
18 October 2017 - Case of the Week #440
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Week page. To subscribe or unsubscribe to Case of the Week or our other email lists, click here.
Thanks to Dr. Jatin S. Gandhi, Consultant at Rajiv Gandhi Cancer Institute and Research Centre, New Delhi (India) for contributing this case, Dr. Belinda Lategan, St. Boniface Hospital, Winnipeg, Manitoba (Canada), for editing the discussion, and to Dr. Genevieve M. Crane, University of Rochester (New York) for her review. To contribute a Case of the Week, first make sure that we are currently accepting cases, then follow the guidelines on our main Case of the Week page.
 Advertisement
Advertisement
Website news:
(1) At the beginning of October, we saw a record 322 jobs posted at PathologyOutlines.com. We try to make our Jobs page as useful as possible, and appreciate the response of our advertisers. Where are all the cytopathology jobs? Scroll down to Regional totals by subspecialty, just below the subspecialties, and pick cytopathology from the drop down menu. Scroll down to see the totals, which are followed by summaries of the ads, followed by the full ads.
(2) See the most recently updated topics here. These are posted regularly on our blog.
(3) We have enlarged the text at the top of the header, making it easier to see. Also, we have moved the Get Involved information to the Contact Us page.
Visit and follow our Blog to see recent updates to the website.
Case of the Week #440
Clinical history:
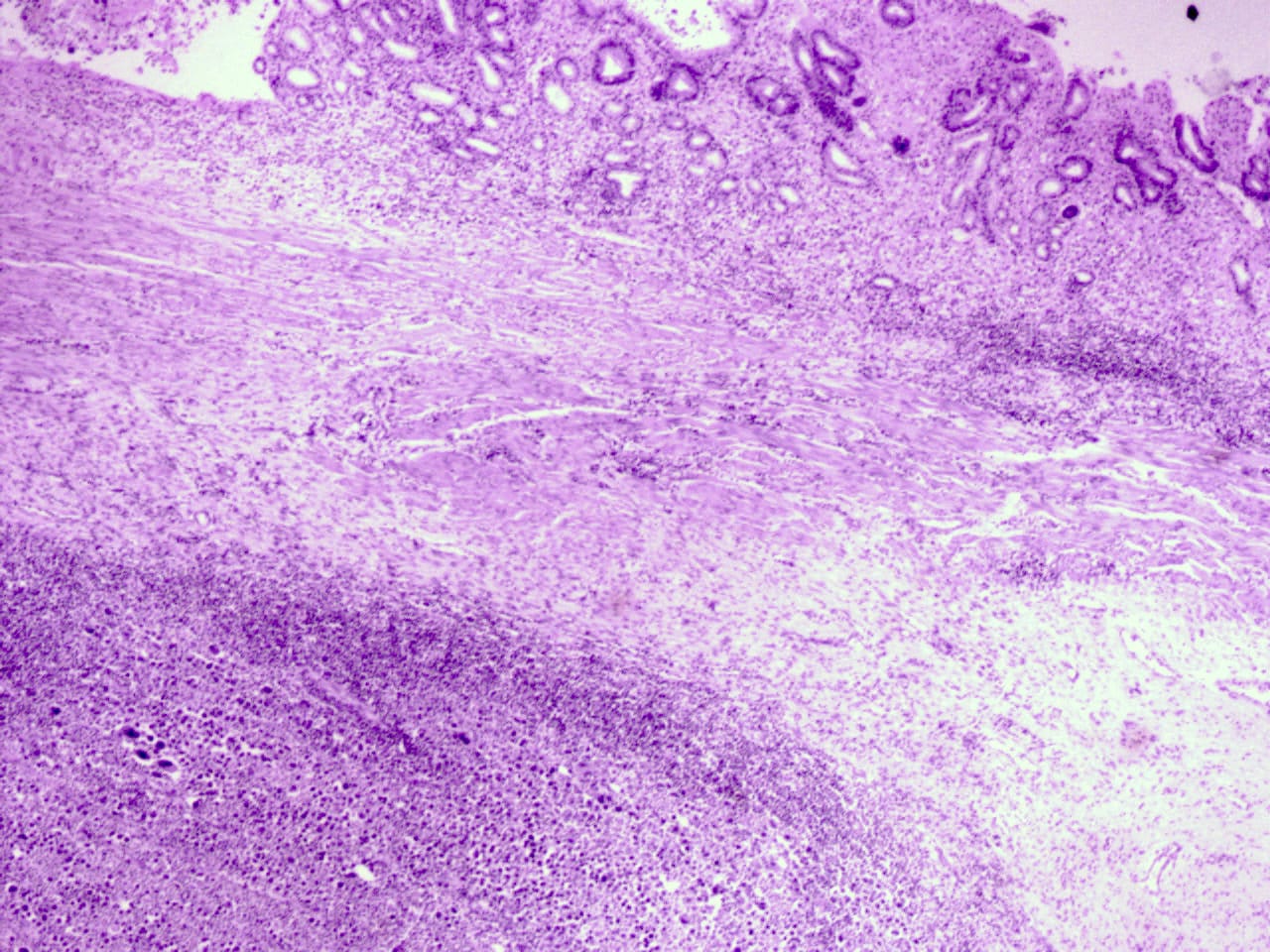
A 37 year old woman presented with recurrent vomiting and abdominal pain, with workup suggestive of gastric outlet obstruction. She underwent an open subtotal gastrectomy.
Histopathology images:

What is your diagnosis?
Diagnosis:
Primary gastric classical Hodgkin lymphoma, British National Lymphoma Investigation (BNLI) grade 2 (but see discussion)
Special stains:
Test question (answer at the end):
What is the most commonly occurring lymphoma of the stomach?
A. Anaplastic large T cell lymphoma
B. EBV related lymphoma of the elderly
C. Diffuse large B cell lymphoma and extranodal marginal zone (MALT) lymphoma
D. Primary gastric classical Hodgkin lymphoma
Discussion:
The stomach is the most common site of primary gastrointestinal lymphomas. The vast majority of gastric lymphomas are diffuse large B cell or extranodal marginal zone (MALT) lymphomas, which together account for up to 50% of all cases. In contrast, primary gastric classical Hodgkin lymphoma is extremely rare (< 1%) (J Korean Surg Soc 2012;83:111).
Lymphomas in the stomach are considered a primary gastric lymphoma when the bulk of disease is located in the stomach itself, as opposed to gastric involvement as part of systemic lymphoproliferative disease (WHO Classification of Tumours of the Digestive System, IARC 2010). Dawson et. al. proposed specific criteria which also requires:
(a) no peripheral lymphadenopathy at presentation
(b) no enlarged mediastinal lymph nodes
(c) normal complete blood count including differential
(d) the predominance of the lesion despite the presence of disease in adjacent lymph nodes
(e) no lymphomatous involvement of the liver or spleen (Br J Surg 1961;49:80).
Akin to Hodgkin lymphoma (HL) in nodal sites, gastric classical Hodgkin lymphoma is characterized by mono- and multinucleated tumor cells (Hodgkin and Reed-Sternberg cells / HRS cells), which are rimmed by rosettes of T lymphocytes, all in a heterogeneous background of nonneoplastic inflammatory and accessory cells (WHO Classification of Tumours of Haematopoietic and Lymphoid Tissue, IARC 2008).
As illustrated in this case, HRS cells are highlighted by CD30, and to a lesser extent, CD15 (the CD15 staining in this case appears questionable). T cell markers (e.g. CD3) demonstrate T cell rosettes around the HRS cells. Although up to 60% of Hodgkin lymphoma cases overall demonstrate EBV DNA sequences by EBER - ISH, this case was negative (Arch Pathol Lab Med 2002;126:1534). The tumor cells were negative for ALK and CD79a (images not available).
This is a difficult case to classify. Arguments against the diagnosis of primary gastric Hodgkin lymphoma are: (a) the tumor cells are not typical for HRS cells; (b) gastric classical Hodgkin lymphoma is exceedingly rare, compared to the more common diffuse large B cell lymphoma and marginal zone lymphomas; (c) although the tumors cells are CD30+, they do not appear to be CD15+; (d) PAX5 is brighter than typical of Hodgkin lymphoma; (e) the negative EBER - ISH is not specific, but if positive, would be more suggestive of Hodgkin lymphoma. Other possibilities include an unusual diffuse large B cell lymphoma or transformation of a marginal zone lymphoma. Anaplastic large cell lymphoma is unlikely due to the PAX5 staining and the slight CD20+. The negative keratin and EMA stains make carcinoma unlikely.
The initial differential diagnosis included grey zone lymphoma intermediate between DLBCL and Hodgkin, anaplastic large cell lymphoma and classical Hodgkin lymphoma, syncytial variant of nodular sclerosis subtype. The case was sent to an expert (within India) and was diagnosed as classical Hodgkin lymphoma based on the background, morphology and immunohistochemistry. The case was then later discussed in the First Indian Cancer Congress, New Delhi in 2012-2013, with the same conclusion.
It is difficult to predict the prognosis of primary gastric classical Hodgkin lymphoma due to its rarity, but several case reports have suggested a poor prognosis, with 40 - 60% of patients succumbing to the disease within 1 year of diagnosis (Arch Pathol Lab Med 2002;126:1534).
Test Question Answer:
C. Diffuse large B cell lymphoma and extranodal marginal zone (MALT) lymphoma
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Week page. To subscribe or unsubscribe to Case of the Week or our other email lists, click here.
Thanks to Dr. Jatin S. Gandhi, Consultant at Rajiv Gandhi Cancer Institute and Research Centre, New Delhi (India) for contributing this case, Dr. Belinda Lategan, St. Boniface Hospital, Winnipeg, Manitoba (Canada), for editing the discussion, and to Dr. Genevieve M. Crane, University of Rochester (New York) for her review. To contribute a Case of the Week, first make sure that we are currently accepting cases, then follow the guidelines on our main Case of the Week page.
Advertisement
Website news:
(1) At the beginning of October, we saw a record 322 jobs posted at PathologyOutlines.com. We try to make our Jobs page as useful as possible, and appreciate the response of our advertisers. Where are all the cytopathology jobs? Scroll down to Regional totals by subspecialty, just below the subspecialties, and pick cytopathology from the drop down menu. Scroll down to see the totals, which are followed by summaries of the ads, followed by the full ads.
(2) See the most recently updated topics here. These are posted regularly on our blog.
(3) We have enlarged the text at the top of the header, making it easier to see. Also, we have moved the Get Involved information to the Contact Us page.
Visit and follow our Blog to see recent updates to the website.
Case of the Week #440
Clinical history:
A 37 year old woman presented with recurrent vomiting and abdominal pain, with workup suggestive of gastric outlet obstruction. She underwent an open subtotal gastrectomy.
Histopathology images:
What is your diagnosis?
Diagnosis:
Primary gastric classical Hodgkin lymphoma, British National Lymphoma Investigation (BNLI) grade 2 (but see discussion)
Special stains:
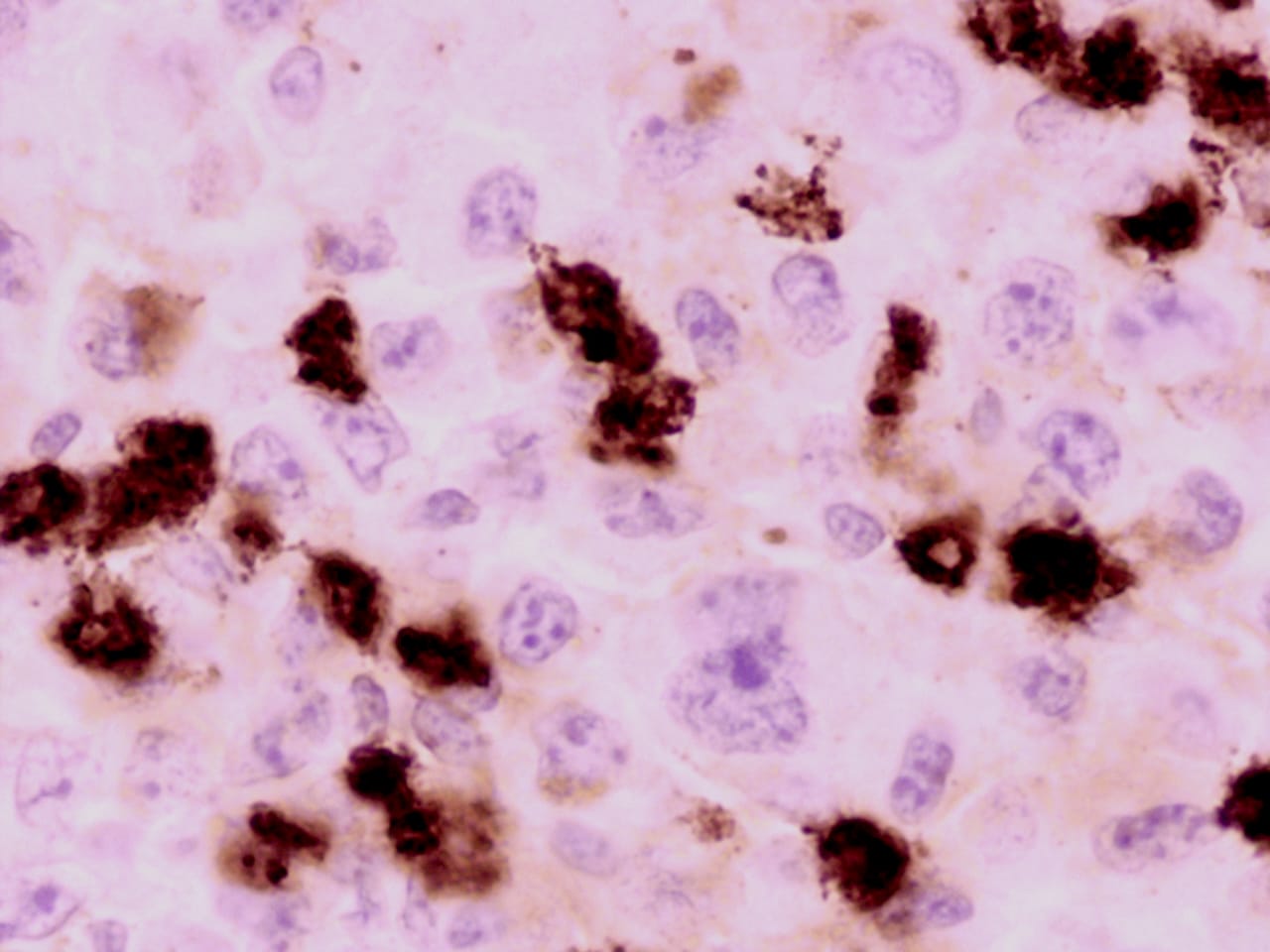
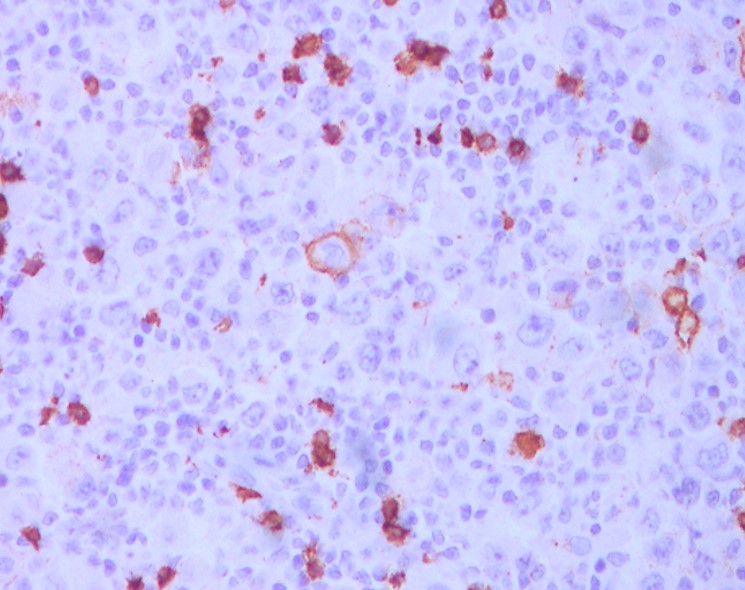
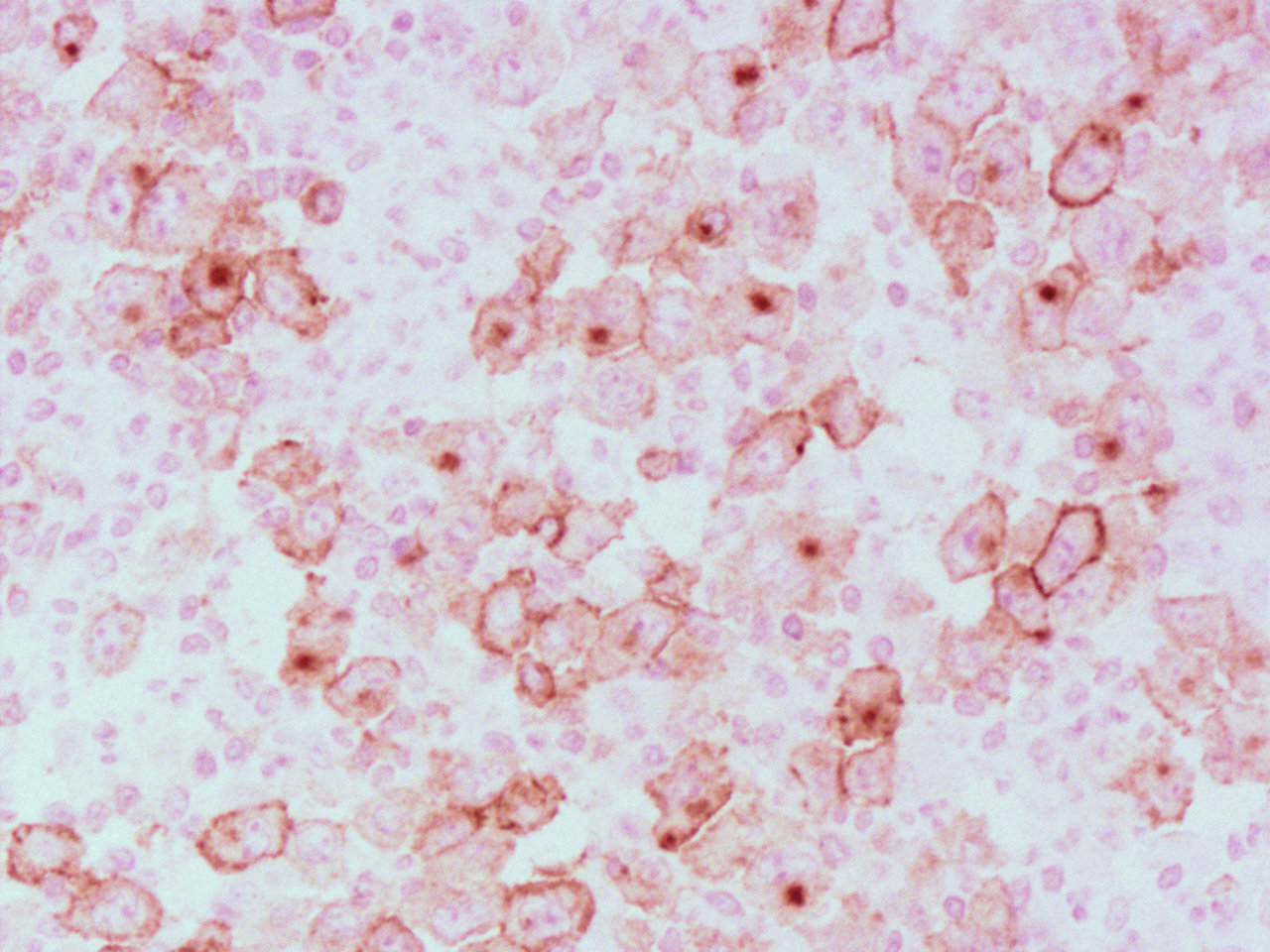
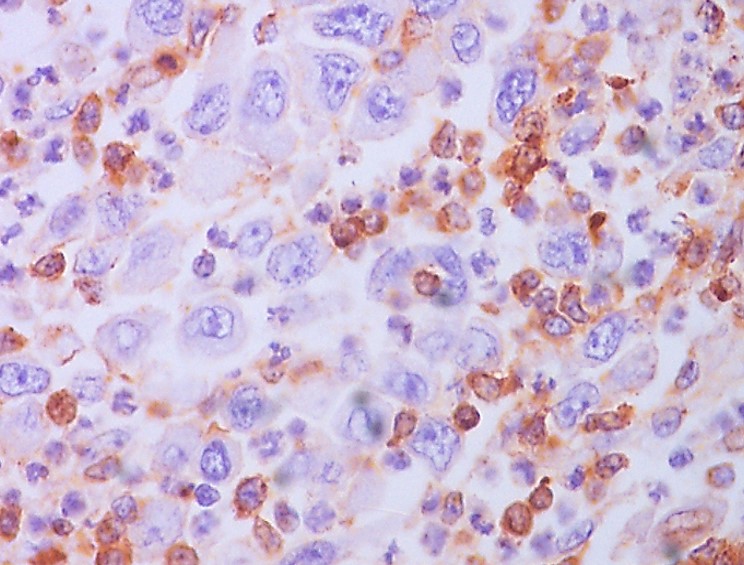
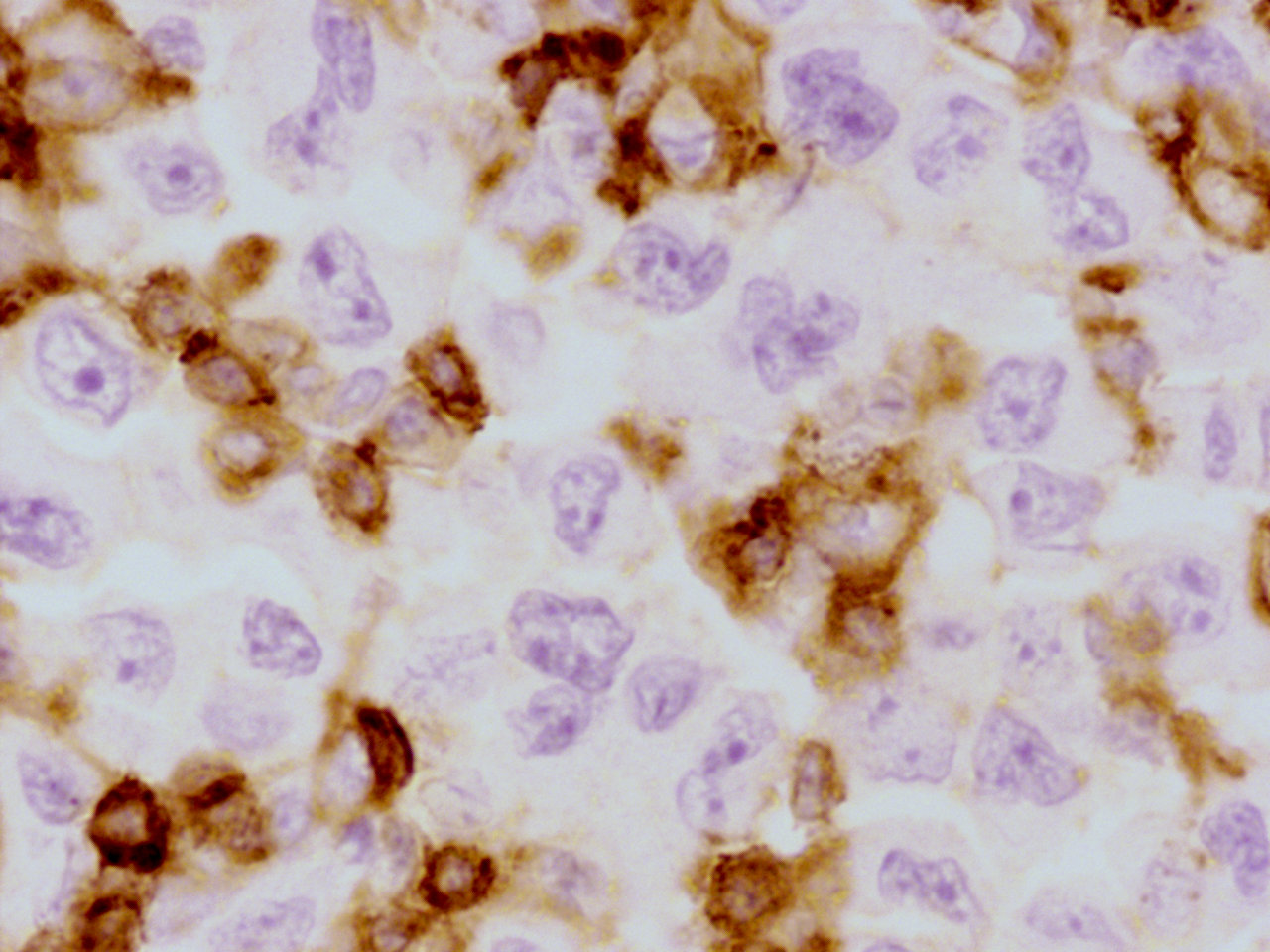
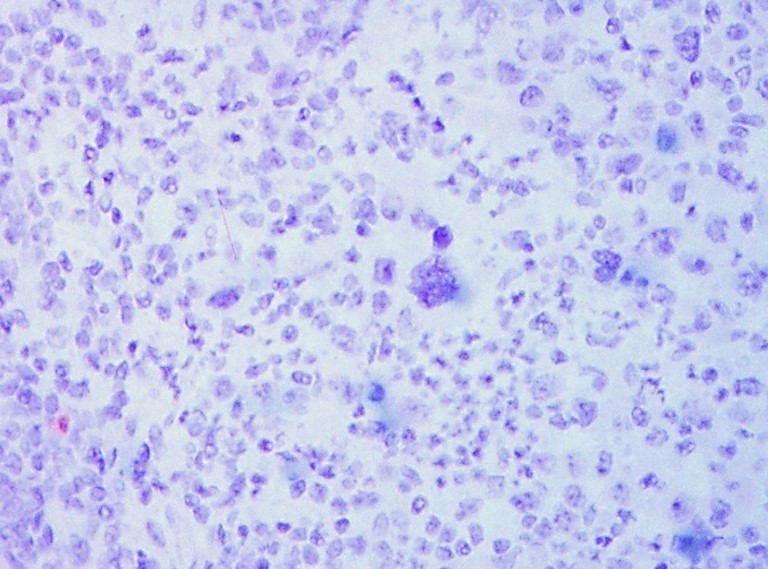
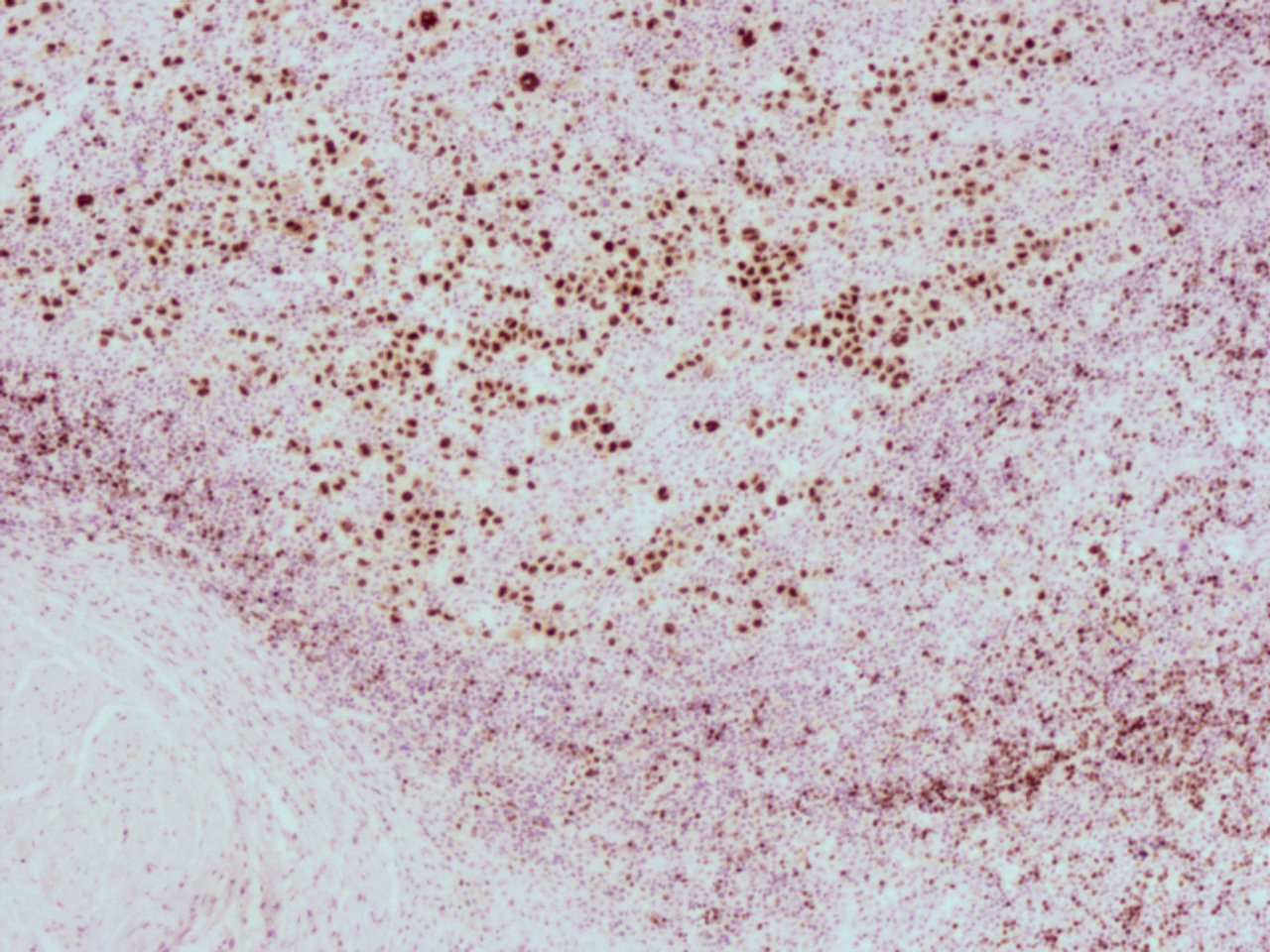
CD3, exhibiting rosettes
CD15
CD20
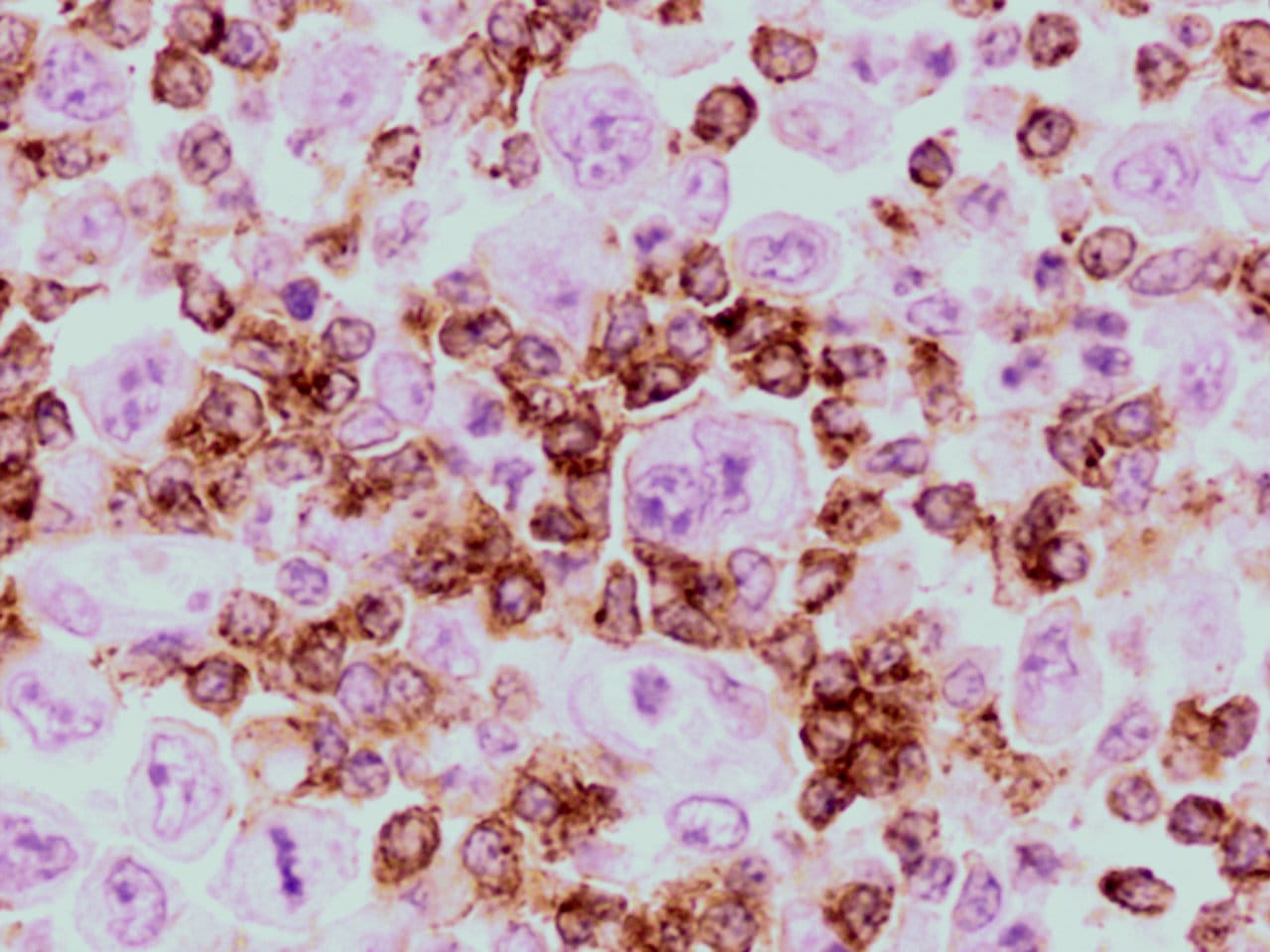
CD30
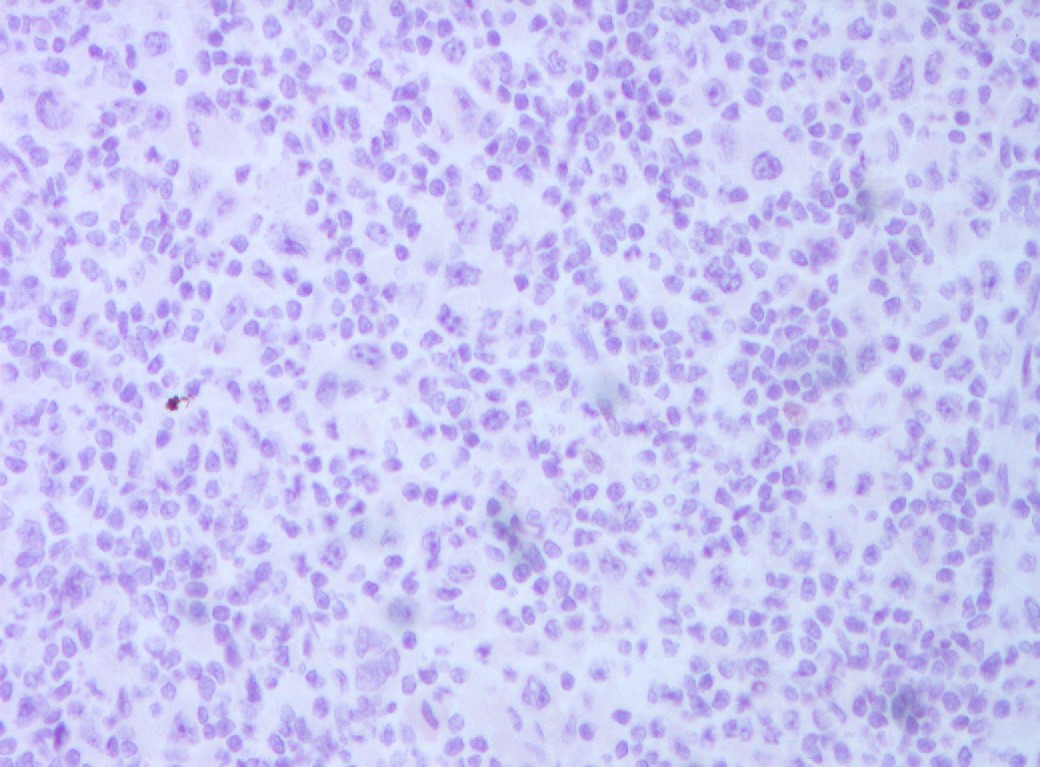
EBER - ISH
EMA, staining plasma cells
LCA
Pan-CK
PAX
Test question (answer at the end):
What is the most commonly occurring lymphoma of the stomach?
A. Anaplastic large T cell lymphoma
B. EBV related lymphoma of the elderly
C. Diffuse large B cell lymphoma and extranodal marginal zone (MALT) lymphoma
D. Primary gastric classical Hodgkin lymphoma
Discussion:
The stomach is the most common site of primary gastrointestinal lymphomas. The vast majority of gastric lymphomas are diffuse large B cell or extranodal marginal zone (MALT) lymphomas, which together account for up to 50% of all cases. In contrast, primary gastric classical Hodgkin lymphoma is extremely rare (< 1%) (J Korean Surg Soc 2012;83:111).
Lymphomas in the stomach are considered a primary gastric lymphoma when the bulk of disease is located in the stomach itself, as opposed to gastric involvement as part of systemic lymphoproliferative disease (WHO Classification of Tumours of the Digestive System, IARC 2010). Dawson et. al. proposed specific criteria which also requires:
(a) no peripheral lymphadenopathy at presentation
(b) no enlarged mediastinal lymph nodes
(c) normal complete blood count including differential
(d) the predominance of the lesion despite the presence of disease in adjacent lymph nodes
(e) no lymphomatous involvement of the liver or spleen (Br J Surg 1961;49:80).
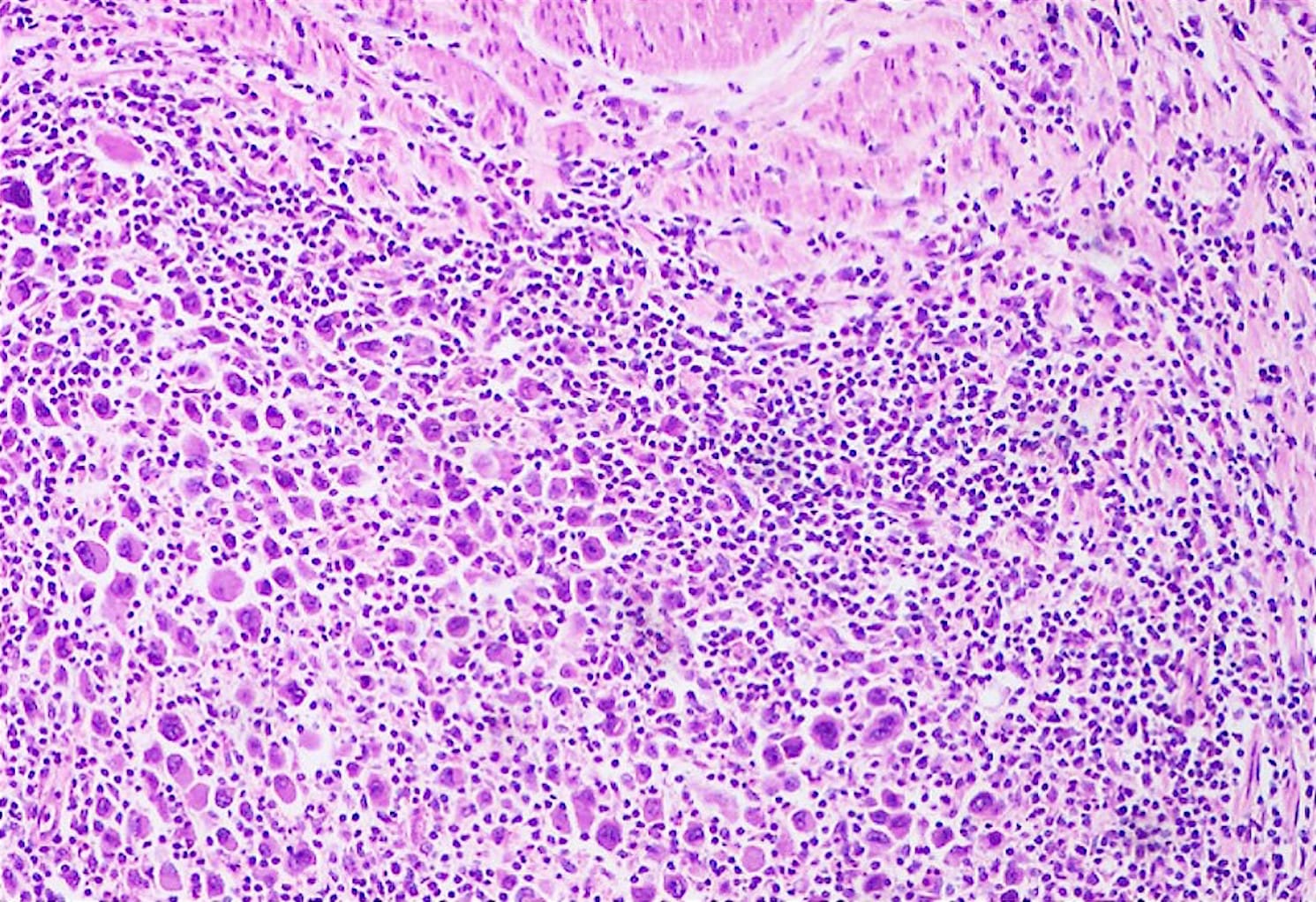
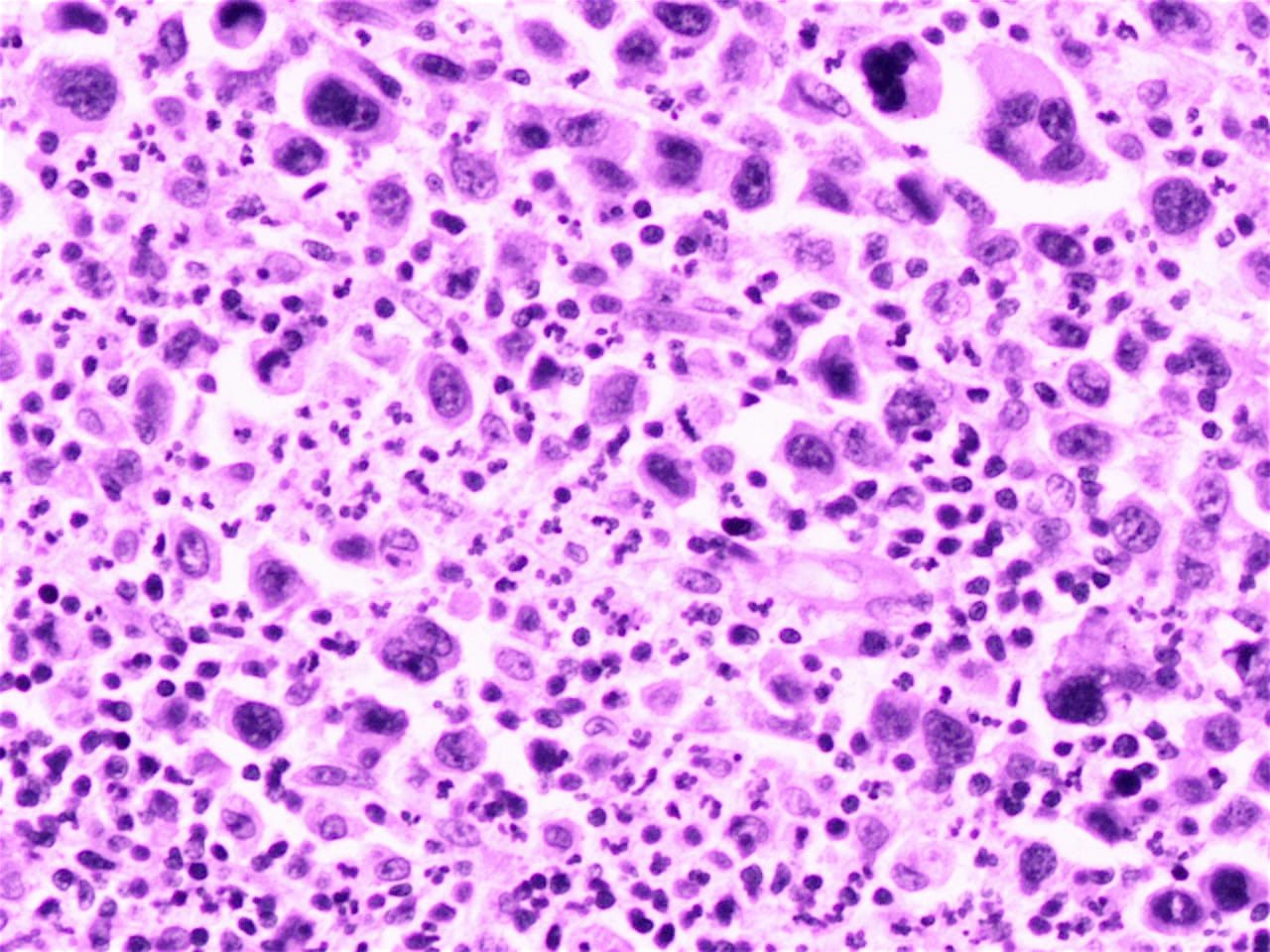
Akin to Hodgkin lymphoma (HL) in nodal sites, gastric classical Hodgkin lymphoma is characterized by mono- and multinucleated tumor cells (Hodgkin and Reed-Sternberg cells / HRS cells), which are rimmed by rosettes of T lymphocytes, all in a heterogeneous background of nonneoplastic inflammatory and accessory cells (WHO Classification of Tumours of Haematopoietic and Lymphoid Tissue, IARC 2008).
As illustrated in this case, HRS cells are highlighted by CD30, and to a lesser extent, CD15 (the CD15 staining in this case appears questionable). T cell markers (e.g. CD3) demonstrate T cell rosettes around the HRS cells. Although up to 60% of Hodgkin lymphoma cases overall demonstrate EBV DNA sequences by EBER - ISH, this case was negative (Arch Pathol Lab Med 2002;126:1534). The tumor cells were negative for ALK and CD79a (images not available).
This is a difficult case to classify. Arguments against the diagnosis of primary gastric Hodgkin lymphoma are: (a) the tumor cells are not typical for HRS cells; (b) gastric classical Hodgkin lymphoma is exceedingly rare, compared to the more common diffuse large B cell lymphoma and marginal zone lymphomas; (c) although the tumors cells are CD30+, they do not appear to be CD15+; (d) PAX5 is brighter than typical of Hodgkin lymphoma; (e) the negative EBER - ISH is not specific, but if positive, would be more suggestive of Hodgkin lymphoma. Other possibilities include an unusual diffuse large B cell lymphoma or transformation of a marginal zone lymphoma. Anaplastic large cell lymphoma is unlikely due to the PAX5 staining and the slight CD20+. The negative keratin and EMA stains make carcinoma unlikely.
The initial differential diagnosis included grey zone lymphoma intermediate between DLBCL and Hodgkin, anaplastic large cell lymphoma and classical Hodgkin lymphoma, syncytial variant of nodular sclerosis subtype. The case was sent to an expert (within India) and was diagnosed as classical Hodgkin lymphoma based on the background, morphology and immunohistochemistry. The case was then later discussed in the First Indian Cancer Congress, New Delhi in 2012-2013, with the same conclusion.
It is difficult to predict the prognosis of primary gastric classical Hodgkin lymphoma due to its rarity, but several case reports have suggested a poor prognosis, with 40 - 60% of patients succumbing to the disease within 1 year of diagnosis (Arch Pathol Lab Med 2002;126:1534).
Test Question Answer:
C. Diffuse large B cell lymphoma and extranodal marginal zone (MALT) lymphoma
