacuoles that are positive for Oil red O and adipophilin.
Immunohistochemistry with β-catenin shows a change from the membranous pattern of normal thyroid cells to cytoplasmic and nuclear staining in tumor cells, which is highly specific for CMV-PTC (Acta Cytol 2004;48:431, Acta Cytol 2013;57:127). In addition, estrogen receptor and progesterone receptor reveal strong nuclear immunopositivity except in morular cells (Mod Pathol 1999;12:400). Immunostaining can be applied to both cytologic and surgical specimens.
Although insular carcinoma and follicular neoplasm may also present with cribriform patterns, these tumors have smaller and rounder spaces, which may contain colloid. Morules may mimic squamous metaplasia but their cytoplasm is not densely stained.
Lobectomy is recommended for non FAP-associated CMV-PTC and total thyroidectomy for FAP-associated CMV-PTC. However, extensive lymph node dissection is not necessary because nodal metastases are rare (Endocr J 2011;58:685, Pathol Res Pract 2015;211:712). The prognosis is excellent (Endocr Relat Cancer 2017;24:R109). The clinician should be alerted to exclude FAP since this diagnosis is the first indicator of FAP syndrome in 25% of cases (Int J Med Sci 2004;1:43).
Test question answer:
B. Familial adenomatous polyposis
Familial adenomatous polyposis is a rare condition transmitted in an autosomal dominant pattern related to germline mutation of the tumor suppressor gene APC, which strongly predisposes to colorectal cancer. Thyroid carcinoma rarely coexists with FAP (in just 0.3-1.2% of cases). When it does, it is almost exclusively CMV-PTC.
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Week page. To subscribe or unsubscribe to Case of the Week or our other email lists, click here.
Thanks to Drs. Safa Alshaikh and Aalaa Mohammed, Salmaniya Medical Complex, (Kingdom of Bahrain) for contributing this case, Dr. Ayana Suzuki, Kuma Hospital, Kobe City (Japan) for writing the discussion and Dr. Andrey Bychkov for the Editorial Board review. To contribute a Case of the Week, first make sure that we are currently accepting cases, then follow the guidelines on our main Case of the Week page.
Advertisement
Website news:
(1) For November 2018, we had a record number of sessions per day of 37,912. This is an increase of 29% from the same month in 2017. Thanks for using our website!
(2) We have posted the third quarter jobs report from 2018. It is also accessible from the Jobs page by clicking on the orange link.
(3) As you may know, we receive a commission from Amazon when you use the Amazon links on our website to buy anything through Amazon. Please use them when you do your holiday shopping this season. Thanks in advance!
Visit and follow our Blog to see recent updates to the website.
Case of the Week #470
Clinical history:
A 19 year old woman presented with a right sided neck swelling, which was increasing in size. Ultrasound showed a hyperechoic thyroid nodule, 2 x 1 cm, with foci of cystic changes. Fine needle aspiration was performed followed by total thyroidectomy.
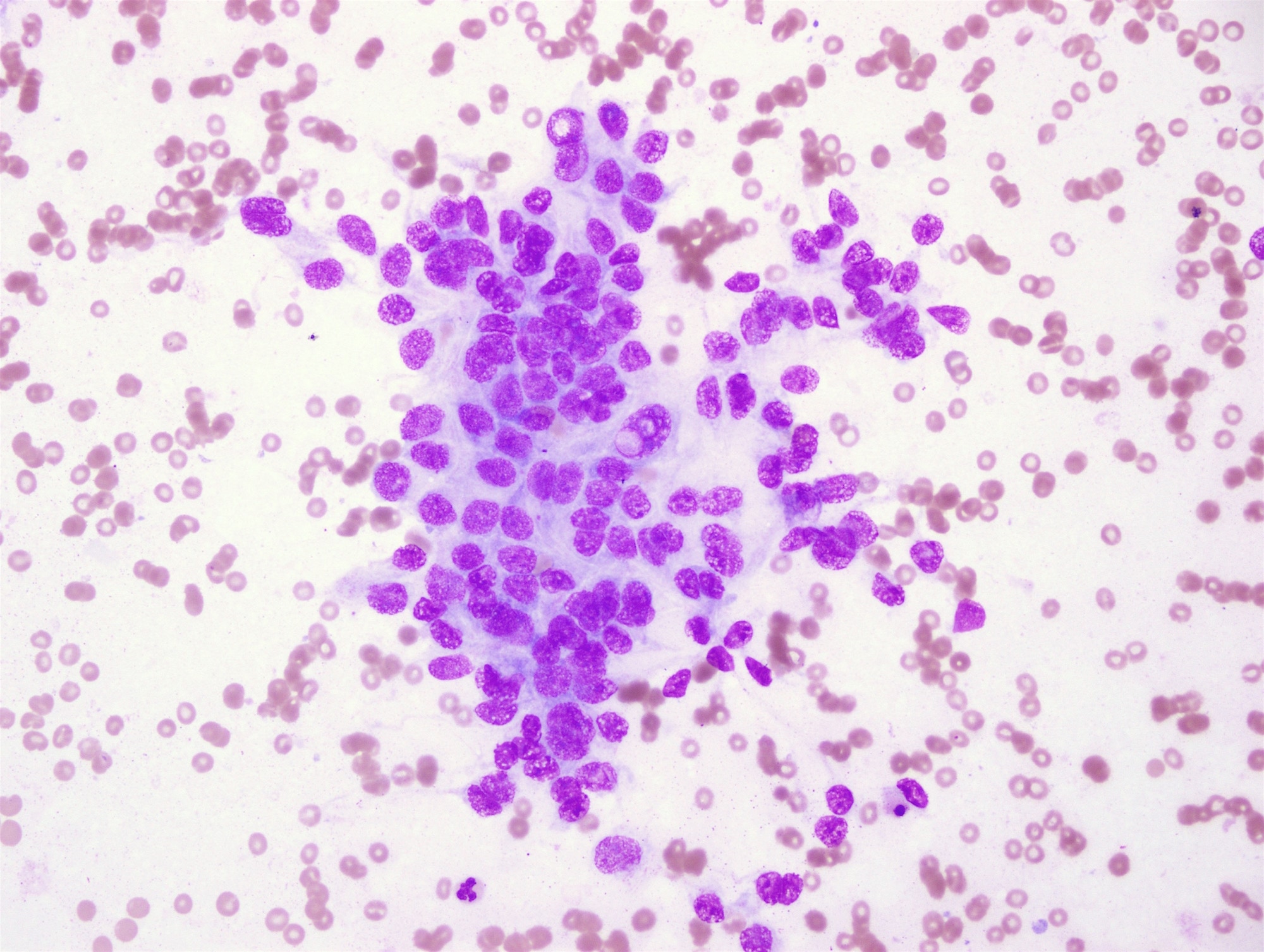
Cytology images:
May Grunwald Giemsa (MGG)
Pap stain
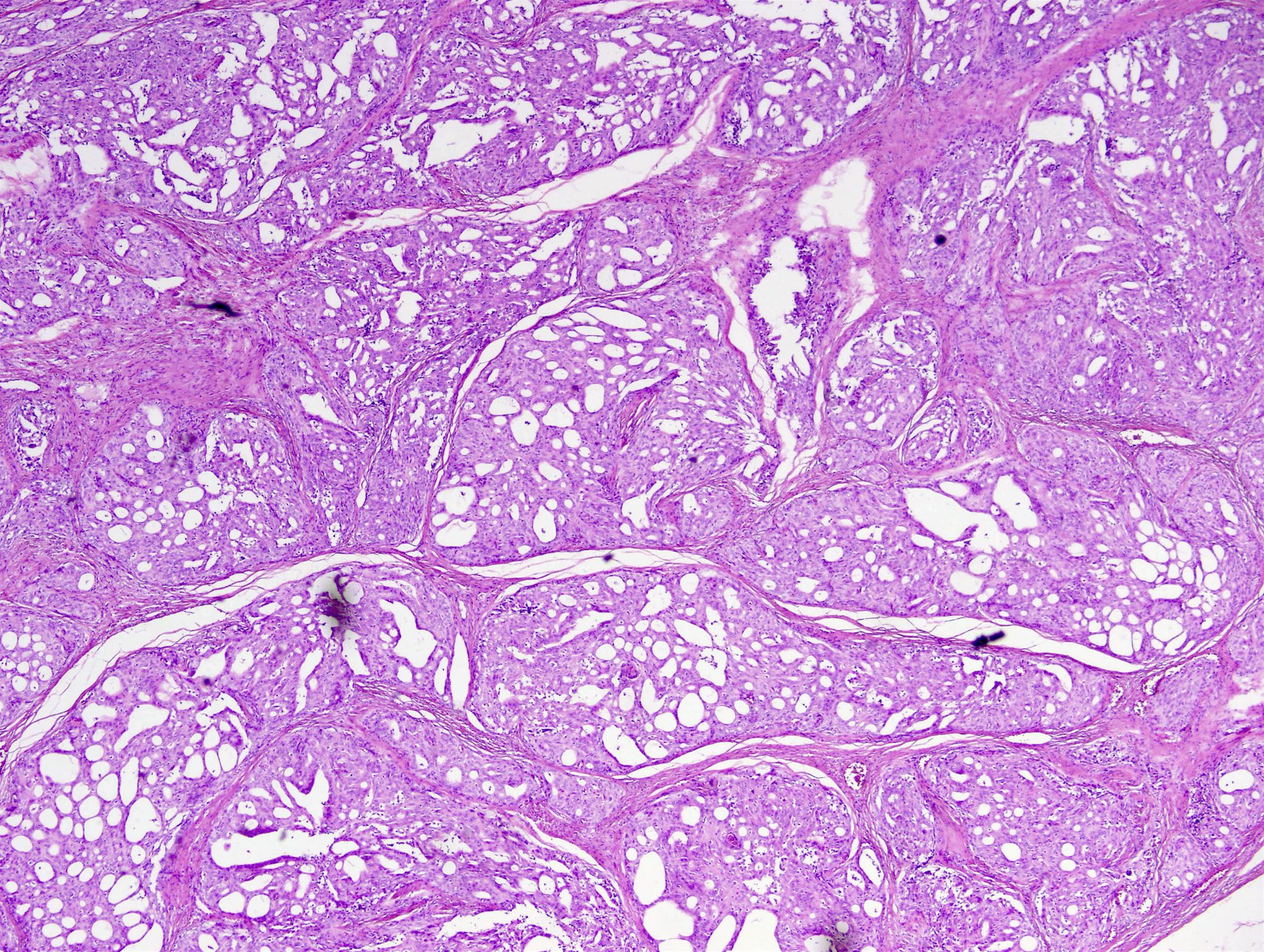
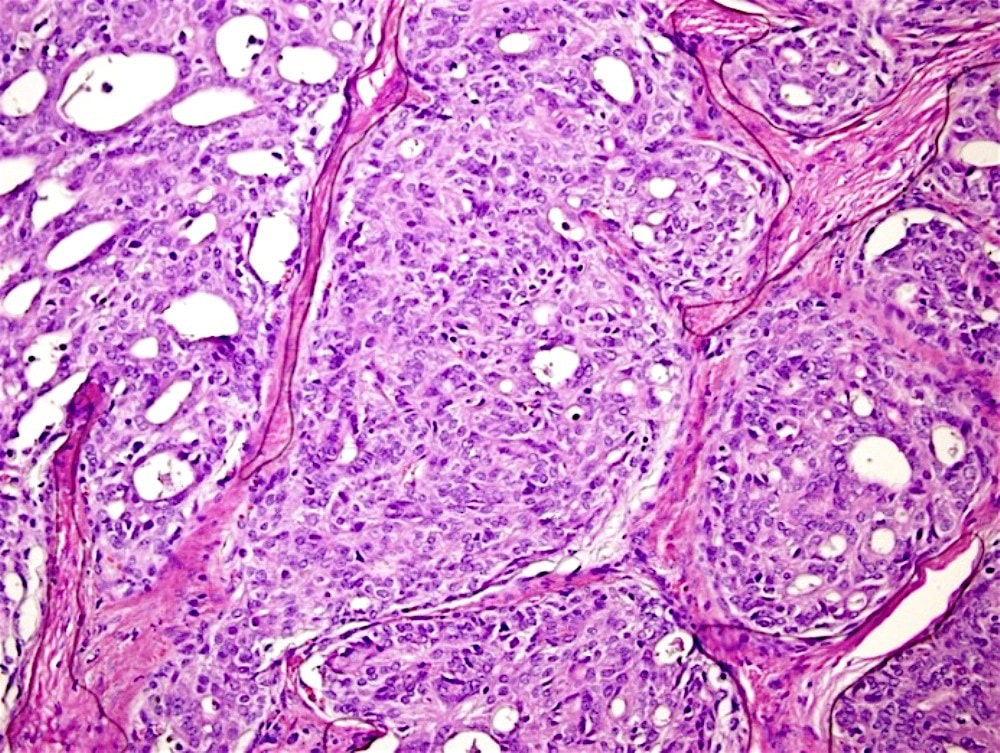
Histopathology images:
What is your diagnosis?
Diagnosis:
Cribriform morular variant of papillary thyroid carcinoma
Test question (answer at the end):
What syndrome is associated with cribriform morular variant of thyroid carcinoma?
A. Carney complex
B. Familial adenomatous polyposis
C. Cowden syndrome
D. Gardner syndrome
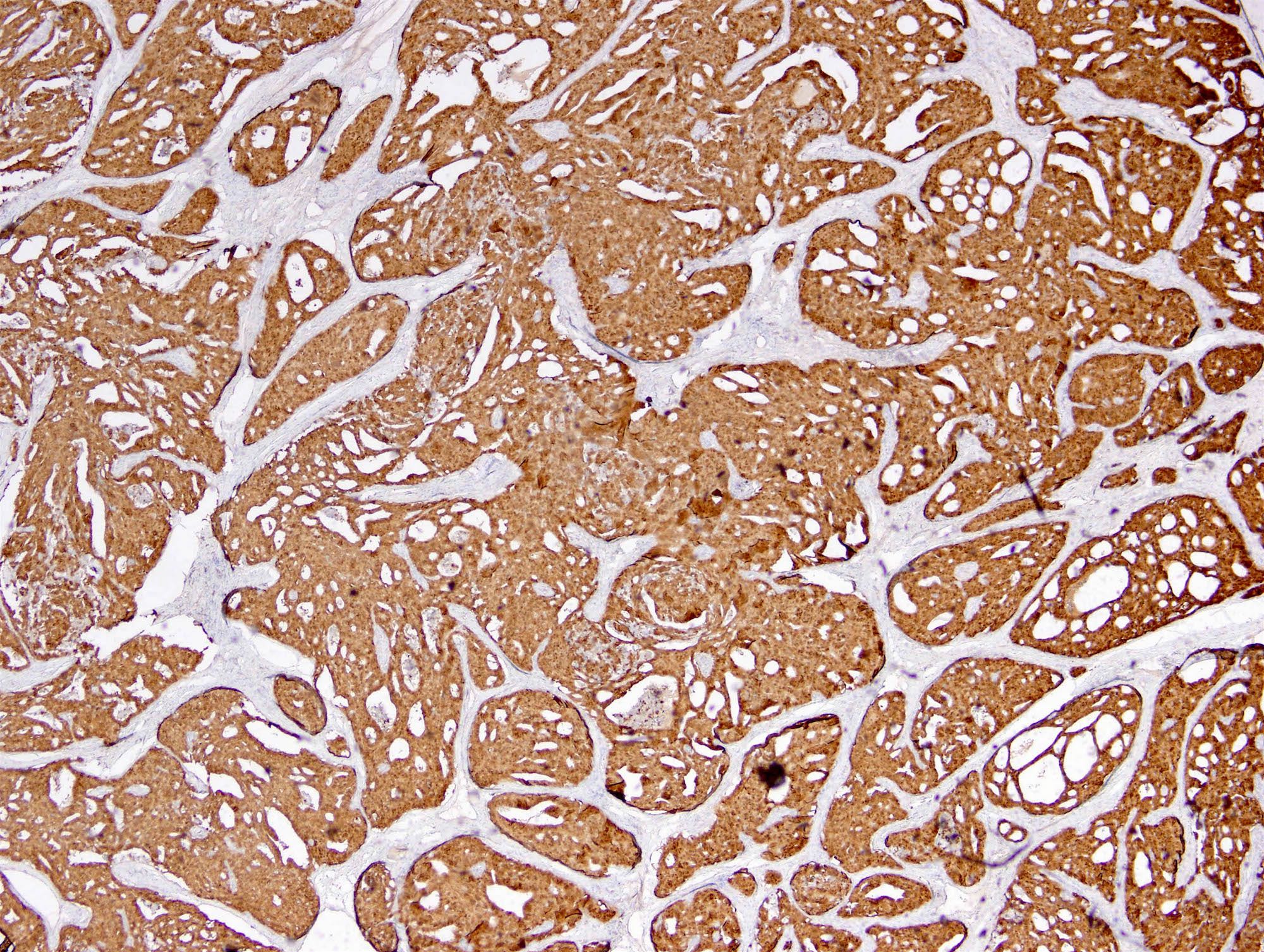
IHC stains:
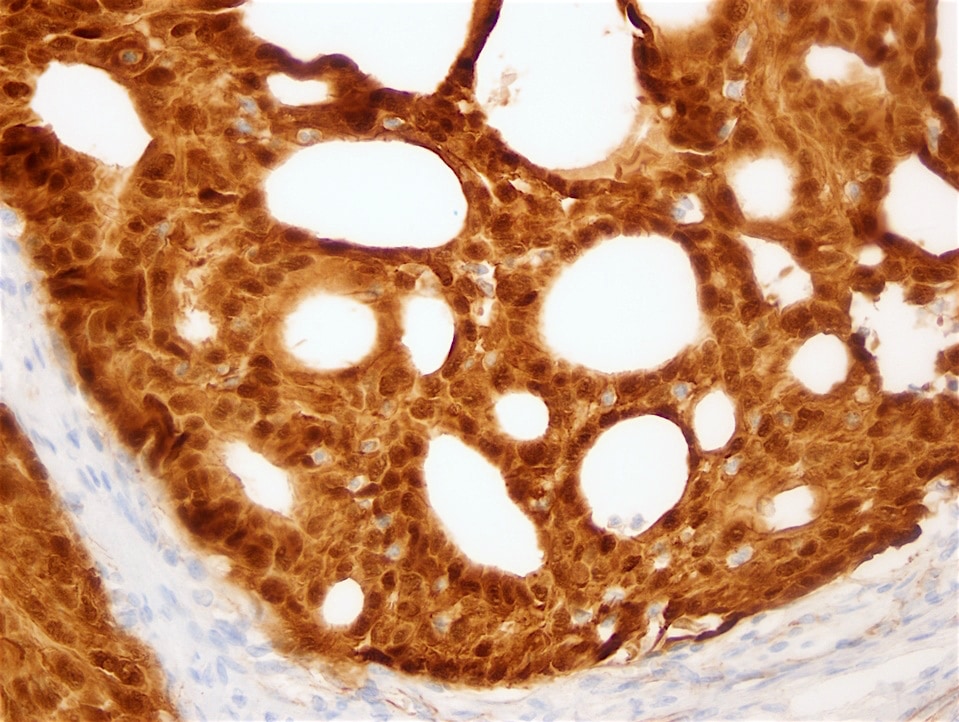
β-catenin
Discussion:
Cribriform morular variant of papillary thyroid carcinoma (CMV-PTC) is rare, accounting for 0.2% of papillary thyroid carcinoma (PTC) cases (World J Surg 2018;42:3616). It is associated with sporadic or germline mutations of the adenomatous polyposis coli (APC) gene (WHO Classification of Tumours of Endocrine Organs, 4th ed., 2017). It occurs almost exclusively in young adult women. Sporadic cases are usually solitary but cases associated with familial adenomatous polyposis (FAP) are often multifocal (Kakudo: Thyroid FNA Cytology, Differential Diagnoses and Pitfalls, 2016).
CMV-PTC mimics follicular neoplasm or nodular goiter at ultrasound (J Med Ultrason 2015;42:83) but cytological preparation shows hypercellularity with many atypical follicular cells containing numerous intranuclear cytoplasmic inclusions and nuclear grooves, which are diagnostic for PTC. CMV-PTC is encapsulated or circumscribed with mixed cribriform, papillary, solid, tall columnar and morular patterns. The lumen of the cribriform areas usually lacks colloid. The cells have abundant eosinophilic cytoplasm and pseudostratification with hyperchromatic nuclei, grooves and pseudoinclusions. Morules are cell clusters with eddy formations usually seen scattered within the tumor (Acta Cytol 2004;48:431, Acta Cytol 2011;55:13). Perinuclear clearing characteristic of this variant is observed in the morules (Kini: Thyroid Cytopathology, an Atlas and Text, 2nd ed., 2015). Its presence, identified by pale staining of most nuclei accompanied by condensed chromatin at their periphery, is useful for diagnosis (Acta Cytol 2004;48:431, Diagn Cytopathol 2010;38:890). Typically there is no definite ground glass appearance (Ali, Cibas: The Bethesda System for Reporting Thyroid Cytopathology, 2nd ed., 2018). Cytoplasmic lipid may be present (Pathobiology 2017;84:251) with vacuoles that are positive for Oil red O and adipophilin.
Immunohistochemistry with β-catenin shows a change from the membranous pattern of normal thyroid cells to cytoplasmic and nuclear staining in tumor cells, which is highly specific for CMV-PTC (Acta Cytol 2004;48:431, Acta Cytol 2013;57:127). In addition, estrogen receptor and progesterone receptor reveal strong nuclear immunopositivity except in morular cells (Mod Pathol 1999;12:400). Immunostaining can be applied to both cytologic and surgical specimens.
Although insular carcinoma and follicular neoplasm may also present with cribriform patterns, these tumors have smaller and rounder spaces, which may contain colloid. Morules may mimic squamous metaplasia but their cytoplasm is not densely stained.
Lobectomy is recommended for non FAP-associated CMV-PTC and total thyroidectomy for FAP-associated CMV-PTC. However, extensive lymph node dissection is not necessary because nodal metastases are rare (Endocr J 2011;58:685, Pathol Res Pract 2015;211:712). The prognosis is excellent (Endocr Relat Cancer 2017;24:R109). The clinician should be alerted to exclude FAP since this diagnosis is the first indicator of FAP syndrome in 25% of cases (Int J Med Sci 2004;1:43).
Test question answer:
B. Familial adenomatous polyposis
Familial adenomatous polyposis is a rare condition transmitted in an autosomal dominant pattern related to germline mutation of the tumor suppressor gene APC, which strongly predisposes to colorectal cancer. Thyroid carcinoma rarely coexists with FAP (in just 0.3-1.2% of cases). When it does, it is almost exclusively CMV-PTC.